Originales

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-SinDerivar 4.0 Internacional.
Recepción: 15 Mayo 2023
Aprobación: 14 Julio 2023
DOI: https://doi.org/10.18566/medupb.v43n1.a02
Abstract:
Objective: mastectomy after breast cancer produces several postural and biomechanical alterations in the frontal and sagittal plane. Such changes lead to disturbed kinematics of the spine, muscle imbalance and altered foot weight bearing. This study aims to describe body balance alterations after mastectomy based on the baropodometric analysis of their mean pressure and static load.
Methodology: a descriptive correlational research was carried out. Foot weight-bearing properties were identified in 17 patients who have undergone a mastectomy. An Ecosanit Foot pressure plate was used to measure foot load at anatomical position and keeping the feet together.
Results: 17 female patients who had undergo mastectomy with a mean age of 54.16 years took part on the research. Patients who have had a dominant-side mastectomy demonstrated significant greater mean pressure at anatomical position when compared to those patients who have had a non-dominant side mastectomy (227.2 ± 22.16 versus 175.6 ± 14.95, p =0.05). There was no significant difference for static load between the patients who have had a dominant side mastectomy and patients who have had a non-dominant side mastectomy at anatomical position (52.43 ± 4.069 versus 49.69 ± 4.094, respectively).
Conclusion: the current results of our research showed the unbalanced weight distribution in patients after mastectomy. Consequently, it describes the postural and muscular alterations, and the static and dynamic imbalance in breast cancer patients.
Keywords: baropodometric, biomechanical, breast cancer, mastectomy, physical therapy.
Resumen:
Objetivo: la mastectomía posterior al cáncer de seno produce diversas alteraciones posturales y biomecánicas en el plano frontal y sagital. Dichos cambios conducen a una cinemática alterada de la columna vertebral, desequilibrio muscular y alteración del soporte del peso del pie. Este estudio pretende describir las alteraciones de la baropodometría después de la mastectomía, con base en análisis baropodométricos de la presión media y la carga estática.
Metodología: se realizó un estudio descriptivo correlacional. Las propiedades de carga del pie se identificaron en 17 mujeres mastectomizadas. Se utilizó una placa de presión Ecosanit Foot para medir la carga del pie en posición anatómica y con los pies juntos.
Resultados: en el estudio participaron 17 mujeres mastectomizadas con una edad media de 54.16 años. Las pacientes reportaron una presión media significativamente mayor en la posición anatómica del lado dominante mastectomizado en comparación con el lado no dominante mastectomizado (227.2 ± 22.16 vs. 175.6 ± 14.95, p =0.05). No hubo diferencia significativa para la carga estática entre el lado dominante mastectomizado y el lado no dominante mastectomizado en la posición anatómica (52.43±4.069 vs. 49.69 ± 4.094, de forma respectiva).
Conclusión: los resultados actuales de nuestro estudio evidenciaron la distribución desequilibrada del peso (vector carga en el pie) en pacientes después de la mastectomía. Por tanto, en este texto se describen las alteraciones posturales, musculares, y el desequilibrio estático y dinámico en pacientes con cáncer de seno.
Palabras clave: baropodometría, biomecánica, cáncer de seno, mastectomía, fisioterapia.
Resumo:
Objetivo: A mastectomia após câncer de mama produz diversas alterações posturais e biomecânicas nos planos frontal e sagital. Tais mudanças levam a alteração da cinemática da coluna, desequilíbrio muscular e alteração do suporte de peso do pé. Este estudo tem como objetivo descrever as alterações baropodométricas após mastectomia, com base em análises baropodométricas de pressão média e carga estática.
Metodologia: foi realizado estudo correlacional descritivo. Propriedades de carga nos pés foram identificadas em 17 mulheres mastectomizadas. Uma placa de pressão Ecosanit Foot foi usada para medir a carga do pé em posição anatômica e com os pés juntos.
Resultados: participaram do estudo 17 mulheres mastectomizadas com idade média de 54,16 anos. Os pacientes relataram uma pressão média significativamente maior na posição anatômica do lado mastectomizado dominante em comparação ao lado mastectomizado não dominante (227,2 ± 22,16 vs. 175,6 ± 14,95, p =0,05). Não houve diferença significativa para a carga estática entre o lado mastectomizado dominante e o lado mastectomizado não dominante na posição anatômica (52,43 ± 4,069 vs. 49,69 ± 4,094, respectivamente).
Conclusão: Os resultados atuais do nosso estudo mostraram distribuição de peso desequilibrada (carga vetorial no pé) em pacientes após mastectomia. Portanto, este texto descreve alterações posturais, musculares e desequilíbrio estático e dinâmico em pacientes com câncer de mama.
Palavras-chave: baropodometria, biomecânica, câncer de mama, mastectomia, fisioterapia.
Introduction
Cancer and its treatment produce a series of side effects which have a considerable impact on the structure and function of the human body. These will depend on the location, type of cancer and received treatment1. It is estimated that 19 million new cases and 9 million deaths occur in The Americas, a percentage which, according to projections, will increase to 30 million by 2040. Breast cancer is the most common malignant tumor in female patients in developed countries2. Due to an early diagnosis and current multimodal treatment, the survival rate for this type of cancer is 90 % after five years3. The main therapeutic methodology for breast cancer consists of encompassing mastectomy surgery and adjuvant treatment consisting of chemotherapy, radiotherapy, and hormone therapy. These treatments can lead to negative consequences. Those complications could occur immediately after treatment such as infection of the surgical site, bleeding, wound margins necrosis, lymphorrhagia and phantom pain. And, late complications including nerve damage, paresthesia, weakness, pain, fibrosis, poor healing, among others4.
Additionally, it is estimated that breast cancer survivors may suffer from secondary shoulder dysfunction, caused by the biomechanical alteration of muscles that have been manipulated during the surgical procedure, in addition to the antalgic postures. These postural and biomechanical alterations can produce important limitations in basic daily activities and daily life5. According to Benton et al., women who experience surgical mastectomy on their dominant side demonstrated significantly greater weakness (11 %) compared to their non-dominant side, this leads to balance alterations and functional impairment which may place them at risk for either acute or chronic injury (p<0,001)6.
On the other hand, the absence of the breast causes a major effect on women’s self-image and a decreased sense of femininity that can lead to anxiety, depression and poor quality of life7. It has been estimated that about 90 % of women who have undergone a mastectomy use permanent breast prosthesis or during the waiting period preceding breast reconstruction8.
Therefore, due to the high incidence of secondary effects, posture after mastectomy has been studied by several authors9,10. The results of these studies describe irregularities in the sagittal plane (thoracic hyperkyphosis) and frontal plane (shoulder elevation, scapular asymmetry, and scoliosis). Such changes lead to disturbed kinematics of the spine, resulting in increased muscle imbalance. Those factors affect axis of extremities, foot weight bearing and shape. Changes of the foot are significant factors leading to mobility loss and increases the hazard of falling11.
Głowacka-Mrotek et al., have reported greater load bearing on non-operated side of breast patients with cancer, which constitutes a side effect even in the long term, up to five years after the mastectomy. This can lead to alterations in weight distribution, balance and gait11. These same alterations were reported even in quadrantectomy patients, with a sample of 116 patients12. Manikowska et al., reported greater similarity between the control group and the group of patients who used external prosthesis, which evidenced a better weight distribution, though, there was no statistically significant difference. The discrepancies in the loads might be due to changes in body posture, muscular imbalance, antalgic trunk and upper limb position13.
There are a few investigations that study weight bearing distribution after mastectomy. This study aims to describe body balance alterations after mastectomy based on the baropodometric analysis of their mean pressure and static load.
Methodology
A descriptive correlational study was carried out to identify balance alterations in women with breast cancer, ethical approval was granted by Fundación Universitaria María Cano Ethics Committee, by registration 01300831-2019-311. All participants were provided with complete details of the study before providing their informed consent and the tests done did not imply any harm or risk for volunteers. The foot weight-bearing properties were identified in 17 women which were selected through a convenience sampling to be evaluated. The data obtained for the sample selection were acquired through the company Mascapacidad S.A.S., via its database. For the inclusion of participants, the following criteria were considered: patients must be legal-age adult women with unilateral mastectomy, with good cognitive faculties. Women with psychiatric or neurological disorders, reconstructive surgery or bilateral mastectomy were excluded.
The results obtained in the test applied to patients included: Anthropometric information of each participant and an ecosanit foot pressure plate, on its 4.0 version, was used for foot load (figure 1).
Figure 1. Plates Ecosanit Foot.
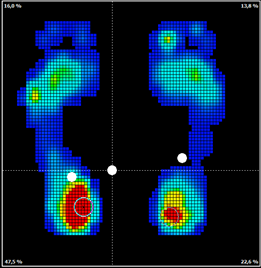
Figure 1
Plates Ecosanit Foot.
During examination, the patient stands on the platform in two positions (ecosanit foot). Position 1: anatomical position with the feet apart at shoulder width. Position 2: anatomical position with feet together. The following parameters were included for test analysis:
Position 1
-Static load (%) for healthy and amputated breast side.
-Mean pressure (kilopascal) for healthy and amputated breast side.
Position 2
-Static load (%) for healthy and amputated breast side.
-Mean pressure (kilopascal) for healthy and amputated breast side.
These positions were chosen because they allow to explain changes and alterations in postural control by identifying faults in plantar proprioceptive response, both from a natural support base and a reduced support base. Which imply additional challenges for proprioceptive receptors and balance.
The patients were assessed on the baropodometric platform on two occasions. The measurements were taken by two physiotherapists with postgraduate training in neurorehabilitation, biomechanics, and clinical leadership in cancer. Each evaluator was responsible for administering both tests to the same participant, to maintain the validity of the variables over time and the quality of the data obtained.
These results are presented as mean ± standard error of the mean (SEM) and percentage. The effect of the breast absence on the baropodometric platform was analyzed with unpaired Mann-Whitney U test and Kruskal-Wallis test followed by Dunn's post-hoc test for unpaired comparisons. Paired comparisons were made with Mann Whitney paired test. Differences were considered statistically significant at p<0.05. The statistical package GraphPad Prism 8v8.0.1 was used.
To analyze the results, a comparison of means was performed, identifying differences in baropodometric variables among breast cancer mastectomy patients. No correlations were conducted between the variables to measure the intensity of linear relationship between two variables because the sample size would limit the reliability of the results.
Results
The foot weight-bearing properties were identified in 17 women who met the inclusion criteria. The anthropometric characteristics serving as baseline of the sample are described in table 1. Mean age in the study group was 54.16 years, with a mean body mass index (BMI) of 29.18 kg/mt, which is on the overweight level. 92.3 % of participants were diagnosed with stage II and III of the disease.
Anthropometric variables and their association with baropodometric parameters
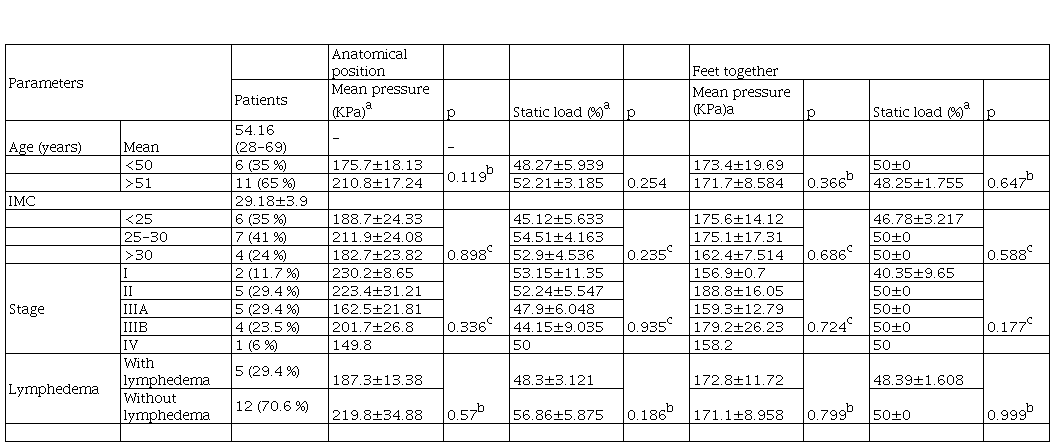
Note: Results are in mean±SEM. aValues for the mastectomy side. bMann-Whitney test. cKruskal-Wallis test. Significance at p<0.05.
Oncological treatments and their relationship with baropodometric parameters
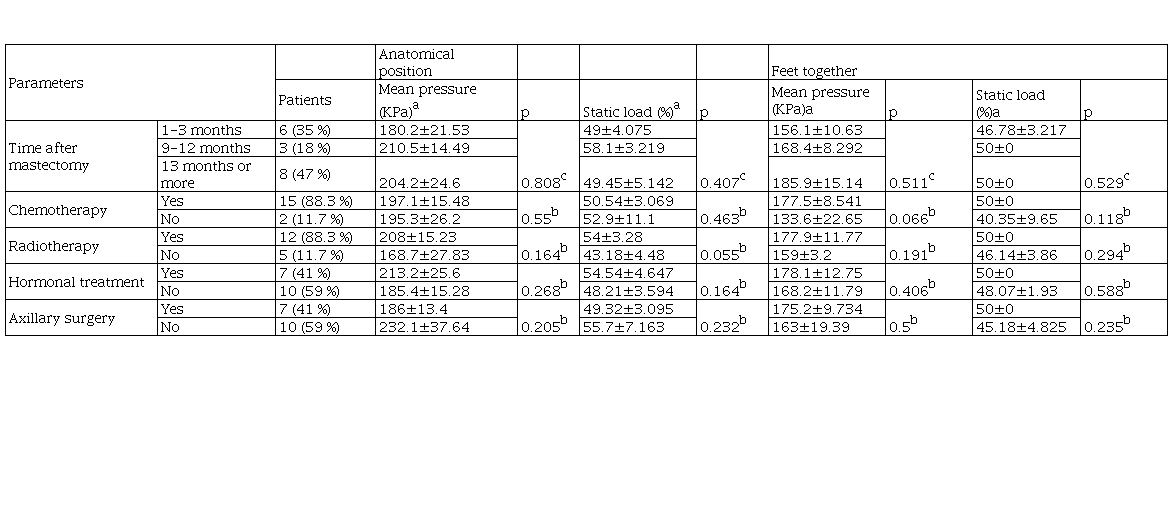
Note Results in mean±SEM.
aValues for the mastectomy side. bMann-Whitney test. cKruskal-Wallis test. Significance at p<0.05.
The table 2 provides a summary of the parameters reflecting static load and mean pressure at anatomical position and with feet together in relation to the oncological treatment received. Patients who received radiotherapy showed a higher mean pressure and statistically significant difference in the static load at anatomical position compared to those subjects who did not receive that treatment (p= 0.055).
Mastectomy and dominant side and their relationship with baropodometric parameters
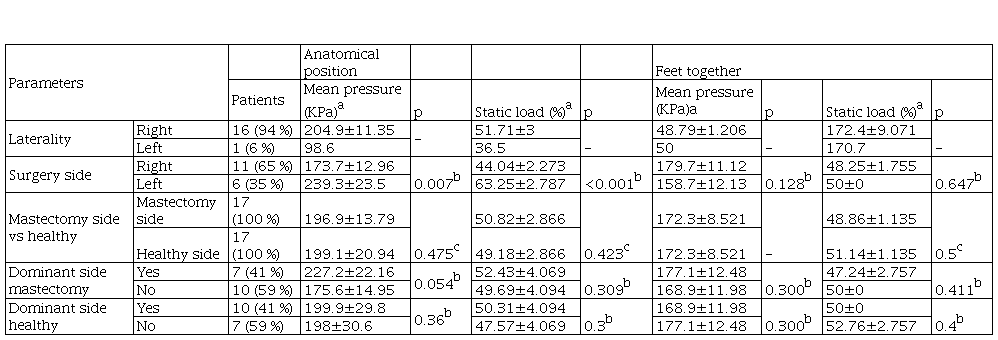
Note Results in mean±SEM.
aAnatomical position values of the mastectomy side. bMann-Whitney test. cMann Whitney test. Significance at p<0.05
The table 3 describes the baropodometric parameters in relationship with amputated breast and laterality. Patients who have had a dominant-side mastectomy demonstrated significant greater mean pressure at anatomical position when compared to those patients who have had a non-dominant side mastectomy (227.2±22.16 versus 175.6±14.95, p = 0.05). There was no significant difference for static load at anatomical position between the patients who have had a dominant side mastectomy and patients who have had a non-dominant side mastectomy (52.43±4.069 versus 49.69±4.094, respectively). Patients showed higher mean pressure at healthy dominant side compared to healthy non-dominant side, however no statistical significance was found (199.9±29.8 versus 198±30.6, respectively).
Discussion
Mastectomy is a widespread surgical technique, which might affect the mobility, thus, motor function can be lessened due to this procedure. Patients after mastectomy have muscular weakness and poor coordination. Alterations of the mobility of the upper extremity affect the lumbosacral spine leading to motor, and also, structural changes. These alterations may explain progressing deformities and unbalanced weight bearing on the foot11. As can be seen on the statistical findings of our research, there is a significant difference between the mean pressure of patients who have had a dominant-side mastectomy compared to those patients who have had a non-dominant side mastectomy (p=0.054). Furthermore, our results showed a higher mean pressure on the mastectomy side compared to the healthy side with a percentage of 50.82±2.866 vs 49.18±2.866 respectively.
This is similar to what was found by Koralewska et al.14, which studied 52 women after unilateral mastectomy. According to their results the mean± SD weight bearing distribution on the amputated side was 50.10 ± 4.86 compared to 49.90 ± 4.86 on the non-amputated side.
In addition, Benton et al.. described that, women who experienced surgical mastectomy on their dominant side demonstrated a significant imbalance in upper extremity strength, and that a progressive resistance training program only two days a week, over an eight-week period can reverse that imbalance. These results may have an influence on spine and weight bearing balance, supporting the results described in our study related to a higher mean pressure on patients who have had a dominant-side mastectomy.
Regarding to women in Colombia, there is little evidence specifically related to baropodometry after a mastectomy, however, in our previous article a higher static load towards the operated side of 10 breast cancer patients at anatomical position was described. Conversely, when the sustentation polygon was smaller, with feet together, the static load leans towards the non-operated side. However, none of the comparisons showed a statistical significance10.
Other authors have reported that a good external breast prosthesis can help women after mastectomy to improve their body image and body posture, and those elements could have a positive impact on socialization and self-confidence15,16. In addition, there is a greater static load distribution between both feet after the use of the prosthesis. This could translate into a better weight distribution on the load vector during daily activities that imply balance and gait changes, such as going up and down stairs, walking through various terrains and carrying large objects. Likewise, the baropodometry reported that using and implant aids weight distribution on both feet, an element that contributes to the postural stability of patients who have had a mastectomy11.
Furthermore, the recommendation based on these findings is the use of an external hypoallergenic silicone prosthesis whose development begins from the geometric analysis of the existing breast shape, taking as reference the size that the woman wears in her underwear and elements that determine the geometry of the implant such symmetries, asymmetries, fixation points of the breast on the trunk and details such as the nipples. The requirements of patients who have had a mastectomy based on their perception and through the anatomical location of the existing breast, combined with numerical and mathematical calculations on the breast, translates into a design that preserves those anthropometric similarities of the female bust, thus consciously promoting the feeling of having a part of their body with themself.
Głowacka-Mrotek et al., described that mastectomy patients did not distribute weight onto both sides similarly, and the difference is statistically significant (p <0.001). The motive behind unbalanced weight bearing has to do whit limited mobility of joints, abnormal posture or weakness of leg muscle. Additionally, they described that pes cavus is more common on the operated breast side, while pes planus, with collapse of transverse arch is more common on the non-operated side. Moreover, they report that 58.8 % of the studied patients utilized external prosthesis throughout the day and 37.5 % occasionally. Not wearing an external breast prosthesis might result in deformities of the bone and abnormalities in the body axis11. Henceforth, adjuvant treatment is an additional issue affecting posture after a mastectomy, producing weakness of postural muscles of the torso, and leading to defects of the bone17.
Our study reported that factors such as a mastectomy on the dominant side and radiotherapy treatments are the greatest precursors of muscular and postural imbalances, together with changes in static and dynamic balance, evidenced by a greater distribution of the plantar load vector on the dominant side. This is explained by pain, inflammation in adjacent muscle tissues and fascial fibrosis caused by radiotherapy, which cause a significant decrease in mobility in the lumbar, thoracic and scapular segment. These alterations are caused by body instability and asymmetry generated by the absence of the breast on the muscle chains18.
According to a meta-analysis a total of 21 out of 29 studies there is evidence that breast cancer survivors display gait and balance impairments that may result from reduced muscle strength and loss in proprioception, which are common adverse effects from breast cancer treatment such as radiotherapy and chemotherapy. Additionally, breast cancer patients appear to have worse balance when the visual and proprioceptive systems were challenged, which is the case of the feet together and one-legged positions. The review recommends to assess gait and balance during and following treatment using a force plate which better detects changes in stability19.
Evidence reported that proper foot posture and weight distribution are important elements ensuring overall postural stability. These elements have an impact on reduced mobility and balance disorders, leading to higher probability of falls20. Likewise, changes to foot shape and deformities decrease the quality of life21. Plantar load distribution is an indicator of stability in terms of postural balance and frailty22.
As exposed by Glowacka‑Mrotek et al., the posture of the foot and the load distribution are healthier in persons with good physical shape and with an active lifestyle. Frequently, women limit physical activity after mastectomy, which might be the motive for progression of structural deformities of joints and bones11.
Finally, the evidence suggests the need to improve the rehabilitation scheme for women undergoing mastectomy, which should not only approach the physical function, but contain reeducation of gait, exercises for muscular balance and improvement of dynamic and static balance. According to the guidelines of the American College of Sports Medicine, exercise is safe as well as effective for patients with cancer, and there is robust evidence about posterior effects in issues such as, health-related quality of life, fatigue, physical function, anxiety, depressive symptoms, as well as lymphedema23. The guideline, in absence of any evidence-based fall prevention studies in cancer survivors, recommend to consider standard fall prevention with exercise approaches that may be of use in advanced age21,22,23,24,25.
There is a need to develop studies with a larger study population regarding the baropodometric alterations after a mastectomy, and the possible effect of external prosthesis on the functional response. Including elements such as control group, an assessment before surgery and long-term analyses.
In conclusion, the current results for our study evidenced the unbalanced weight distribution in patients after mastectomy. Therefore, it describes the postural and muscular alterations, and the static and dynamic imbalance in breast cancer patients. The existing physical therapy approach for breast cancer patients emphasizes on shoulder mobility restrictions and lymphedema treatment, leaving behind other important comorbidities that may impact daily activities such as balance and proprioception. There is a need to improve oncology rehabilitation by promoting a comprehensive model seeking for the patient´s benefit. Physical therapy interventions should include education about biomechanical and balance alterations which could have a positive impact on life quality, favoring the patient functionality and re-adaptation to social and occupational life.
These results show the need for enlargement of the knowledge on this field and further study in oncology rehabilitation, specifically adapted to the patient needs and long-term comorbidities.
References
1. Stout NL, Silver JK, Raj VS, Rowland J, Gerber L, Cheville A, et al. Towards a national initiative in cancer rehabilitation: Recommendations from a subject matter expert group. Arch Phys Med Rehabil. 2016;97(11):2006-15.
2. WHO. Global cancer observatory [Internet]. 2020 [citado 6 de mayo de 2021]. Disponible en: https://gco.iarc.fr/
3. ASCO. Breast cancer: Statistics [Internet]. 2021 [citado 6 de mayo de 2021]. Disponible en: https://www.cancer.net/cancer-types/breast-cancer/statistics#:~:text=The%20average%205%2Dyear%20survival,with%20breast%20cancer%20is%2099%25
4. Głowacka I, Nowikiewicz T, Hagner W, Nowacka K, Sowa M, Zegarski W. Sagittal plane postural changes in female patients with breast cancer after different surgical techniques. Breast J. 2017;23(1):109-11.
5. Malicka I, Barczyk K, Hanuszkiewicz J, Skolimowska B, Woźniewski M. Body posture of women after breast cancer treatment. Ortop Traumatol Rehabil. 2010;12(4):353-61.
6. Benton MJ, Schlairet MC. Upper extremity strength imbalance after mastectomy and the effect of resistance training. Sports Med Int Open. 2017;1(5):E160-5.
7. Zehra S, Doyle F, Barry M, Walsh S, Kell MR. Health-related quality of life following breast reconstruction compared to total mastectomy and breast-conserving surgery among breast cancer survivors: a systematic review and meta-analysis. Breast Cancer. 2020;27(4):534-66.
8. Liang Y, Xu B. Factors influencing utilization and satisfaction with external breast prosthesis in patients with mastectomy: A systematic review. International Journal of Nursing Sciences. 2015;2(2):218-24.
9. Hojan K, Manikowska F, Chen BPJ, Lin CC. The influence of an external breast prosthesis on the posture of women after mastectomy. J Back Musculoskelet Rehabil. 2016;29(2):337-42.
10. Lopera-Muñeton C, Valencia-Legarda F, Bedoya-Bedoya OM, Correa-Castaño D, Páramo-Velásquez CA. Body posture and biomechanics in women after mastectomy. J Phys: Conf Ser. 2019;1418:012009.
11. Głowacka-Mrotek I, Sowa M, Siedlecki Z, Nowikiewicz T, Hagner W, Zegarski W. Evaluation of changes to foot shape in females 5 years after mastectomy: a case-control study. Breast Cancer Res Treat. 2017;163(2):287-94.
12. Głowacka-Mrotek I, Sowa M, Nowikiewicz T, Siedlecki Z, Hagner W, Zegarski W. Foot posture in female patients 5 years after breast-conserving surgery: a case–control study. Breast Cancer. 2018;25(3):325-33.
13. Manikowska F, Ozga-Majchrzak O, Hojan K. The weight of an external breast prosthesis as a factor for body balance in women who have undergone mastectomy. Homo. 2019;70(4):269-76.
14. Koralewska A, Domagalska-Szopa M, Łukowski R, Szopa A. Influence of the external breast prosthesis on the postural control of women who underwent mastectomy: Cross-sectional study. Front Oncol. 2022;12:920211.
15. Hojan K. Does the weight of an external breast prosthesis play an important role for women who undergone mastectomy? Rep Pract Oncol Radiother. 2020;25(4):574-8.
16. Jetha ZA, Gul RB, Lalani S. Women experiences of using external breast prosthesis after mastectomy. Asia Pac J Oncol Nurs. 2017;4(3):250-8.
17. Atanes AC, Dias MR, Yugo J, Filassi JR, Chada E, Alves E. Body posture after mastectomy: comparison between immediate breast reconstruction versus mastectomy alone. Physiother Res Int. 2017;22(1):34-43.
18. Ejaz A, Greenberger JS, Rubin PJ. Understanding the mechanism of radiation induced fibrosis and therapy options. Pharmacology & Therapeutics. 2019;204:107399.
19. Hsieh KL, Wood TA, An R, Trinh L, Sosnoff JJ. Gait and balance impairments in breast cancer survivors: A systematic review and meta-analysis of observational studies. Arch Rehabil Res Clin Transl. 2019;1(1-2):100001.
20. Lee DY, Seo SG, Kim EJ, Kim SJ, Lee KM, Choi IH. Inter-segmental motions of the foot in healthy adults: Gender difference. J Orthop Sci. 2016;21(6):804-9.
21. Davis AM, Galna B, Murphy AT, Williams CM, Haines TP. Effect of footwear on minimum foot clearance, heel slippage and spatiotemporal measures of gait in older women. Gait Posture. 2016;44:43-7.
22. Gomes FM, Santos KT, Silva SME, Pinho CPS, Silva A, Gomes FM, et al. Fragilidad en ancianos oncológicos en tratamiento con quimioterapia. Revista Chilena de Nutrición. 2019;46(4):384-91.
23. Campbell KL, Winters-Stone KM, Wiskemann J, May AM, Schwartz AL, Courneya KS, et al. Exercise guidelines for cancer survivors: Consensus statement from international multidisciplinary roundtable. Med Sci Sports Exerc. 2019;51(11):2375-90.
24. Stevens J, Burns E. CDC compendium of effective fall interventions: What works for community-dwelling older adults, 3rd Edition. Home and Recreational Safety, CDC Injury Center [Internet]. 2015 [citado 6 de mayo de 2021]. Disponible en: https://www.cdc.gov/homeandrecreationalsafety/falls/compendium.html
25. Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, Beil TL, Thompson JH. Interventions to prevent falls in community-dwelling older adults: A systematic review for the U.S. preventive services task force [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 [citado 6 de mayo de 2021]. Disponible en: http://www.ncbi.nlm.nih.gov/books/NBK525700/
Notas de autor
fannyvalencialegarda@fucm.edu.co
Información adicional
Conflict of interests: The authors declare that they have no conflict of interests.
Research funding: Center for Research and Business Development (CIDE).
