Artículos
Prototypical values in the avoidant personality disorder
Valores prototípicos del trastorno evitativo de la personalidad
Prototypical values in the avoidant personality disorder
Anuario de Psicología, vol. 45, no. 3, 2015
Universitat de Barcelona
Abstract: This ex post facto retrospective case-control study sought to establish the identification of a group of male and female participants with avoidant personality disorder through a repertoire of prototypical values of this psychopathological entity in opposition to an equivalent group without this disorder. The SCID-II interview, Millon's Multiaxial Inventory Personality (MCMIIII) and the evocative self-report for avoidant prototypical values were applied. The hypothesis was confirmed, and we found - into the group of cases, but not in the group of controls - such values as certainty, preparation, personal initiative, fortitude, self-control, determination, self-confidence and prediction. It is concluded that these are prototypical values in the avoidant personality disorder
Keywords: Disorder, avoidance, personality, ACT.
Resumen: El presente estudio ex post facto retrospectivo de casos y controles buscó establecer en un grupo de participantes masculinos y femeninos con trastorno de personalidad por evitación en contraste con uno equivalente sin dicho trastorno, su identificación con un repertorio de valores prototípicos de esta entidad psicopatológica. Se aplicó la entrevista SCID-II, el Inventario Multiaxial de Personalidad de Millon (MCMI-III) y el autoinforme evocativo de valores prototípicos evitativos. Se confirmó la hipótesis de estudio hallando en los participantes con el trastorno evitativo de la personalidad su identificación con los valores aludidos a diferencia de los participantes sin este trastorno. Tales valores fueron: certidumbre, preparación, iniciativa, fortaleza, control, resolución, confianza, predicción, habilidad y optimismo. Estos valores mostraron predicción respecto a esta entidad psicopatológica. Se concluye que estos valores son prototípicos del trastorno evitativo de la personalidad
Palabras clave: trastorno, evitación, personalidad, ACT.
The prevalence of personality disorders has increased in world population (Roca & Bernardo, 1998), and they have now reached the level of traditional psychopathologies such as depression, anxiety, and psychosis (Millon & Everly, 1994; Echeburúa & Corral, 1999). However, although the information available on their clinical treatments is vast, it is also very dissimilar (Caballo, 1998; Gunderson & Gabbard, 2000).
In the case of the avoidant personality disorder treatment, there are very few empirical studies proving the efficacy of clinical interventions. So far, the approach with the most empirical incursions and with reproducible results has been cognitive-behavioral (Stravynski, Marks & Yule, 1982; Echeburúa & Corral, 1999; Robin & Di Giuseppe, 1993). Other studies have tackled this disorder, but their lack in design and control affect their reliability, despite some authors' opinion to the contrary (Pérez-Álvarez, 2001; Sanislow & McGlashan, 1998; Perry, Bannon & Ianni, 1999; Perry & Bond, 2000).
One of the most relevant aspects in the interventions on this disorder is the behavioral-training disorder (Stravynski, Belisle, Marcouiller, Lavallee & Elie, 1994), mainly with reinforcement and extinction techniques carried out on fear and avoidance conducts. Only modest results have been reported in this respect, though (Stravynski, Grey & Elie, 1987). In addition, it has been pointed out that such techniques were inconclusive in maintaining the long-term results (Quiroga & Errasti, 2001), and such was also the case with social skills training (Alden, 1989). However, it has been found that systematic desensibilization and differentially reinforced behavioral trial, along with the modification of self-image, generate significant changes in different behaviors of the avoidant personality disorder (Renneberg, Goldstein, Phillips & Chambless, 1990).
A promising alternative as compared to the ones mentioned above is Acceptance and Commitment Therapy, as it highlights in the client the realization of new value directions when in contact with aversive stimulation which allow them to regain the control of their experience in the context of new priorities in several domains of their life (Hayes, Strosahl & Wilson, 1999; Luciano, Rodríguez & Gutiérrez, 2004; Luciano & Hayes, 2001; Wilson & Luciano, 2002). This clinical approach showed high efficacy in disorders such as substance abuse (Gifford et al., 2004; Hayes et al., 2004; Twohig, Shoenberger & Hayes, 2007), sexual dysfunction (Montesinos, 2003), eating disorders (Baer, Fischer & Huss, 2005; Heffner, Sperry, Eifert & Detweiler, 2002), and psychosis (Bach & Hayes, 2002; Gaudiano & Herbert, 2006) among others. However, no approaches or results have yet been reported in personality disorders. Although values are idiosyncratically generated by the client in ACT, and they are part of their historic baggage (Páez, Gutiérrez, Valdivia & Luciano, 2006), the chance for a specific repertoire of these in avoidant personality disorder deserves considering its exploitation, as it would yield a general contextual framework to manage the disentanglement processes of idyosincratic values, cognitive defusion and delliteration, among other processes of ACT (Hayes & Bronstein, 1986). Especially in this disorder, clients present excessive difficulties to clear their values and set forth new evaluative directions for the good of their mental health (Luciano et al., 2004).
In light of the above, the present case-control study intends to assess the hypothesis that a group of men and women with avoidance personality disorder - unlike their control counterparts - identify themselves with a prototypical repertoire of values emerging in the evaluated person's context by means of a self-report.
Method
We conducted a quasi-experimental type of study, a case-control ex post facto design, in order to determine whether differences exist between a group of men and women with avoidance personality disorder and a group of their peers without the disorder when identifying them through a repertoire of prototypical values of this psychopathological entity.
Sample
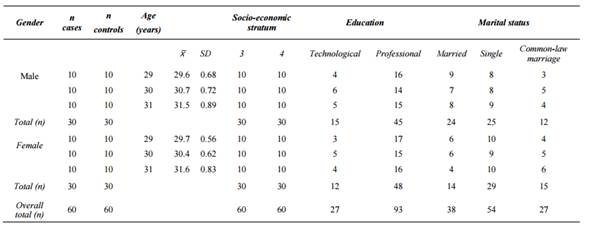
Out of a general population of 399 adults (147 women and 132 men) registered in a record of eligible parties for the study, we selected a convenient sample of 120 participants who eventually took part in it as follows: 30 men and 30 women diagnosed with avoidance personality disorder according to the criteria of DSM-IV-TR(r) (Frances, Pincus & First, 2008), and an equivalent group of 30 men and 30 women without avoidance personality disorder. The remaining 279 participants out of the initial 399 registered were discarded by the research team as they did not comply with the necessary criteria for the study and, in other cases, because they withdrew from it. The selection of participants was conducted through an interview and assessment of their scores in the 2007 Spanish edition (Cardenal & Sánchez, 2007; Cardenal, Sánchez & Ortiz-Tallo, 2007) of Theodore Millon's MCMI-III(r) Personality Multiaxial Inventory (MCMI-III). We obtained the following scores: for the presence of phobic personality disorder (case group), a base rate over 85 (Weltzler, 1990); and for the non-presence of such disorder (control group), scores (TB) between 0 and 15 (Millon & Davis, 1998; Cardenal & Sánchez, 2007). For both groups, only the subjects with an honesty index of X>590 were selected. The ages of the participants were between 29 and 31 years, with completed technological or professional studies, belonging to the socioeconomic strata 3 and 4 of the city of Bucaramanga (Colombia). The latter belong to the Colombian socio-economic stratification conducted by the National Statistics Administrative Department (DANE, 2011), a classification of the homes of citizens based on their physical characteristics and those of their surroundings.
It also includes a classification according to the capabilities of their inhabitants to satisfy their basic needs and to pay public services bills, according to law 142 of 1994, which was amended by the Conpes 3386 (Departamento Nacional de Planeación de Colombia, 2005), which comprises the information of the general population censuses of Colombia.
Instruments
We used the following instruments to diagnose avoidant personality disorder:
Millon's Multiaxial Clinical Inventory - III (Cardenal & Sánchez, 2007; Cardenal, Sánchez & Ortiz-Tallo, 2007), spanish version. This instrument evaluates ten clinical syndromes from moderate to severe in subjects from 17 years of age onwards through 175 dichotomic items with a true/false response format. It comprises validity and response tendency scales and it is assessed though direct scores and base rates, segmented by sex. The clinical personality traits are framed in scores between 75 and 85 and the disorder scores over 85 points. Its honesty index invalidates the test with scores below 34 and over 178. Its reliability is .80 and test-retest was .84 and .96. The time of application ranges between 15 and 25 minutes.
Clinical structured interview for personality disorders of axis II of DSM-IV-TR (First, 1999; Frances, Pincus & First, 2008). In a semi-structured diagnostic interview to evaluate twelve personality disorders of axis II of DMS-IV-TR for both a categorial (present or absent) and a dimensional (amount of criteria coded for personality disorder) diagnosis. Within its structure, the interview considers ten specific personality disorders and two appendix categories successively. It comprises questions and criteria from DSMIV-TR (First, 2001) for diagnosis. Likewise, it includes scores for personality disorder criterion items such as (?), (1), (2), (3), where the (?) sign means "inadequate information to code the criterion as 1, 2, 3". Value 1 means "absent or false"; value 2 means a "sub threshold" level, i.e., it means that "the level was almost reached, the trait is present but it is not severe enough to cause deterioration or discomfort"; and finally value 3 means "threshold or true", which comprises the following features: pathological, persistent, and generalized (Frances, Pincus & First, 2008). In case more than one personality disorder's criteria are met, the interviewer must indicate the main diagnosis of axis II. The interviewee is usually the only source of information; however, we should take into account information from previous therapists, family members, or other referents to settle the matter.
To evaluate the personal identification with the prototypical values of avoidant personality disorder we used the following instrument:
Evocative self-report of prototypical values of the avoidant personality disorder (Álvarez, 2014). Built on the basis of scientific literature and reports of clinical cases on the characteristics and manifestations of avoidant personality disorder, it evaluates the degree of personal identification the examinee experiences towards a set of ten values emerging from the context of the disorder: control, certitude, foresight, resolution, hope, confidence, confrontation, prediction, ability, and optimism. Each of them is defined in an appreciatory or evaluative proposition, like "I need to understand things at all costs to take a position and a course of action", "I always need to know what I'm going to do", "I always wait for others to take the first step", "I get easily intimidated and overwhelmed", "Problems overwhelm me and I don't know what to do", "I always walk away from problems and difficulties", "I feel others can fail me at any time", "The unknown makes me anxious", "I am unskilled", "Things can't get any better". Having a high priority in the hierarchy of the avoidant personality disorder experience, these values cause psychological discomfort and associated suffering, more specifically: giving excessive value to certitude, getting easily and permanently confused; giving an extremely high value to foresight, maximum fear of improvising and being influenced; giving disproportionate value to hope, a feeling of overwhelming helplessness; giving extreme value to control, lack of control; giving excessive value to confrontation, avoidance; giving a disproportionate value to confidence, lack of confidence; giving excessive value to prediction, lack of prediction; giving excessive value to ability, the feeling of self-inefficacy of unskillfulness; giving extreme value to optimism, permanent pessimism. The person being evaluated must score - in a scale from 0 to 5 - their subjective degree of identification with the value and its corresponding appreciatory proposition as follows: 0 (None); 1 (Minimum); 2 (Somewhat); 3 (Medium); 4 (Very); 5 (Maximum). This instrument presents a reliability of α = .84 and an interjudge validity with a coefficient of K = .85 and with H0: K=0 y H1=k≠0, with α =0.001 (Fleiss, 1971; Anastasi, 1976; Magnusson, 1982)
Procedure
First stage
We obtained approval for the protocol of the procedure from the university's ethics committee. We gathered 399 participants (men and women) who had registered in a record of eligible parties for the study based on persons related to students of the university's Psychology degree. We incorporated those presenting symptomatology akin to avoidant personality disorder and peer counterparts who did not in order to complete the groups of cases and controls through an analysis conducted by the research team.
Second stage
We contacted the participants who agreed to participate with no monetary compensation and we proceeded to structure the calendar to conduct the interviews in order to select the groups of cases and controls by administering the SCID-II (First, 1999; Frances et al., 2008) for the diagnosis of avoidant personality disorder. They had been previously given the APA informed consent form where the goal of the study was explained, as were the procedures to follow, the instruments to apply, information confidentiality matters, the process to hand back the results in an individual session, the risks of the study, and other related aspects. We obtained everyone's consent and signature verified through their ID. This task was conducted by students from higher semesters from the Psychology degree who had been trained by the study's professional supervision team. Out of the participants registered in the record, 38 women and 34 men (case group) complied with the clinical diagnostic criteria of avoidant personality disorder, out of which, six women and two men eventually refused to be part of the study, and later on, for different reasons, two of each gender dropped out, thus leaving a final case group with 30 male and 30 female participants. Thirty paired-up participants (male and female) were selected for the control group. We also applied the 2007 Spanish version of the Millon's Miltiaxial Clinical Inventory (Cardenal & Sánchez, 2007), and then, the Evocative selfreport of prototypical values of avoidant personality disorder (Álvarez, 2014).
Third stage
All the procedures were recorded in video and classified for a later review by the team of professionals in charge of the research. Confidentiality of information was guaranteed through custody of the material obtained in a restricted-access file by the Psychology professionals in charge of the process. Each participant was approached individually to guarantee their anonymity and to prevent any contact between them.
Fourth stage
The instruments used were revised and the videos were analyzed individually by three professional psychologists from the Psychology department. Clinical assistance was guaranteed by means of a follow-up during the contact, the information gathering, the process to hand back the results individually, and accompaniment when it was consented.
Results
Below we will present the results of the study: firstly, the chi square test results show what significance there was to confirm the hypothesis of no relation between identification with values between the groups of cases and controls by gender; secondly, we will display the values of the Student t test for the groups of cases and controls (male and female) when analyzing their means according to each prototypical value; and lastly, we will present the values of the logistic regression to indicate whether such values have a predictive value (linear relation) with respect to avoidant personality disorder in the group of cases.
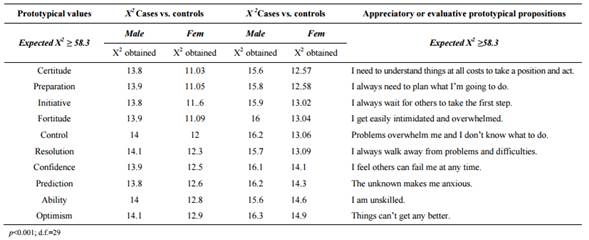
In table 2 (see next page), we can observe the results of the chi square test for the groups of cases and controls, both for male (ncases = 30 and ncontrols = 30) and female (ncases = 30 and ncontrols = 30). We can see that the X2 scores of identification with the values in the male group of cases vs. controls yielded scores in the interval 13.8<X2<14.1, and 11.03<X2<12.9 in the female group, which means that such scores were below the expectations (X2 ≥58.3). In turn, this means that, with p<0.001 and d.f.=29X2 is not significant. Therefore the variables are not related, i.e., the group of cases (both genders) identifies in the maximum degree with the prototypical values proposed as representations of their experience with avoidant personality disorder, unlike the group of controls (both genders). Such values are the following: certitude, preparation, initiative, fortitude, control, resolution, confidence, prediction, ability, and optimism. Each is given the highest priority by the persons with this disorder, for which reason their life experience becomes extremely discomforting. This is expressed through feelings of excessive fear of the unknown, of that which does not come; a desire to have everything prearranged in their life, refusing improvisation or the unexpected; a compensatory initiative acting as a relief of fear for not knowing how to control the environment; trying to compensate for one's own perceived personal weakness; the ambition to control every aspect and relationship; the irresistible need to permanently avoid doubt and to react with a determination perceived as scarce in oneself; the permanent illusion of being supported, loved, included to compensate for their own lack of confidence; the final urgency to predict their life and relationships, to become skilled in everything possible so as to be less dependent on others and to find personal meaning in their actions and feelings. Each of these values matches an appreciatory or evaluative prototypical proposition as follows: "I need to understand things at all costs to take a position and act", "I always need to plan what I'm going to do", "I wait for others to take the first step", "I get easily intimidated and overwhelmed", "Problems overwhelm me and I don't know what to do", "I always walk away from problems and difficulties", "I feel others can fail me at any time", "Everything unknown makes me anxious", "I am unskilled", "Things can't get any better".
In table 3, we can see the results obtained when comparing the means between the case and control groups as regards their identification with the prototypical values of avoidant personality disorder through the Student t test. The t scores calculated for each of the values were comprised between 2.51≤ t≤ 2.78, higher than the expected t score = 2.390. This confirmed the hypothesis about the differences between these two groups and in favor of the case group with respect to their relation to the prototypical values of avoidant personality disorder.
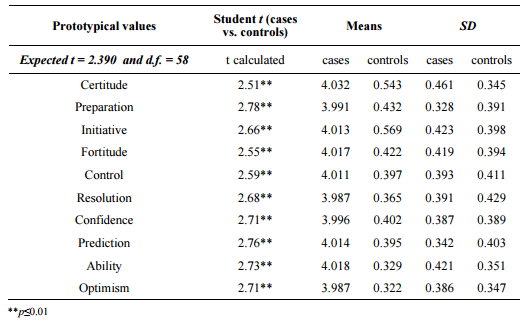
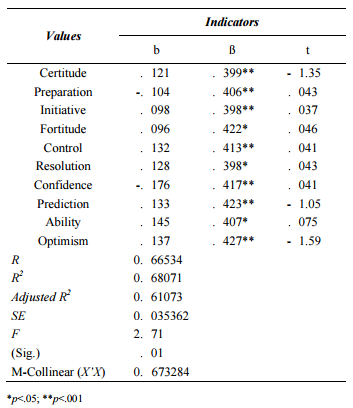
Table 4 shows the results of the logistic regression between independent variables (the prototypical values of avoidant personality disorder) and the case group of the present study. As a whole, the values were predictively significant for the group of cases with F (10,49)= 2.71 with p= 0.01. The results of the coefficient of determination indicate a significant linear relationship (R2 =0.68071), i.e., it went up to 68 % in the explanation of variance and adjusted R2 (R2 = 0.61073). The value SE=0.035362 ratifies the previous results. More specifically, the ten prototypical values reached a value of .398<β<.427, with p≤0.01, and .398<β<.422 with p≤0.05 in the standardized partial coefficient of regression, which indicates its predictive character in this disorder. This was ratified by the critical levels of t≤.05, as well as the value of multicolinearity (X'X=0.673284).
Discussion
The values are conceptualized in ACT as individual, dynamic behavioral patterns which cover different life spheres and provide a sense of direction. At the same time they are unique, i.e., they are typical and idiosyncratic of everyone (Wilson & Byrd, 2004). However, the current study found that it is possible to bear in mind the existence of a prototypical characteristic repertoire of these values in avoidant personality disorder. Based on this repertoire, each individual assigns an idiosyncratic assessment to their experience. Accordingly, it is a resource to be considered within the therapeutic process in ACT (Luciano, 2001) and, theoretically, within the relational framework theory (Hayes, Barnes-Holmes & Roche, 2001). This basic repertoire of values arises with the context along with the thoughts and feelings of the persons affected. Thus, they function as an initial guide to acknowledge the client's life priorities and help them make explicit what they give most importance to in their experience (Dahl, Wilson, Luciano & Hayes, 2005; Hayes, Follette & Linehan, 2004; Wilson & Luciano, 2002) in the different domains of their life (Luciano & Hayes, 2001, Wilson & Luciano, 2002). More specifically, having a set of prototypical values of avoidant personality disorder as a referent allows therapists to redirect clients with respect to their unattainable goals towards what they desire in their life (Eifert & Forsyth, 2005). For therapists, the prototypical values of avoidant personality disorder might help them channel the appreciatory disentanglement process with their clients (Pérez Alvarez, 1996; Hayes & Strosahl, 2004), especially those with serious difficulties to visualize, clarify, and specify them in the therapeutic process due to their condition.
An aspect to consider about these findings is that the aforementioned prototypical values have an explicative character of the disorder, which contributes to confirming its functional role within the therapeutic problem (Barnes-Holmes, Barnes-Holmes, Hayes & McHugh 2004; Whelan & Barnes Holmes, 2004). In this sense, the prototypical values of the disorder may be designed according to the control they had, they have, and they might continue to have within the person's psychological experience in the history and eventualities of their life (Millon & Everly, 1994). They may also be designed according to the way they were internalized under the social rules regulating them (Wilson & Luciano, 2002) in the community where the client was brought up (Luciano, Rodríguez & Gutiérrez, 2004).
An aspect to highlight is the maximum degree of priority within the hierarchy, urgency, or finality of the prototypical values of the disorder. The fact that they are maximum - as with the case group - means they become dominant in the life experience. Therefore, they generate fears, displeasure, and distress which are absent in the experiences of those who assign a lower priority to these values - as with the control group - thus affecting the general avoidance experience (Hayes, Wilson, Gilfford, Follette & Strosahl, 1996; Luciano & Hayes, 2001). These maximum degrees of priority in the hierarchy bear implications to realize the defusion processes in ACT. In cases where these are very strong, the clients tend to lose themselves in such assessments and, therefore, their selves experience difficulties to differentiate themselves and then distance themselves from them, and to delliterate (Dahl et al., 2005; Hayes et al., 2004; Wilson & Luciano, 2002).
The implications these findings have within ACT are that they allow us to conceive the prototypical values of avoidant personality disorder as global life directions which, at some point, were verbally chosen, desired, and built (Páez et al., 2006). They were attained through conduct, but this being an unfinished process, it is possible to think they can be reformulated and redirected by the person for a better quality of life (Wilson & Luciano, 2002; Dahl et al., 2005; Hayes et al., 2004). In this sense, it implies observing them as legitimate, given that - from the point of view of ACT - they are choices, not opinions given by someone deciding on the perfection or imperfection of such values (Hayes, 1993). For this reason, these values provide a starting point for the processes to clarify and specify them, prior to the client's reformulation.
Conclusions
We found that the individuals with avoidant personality disorder identify themselves with a characteristic repertoire of values typical of their emotional experience. These values proved to be predictors of the disorder and they responded to a maximum degree of priority in the evaluative hierarchy of aspects such as control, certitude, preparation, resolution, hope, confidence, confrontation, prediction, ability, and optimism which derive into confusion, fear of improvisation, apathy, helplessness, lack of control, escape, lack of confidence, uncertainty, self-inefficacy, and pessimism.
The findings obtained in the current study present some limitations regarding the amount of participants used. Another limitation regards the socio-economic strata and ages of the participant, which should be broadened to find out the responses obtained in older ages. Studies in other cultures are necessary to contrast these findings. Likewise, papers on associated personality disorders are also needed, like for example dependent personality disorder, in order to make divergent validations that show whether there exist overlapping values and thus obtain greater accuracy with respect to the prototypical values.
Among the study's implications is having a preliminary delimitation of the repertoire of prototypical values of avoidant personality disorder that may favor the channeling of clinical interventions focused on that disorder so as to facilitate defusion and delliteration processes in ACT as well as a specific working path for the client to recognize the values involved in their situation. On the other hand, the current study may open an exploration scenario for other clinicians and researchers interested in delving in the topic, as little empirical exploration exists on it.
References
Alden, L. (1989). Shortterm structured treatment for avoidant personality disorder. Journal of Consulting Clinical Psychology, , 75664.
Álvarez, L. (2014). Auto informe evocativo de valores típicos del trastorno de la personalidad por evitaciónUnpublished manuscript.
Anastasi, A. (1976). Psychological Testing. New York: Macmillan.
Bach, P. & Hayes, S.C. (2002). The use of acceptance and commitment therapy to prevent the rehospitalization of psychotic patients: A randomized controlled trial. Journal of Consulting and Clinical Psychology, , 1129-1139.
Baer, R.A., Fischer, S., & Huss, D.B. (2005). Mindfulness-based cognitive therapy applied to binge eating: A case study. Cognitive and Behavioral Practice, 12(3), 351.
Barnes-Holmes, D., Barnes-Holmes, Y., Hayes, S. C., & McHugh, L. (2004). Relational Frame Theory: Some Implications for Understanding and Treating Human Psychopathology. International Journal of Psychology and Psychological Therapy355-375.
Caballo, V.E. (1998). Tratamiento cognitivo-conductual de los trastornos de la personalidad. En Caballo, V. (Coord.), Manual para el tratamiento cognitivo-conductual de los trastornos psicológicos. Vol. II. Madrid: Siglo XXI.
Cardenal, V. & Sánchez, M.P. (2007). Adaptación y baremación al español del Inventario Clínico Multiaxial de Millon III (MCMI-III). Madrid: TEA, Ediciones.
Cardenal, V., Sánchez, M.P., & Ortiz-Tallo, M. (2007). Adaptación y baremación al español del Inventario Clínico Multiaxial de Millon III (MCMI-III)Madrid: TEA, Ediciones.
Dahl, J., Wilson, K.G., Luciano, C., & Hayes, S.C. (2005). Acceptance and Commitment Therapy for Chronic Pain. Reno, NV: Context Press.
DANE (2011). Infraestructura Colombiana de datos. Retrieved from http://190.25.231.246:8080/Dane/tree.jsf
Departamento Nacional de Planeación de Colombia (2005). Documento 3386 del Consejo Nacional de Política Económica y SocialRetrieved from: http://www.dnp.gov.co/PortalWeb/Portals/0/archivos/documentos/Subdireccion/Conpes/3386.pdf
Echeburúa, E. & Corral, P. (1999). Avances en el tratamiento cognitivo conductual de los trastornos de la personalidad. Análisis y Modificación de Conducta, , 585-614.
Eifert, G.H., & Forsyth, J.P. (2005). Acceptance and Commitment Therapy for anxiety disorders: A Practitioner's treatment guide to using mindfulness, acceptance, and values-based behavior change strategies. Oakland, CA: New Harbinger.
First, M. (2001). DSM-IV-TR: Manual de Diagnóstico y Estadístico de los Trastornos MentalesMasson.
First, M. (1999). SCID-II: entrevista clínica estructurada para los trastornos de la personalidad del eje II del DSM-IV. Guía del usuario. Entrevista clínica. Cuestionario de personalidad. Masson.
Fleiss, J.L. (1971). Measuring nominal scale agreement among many raters. Psychology Bulletin, : 378-382.
Frances, A., Pincus, H., & First, M. (2008). Manual diagnóstico y estadístico de los trastornos mentales(r). Madrid: Masson .
Gaudiano, B.A. & Herbert, J.D. (2006). Acute treatment of inpatients with psychotic symptoms using acceptance and commitment therapy: Pilot results. Behaviour Research and Therapy, , 415-437.
Gunderson, J. & Gabbard, G. (2000). Psychotherapy for Personality Disorders. Review of PsychiatryVol. 19. Washington, D. C.: American Psychiatric Press.
Gifford, E.V., Kohlenberg, B.S., Hayes, S.C., Antonuccio, D.O., Piasecki, M.M., Rasmussen Hall, M.L., & Palm, K.M. (2004). Acceptance theory-based treatment for smoking cessation: An initial trial of Acceptance and Commitment Therapy. Behavior Therapy, 689-705.
Hayes, S.C. (1993). Analytic goals and the varieties of scientific contextualism. In S. C. Hayes, L. J. Hayes, H. W. Reese, & T. R. Sarbin (Eds.), Varieties of scientific contextualism. Reno, NV: Context Press.
Hayes, S.C. & Brownstein, A.J. (1986). Mentalism, behavior-behavior relations, and a behavioranalytic view of the purposes of science. The Behavior Analyst(2), 175-190.
Hayes, S.C. & Strosahl, K.D. (Eds.). (2004). A practical guide to Acceptance and Commitment Therapy. New York: Springer-Verlag.
Hayes, S.C., Barnes-Holmes, D., & Roche, B. (Eds.). (2001). Relational Frame Theory: A Post-Skinnerian account of human language and cognition. New York: Plenum Press.
Hayes, S.C., Follette, V. M., & Linehan, M.M. (Eds.). (2004). Mindfulness and acceptance: Expanding the cognitive-behavioral tradition. New York: Guilford Press.
Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (1999). Acceptance and Commitment Therapy. An experiential approach to behavior change. New York: Guilford.
Hayes, S.C., Wilson, K.G., Gifford, E.V., Follete, V.M., & Strosahl, K. (1996). Experiential avoidance and behavior disorder: a functional dimensional approach to diagnoses and treatment., Journal of Consulting and Clinical Psychology , 1.152-1.168.
Hayes, S.C., Strosahl, K.D., Wilson, K.G., Bissett, R.T., Pistorello, J., Toarmino, D. & Mc Curry, S.M. (2004). Measuring experiential avoidance: A preliminary test of a working model. The Psychological Record, , 553-578.
Heffner, M., Sperry, J., Eiftert, G.H., & Detweiler, M. (2002). Acceptance and commitment therapy in the treatment of an adolescent female with anorexia nervosa: A case example., Cognitive and Behavioral Practice (3), 232-236.
Congreso de la República de Colombia. Ley 142 de 1994 Por la cual se establece el régimen de los servicios públicos domiciliarios y se dictan otras disposiciones. Retrieved from: https://comision6senado.files.wordpress.com/2013/03/ley-142-de-1994.pdf
Luciano, M.C., Rodríguez Valverde, M. & Gutiérrez Martínez, O. (2004). A proposal for synthesizing verbal contexts in Experiential Avoidance Disorder and Acceptance and Commitment Therapy. International Journal of Psychology and Psychological Therapy, 377-394.
Luciano, M.C. (2001) (Ed.) Terapia de Aceptación y Compromiso (ACT). Libro de casos. Valencia: Promolibro.
Luciano, M.C., Rodríguez, M., & Gutiérrez, O. (2004). A proposal for synthesizing verbal contexts in Experiential Avoidance Disorder and Acceptance and Commitment Therapy., International Journal of Psychology and Psychological Therapy , 377-394.
Luciano, M.C. & Hayes, S.C. (2001). Trastorno de evitación experiencial. Revista Internacional de Psicología Clínica y de la Salud, , 109-157.
Magnusson, D. (1982). Teoría de los tests. México: Trillas
Millon, T. & Everly, G. (1994). La personalidad y sus trastornos. Barcelona: Martínez Roca.
Millon, T. & Davis, R. (1998). Trastornos de personalidad. Más allá del DSM-IV. Barcelona: Masson.
Millon, T. & Everly, G.S. (1994). La personalidad y sus trastornos Barcelona: Martínez Roca.
Montesinos, F. (2003). ACT, Orientación del Deseo Sexual y Trastornos de la Erección. Un Estudio de Caso. Análisis y Modificación de Conducta291-320.
Paéz, M., Gutiérrez, O., Valdivia, S., & Luciano, C. (2006). Terapia de Aceptación y Compromiso (ACT) y la importancia de los valores personales en el contexto de la terapia psicológica. International Journal of Psychology and Psychological Therapy(1), 1-20.
Pérez Álvarez, M. (1996). Tratamientos psicológicos. Madrid: Universitas.
Pérez Álvarez, M. (2001). Afinidades entre las nuevas terapias de conducta y las terapias tradicionales con otras orientaciones., Revista Internacional de Psicología Clínica y de la Salud , 15-33.
Perry, J., Banon, E., & Ianni, F. (1999). Effectiveness of psychotherapy for personality disorders. American-Journal-of-Psychiatry, (9), 1.312-1.321.
Perry, J.C. & Bond, M. (2000). Empirical studies of psychotherapy for personality disorders. In J.G. Gunderson & G.O. Gabbard (Coords.), Psychotherapy of personality disorders. Washington, DC: American Psychiatric Press.
Quiroga, E. & Errasti, J. M. (2001). Tratamientos psicológicos eficaces para los trastornos de personalidad. Psicothema, , 393-406.
Renneberg, B., Goldstein, A.J., Phillips, D., & Chambless, D. (1990). Intensive behavioral group treatment of avoidant personality disorder., Behavior Therapy (3), 363-377.
Robin, M.W. & Di Giuseppe, R. (1993). Rational-emotive therapy with an avoidant personality. In K.T. Kuehlwein, & H. Rosen, Cognitive therapies in action: Evolving innovative practice (pp. 143-159). San Francisco, CA: Jossey-Bass Inc, Publishers.
Roca, M. & Bernardo, M. (1998). Epidemiología. In Bernardo, M. & Roca, M. (Coords.), Trastornos de la personalidad: Evaluación y Tratamiento. Perspectiva psicobiológica (pp. 1-17). Barcelona: Masson.
Sanislow, C.A. & McGlashan, T.H. (1998). Treatment outcome of personality disorders. Canadian Journal of Psychiatry, (3), 237-250.
Shedler, J., Maymann, M., & Manis, M. (1993). The illusion of mental health. American Psychologist(11), 1117-1131.
Stravynski, A., Belisle, M., Marcouiller, M., Lavallee, Y., & Elie, R. (1994). The treatment of avoidant personality disorder by social skills training in the clinic or in real-life setting., Canadian Journal of Psychiatry (8), 377-383.
Stravynski, A., Grey, S., & Elie, R. (1987). An outline of the therapeutic process in social skills training with socially dysfunctional patients., Journal of Consulting Clinical Psychology , 224-228.
Stravynski, A., Marks, I. & Yule, W. (1982). Social skills problems in neurotic outpatients: social skills training with and without cognitive modification. Archives of General Psychiatry, , 1378-1385.
Twohig, M.P., Shoenberger, D., & Hayes, S.C. (2007) A Preliminary Investigation of Acceptance and Commitment Therapy as a Treatment for Marijuana Dependence in Adults. Journal of Applied Behavior Analysis, , 619-632.
Weltzler, S. (1990). The Millon Clinical Multiaxial Inventory (MCMI): A review. Journal of Personality Assessment445-464.
Whelan, R. & Barnes-Holmes, D. (2004). The transformation of consequential functions in accordance with the relational frames of same and opposite. Journal of the Experimental Analysis of Behavior, 177-195.
Wilson, K.G. & Luciano, M.C. (2002). Terapia de Aceptación y Compromiso (ACT). Un tratamiento conductual orientado a los valores. Madrid: Pirámide.
Wilson, K.G., & Byrd, M.R. (2004). Acceptance and Commitment Therapy for Substance Abuse and Dependence. In S. C. Hayes & K. Strosahl (Eds.). A Practical Guide to Acceptance and Commitment Therapy (pp. 153-184). New York: Springer Press.