Artigos
Regionalization of health services in Brazil: an analysis of socioeconomic and health performance inequalities
Regionalization of health services in Brazil: an analysis of socioeconomic and health performance inequalities
Gestão & Regionalidade, vol. 38, núm. 113, pp. 329-343, 2022
Universidade Municipal de São Caetano do Sul

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-SinDerivar 4.0 Internacional.
Recepción: 05 Junio 2020
Aprobación: 24 Marzo 2021
Abstract: This paper aims at reaching an understanding on the standards applied in health regions of Brazil concerning both performance in health and socioeconomic conditions. In order to reach such, two cluster analyses of the current 438 health regions were used, composed of structural constraint indicators and health associated dimensions. The first cluster analysis employed the 3 indicators that constitute the structural constraints, while the second cluster analyses the 6 dimensions of health. The results demonstrate that the health regions with the worst values for structural constraints and financial performance, human resources, infrastructure and quality are located mainly in the macro regions of the North and Northeast of Brazil. In addition, 25% of the health regions in Brazil show a better performance in coverage and quality, and these can be found in the Southeast as well as Northeast regions. Therefore, the conclusion is reached that the regions of health in Brazil still undergo wide-reaching inequalities in regional health both in socioeconomic conditions and health performance.
Keywords: regionalization of health, inequality, performance in health, socioeconomic conditions, evaluation of public policies.
Resumo: Este artigo visa compreender os padrões das regiões de saúde no Brasil quanto à performance em saúde e às condições socioeconômicas. Para atingi-lo, utilizou-se de 2 análises de clusters das 438 regiões de saúde, composta de indicadores de condicionantes estruturais e dimensões de saúde. A primeira análise de clusters empregou os 3 indicadores que compõem os condicionantes estruturais, e a segunda análise de clusters as 6 dimensões de saúde. Os resultados demonstram que as regiões de saúde com os piores valores de condicionantes estruturais e performance em financiamento, recursos humanos, infraestrutura e qualidade, estão localizadas em grande parte nas macrorregiões Norte e Nordeste. Além disso, 25% das regiões de saúde no Brasil possuem melhor performance em cobertura e qualidade, e estão localizadas no Sudeste e Nordeste. Portanto, pode-se afirmar que as regiões de saúde no Brasil ainda possuem grandes desigualdades regionais quanto às condições socioeconômicas e performances na saúde.
Palavras-chave: regionalização da saúde, desigualdade, desempenho na saúde, condições socioeconômicas, avaliação de políticas públicas.
1 INTRODUÇÃO
The moment one starts to study collective and public health in Brazil, one studies also the inequality of the model when it comes to providing a service, which despite basing itself upon the ideals of equality and fairness, reflects inequality and the social problems that intensely affect the country (CAMPOS et al., 2012). Since the implementation of the Federal Constitution of 1988, health became a right of all Brazilian citizens, and the State has the responsibility of attending to the needs of public health (BRASIL, 1988).
In light of this perspective, from 1988 and the years following, SUS (The Unified Public Health System) was not only created but molded around health needs, where the underlying objective was to attend to the demands of the population in a universal, equal and full manner (BRASIL, 1990a; BRASIL, 1990b). From these beginnings, a number of strategies were created to fulfill these objectives laid out for SUS as the national unified public health system, among such strategies were decentralization, family health, plural healthcare networks, service providedaccording to complexity, social participation, among others (WAGNER, 2016).
However, over the years attempts at decentralizing health services were shown as not being sufficient for attending to public needs, generating as such the need of an approximation between the federative entities (PESTANA; MENDES, 2004; DUARTE et al., 2015). In order to fulfill this need, there arose the strategy of regionalization of SUS, first through the operational standards published in 2001 and 2002, then later with the management pact and finally, with the implementation of the Regional Inter-management Commissions(CIRs) in 2011 (BRASIL, 2001; BRASIL 2002; BRASIL; 2006; BRASIL, 2011a).
Therefore, the strategy of the regionalization of health goes on to gain importance, and scientific research takes on the role of studying it more profoundly, firstly through more qualitative studies on the perspectives of this process and then subsequently through some quantitative studies, but with the focus on State and regional perspectives (ALBUQUERQUE et al., 2017; RIBEIRO et al., 2017; VIANA et al., 2019).
Therefore, one notes there is an academic gap in the analysis of the health regionalization process in a quantitative sense, especially when looking from the national perspective (VIANA et al., 2019). Looking out from the above demonstrated perspective, one arrives at the following problematic: How do health regions in Brazil behave from the point of view ofstructural constraints and the performance of health dimensions?
To answer the problems listed, the general objective of this article is to analyze the standards created among the health regions in Brazil, concerning the structural constraints and performance of associated health dimensions. Focusing on the aforementioned as specific objectives, the intention here is to discuss inequality among the health regions in Brazil and map the standards associated with the health regions, regarding socioeconomic conditions and performance in health.
Additionally, this research study is justified as it:
•contributes with a National Agenda of Research Priorities in Health on the following axes: 2.3.16 – Impacts from the decentralization process, regionalization and primary mental health care; 20.1.2.17 – Development of methodologies for regionalization and hierarchical processing of systems and health services; and22.2.1 – Studies concerning basic organization of system, integration, decentralization, regionalization, intersectionality, coverage, access and continuity, quality and effectiveness(BRASIL, 2015);
•developsan assessment study of published policies that cover a wide geographical area concerning health regions in Brazil, as a large part of studies on regionalization of health in Brazil are qualitative and with a state or regional focus, with emphasis on the few studies that aim to quantitatively evaluate this strategy (VIANA et al., 2015; RIBEIRO et al., 2017; PASCHOALOTTO et al., 2018); and broaden the view on health regions in Brazil, in a way that brings out contrasts and inequalities in a visual and numeric form(PESTANA; MENDES, 2004).
2 THEORETICAL FOUNDATION
The regionalization of health is one of the strategies applied in the world through national health systems to attend to the demands made by society, this is highlighted in the systems found in Italy and Portugal(SERAPIONI, 2017; CAVALIERI, FERRANTE, 2020). In the case of Italy, the health regions are autonomous, even in budgetary management, in a way that generates inequalities concerning the service provided and care given(CAVALIERI, FERRANTE, 2020). However, the Portuguese caseis reflected as an intermediary between the Italian and Brazilian case, also with autonomy from the 5 mainland health regions, but with budgetary links and central control(SERAPIONI, 2017). In this sense, in both systems, one also notes inequality in the provision of health services from the standpoint of the sociodemographic conditions of each region (SERAPIONI, 2017; CAVALIERI, FERRANTE, 2020).
Therefore, in relationto the structural constraints, the sociodemographic profile has a relationship with the performance of health regions in aspects of financing and quality of the health services provided (GARNELO; SOUSA; SILVA, 2017). Broadening this perspective, one finds that the development of a population and the socioeconomics of a region also affect the services offered, with an impact across all the dimensions of regionalization of health in Brazil, touching aspects such as coverage and finances and down to the effectiveness of the system(VIANA; LIMA; FERREIRA, 2010).
This possible correlation between the structural constraints and the performance of health regions has generated initiatives toward understanding its standards across the whole country (VIANA et al., 2017). Researchers in Albuquerque et al. (2019) corroborated these findings by pointing out a direct relationship between socioeconomic development and the offer of services, with an improved performance in health surveillance. Furthermore, Duarte et al.(2015) contributed to this understanding by calculating the HDI of health regions across the whole of Brazil, so as to facilitate future statistical and multivariate analyses.
The study by Viana et al. (2015) points to a heterogeneous profile of Brazilian health regions, where the following scenario is clearly visible: 1) a low socioeconomic development and a low offer of health services concentrated in the regions of the North and Northeast; 2) a medium/high socioeconomic development and a low offer of health services spread over the whole country, however concentrated in the Central West region; 3) a medium socioeconomic development and a medium/high offer of health services; 4) a high socioeconomic development and a medium offer of services; 5) and a high socioeconomic development and a high offer of health services, concentrated across the regions of the South and Southeast.
The study by Calvo et al. (2016) also contributed to this discussion by establishing that the North and Northeast regions of Brazil have a higher concentration of medium to small municipalities, which are in an unfavorable situation according to the socioeconomic profile, financial capacity and intervention of health services. However, the regions South and Southeast have a concentration of medium to small municipalities, with favorable or more regular situations. Another factor that can also influence the quality of services provided, as well as in their coverage is migratory flow, due to increased demand in a particular region and the possible misallocation of resources due to population displacement (MORAIS et al., 2018).
The authors Machado, Lima and Baptista (2017) discuss that the financing, the structure, the services and the quality of SUS have not followed the evolution of the structural constraints of society over the last 30 years, thus reinforcing the points discussed by previous authors. Noteworthy here is that these evaluations are only being realized due to the analysis of indicators in a joint and multidimensional manner, from the aspect of conditions of the population and structural constraints until the efficiency and the effectiveness of the regionalization of health services across the whole Brazilian territory(ALBUQUERQUE; MARTINS, 2017).
A relevant point is the term “performance”, which is used throughout this study. The use of this word means efficiency, efficacy and effectiveness, as defined by Howlett, Ramesh and Perl (2013) and Jannuzzi (2012): the public health services provided were of quality and managed to reach a low level of cost (efficiency); the public health services provided reach the objectives and goals previously delimited (efficacy); and the health services provided generate an impact in society, that is, they generate a social justice in terms of the healthcare given (effectiveness).
3 METHODS
This study, particularly concerning its finalization, can be defined as: exploratory, as it performs a discussion on the regionalization of health and socioeconomic conditions; and descriptive, as it points to characteristics of the clusters created by the health regions over the whole country (MATIAS-PEREIRA, 2016). Concerning the type of research, it can be defined as quantitative as it uses statistical methods to arrive at the proposed results(RICHARDSON, 2017).
Under the objective of grouping the health regions in accordance with their homogeneities and separate these according to heterogeneities, the cluster analysis was incorporated based on the values reached in the dimensions and on the ISRS (HAIR JÚNIOR et al., 2009; FÁVERO; BELFIORE, 2017). In this study, the analysis of clusters was applied to the 438 health regions spread across the country, by considering the year of 2016.
In order to create the dimensions for evaluation, two methods were used: electronic questionnaire with specialists, and then the application of the Principal Component Analysis technique.
In its first stage the options for dimensions and indicators were listed from (a) IDSUS (Public Healthcare Performance Index), which was in use until 2011(BRASIL, 2011b); synthetic index created by the Region and Networks group (REGIÃO E REDES, 2018); and researchwork developed by Paschoalotto et al. (2018), which proposed a synthetic index of assessment for health regions in the State of São Paulo. From these dimensions and indicators, an electronic questionnaire was put together on the Google Docs platform and sent to 117 academics, those being, specialists linked to the area of health regionalization that possess publications on an A1 to A2 level, or a book of reference. The questionnaire reached the number of 17 responses, representing 15.45% of the selected sample, and which define the dimensions and indicators from the criterion of 8+1 responses (50% + 1), as shown on Table 1.
With the indicators and dimensions established, one proceeded with collecting data from Proadess (FIOCRUZ, 2011). In order to organize the collected data, the program Microsoft Excel 2010 was used, as a way of preparing and manipulating the data, perform descriptive statistics and then build the ISRS. To run the ACP (HAIR JÚNIOR et al., 2009; FÁVERO; BELFIORE, 2017) the softwareIBM SPSS Statistics v.17 was used, with the aim of standardizing the data, while running more complex statistics.
By means of the indicator definition and of the dimensions that constitute the ISRS Brazil, one can enter into the quantitative part of creating the dimensions and the index. Therefore, to better demonstrate the performed steps, these are given in a systematized fashion in the following:
A – Following the collection of indicators (FIOCRUZ, 2011), one can analyze the database for outliers, which were excluded from the analysis. After this step, in order to obtain a normalized sample, one applies the standardization Score Z (HAIR JÚNIOR et al., 2009; FÁVERO; BELFIORE, 2017);
B – As a means to deal with the outliers (values below -3 and above 3), a sweep was performed and all values below-3 were altered to “-3”, and above 3, to “3” (FÁVERO; BELFIORE, 2017). In addition, the value of 3 was added to the standardized observations, under the intent of generating a clearer visualization of the indicator or index performance
Indicadores Regionais = X + 6
(1) X – Valor padronizado das observações
From the equation above, the regional indicators go on to have an interval value between 0 and 6, that is, all the dimensions and the future indexes were given a value between 0 and 6;
C – To finalize the preparation of the database, two indicators – Infant mortality and Maternal mortality (direct) -, which have an inverse relationship to the remainder (the lower the indicator, the better), go on to the last treatment, using the following equation:
| Coverage | Coverage through the Family Health Strategy | 43,76% | 15,48% |
| population coverage estimated by primary care teams | 44,09% | ||
| Hospital births performed within the health region of residence | 11,85% | ||
| Immunization of children under one year of age withtetra or pentavalent | 0,30% | ||
| Finance | Total public spending on health per inhabitant | 50% | 15,31% |
| Personal resources destined to health per inhabitant | 50% | ||
| Human Resources | Proportion of doctors for every 1,000 inhabitants | 50% | 26,72% |
| Proportion of nurses for every 1,000 inhabitants | 50% | ||
| Infrastructure | Proportion of beds for every 1,000 inhabitants | 37,00% | 16,64% |
| Proportion of ICU/Neonatal beds forevery 1,000 live births | 31,59% | ||
| Proportion of ultrasound equipment for every 100,000 inhabitants | 31,41% | ||
| SUS services | Rate of hospital admittance for every 1,000 inhabitants | 2,54% | 11,39% |
| Surgical admissions performed outside the health region of residence | 23,81% | ||
| Surgical admissions performed within the health region of residence | 23,81% | ||
| Clinical admissions performed outside the health region of residence | 24,93% | ||
| Clinical admissionsperformed withinthe health region of residence | 24,93% | ||
| Quality of SUS | Infant mortality | 34,52% | 14,46% |
| Maternal mortality(direct) | 30,77% | ||
| Hospitalization for conditions sensitive to primary care | 34,71% |
D – The next step was to define the weights for each indicator in relation to the dimension, as well as each dimension to the ISRS. To perform this process, the ACP was used together with the indicators from 2016, by means of dividing the factorial loads of each indicator/dimension by the total variance of the dimension/of the index created. In this way, one can synthesize the indicators for each one of its dimensions and subsequently, the dimensions on the ISRS (HAIR JÚNIOR et al., 2009; FÁVERO; BELFIORE, 2017).
E – With the distribution of the weights realized, one can thus create the defined dimensions through the equation below:
When creating the dimensions, the absent indicators were substituted in the calculation by the multiplying of its weight by the mean of the remaining indicators that constitute that dimension; F – With the dimensions created, one can then create the ISRS with the equation below:

In the creating of the ISRS, the absent indicators were substituted by the multiplication of its weight by the mean of the remaining dimensions that constitute the formation of the ISRS.
To this end, after creating the final database, two cluster analyses were used to measure two standards of homogeneity. The first used the indicators of structural constraints: literacy rate, Income per capita and demographic Density (VIANA et al., 2015), with the objective of analyzing the distribution of performance of the health regions divided by the sociodemographic characteristics.
The second used the six dimensions created to establish the homogeneous groups, with greater focus on performance of the health regions for division(PASCHOALOTTO et al., 2018). Both the analyses used the hierarchical cluster, with the definition of the number of clusters fromthe established dendrogram and the Ward method, with the measurement by the quadratic Euclidean distance (FÁVERO; BELFIORE, 2017).
Finally, for the creating of geographic maps from the indicators used, the software Tabwin v.4.1.5 was employed, which brought a spatial view of the 2 clustering processes defined above.
4 RESULTS AND DISCUSSIONS
This topic presents the two cluster analyses performed, with the objective of demonstrating the performance of health regions across the country, according to theirhomogeneities (FÁVERO; BELFIORE, 2017). The first analysis used the three main indicators (VIANA et al., 2015), which are composed of the structural constraints of the health regions, while the second used the six dimensions formulated for the ISRS.
4.1 Socioeconomic clustering of health regions
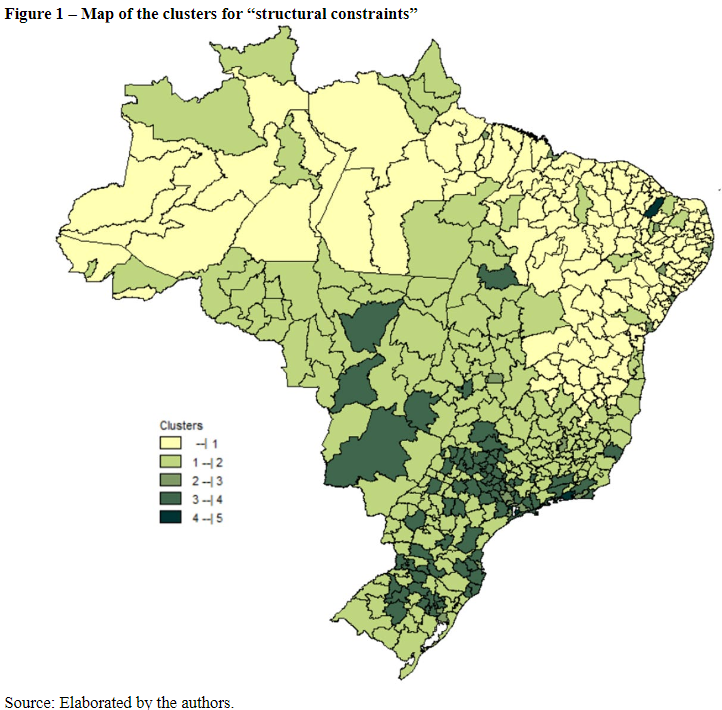
As noted on Table 2 and in Figure 1, cluster 1 is second in terms of more health regions across the country as a whole, mainly in the macro-regions of the North and Northeast, with the highest rate of illiteracy, the second lowest demographic density, the lowest income per capita and the worst performance in the dimensions of finances, human resources, infrastructure, quality of SUS and ISRS (LIMA et al., 2012; VIANA et al., 2015; ALBUQUERQUE; MARTINS, 2017; SOUZA et al., 2018; ALBUQUERQUE et al., 2019; VIACAVA et al., 2019; VIANA et al., 2019). Despite this, this cluster has the best performance in the dimension of coverage of health regions (FERREIRA et al., 2018; VIACAVA et al., 2019).
Cluster2 encompasses the highest number of health regions across the country, with nearly 50% of the macro-region of the North, along with a small part of the Northeast and most of the Central West, Southeast and South. The socioeconomic indicators associated with these regions present the second highest illiteracy rate and the second lowest income per capita. The performance within the dimensions of cluster 2 are highlighted as having the second highest coverage, the second worst values for finance and human resources, as well as a quality very close to that of cluster 1 (LIMA et al., 2012; ALBUQUERQUE; MARTINS, 2017; VIANA et al., 2019).
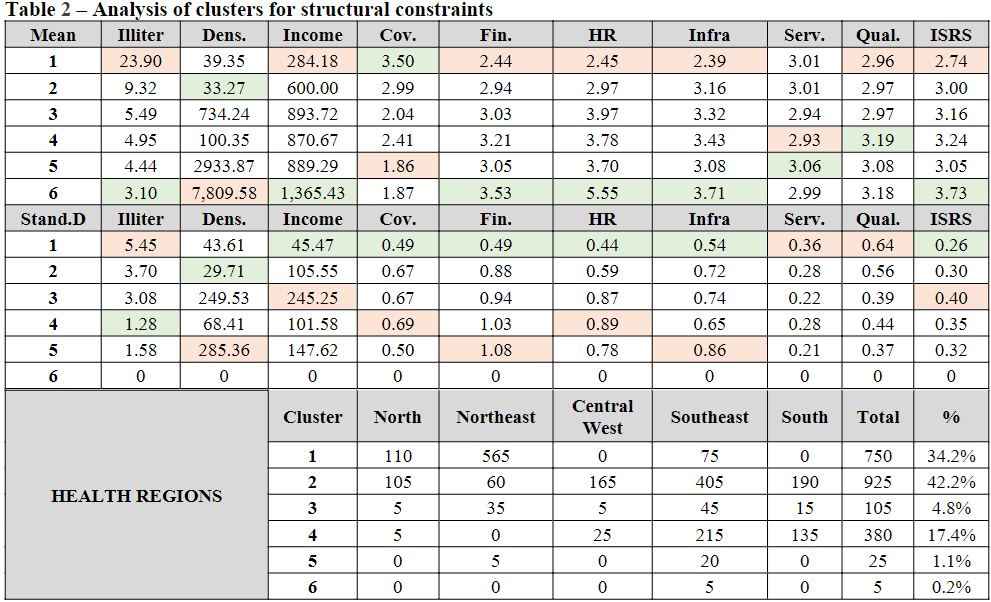
Cluster 3 is composed of health regions from all macro-regions of the country, without a pronounced representativeness and a mean performance across all indicators and dimensions used for analysis. However, cluster 4 composed largely of health regions from the Central West, Southeast and South, present a mean behavior across a majority of the indicators and dimensions, with exception to the dimension of SUS services, where it demonstrated the worst performance and SUS quality, with the best performance between clusters (OLIVEIRA et al., 2017; PASCHOALOTTO et al.2018; ALBUQUERQUE et al., 2019).
Finally, clusters 5 and 6 have the same characteristics in their health regions: large cities, lower rates of illiteracy and higher income per capita, besides performance above the Brazilian average or higher performance across all dimensions, with exception to coverage, where cluster 5 has the worst performance(ALBUQUERQUE; MARTINS, 2017; PASCHOALOTTO et al., 2018).
Therefore, from the clustering by means of the structural constraints, one notes an inequality in the Brazilian health regions, with a concentration of the best sociodemographic conditions in the macro-regions of the Southeast and South, together with a better performance in the health dimensions, with the exception of the dimension coverage (ALBUQUERQUE; MARTINS, 2017; VIANA et al., 2019).
4.2 Clusters of dimensions in the health regions
In the second cluster analysis performed, one notes from Table 3 and figure 2, through a consideration of ISRS, that cluster 1 is made up, in greater part, of health regions from the Northeast and others from the remaining macro-regions. It has the second and best performance in the dimensions coverage and SUS services, respectively, whereas in the dimensions human resources, infrastructure, SUS quality and on the ISRS, it has the worst performance (LIMAet al., 2012; ALBUQUERQUE et al., 2019).
Cluster2 has the highest number of health regions, which are also made up, in greater part, of health regions from the Northeast and a large part of the Southeast. The best performance for cluster 2 is in the dimensions of coverage and SUS quality, but also demonstrates a mean performance in the remaining dimensions (VIACAVA et al., 2019; VIANA et al., 2019).
Cluster 3, which, as a majority, ismade up of the North and Southeast of Brazil has the worst performances concerning the dimensions of finance and SUS services, while presenting a mean performance on the remaining dimensions(LIMA et al., 2012; VIANA et al., 2015). However, cluster 4, made up, in greater part, by health regions of the Southeast and South present the best performance in the dimension of human resources and mean behavior in the other dimensions(GIRARDI et al., 2016; SANTOS NETO, 2017).
| 3,38 | 2,57 | 2,49 | 2,24 | 3,05 | 2,68 | 2,69 |
| 3,60 | 2,57 | 2,70 | 2,76 | 3,00 | 3,13 | 2,92 |
| 2,69 | 2,51 | 2,68 | 2,58 | 2,96 | 2,97 | 2,71 |
| 2,42 | 3,09 | 3,97 | 3,64 | 2,98 | 3,05 | 3,29 |
| 3,28 | 3,05 | 2,90 | 3,66 | 3,00 | 2,99 | 3,13 |
| 2,39 | 3,35 | 3,14 | 2,89 | 2,97 | 3,13 | 2,99 |
| 0,49 | 0,58 | 0,42 | 0,52 | 0,33 | 0,58 | 0,22 |
| 0,38 | 0,61 | 0,55 | 0,58 | 0,34 | 0,64 | 0,26 |
| 0,66 | 0,76 | 0,58 | 0,61 | 0,33 | 0,50 | 0,30 |
| 0,62 | 0,91 | 0,90 | 0,60 | 0,20 | 0,45 | 0,34 |
| 0,56 | 0,83 | 0,58 | 0,69 | 0,29 | 0,52 | 0,27 |
| 0,79 | 1,14 | 0,56 | 0,52 | 0,33 | 0,49 | 0,28 |
| 60 | 205 | 25 | 40 | 15 | 345 | 15,8% |
| 45 | 300 | 30 | 150 | 25 | 550 | 25,2% |
| 90 | 70 | 25 | 100 | 30 | 315 | 14,4% |
| 25 | 50 | 25 | 200 | 120 | 420 | 19,2% |
| 5 | 35 | 55 | 90 | 75 | 260 | 11,9% |
| 0 | 5 | 30 | 185 | 75 | 295 | 13,5% |
Cluster 5 has the least representativeness of the health regions when compared to the other clusters, and is located, in greater part, in the Southeast and South. This cluster has a mean performance in a majority of dimensions, with exception to infrastructure and ISRS, where it presents the best performance in these dimensions between the clusters(FACCHINI; TOMASI; DILÉLIO, 2018).
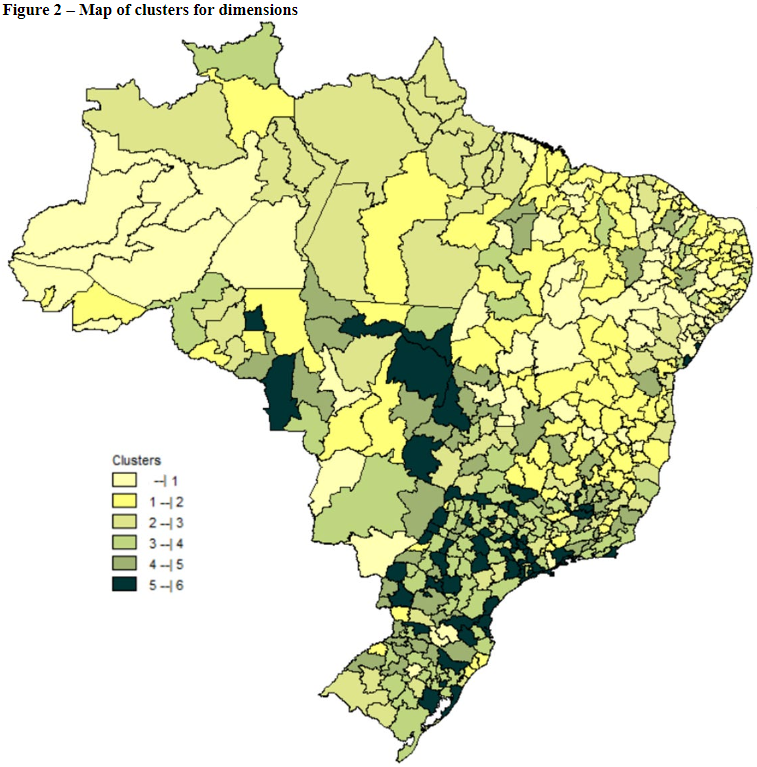
Finally, cluster 6 is, in its greater part, constituted of the health regions from the Southeast. Despite having the worst performance for the dimension of coverage, it reached the best performance in the dimensions of finance and SUS quality(FERREIRA et al., 2018; VIACAVA et al., 2019). As such, from the clusters formed through the health dimensions and the synthetic index, one notes an unequal distribution of performance in the health inter and intra macro-regions, with high values for standard deviation, mainly in the macro-regions South and South East(ALBUQUERQUE et al., 2019; VIANA et al., 2019).
5 FINAL CONSIDERATIONS
The health regions of Brazil, despite their creation to mitigate the socio-economic inequalities and low performance in health, have shown very little in terms of advance (ALBUQUERQUE et al., 2017; CASANOVA et al., 2017). Although there exist studies that point to a reduction in inequalities among the health regions across the country as a whole (MOREIRA; FERRÉ; ANDRADE, 2017; ALBUQUERQUE et al., 2019; VIACAVA et al., 2019), the data demonstrated herein points out that this has not happened in a uniform fashion between dimensions(FERREIRA et al., 2018; VIANA et al., 2018).
The results and the mapping of health regions developed herein point out that the socio-economic are intimately correlated with the performance of indicators and dimensions in the health regions, with exception of the coverage indicators, in a way that: (a) enhances studies on intersectorality (VIANA; LIMA; FERREIRA, 2010; CARVALHO et al., 2015; GARNELO; SOUSA; SILVA, 2017; VIANA et al., 2017; PASCHOALOTTO et al., 2018); (b) the economic-financial capacity of the health regions can directly influence their human resources and materials, but not the services provided or their quality (AMORIM; PINTO JÚNIOR; SHIMIZU, 2015; FERREIRA et al., 2018; PASCHOALOTTO et al., 2018); and (c) there exist health regions with similar behaviors under socio-economic conditions and performance in health, but are in different macro-regions of the country (VIACAVA et al., 2019; VIANA et al., 2019).
In addition, the research study developed herein presented contributions to the scientific academy and to the Brazilian public administration, mainly in respect to the administration of the health regionalization process in Brazil, through the development of those points listed by previous studies, those being: (I) to evaluate the public health regionalization policy in Brazil after the 2011 decree (BRASIL,2011a), which consolidated the health regions in the country, in a way that gives a panoramic view of the performance of health regions divided into macro-regions (VIANA et al., 2015; RIBEIRO et al., 2017; PASCHOALOTTO et al., 2018); and (II) point to relationships between the best socio-economic conditions and quality of health services provided; in the absence of and in light of the inadequate standard of financing in health regions (ALBUQUERQUE et al., 2017; COSTA, 2017).
As a limitation of this study, one can point to: (I) the use of secondary data for creating the ISRS, which can bias the development of the study and jeopardize it due to unreliable data; (II) the use of ACP for creating the dimensions and the ISRS, which pushes pure indicators in the direction of losing information and representativity and (III) absent secondary data coming from public administration that hinders a more refined and in-depth analysis.
For future research, the following are contemplated: (I) the broadening ofanalyses between health indicators and the structural constraints of health regions in Brazil, with the possible inclusion of new control variables and (II) the comparison between private and public sectors in these health regions and their consequences, with the inclusion of supplementary health data.
REFERENCES
ALBUQUERQUE, A. C. de et al.Avaliação de desempenho da regionalização da vigilância em saúde em seis Regiões de Saúde brasileiras. Cadernos de Saúde Pública, Rio de Janeiro, v. 35, 2019. Supl. 2.
ALBUQUERQUE, M. V. de et al.Desigualdades regionais na saúde: mudanças observadas no Brasil de 2000 a 2016. Revista de Ciência & Saúde Coletiva, Rio de Janeiro, v. 22, n. 4, p. 1055-1064, 2017.
ALBUQUERQUE, M. V. de; MARTINS, M. Indicadores de desempenho no Sistema Único de Saúde: uma avaliação dos avanços e lacunas. Saúde em Debate, Rio de Janeiro, v. 41, n. especial, p. 118-137, 2017.
AMORIM, A. S.; PINTO JÚNIOR, V. L.; SHIMIZU, H. E. O desafio da gestão de equipamentos médico-hospitalares no Sistema Único de Saúde. Saúde em Debate, Rio de Janeiro, v. 39, n. 5, p. 350-362, 2015.
BRASIL. [Constituição 1988].Constituição da República Federativa do Brasil. Brasília: Senado Federal, 1988.
BRASIL. Conselho Nacional de Secretários de Saúde. A gestão do SUS.Brasília: CONASS, 2011a. (Coleção Para Entender a Gestão do SUS, v.1).
BRASIL. Lei nº 8.080, de 19 de setembro de 1990. Dispõe sobre as condições para a promoção, proteção e recuperação da Saúde, a organização e o funcionamento dos serviços correspondentes e dá outras providências. Diário Oficial da União, Brasília, 1990a. Disponível em: http://www.portal.saude.gov.br/portal/arquivos/pdf/lei8080.pdf. Acesso em: 26 fev. 2016.
BRASIL. Lei nº 8.142, de 28 de dezembro de 1990. Dispõe sobre a participação da comunidade na gestão do Sistema Único de Saúde (SUS) e sobre as transferências intergovernamentais de recursos financeiros na área da saúde e dá outras providências. Diário Oficial da União, Brasília, 1990b. Disponível em: http://www.planalto.gov.br/ccivil_03/leis/l8142.htm. Acesso em: 27 fev. 2016.
BRASIL. Ministério da Saúde. IDSUS: Índice de Desempenho do Sistema Único de Saúde. Ministério da Saúde, 2011b. Disponível em: http://www.portal.saude.gov.br/portal/arquivos/pdf/IDSUS_06-03-12.pdf. Acesso em: 26 jun. 2018.
BRASIL. Ministério da Saúde. Pactos pela vida, em defesa do SUS e de gestão – diretrizes operacionais. Brasília: Departamento de Apoio à Descentralização; Secretaria Executiva, 2006. (Pactos pela Saúde 2006, v. 1).
BRASIL. Ministério da Saúde. Secretaria de Assistência à Saúde. Portaria MS/GM nº 373, de 28 de fevereiro de 2002.Dispõe sobre a Norma Operacional da Assistência à Saúde: NOAS-SUS 01/02. Diário Oficial da União, seção 1, Brasília, 28 de fevereiro de 2002.
BRASIL. Ministério da Saúde. Secretaria de Assistência à Saúde. Regionalização da assistência à saúde: aprofundando a descentralização com equidade no acesso Norma Operacional da Assistência à Saúde – NOAS-SUS 01/01 (Portaria MS/GM n.º 95, de 26 de janeiro de 2001, e regulamentação complementar). Brasília: Ministério da Saúde, 2001. (Série A. Normas e Manuais Técnicos, n. 116).
BRASIL. Ministério da Saúde. Secretaria de Ciência, Tecnologia e Insumos Estratégicos. Departamento de Ciência e Tecnologia. Agenda nacional de prioridades de pesquisa em saúde. 2. ed. Brasília: Editora do Ministério da Saúde, 2015.
CALVO, M. C. M. et al. Estratificação de municípios brasileiros para avaliação de desempenho em saúde. Epidemiol. Serv. Saúde, Brasília, v. 25, n. 4, p. 767-776, 2016.
CAMPOS, G. W. S. et al. Tratado de Saúde Coletiva. 2. ed. rev. aum. São Paulo: Hucitec, 2012.
CARVALHO, R. A. da S. et al.Desigualdades em saúde: condições de vida e mortalidade infantil em região do nordeste do Brasil. Revista de Saúde Pública, São Paulo, v. 49, n. 5, 2015
CASANOVA, A. O. et al. A implementação de redes de atenção e os desafios da governança regional em saúde na Amazônia Legal: uma análise do Projeto QualiSUS-Rede. Revista de Ciência & Saúde Coletiva, Rio de Janeiro, v. 22, n. 4, p. 1209-1224, 2017.
CAVALIERI, M.; FERRANTE, L. Convergence, decentralization and spatial effects: An analysis of Italian regional health outcomes. Health Policy, 124(2), p. 164-173, 2020.
COSTA, Nilson do Rosário. Austeridade, predominância privada e falha de governo na saúde. Revista de Ciência & Saúde Coletiva, Rio de Janeiro, v. 22, n. 4, p. 1065-1074, 2017.
DUARTE, C. M. R. et al. Regionalização e desenvolvimento humano: uma proposta de tipologia de Regiões de Saúde no Brasil. Cadernos de Saúde Pública, Rio de Janeiro, v. 31, n. 6, p. 1163-1174, 2015.
FACCHINI, L. A.; TOMASI, E.; DILÉLIO, A. S. Qualidade da atenção primária à saúde no Brasil: avanços, desafios e perspectivas. Saúde em Debate, Rio de Janeiro, v. 42, n. esp. 1, p. 208-223, 2018.
FÁVERO, L.; BELFIORE, P. Manual de análise de dados. Rio de Janeiro: Elsevier. 2017.
FERREIRA, J. et al. Planejamento regional dos serviços de saúde: o que dizem os gestores? Saúde e Sociedade, São Paulo, v. 27, n. 1, p. 69-79, 2018.
FIOCRUZ. Fundação Oswaldo Cruz. Proadess: Programa de Avaliação do Desempenho do Sistema Único de Saúde. Fiocruz, 2011. Disponível em: https://www.proadess.icict.fiocruz.br. Acesso em: 10 jan. 2018.
GARNELO, L.; SOUSA, A. B. L.; SILVA, C. de O. da. Regionalização em saúde no Amazonas: avanços e desafios. Revista de Ciência & Saúde Coletiva, Rio de Janeiro, v. 22, n. 4, p. 1225-1234, 2017.
GIRARDI, S. N. et al. Impacto do Programa Mais Médicos na redução da escassez de médicos em Atenção Primária à Saúde. Ciência & Saúde Coletiva, Rio de Janeiro, v. 21, n. 9, p. 2675-2684, 2016.
HAIR JÚNIOR, J. F. et al.Multivariate Data Analysis. 7. ed. Pearson, 2009.
HOWLETT, M.; RAMESH, M.; PERL, A. Política pública: seus ciclos e subsistemas – uma abordagem integradora. Rio de Janeiro: Elsevier, 2013.
JANNUZZI, Paulo de Martino. Indicadores sociais no Brasil. 5. ed. Campinas, SP: Alínea, 2012.
LIMA, L. D. de et al. Regionalização da saúde no Brasil. In: GIOVANELLA, Lígia (org.). Política e sistema de saúde no Brasil. 2. ed. rev. e ampl. Rio de Janeiro: Editora Fiocruz, 2012.
MACHADO, C. V.; LIMA, L. D. de; BAPTISTA, T. W. da F. Políticas de saúde no Brasil em tempos contraditórios: caminhos e tropeços na construção de um sistema universal. Cadernos de Saúde Pública, Rio de Janeiro, v. 33, 2017. Supl. 2.
MATIAS-PEREIRA, José. Manual de metodologia da pesquisa científica. 4. ed. São Paulo: Atlas, 2016.
MORAIS, M. S. de et al. Retrato de uma região: impacto da indústria sucroalcooleira, indicadores de saúde e a percepção dos gestores. Saúde e Sociedade, São Paulo, v. 27, n. 3, p. 922-928, 2018.
MOREIRA, L. M. C.; FERRÉ, F.; ANDRADE, E. I. G. Financiamento, descentralização e regionalização: transferências federais e as redes de atenção em Minas Gerais, Brasil. Ciência & Saúde Coletiva, Rio de Janeiro, v. 22, n. 4, p. 1245-1256, 2017.
OLIVEIRA, M. J. C. et al.Contextualização da diarreia infantil no brasil: revisão de literatura. ReonFacema, Maranhão, v. 3, n. 2, p. 506-512, 2017.
PASCHOALOTTO, M. A. C et al. A regionalização do SUS: proposta de avaliação de desempenho dos Departamentos Regionais de Saúde do estado de São Paulo. Saúde e Sociedade, São Paulo, v. 27, n. 1, p. 80-93, 2018.
PESTANA, M; MENDES E. V. Pacto de gestão: da municipalização autárquica à regionalização cooperativa. Belo Horizonte: Secretaria do Estado de Minas Gerais, 2004.
REGIÃO e REDES. Políticas, planejamento e a gestão das regiões e redes de atenção à saúde no Brasil. Região e Redes, 2018. Disponível em: http://www.resbr.net.br/apresentacao/. Acesso em: 20 fev. 2018.
RIBEIRO, J. M. et al. Políticas de saúde e lacunas federativas no Brasil: uma análise da capacidade regional de provisão de serviços. Revista deCiência e Saúde coletiva, Rio de Janeiro, v. 22, n. 4, p. 1031-1044, 2017.
RICHARDSON, R. J. Pesquisa social: métodos e técnicas. 4. ed. São Paulo: Atlas, 2017.
SANTOS NETO, J. A. dos et al. Análise do financiamento e gasto do Sistema Único de Saúde dos municípios da região de saúde Rota dos Bandeirantes do estado de São Paulo, Brasil. Ciência & Saúde Coletiva, Rio de Janeiro, v. 22, n. 4, p. 1269-1280, 2017.
SERAPIONI, M. Economic crisis and inequalities in health systems in the countries of Southern Europe. Cadernos de Saúde Pública, v. 33, n. 9, e00170116, 2017.
SOUZA, M. de F. M. et al. Transição da saúde e da doença no Brasil e nas Unidades Federadas durante os 30 anos do Sistema Único de Saúde. Revista de Ciência & Saúde Coletiva, Rio de Janeiro, v. 23, n. 6, p. 1737-1750, 2018.
VIACAVA, F. et al. Desigualdades regionais e sociais em saúde segundo inquéritos domiciliares (Brasil, 1998-2013). Ciência & Saúde Coletiva, Rio de Janeiro, v. 24, n. 7, p. 2745-2760, 2019.
VIANA, A. L. D. et al. Região e Redes: abordagem multidimensional e multinível para análise do processo de regionalização da saúde no Brasil. Rev. Bras. Saúde Matern. Infant., Recife, v. 17, p. S17-S26, 2017. Supl. 1.
VIANA, A. L. D. et al. Tipologia das regiões de saúde: condicionantes estruturais para a regionalização no Brasil. Saúde e Sociedade, São Paulo, v. 24, n. 2, p. 413-422, 2015.
VIANA, A. L. D.; LIMA, L. D. de; FERREIRA, M. P. Condicionantes estruturais da regionalização na saúde: tipologia dos Colegiados de Gestão Regional. Ciência & Saúde Coletiva, Rio de Janeiro, v. 15, n. 5, p. 2317-2326, 2010.
WAGNER, Gastão. Estratégias para consolidação do SUS e do direito à saúde. Revista Ensaios & Diálogos em Saúde Coletiva, Rio de Janeiro, v. 3, p. 36-40, 2016.