Original Article
Received: 27 December 2021
Accepted: 06 June 2022
DOI: https://doi.org/10.17533/udea.iee.v40n3e03
Abstract
Objective. : To assess the effectiveness of a brief intervention and motivational interviewing in reducing the use of different tobacco-related products in adults
Methods.: For this systematic review, PubMed, Web of Science, and PsychINFO databases were electronically searched for randomized controlled trials on the effect of a brief intervention and / or motivational interview on tobacco reduction among healthy adults published between January 1, 2011 to January 1, 2021. Data from eligible studies were extracted and analyzed. CONSORT guidelines were used to assess the quality of the studies by two reviewers for the included studies. The titles and abstracts of the search results were screened and reviewed by two independent reviewers for eligibility criteria per the inclusion and exclusion criteria. Cochrane review criteria were used to assess the risk of bias in included studies.
Results.: A total of 12 studies were included in the final data extraction of 1406 studies. The brief intervention and motivational interviewing showed varied effects on tobacco use reduction among adults at different follow-ups. Seven of the 12 studies (58.3%) reported a beneficial impact on reducing tobacco use. Pieces of evidence on biochemical estimation on tobacco reduction are limited compared to self-reports, and varied results on quitting and tobacco cessation with different follow-ups.
Conclusion. : The current evidence supports the effectiveness of a brief intervention and motivational interviewing to quit tobacco use. Still, it suggests using more biochemical markers as outcome measures to reach an intervention-specific decision. While more initiatives to train nurses in providing non-pharmacological nursing interventions, including brief interventions, are recommended to help people quit smoking.
Descriptors: Motivational interviewing, tobacco use cessation, tobacco use, adult.
Resumen
Objetivo. : Evaluar la eficacia de una intervención breve y de la entrevista motivacional para reducir el consumo de diferentes productos relacionados con el tabaco en adultos.
Métodos. : Para esta revisión sistemática, se buscaron en las bases de datos PubMed, Web of Science y PsychINFO ensayos controlados aleatorizados sobre el efecto de una intervención breve y/o una entrevista motivacional en la reducción del consumo de tabaco entre adultos sanos, que hubieran sido publicados entre el 1 de enero de 2011 y el 1 de enero de 2021. Los títulos y los resúmenes de los artículos incluidos fueron evaluados por dos revisores independientes para determinar los criterios de elegibilidad, se analizó la calidad de los estudios con la guía CONSORT y se utilizaron los criterios de Cochrane para evaluar el riesgo de sesgo.
Resultados. : Se incluyeron un total de 12 de los 1406 estudios que arrojó la búsqueda. La intervención breve y la entrevista motivacional mostraron efectos variados en la reducción del consumo de tabaco entre los adultos en diferentes seguimientos. Siete de los 12 estudios (58.3%) informaron de un impacto beneficioso en la reducción del consumo de tabaco. La utilización de indicadores bioquímicos de la reducción del consumo de tabaco fueron limitados en comparación con los autoinformes. Los resultados sobre el abandono y la cesación del tabaco fueron variados con diferentes seguimientos.
Conclusión. : La evidencia apoyó la efectividad de una intervención breve y de la entrevista motivacional para la cesación del consumo de tabaco. Sin embargo, se sugiere realizar más estudios con marcadores bioquímicos como medidas de resultado para llegar a una decisión específica de la intervención. Se recomienda formar a los enfermeros en la realización de intervenciones de enfermería no farmacológicas, incluidas las intervenciones breves, para ayudar a las personas a dejar de fumar.
Descriptores: Entrevista motivacional, cese del uso de tabaco, uso de tabaco, adulto.
Resumo
Objetivo: . Avaliar a eficácia de uma intervenção breve e entrevista motivacional na redução do uso de diferentes produtos relacionados ao tabaco em adultos.
Métodos: . Para esta revisão sistemática, se buscou nas bases de PubMed, Web of Science e PsychINFO ensaios controlados aleatórios sobre o efeito de uma breve intervenção e/ou entrevista motivacional na redução do uso de tabaco entre adultos saudáveis, publicados entre 1º de janeiro de 2011 e 1º de janeiro de 2021. Os títulos e resumos dos artigos incluídos foram avaliados por dois revisores independentes para critérios de elegibilidade, a qualidade do estudo foi avaliada usando a diretriz CONSORT e os critérios Cochrane foram usados para avaliar o risco de viés.
Resultados: . Um total de 12 dos 1.406 estudos retornados pela busca foram incluídos. Intervenção breve e entrevista motivacional mostraram efeitos mistos na redução do uso de tabaco entre adultos em diferentes acompanhamentos. Sete dos 12 estudos (58.3%) relataram um impacto benéfico na redução do uso de tabaco. O uso de indicadores bioquímicos de redução do uso de tabaco foi limitado em relação ao autorrelato. Os resultados sobre parar de fumar e parar de fumar foram variados com diferentes seguimentos.
Conclusão: . As evidências apoiaram a eficácia de uma intervenção breve e entrevista motivacional para a cessação do uso do tabaco. No entanto, mais estudos com marcadores bioquímicos como medidas de resultados são sugeridos para chegar a uma decisão de intervenção específica. Recomenda-se que os enfermeiros sejam treinados na execução de intervenções de enfermagem não farmacológicas, incluindo intervenções breves, para ajudar as pessoas a parar de fumar.
Descritores: Entrevista motivacional, abandono do uso de tabaco, uso de tabaco, adulto.
Introduction
Tobacco in any form is harmful and affects millions of lives every year.1 In 2017, 8 million lives were lost due to smoking-related diseases.2 Tobacco-related deaths are rising even after a decline in tobacco use trends because of the chronic nature of conditions.3 In 2000, around 33.3% of the global population over 15 years old were current tobacco users.3 The negative consequences of tobacco use are well known and extend beyond individuals and countries regarding increasing health care expenditure and loss of productive life.4 The tobacco consumption trend was three times higher in males than females in 2000, which was increased to four times in 2015 and is projected to be five times by 2025.1,3 Notably, the detrimental effects of tobacco use gravely affected lower socio-economic populations with higher smoking prevalence.5 However, tobacco use practices are varied and influenced by the locally available tobacco products in the different regions worldwide.6
Smoking is one of the modifiable risk factors for many life-threatening health problems, including respiratory and cardiovascular health and genitourinary problems.7 It has been estimated that 50% of smokers who start smoking in adolescence die due to tobacco-related health problems.8 Thus, an effective measure to control tobacco addiction is paramount. Implementing a wide range of interventions and strengthening tobacco control policy, including taxation, ban on tobacco use in public places, restriction on advertising of tobacco products, and creating smoke-free zones in educational institutions, brought a substantial decline in tobacco use in recent decades.4 In addition to government initiatives to curb tobacco use, many pharmacological and non-pharmacological approaches are also involved in reducing tobacco-associated mortality and the burden of diseases.6,9 Earlier studies reported that using a combination of pharmacologic and non-pharmacologic intervention is highly effective in reducing tobacco use. 10-12 However, non-pharmacological interventions have advantages over pharmacological interventions, including no side effects, long-term behavior changes,13 knowing the real health hazards of long-term tobacco use, and cost-effective to show higher compliance.11,12,14
Non-pharmacologic interventions for tobacco cessation include telephone counseling, individual and group counseling, health care provider interventions, exercise programs, and self-help programs.12 Brief intervention or motivational interview is a brief yet realistic strategy offered to those who have a low motivation to quit.15 Brief intervention is goal-directed but non-directive communication designed to improve motivation for change in quit behavior by eliciting feedback to plan for change.12,16-20 The terms brief intervention (BI) and motivational interview (MI) are used with a common principle of active engagement of the client in the process of reduced use and teaching alternative coping skills.21 These interventions are based on the philosophy that the client holds a key role in showing commitment and successful recovery.22 Brief intervention sometimes follows the principles of the motivational interview to motivate the specific behavior of an individual to reduce or quit substance use.23
However, these interventions are substantially modified in the delivery approach, format, and content in earlier published work.12 Brief intervention primarily focuses on present concerns and stressors rather than exploring the historical antecedents of an individual and is conducted by a trained therapist.20,24 Earlier work on the efficacy of brief intervention reported evidence that brief intervention increases the motivation to quit short-term use.18,25 However, the evidence on long-term effects of brief interventions is equivocal, with no reduction of tobacco use at three months while higher self-reported abstinence at 1-year post-brief intervention.26 Conversely, the brief intervention was found to be effective in improving quit rates, prolonging abstinence, and improving self-reported continuous abstinence among smokers at six months27 and 1-year post-intervention28 in other work. Still, there is a lack of consistent evidence on brief interventions to reduce use or quit tobacco use among the adult population.
Nurses are an essential attribute of the health care system and play a vital role in delivering various interventions. It is natural to expect that nurses with adequate knowledge and skills in the brief intervention will do more to help their patients quit smoking. This meta-analysis will highlight the need for encouragement and opportunities to nurses to receive training on smoking cessation interventions. In addition, this will be insightful for the nurses to understand the significance of a non-pharmacological intervention to quit smoking. Towards this end, training nurses in the brief intervention using motivational interviews may be helpful to smokers and their families. Consequently, this systematic review aims to assess the effectiveness of the brief intervention in reducing tobacco use among adults.
Methods
A literature review was conducted with online databases PubMed, Web of Science, and PsychINFO. A literature search was completed using Boolean operators and truncations for the following key terms: (1) "Brief Intervention, (2) OR Screening and Brief Intervention” "tobacco products” AND (3) “Tobacco OR "tobacco products,” (MESH terms are also included in the search). The problem/disease was tobacco use among adults in the experimental group. The primary outcomes of interest were cessation in tobacco use, motivation/readiness to quit, reduction in tobacco quantity, days, abstinence days, quit attempts, and point prevalence measured by self-reported methods or biochemical verification at different intervals.
Selection criteria and data extraction. The inclusion criteria for the studies included in this review were as follows: (1) the content of the article mainly focused on the provision of brief intervention and/or motivational interview for tobacco use reduction or cessation; (2) the participants were current smokers and adults; (3) the articles were published in peer-reviewed journals within the last ten years; (4) the study method reflected a randomized control trial (RCT). Articles were excluded if they focused primarily on other pharmacologic interventions, included any other substance use, were not designed as an RCT, or had mixed interventions. The search strategy was based on the population, intervention, control, and outcomes (PICO) approach with a PICO question, ‘does motivational interviewing and brief interventions helpful in reducing tobacco use in healthy adults?’; where P- Healthy tobacco users, I- Motivational Interview and/or Brief Intervention, C- Usual care or on other interventions and O- Smoking cessation.29 A total of 1406 articles were included for a title and abstract review; at least two team members discussed discrepancies. 77 articles met the inclusion criteria for a full-text review, and 12 articles were selected for data extraction. See the PRISMA framework (Figure 1) that guided the review process.30
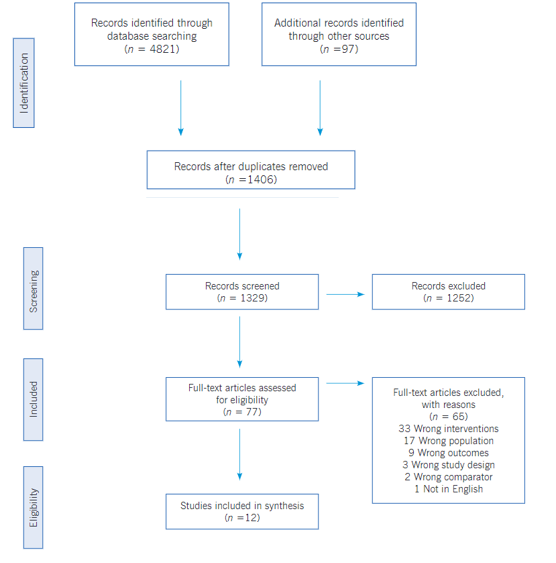
Figure 1
PRISMA Flow Diagram
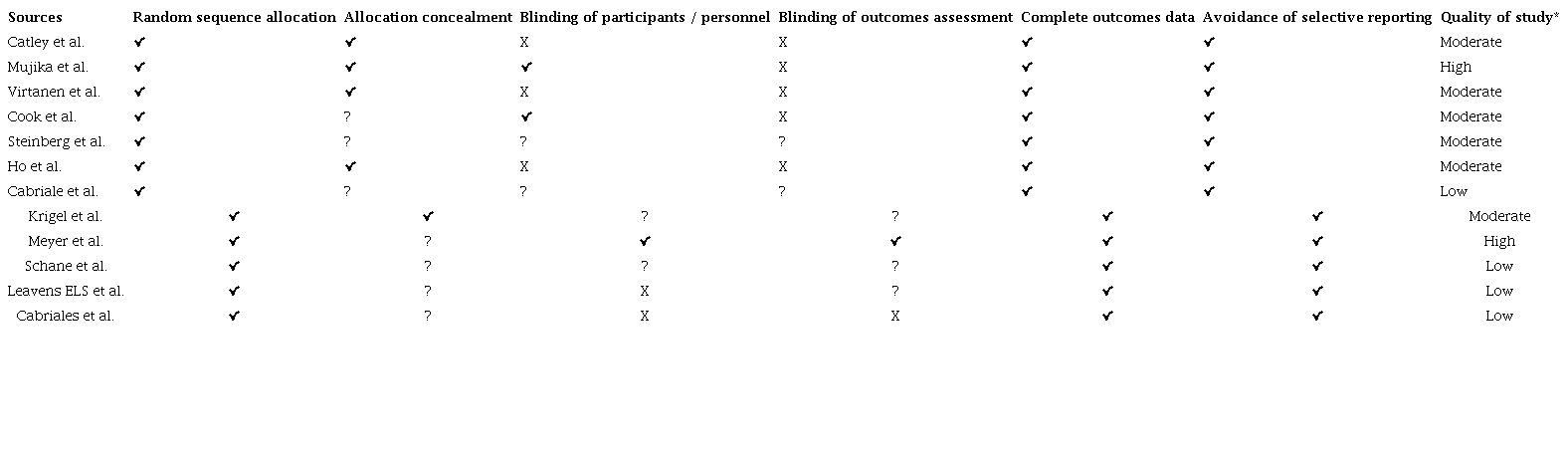
Bias assessment. Cochrane review criteria were used to assess the risk of bias in included studies in the review (Table 1).31 All studies were evaluated on six evidence-based domains: allocation concealment, random sequence generation, participants and personnel blinding, outcome blinding, incomplete outcome data, and selective reporting.31 Allocation concealment refers to concealing the information on the randomization process to the subjects. Random sequence generation occurs when study participants are not aware of the random sequence generation process. Blinding of participants and personnel refers to when participants and team members do not know the intervention or control condition to which subjects are assigned. Blinding of outcomes assessment refers to whether outcome measurement could have been changed by prior intervention knowledge to participants or team members delivered in work. Selective reporting refers to presenting only findings of interest. An incomplete outcome does not consider attrition while submitting the result.31 For each study, these components are shown in ‘high risk,’ ‘low risk,’ or ‘unclear’ as written in the published version of the manuscript to decide on bias assessment. In data extraction, two authors assessed each study for bias. The authors discuss the risk bias criteria of the study using a checklist and conclude. The discrepancies were resolved after a discussion with the third author Table 1.
Quality assessment of the included studies
Results
The electronic search produced a total of 3162 articles. 1406 articles were found suitable after removing duplicate records. Abstracts of all articles were reviewed independently by two reviewers. A total of 1262 articles were excluded after careful scrutiny of abstracts. Full-text articles were retrieved for 79, and after reviewing these articles independently, 67 articles were further excluded for a specific reason. After applying the eligibility criteria, 12 articles were included in the present review. The PRISMA flow diagram (Figure 1) summarizes the study selection and scrutiny process used for the articles. A summary of the selected studies summarized by year of publication, author, setting, type of study, sampling techniques, sample size, eligibility criteria (inclusion and exclusion), intervention, outcomes, strengths and limitations, and any other specific notes to the study.
Study characteristics. Of the 12 included studies, eight were conducted in the United States, one in Sweden, one in Hong Kong, one in Germany, and one in Spain. All studies used a randomized controlled trials design with one or another trial feature, including allocation concealment and blinding. Of the 12 studies, 3 studies used brief intervention or brief advise,30,32,35,38,41 6 studies used motivational interviews 15,30,33,34,37,40, and one study used brief counseling on harm to self and harm to others 39 and quit immediately award model based on brief intervention approach. Seven of the 12 studies (58.3%) reported a beneficial effect of brief advice or motivational interview on reducing tobacco use (Table 2).
Motivational Interviewing (MI). The concept and use of motivational interviewing as an intervention is not new in substance use,42 smoking reduction,43 chronic lifestyle disease,44 health behavior,45 medication adherence,46,47 oral health in adolescents,48 and chronic pain management.49 The concept was published by Miller & Rollnick and presented as a therapeutic effort to strengthen personal motivation and commitment to a specific goal by eliciting and exploring the individual’s reason for a change in behavior with compassion and acceptance.16
Motivational interviewing (MI) is a patient-centered, directive therapeutic style to improve readiness to change behavior by resolving the ambivalence.43 MI was found to be an effective method in a series of addictive behaviors.50 Some research33 among healthy adult smokers tested multiple interventions revealed a promising effect of motivational interviewing on smoking reduction. However, the study concluded50 that motivational interviewing and other interventions will produce the most consistent and marked reduction in smoking. A contrasting study15 used motivational interviewing over health education and brief advice but did not report any change in quit attempts at 6 months. However, the same study reported increased cessation of medication use, motivation, and confidence to quit compared to brief advice, which further indicates the effectiveness of MI in behavior changes to quit smoking. In a study34 at a Northeastern US State, daily smokers attended brief motivational interviewing and significantly reduced cigarette use. Likewise, motivational interviewing effectively improved quitting smoking among nurses over brief advice in a study conducted in Spain.30 However, in another work37 on college tobacco smokers, the use of motivational interviewing over health education (HE) showed no significant reduction in motivation to quit, abstinence, and quit attempts. Likewise, the consistent findings are presented in earlier studies15,51 that reported no significant advantage of MI on smoking cessation compared to alternative interventions. In a recent work conducted in the Midwest United States, a brief motivational interview showed no improvement in reducing water pipe use40; however, MI was found to improve awareness of risk perceptions, commitment, and confidence to quit waterpipe (WP) smoking.
Furthermore, in a recent meta-analysis, MI reported a modest yet significant beneficial increase in quitting rates in a group that utilized motivational interviewing. Further, findings revealed that long-term motivational interviewing by a primary physician or counselor is more effective in quitting tobacco. However, there is no specific evidence on the duration and number of MI sessions on quitting the behavior. Another meta-analysis52 reported a greater likelihood of abstinence behavior in the experimental arm comprising adults and adolescents when compared to the comparison group. Still, only a few older interventions and meta-analyses demonstrate the effectiveness of motivational interviewing in smoking cessation. There is evidence that motivational interviewing is less effective in low-motivation patients.18,53 However, the conclusive evidence to prove the quality and fidelity of MI implementation remains contentious concerning its effectiveness in smoking reduction.
Brief Intervention. Brief intervention or advice for harmful substance use has been practiced for many years. 54 It aims to identify the current and potential problems with substance use and motivate people to change high-risk behavior.55 Brief intervention is a personalized, supportive and non-judgmental approach to treatment.55 It is also defined as a verbal ‘stop smoking’ message loaded with harmful effects of tobacco use.56 Brief intervention can be used in various methodologies, including unstructured counseling and feedback to formal structured treatment.57-59 World Health Organization uses education, simple advice, and brief counseling as alternative types of brief interventions for high-risk individuals with alcohol use disorders.60 Brief intervention also uses screening and referral services and is therefore called screening, brief intervention, and referral to treatment (SBIRT).61 Brief therapy can help motivate an individual to change his high-risk behavior at a different stage of behavior change.62 The stage of change model proposed by Prochaska & DiClemente, helps clinicians tailor a brief intervention to the stage of behavior change and the client's needs.63
Brief interventions for tobacco use disorders aim to enhance motivation for change and provide evidence-based resources to reduce usage or complete cessation of tobacco products. The 5A’s approach (Ask, Advise, Assess, Assist, & Arrange) is an evidence-based approach that helps tobacco users in different settings with motivational strategies in a systematic fashion.64 In addition, FLAGS-Feedback, Listen, Advice, Goals, Strategies and ‘FRAMES’-Feedback, Responsibility, Advice, Menu of options, Empathy, and Self-efficacy, are other frameworks used to deliver brief interventions.65
The brief intervention is effective in many ways, including cost-effectiveness in terms of time and money,66 increased abstinence rate and days,35,67 and early days of discharge, and regular follow-ups 68. Similarly, a more intensive planned brief advice (>20 minutes) may augment the effect on quit rate and 6-months abstinence compared to minimal brief advice.69 Additionally, the use of brief components in AWARD [Ask, Warn, Advice, Refer, Do-It Again) model, and cut down to quit: [CDTQ]), reported a higher quit rate in the former group. 35 Furthermore, brief advice in combination with tailored practice was highly effective on 7-days point prevalence and 7-days and 6-months abstinence rate among adult smokers. 38 Brief counseling also reported a significant reduction in quit rate, abstinence phenomenon, improved motivation, and self-efficacy in a regular follow-up in a group of nondaily smokers.36,39 Conversely, brief therapy showed no significant changes in abstinence rate among adults who underwent immediate and delayed intervention at the family health clinic U.S.-Mexico border,41 and hence, the efficacy of brief therapy has been questioned in recent years.70
Further, brief treatment can be helpful for varied kinds of the population, including adolescents, older smokers, smokers with mental illness and co-morbidities, alcohol users, and pregnant women across different racial and ethnic groups.66,70 However, current or former tobacco smokers who were willing or unwilling to make quit attempts are the most eligible groups to attend the brief intervention.66
Discussion
The use of tobacco has innumerable adverse effects on health. The present review aimed to assess the effectiveness of a brief intervention in reducing tobacco use among adults. The review findings indicate that brief intervention alone or combined with Motivational Interviews or Health Education was effective, supported by previous results.15,52 In contrast, an earlier systematic review documented that motivational interviewing was modestly successful in promoting smoking cessation compared with usual care or brief advice.25 Conversely, motivation to quit was higher after Brief Advice than MI.71 Another recent systematic review conducted with 37 studies reported insufficient evidence to show whether MI helps people stop smoking compared with no intervention, as an addition to other types of behavioral support, or compared with different kinds of behavioral support for smoking cessation.72
Modality and intensity of interventions with follow-up and primary outcomes were also determining factors for the effectiveness of the studies. In the current review, the intervention modality varied in face‐to‐face sessions or a combination of face‐to‐face and telephone sessions. Initial sessions were conducted face-to-face, and the follow-up was done over the telephone for most of the study, which is usual with much other previous work.72 Brief intervention provided through telephone has great significance in the present scenario. Amid the COVID-19 pandemic, when individuals have restricted movement or limited resources available, virtual or phone delivered brief intervention can play a significant role in helping the adults quit smoking or reduce tobacco use. A previous study has documented moderate‐certainty evidence of proactive telephone counseling in increasing the quit rates in smokers who seek help from quitlines.73
The included studies had intervention sessions as little as one brief session37 to four sessions based on Motivational Interviews. 30 Prior literature suggests that multiple sessions might increase the likelihood of quitting over single-session treatment, but positive outcomes were reported in both cases.25 However, there is no specific evidence on the duration and number of MI sessions on quitting the behavior.72The current review found that the included studies had a follow-up of the intervention ranging from 3 months to 12 months. However, face-to-face or telephone counseling follow-up did not show a significant effect of an intervention. However, reduction of smoking behavior or abstinence was not sustained over time. These findings were supported by a previous work where smoking abstinence averaged 10% at 1 month and around 2% at 3, 6, and 12 months.71 At present, evidence is unclear on the optimal number of follow-up calls.25,43
The primary outcomes of the studies were smoking abstinence, reduction in smoking rates, and an increase in motivation to quit. However, outcomes other than cessation may be essential to assess when determining the effects of brief interventions for tobacco use. Hence, different outcomes were self-efficacy, motivation, and changes in depression over the studies. Biological tests to confirm tobacco abstinence provided more reliable findings than self-reported abstinence.
Intervention programs on Smoking cessation, such as brief advice, motivational interviews, or the 5A approach (Ask, Advise, Assess, Assist, and Arrange), are effective among specific populations or specialized clinical settings.45,74 Professional support and cessation interventions or medications significantly increase the chance of successfully quitting.3 A systematic review and meta-synthesis explored smokers' perspectives regarding smoking cessation and reported that lack of motivation to quit was one of the significant issues they felt for tobacco cessation.75 Nonetheless, these non-pharmacological interventions had shown efficacy similar to the pharmacological intervention74 with additional benefits of cost-effectiveness, competency of the provider, and accessibility to the treatment center.
Tobacco-related deaths and disabilities are increasing around the globe because of the continued use of different kinds of tobacco products. Many earlier studies confirmed the beneficial effect of a brief intervention based on motivational principles to reduce tobacco use. Nurses' role is precise in tobacco cessation to endorse the International Council of Nurses statement to integrate tobacco use prevention and cessation as part of their regular nursing practice.76 This systematic review indicates the potential benefits of brief intervention, which can be a breakthrough for nurses in tobacco reduction around the globe. However, nursing policymakers should incorporate smoking cessation interventions as a part of standard practice for all the patients. Hence, brief intervention or motivational interviews provide promising results in cessation or reduction of tobacco use which needs to be further supported by evidence.
The present review should be appraised under its many limitations and strengths. Among its strengths is that it provides coverage of randomized controlled trials that included brief intervention and motivational interviewing on smoking and other tobacco use among adults. This review included samples of those with clinical and non-clinical samples using tobacco. The major strength of this review lies in the inclusion of RCT studies that give a clear description of participants' characteristics, methodology, and implemented intervention. Secondly, the risk of bias assessment showed that most studies had low to moderate risk. This review highlights several opportunities for future research, such as brief intervention or motivational interview combined with other adjuncts to improve outcomes and further research integration of these interventions with combination therapies of psychotherapeutic and pharmacological interventions.
In terms of limitations, the heterogenicity of the selected studies did not allow to reach a specific conclusion. Studies included in this review used different brief intervention and motivational interview forms, making it challenging to synthesize the results and suggest a potential use of these interventions in day-to-day practice. Heterogeneity in population also made it challenging to generalize the findings across all people around the globe. Further, studies involved in the review only investigated tobacco cessation among healthy adults may confer unique limitations on the generalizability of results. The authors suggest interpreting and using review findings cautiously due to variations in treatment fidelity and the inclusion of a limited number of studies.
Conclusion.
Over time there have been changes in treatment modalities for tobacco cessation. Preference for non-pharmacological intervention over pharmacological has led the researchers to find supportive evidence. The present review highlights the effectiveness of a brief intervention and motivational interviewing in reducing tobacco use among adults. It also demonstrates that the effects are far-reaching. However, it remains inconclusive which intervention is more effective than the other. Future longitudinal studies or RCTs with direct comparison of different interventions may further refine the evidence-based practice on tobacco cessation among adults.
Characteristics of included studies in the review

References
World Health Organization. WHO Global Report: Mortality Attributable to Tobacco [Internet]. Who Global Report. Geneva: WHO; 2012 [cited 2021 Jun 29]. p. 392. Available from: Available from: http://www.who.int/tobacco/publications/surveillance/fact_sheet_mortality_report.pdf
WHO. Who Report on the Global Tobacco Epidemic, 2013 [Internet]. Vol. 23, ASHE-ERIC Higher Education Report. Geneva: WHO ; 1994. p. iii-vii. Available from: http://www.who.int/tobacco/global_report/2013/en/index.html%5Cnhttp://doi.wiley.com/10.1002/aehe.3640230702
World Health Organization (WHO). WHO global report on trends in prevalence of tobacco use 2000-2025 [Internet]. Third. WHO, editor. World Health Organization. Geneva: WHO : World Health Organization; 2019. Available from: https://www.who.int/publications/i/item/who-global-report-on-trends-in-prevalence-of-tobacco-use-2000-2025-third-edition
GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet: (London, England). 2017; 389(10082):1885-906.
Parsons VL, Moriarity C, Jonas K, Moore TF, Davis KE, Tompkins L. Design and estimation for the national health interview survey, 2006-2015. Vital Health Stat 2. 2014; (165):1-53.
Haokip HR, Kumar DR, Singh Rawat DV, Kumar Sharma DS. Efficacy of standard nicotine replacement therapy (NRT) versus video-assisted nurse-led NRT on tobacco cessation: A randomized controlled pilot trial. Clin. Epidemiol. Glob. Health. 2021; 9:141-6.
Fagerström K. The epidemiology of smoking: health consequences and benefits of cessation. Drugs. 2002; 62 Suppl 2:1-9.
Organization WH. Tobacco Fact Sheet No.339. World Health Organization [Internet]. 2013 [cited 2021 May 14]. Available from: Available from: https://www.drugsandalcohol.ie/17528/
Hatsukami D, Jensen J, Allen S, Grillo M, Bliss R. Effects of behavioral and pharmacological treatment on smokeless tobacco users. J. Consult. Clin. Psychol. 1996; 64(1):153-61.
Giulietti F, Filipponi A, Rosettani G, Giordano P, Iacoacci C, Spannella F, et al. Pharmacological Approach to Smoking Cessation: An Updated Review for Daily Clinical Practice. High blood Press. Cardiovasc. Prev. 2020; 27(5):349-62.
Cornuz J, Willi C. Nonpharmacological smoking cessation interventions in clinical practice. Eur. Respir. Rev. 2008; 17(110):187-91.
Niaura R. Nonpharmacologic therapy for smoking cessation: characteristics and efficacy of current approaches. Am. J. Med. 2008; 121(4 Suppl 1):S11-9.
Laland KN R. Social Learning: Theory. In: Choe JC Editors. Encyclopedia of Animal Behavior [Internet]. 2nd Ed. 2010 [cited 31 May 2022]. p. 380-6 p. Available from: Available from: https://doi.org/10.1016/B978-0-12-813251-7.00057-2
Cornuz J, Gilbert A, Pinget C, McDonald P, Slama K, Salto E, et al. Cost-effectiveness of pharmacotherapies for nicotine dependence in primary care settings: a multinational comparison. Tob. Control. 2006; 15(3):152-9.
Catley D, Goggin K, Harris KJ, Richter KP, Williams K, Patten C, et al. A randomized trial of motivational interviewing: Cessation induction among smokers with low desire to quit. Am. J. Prev. Med. 2016; 50(5):573-83.
Miller WR RS. Motivational Interviewing: Helping People Change. 3rd ed. New York, NY, US: Guilford Press; 2013.
Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst. Rev. 2017; 3(3):CD001292.
Hettema JE, Hendricks PS. Motivational interviewing for smoking cessation: a meta-analytic review. J. Consult. Clin. Psychol. 2010; 78(6):868-84.
Rice VH, Heath L, Livingstone-Banks J, Hartmann-Boyce J. Nursing interventions for smoking cessation. Cochrane Database Syst. Rev. 2017; 12(12):CD001188.
World Health Organization (WHO). The ASSIST-linked brief intervention for hazardous and harmful substance use. Manual for use in primary care [Internet]. 2012 [cited 2021 Jul 2]. Available from: Available from: https://www.who.int/publications/i/item/the-assist-linked-brief-intervention-for-hazardous-and-harmful-substance-use
Heather N ST. The essential and book of treatment and prevention of alcohol patients. London: John Wiley & Sons Ltd.; 2004.
Huffstetler AN. Brief Interventions and Motivational Interviewing [Internet]. 2021 [cited 2022 May 31]. Available from: Available from: https://www.dynamed.com/evaluation/brief-interventions-and-motivational-interviewing/about
Tucker JS, D’Amico EJ, Ewing BA, Miles JN V, Pedersen ER. A group-based motivational interviewing brief intervention to reduce substance use and sexual risk behavior among homeless young adults. J. Subst. Abuse Treat. 2017; 76:20-7.
Center for Substance Abuse Treatment. Brief Interventions and Brief Therapies for Substance Abuse. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 1999. Report No. 99-3353.
Lai DT, Cahill K, Qin Y, Tang JL. Motivational interviewing for smoking cessation. Cochrane Database Syst. Rev. 2010; (1):CD006936.
Colby SM, Nargiso J, Tevyaw TO, Barnett NP, Metrik J, Lewander W, et al. Enhanced motivational interviewing versus brief advice for adolescent smoking cessation: results from a randomized clinical trial. Addict. Behav. 2012; 37(7):817-23.
Cabezas C, Advani M, Puente D, Rodriguez-Blanco T, Martin C. Effectiveness of a stepped primary care smoking cessation intervention: Cluster randomized clinical trial (ISTAPS study). Addiction. 2011; 106(9):1696-706.
Lindqvist H, Forsberg LG, Forsberg L, Rosendahl I, Enebrink P, Helgason AR. Motivational interviewing in an ordinary clinical setting: a controlled clinical trial at the Swedish National Tobacco Quitline. Addict. Behav. 2013; 38(7):2321-4.
Eriksen MB, Frandsen TF. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J. Med. Libr. Assoc. 2018; 106(4):420-31.
Mujika A, Forbes A, Canga N, de Irala J, Serrano I, Gascó P, et al. Motivational interviewing as a smoking cessation strategy with nurses: an exploratory randomised controlled trial. Int. J. Nurs. Stud. 2014; 51(8):1074-82.
The Cochrane Collaboration. Cochrane Risk of Bias Tools for Randomized Trials [Internet]. 2011 [cited 2022 May 25]. Available from: Available from: https://methods.cochrane.org/bias/resources/cochrane-risk-bias-tool
Virtanen SE, Zeebari Z, Rohyo I, Galanti MR. Evaluation of a brief counseling for tobacco cessation in dental clinics among Swedish smokers and snus users. A cluster randomized controlled trial (the FRITT study). Prev. Med. (Baltim). 2015; 70:26-32.
Cook JW, Collins LM, Fiore MC, Smith SS, Fraser D, Bolt DM, et al. Comparative effectiveness of motivation phase intervention components for use with smokers unwilling to quit: a factorial screening experiment. Addiction. 2016; 111(1):117-28.
Steinberg ML, Rosen RL, Versella M V, Borges A, Leyro TM. A Pilot Randomized Clinical Trial of Brief Interventions to Encourage Quit Attempts in Smokers from Socioeconomic Disadvantage. Nicotine Tob. Res. 2020; 22(9):1500-8.
Ho KY, Li WHC, Wang MP, Lam KKW, Lam TH, Chan SSC. Comparison of two approaches in achieving smoking abstinence among patients in an outpatient clinic: A Phase 2 randomized controlled trial. Patient Educ. Couns. 2018; 101(5):885-93.
Cabriales JA, Suro Maldonado B, Cooper T V. Smoking transitions in a sample of Hispanic daily light and intermittent smokers. Addict. Behav. 2016; 62:42-6.
Krigel SW, Grobe JE, Goggin K, Harris KJ, Moreno JL, Catley D. Motivational interviewing and the decisional balance procedure for cessation induction in smokers not intending to quit. Addict Behav. 2017; 64:171-8.
Meyer C, Ulbricht S, Gross B, Kästel L, Wittrien S, Klein G, et al. Adoption, reach and effectiveness of computer-based, practitioner delivered and combined smoking interventions in general medical practices: a three-arm cluster randomized trial. Drug Alcohol Depend. 2012; 121(1-2):124-32.
Schane RE, Prochaska JJ, Glantz SA. Counseling nondaily smokers about secondhand smoke as a cessation message: a pilot randomized trial. Nicotine Tob. Res. 2013; 15(2):334-42.
Leavens ELS, Meier E, Tackett AP, Miller MB, Tahirkheli NN, Brett EI, et al. The impact of a brief cessation induction intervention for waterpipe tobacco smoking: A pilot randomized clinical trial. Addict Behav. 2018; 78:94-100.
Cabriales JA, Cooper T V., Salgado-Garcia F, Naylor N, Gonzalez E. A randomized trial of a brief smoking cessation intervention in a light and intermittent Hispanic sample. Exp. Clin. Psychopharmacol. 2012; 20(5):410-9.
Sayegh CS, Huey SJ, Zara EJ, Jhaveri K. Follow-up treatment effects of contingency management and motivational interviewing on substance use: A meta-analysis. Psychol. Addict. Behav. 2017; 31(4):403-14.
Lindson-Hawley N, Thompson TP, Begh R. Motivational interviewing for smoking cessation. Cochrane Database Syst. Rev. 2015; (3):CD006936.
O’Halloran PD, Blackstock F, Shields N, Holland A, Iles R, Kingsley M, et al. Motivational interviewing to increase physical activity in people with chronic health conditions: a systematic review and meta-analysis. Clin. Rehabil. 2014; 28(12):1159-71.
Frost H, Campbell P, Maxwell M, O’Carroll RE, Dombrowski SU, Williams B, et al. Effectiveness of Motivational Interviewing on adult behaviour change in health and social care settings: A systematic review of reviews. PLoS One. 2018; 13(10):e0204890.
Binning J, Woodburn J, Bus SA, Barn R. Motivational interviewing to improve adherence behaviours for the prevention of diabetic foot ulceration. Diabetes Metab. Res. Rev. 2019; 35(2):e3105.
Palacio A, Garay D, Langer B, Taylor J, Wood BA, Tamariz L. Motivational Interviewing Improves Medication Adherence: a Systematic Review and Meta-analysis. J Gen Intern Med. 2016 Aug;31(8):929-40.
Wu L, Gao X, Lo ECM, Ho SMY, McGrath C, Wong MCM. Motivational Interviewing to Promote Oral Health in Adolescents. J Adolesc Heal Off Publ Soc Adolesc Med. 2017; 61(3):378-84.
Alperstein D, Sharpe L. The efficacy of motivational interviewing in adults with chronic pain: A meta-analysis and systematic review. J. Pain. 2016; 17(4):393-403.
Madson MB, Loignon AC, Lane C. Training in motivational interviewing: a systematic review. J. Subst. Abuse Treat. 2009; 36(1):101-9.
Davis MF, Shapiro D, Windsor R, Whalen P, Rhode R, Miller HS, et al. Motivational interviewing versus prescriptive advice for smokers who are not ready to quit. Patient Educ. Couns. 2011; 83(1):129-33.
Heckman CJ, Egleston BL, Hofmann MT. Efficacy of motivational interviewing for smoking cessation: a systematic review and meta-analysis. Tob. Control. 2010; 19(5):410-6.
Apodaca TR, Longabaugh R. Mechanisms of change in motivational interviewing: A review and preliminary evaluation of the evidence. Addiction. 2009; 104(5):705-15.
McCambridge J, Cunningham JA. The early history of ideas on brief interventions for alcohol. Addiction. 2014; 109(4):538-46.
World Health Organization. Screening and brief interventions for substance use problems [Internet]. 2012 [cited 2022 May 25]. Available from: Available from: https://www.who.int/activities/screening-and-brief-interventions-for-substance-use-problems
Collins SE, Witkiewitz K, Kirouac M, Marlatt GA. Preventing Relapse Following Smoking Cessation. Curr. Cardiovasc. Risk Rep. 2010; 4(6):421-8.
Center for Substance Abuse Treatment. . Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 1999. (Treatment Improvement Protocol (TIP) Series, No. 34.) Chapter 2-Brief [Internet]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK64942/
Kristenson H, Ohlin H, Hultén-Nosslin MB, Trell E, Hood B. Identification and intervention of heavy drinking in middle-aged men: results and follow-up of 24-60 months of long-term study with randomized controls. Alcohol Clin. Exp. Res. 1983 ;7(2):203-9.
Chick J, Lloyd G, Crombie E. Counselling problem drinkers in medical wards: a controlled study. BMJ. 1985; 290(6473):965-7.
Babor T, Higgins-Biddle JC. Brief intervention for hazardous and harmful drinking: A manual for use in primary care [Internet]. Geneva: World Health Organization. 2001 [cited 2021 Aug 21]. Available from: Available from: https://apps.who.int/iris/handle/10665/67210
Sarkar S, Pakhre A, Murthy P, Bhuyan D. Brief Interventions for Substance Use Disorders. Indian J. Psychiatry. 2020; 62(Suppl 2):S290-8.
World Health Organization (WHO). The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): manual for use in primary care [Internet]. Geneva: WHO ; 2010 [cited 2021 Aug 21]. Available from: Available from: https://apps.who.int/iris/handle/10665/44320
Prochaska JO, DiClemente CC. Self change processes, self efficacy and decisional balance across five stages of smoking cessation. Prog. Clin. Biol. Res. 1984; 156:131-40.
Royal Australian College of General Practitioners. Smoking, nutrition, alcohol, physical activity (SNAP): a population health guide to behavioural risk factors in general practice [Internet]. 2nd ed. Melbourne; 2015 [cited 2022 May 25]. Available from: Available from: https://www.racgp.org.au/your- practice/guidelines/snap
Haber P, Lintzeris N, Proude E LO. Guidelines for the treatment of alcohol problems [Internet]. Canberra; 2009 [cited 2022 May 25]. Available from: Available from: http://www.alcohol.gov.au/internet/alcohol/publishing.nsf/Content/guidelines-treat-alc-09
Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am. J. Prev. Med. 2008; 35(2):158-76.
Carr AB, Ebbert JO. Interventions for tobacco cessation in the dental setting. A systematic review. Community Dent. Health. 2007; 24(2):70-4.
Maryland: Tobacco Control Resource Center. Brief Interventions [Internet]. [cited 2021 Aug 21]. Available from: Available from: https://marylandtcrc.org/cessation-programs/brief-interventions
Stead LF, Bergson G, Lancaster T. Physician advice for smoking cessation. Cochrane database Syst. Rev. 2008 Apr;(2):CD000165.
Rodgers C. Brief interventions for alcohol and other drug use. Aust. Prescr. 2018; 41(4):117-21.
Rohsenow DJ, Martin RA, Monti PM, Colby SM, Day AM, Abrams DB, et al. Motivational Interviewing versus Brief Advice for Cigarette Smokers in Residential Alcohol Treatment. J. Subst. Abuse Treat. 2014; 46(3):346.
Lindson N, Thompson TP, Ferrey A, Lambert JD, Aveyard P, Group CTA. Motivational interviewing for smoking cessation. Cochrane Database Syst. Rev. 2019; 7(7): CD006936.
Matkin W, Ordóñez‐Mena JM, Hartmann‐Boyce J, Group CTA. Telephone counselling for smoking cessation. Cochrane Database Syst. Rev. 2019; 5(5):CD002850.
Chen D, Wu LT. Smoking cessation interventions for adults aged 50 or older: A systematic review and meta-analysis. Drug Alcohol Depend. 2015; 154:14-24.
Manolios E, Sibeoni J, Teixeira M, Révah-Levy A, Verneuil L, Jovic L. When primary care providers and smokers meet: a systematic review and metasynthesis. Prim. Care Respir. Med. 2021; 31(1):1-8.
International Council of Nurses. Tobacco use and health ICN Position [Internet]. International Council of Nurses; 2012 [cited 2022 May 26]. Available from: Available from: https://www.icn.ch/sites/default/files/inline-files/A18_Tobacco_Use_Health.pdf
Notes
