Original works
Received: 09 February 2021
Accepted: 03 February 2022
DOI: https://doi.org/10.36104/amc.2022.2109
Abstract
Objective: to determine which factors are related to deep vein thrombosis in patients with lower extremity cellulitis/erysipelas.
Materials and methods: a case-control study. Patients seen at Hospital Pablo Tobón Uribe and the university hospital between January 2018 and December 2019 who were diagnosed with cellulitis/erysipelas and underwent lower extremity venous Doppler. Demographic, clinical, laboratory and imaging variables were considered.
Results: altogether, 637 patients with a diagnosis of lower extremity cellulitis and erysipelas were found during the study period in both institutions. Of these, 18.5% (118 patients) had a lower extremity Doppler ultrasound ordered to rule out deep vein thrombosis, finding a total of 25 positive studies (21.19%). Out of the total sample, 56 (47.4%) were male, with a mean age of 65 years. Most of the cases (55.08%) had an intermediate risk according to the Wells scale. The most common patient factors related to thrombosis were: immobility 33%, lymphedema 29.66%, and chronic kidney disease 23.73%. Neoplasms were the factor which showed statistical significance for the presence of thrombosis OR 5 (1.64-15.16) (P=0.0056).
Conclusions: cellulitis is not a unique finding to justify carrying out a Doppler test, and the routine use of this imaging technique in the diagnostic approach is not justified if there are no other risk factors for thrombosis. (Acta Med Colomb 2022; 47. DOI:https://doi.org/10.36104/amc.2022.2109).
Keywords: Deep vein thrombosis, cellulitis, erysipelas, risk factors.
Resumen
Objetivo: determinar cuáles son los factores que se relacionan con trombosis venosa profunda (TVP) en pacientes con celulitis/erisipela en miembros inferiores.
Materiales y métodos: estudio de casos y controles. Pacientes atendidos en el Hospital Pablo Tobón Uribe y la IPS universitaria entre enero de 2018 y diciembre de 2019 con diagnóstico de celulitis/erisipela y a quienes se les realizó Doppler venoso de miembros inferiores. Se consideraron variables demográficas, clínicas, paraclínicas e imagenológicas.
Resultados: en total se identificaron 637 pacientes con diagnóstico de celulitis y erisipela de miembros inferiores en el periodo de estudio en ambas instituciones. De estos en 18.5% (118 pacientes) se solicitó ecografía Doppler de miembros inferiores para descartar trombosis venosa profunda, encontrando un total de 25 estudios positivos (21.19%). Del total de esta muestra fueron 56 hombres (47.4%) con una media de edad de 65 años. La mayoría de casos (55.08%), tuvieron riesgo intermedio según la escala de Wells. Los antecedentes más frecuentes relacionados con trombosis fueron: inmovilización 33%, linfedema 29.66%, enfermedad renal crónica 23.73%. La presencia de neoplasia fue el antecedente que demostró significancia estadística para la presencia de trombosis OR 5 (1.64-15.16) (P=0.0056).
Conclusiones: la presencia de celulitis no es un hallazgo único que justifique la realización de Doppler, y el uso de imagen de rutina dentro del abordaje diagnóstico no está justificado si no existen otros factores de riesgo de trombosis. (Acta Med Colomb 2022; 47. DOI:https://doi.org/10.36104/amc.2022.2109).
Palabras clave: Trombosis venosa profunda, celulitis, erisipela, factores de riesgo.
Introduction
Deep vein thrombosis (DVT) of the lower extremities is a highly morbid condition which leads to complications like secondary pulmonary embolism and post-thrombotic syndrome, with the main risk factors described being a hypercoagulable state, family history of thrombosis, vascular wall injury, surgery, immobility, active cancer, age, obesity, hospitalization, and the use of estrogen and progesterone 1,2. Doppler ultrasound of the lower extremities is the standard diagnostic test as it has good sensitivity and specificity and is noninvasive. However, the current problem is overuse of this tool without an adequate correlation between the clinical findings and DVT risk factors to justify its use 3,4.
The clinical findings in lower extremity cellulitis/erysipelas and extremity DVTs are similar and, in most cases, unclear. In both situations there is calf pain, edema or sensitivity, erythema and hardening of the skin with occasional changes in coloring, which makes it difficult to distinguish one condition from the other based solely on the physical exam. It is common for many patients admitted with a diagnostic suspicion of cellulitis/erysipelas (CE) to undergo Doppler ultrasound of the lower extremities to assess for the presence of concomitant DVT, a test which is very rarely positive. This suggests that the clinical predictors are not very specific, and this diagnostic tool is overused, with a high percentage of inconclusive results which are not useful and, on the contrary, increase healthcare costs 3. The objective of this paper was to determine which factors related to deep vein thrombosis in patients with lower extremity cellulitis/erysipelas justify performing Doppler imaging. The hypothesis is that a history of conditions related to hypercoagulability and venous stasis are the most significant risk factors for DVT in CE.
Materials and methods
A case-control study was performed including patients over the age of 18 who were seen in the emergency room with a diagnosis of lower extremity CE and underwent Doppler between January 2018 and December 2019. Patients with the complication of necrotizing fasciitis were excluded. Cases were defined as patients diagnosed with lower extremity CE with a documented DVT on Doppler. Controls, in turn, were defined as patients diagnosed with CE who underwent Doppler for suspected DVT, but whose study was negative for thrombosis.
A simple randomized probabilistic sample was calculated, considering the most common antecedent in prior studies: DVT, with a case prevalence of 44%. A 95% confidence interval, 80% power, 0.05 error, 1:4 case-control ratio and odds ratio (OR) of 5 required a total of 95 patients: 19 cases and 76 controls.
A pilot study was conducted initially to document the frequency of Doppler tests in the patients and a complete description of the study variables.
For bias control, a representative sample of the population, with a different severity but during the same period of time, was included, incorporating those admitted to the emergency room and hospital wards. Each investigator reviewed each institution's information and recorded variables.
Analysis plan
Using a Microsoft Excel database, data analysis was performed with the Epi Info 7.2.4 program.
Univariate analysis: a table of frequencies was constructed describing the mean and standard deviation for quantitative variables, and absolute and relative frequencies for qualitative variables.
To compare the groups of patients with and without DVT in the bivariate analysis, Chi square or Fisher's exact test were used for qualitative variables, and the OR was calculated with its respective confidence interval. The level of statistical significance was a P less than 0.05. The only quantitative variable was age, and this was not included in the bivariate analysis. Logistic regression was run to determine the effect of confounding variables and those related to the dependent variable DVT.
Results
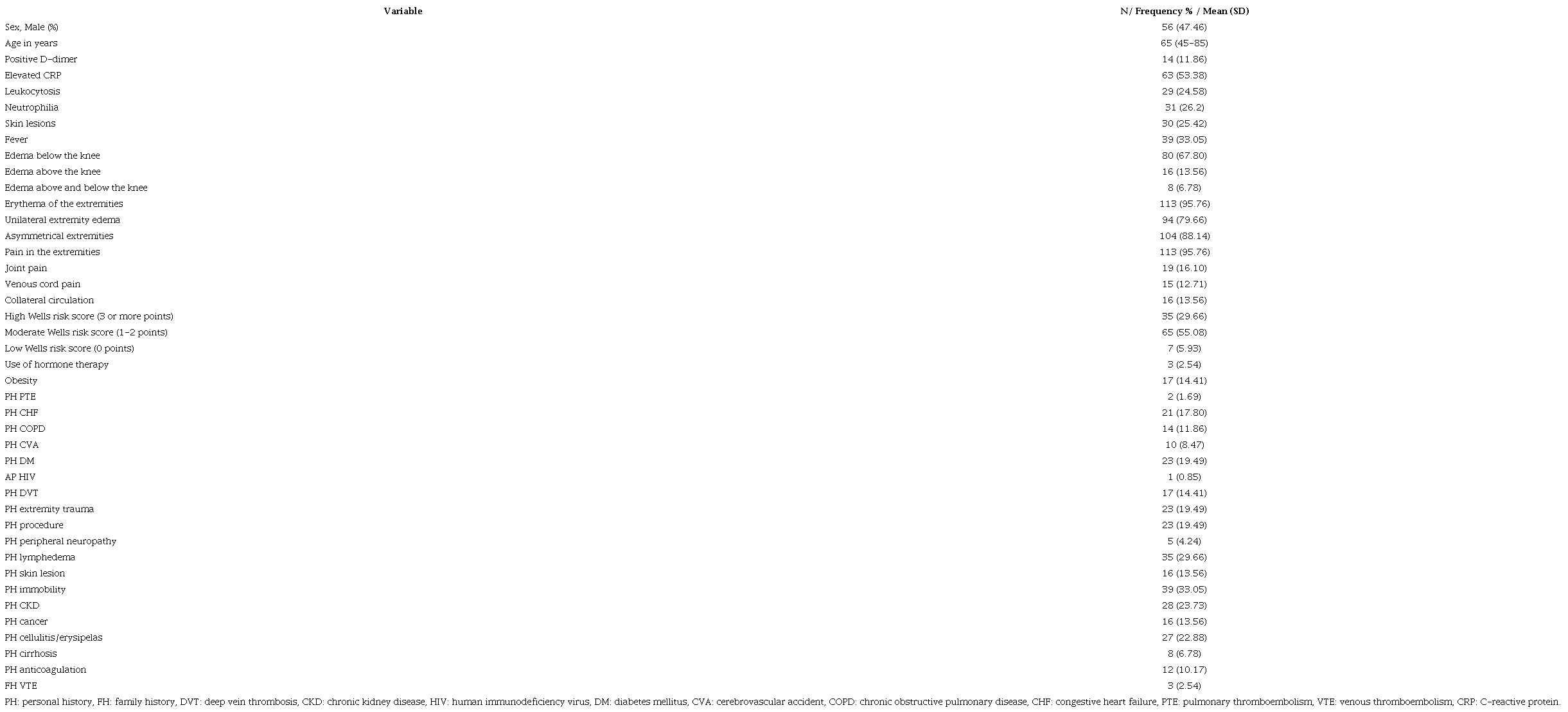
A total of 637 patients were found with a diagnosis of lower extremity CE between 2018 and 2019 in both institutions. Of these, 118 patients had a lower extremity Doppler ordered, finding a total of 25 positive cases for DVT (21.19%). The demographic, clinical and laboratory characteristics of both groups are described in Table 1. The most prevalent clinical sign was extremity pain in 95.76% of the patients, followed by extremity asymmetry in 88.14% and unilateral edema in 79.66%. Fever only occurred in 33.05%. The Wells scale was not calculated in 11 cases, with most cases (55.08%) having an intermediate risk.
Patients' demographic and clinical characteristics (n= 118).
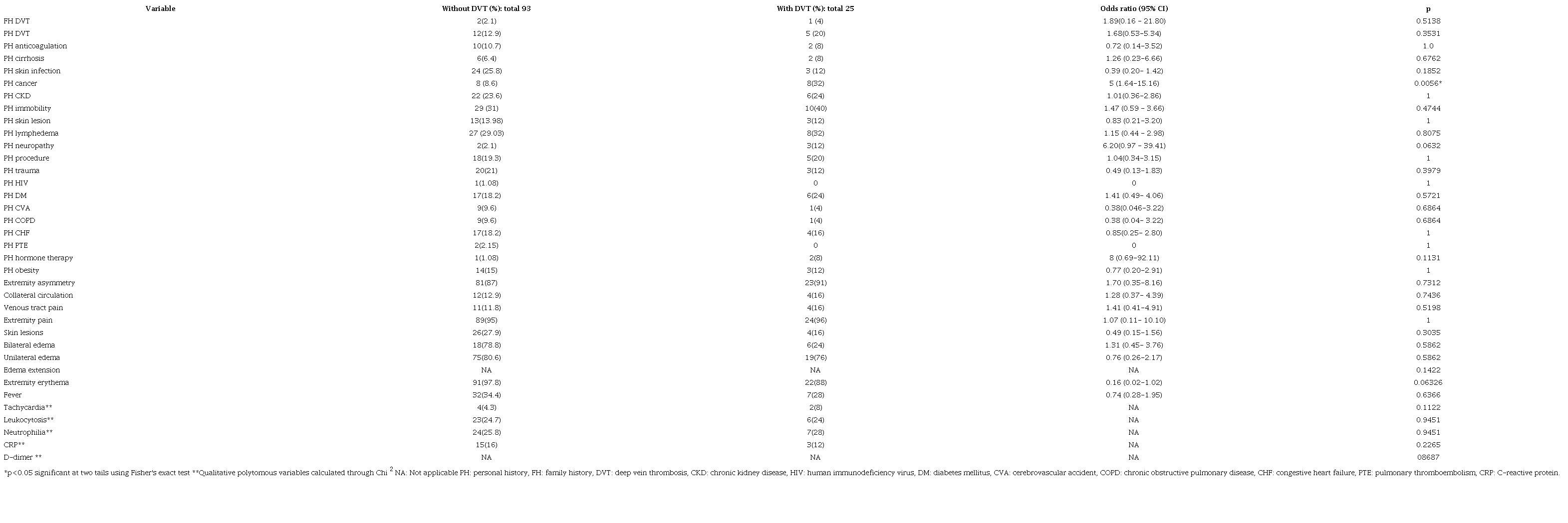
Patients were divided into those with and those without DVT. A bivariate analysis was then carried out to compare the DVT risk factors in both groups, finding an increased risk not due to chance for a history of cancer, with an OR of 5 (1.64-15.16) (P= 0.0056). None of the other clinical or laboratory variables showed a statistically significant difference, although it is worth noting that a history of peripheral neuropathy had an OR of 6.2 with a lower limit of the confidence interval very close to the unit, but not statistically significant (0.97-39.41) (P= 0.063). Likewise, limb erythema had an OR of 0.16 (0.02-1.02) (P=0.063) with the upper limit of the interval close to 1 (Table 2).
Bivariate analysis.
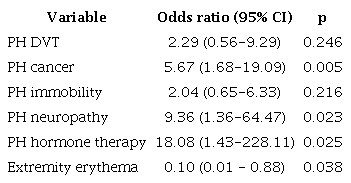
For the logistic regression analysis, the effect of variables related to a known history of conditions that increase the probability of venous thromboembolic disease such as: a history of immobility, cancer, use of hormone therapy, personal history of DVT, and peripheral neuropathy was established with a 95% confidence level; as was the effect of potentially confounding variables related to physical exam findings: extremity erythema, not including those with probable collinearity such as asymmetrical edema and extremity pain. The DVT-related factors which showed a statistically significant difference were hormone therapy, with an OR of 18.08 (1.43-228.11), a history of cancer with an adjusted OR of 5.67 (1.68-19.09), and peripheral neuropathy with an adjusted OR of 9.36 (1.36-64.47). No relationship was found with limb erythema, with an OR of 0.10 (0.01-0.88) (Table 3).
Multivariate logistic regression analysis Análisis por regresión logística multi-variable.
Discussion
The prevalence of DVT in concomitant cellulitis or erysipelas ranges from 0-15% 5,6. We found a percentage slightly greater than 21%. Maze et al. reported 15% of patients with cellulitis who underwent Doppler, of whom only 0.5% were positive for DVT 7, and a systematic review and a meta-analysis published in 2013 included 1,054 patients with cellulitis/erysipelas, of whom 18 had DVT, with a general incidence rate of 2.1%, but all showed a low concurrence of both conditions 8. In addition, we found that Doppler ultrasound was performed in 18.5%, similar to and even lower than what was reported in other articles. Afzal et al. published a retrospective study in patients with extremity cellulitis in whom the percentage of Doppler tests performed was close to 70%, with only 6% of these positive for DVT 4. This shows that this diagnostic tool is also overused in our setting, increasing unjustified costs for the healthcare system.
Specifically for lower extremity cellulitis/erysipelas, the risk factors for concomitant thrombosis are not clearly defined, as some have not been shown to be related in the studies, which explains the limited usefulness of the usual clinical prediction models for DVT 4-8. Afzal et al. found that a history of thrombosis, prior cerebrovascular accident, calf edema and hypertension were statistically significant for concurrence of both conditions 4. In our study, we found that a history of cancer was a significant and precise variable for DVT in a cellulitis context. Although it is a known risk factor for thrombosis, its association with concurrent infection had not been shown in other reports 4-8. Likewise, a history of peripheral neuropathy and hormone therapy showed an association on multivariate analysis after adjusting for variables related to DVT. Regarding clinical signs, we did not find that acute phase reactants or inflammatory or measurement changes in the limb were indicative of DVT. This finding was similar to what was reported in other cohorts 8, but it is interesting that, in our study, limb erythema behaved as a factor against a DVT diagnosis, showing statistical significance after adjusting for possible confounding variables, which generates a hypothesis which will need to be confirmed in subsequent studies. While infection may be a risk factor for thrombosis, we found, as did previous articles, that it should not be the only finding to justify performing a Doppler test. Given that the occurrence of both diagnoses together is rare, most authors suggest that, in the absence of known DVT risk factors, routine use of this imaging is unnecessary within the initial diagnostic approach 5-7. As a case-control study, this paper has limitations, as it is subject to selection and information biases, and we cannot determine the percentage of patients with cellulitis who did not undergo Doppler and did have a DVT, which underestimates the incidence of this diagnosis. Also, the study only included two years of follow up at two institutions in the city, with a small sample size, which could explain the lack of association of some of the variables. However, our results are important since they propose an initial idea of the coexistence of these two conditions and potentially related factors, and provide guidelines to improve clinical practice with an appropriate use of this resource.
Conclusions
-
The finding of cellulitis alone does not justify performing a Doppler, and the routine use of this imaging within the diagnostic approach is not justified if there are no other risk factors for thrombosis.
-
This paper suggests that a history of cancer, peripheral neuropathy and hormone therapy are clinical predictors of associated DVT in the context of soft tissue infection, which can be taken into account in daily practice.
-
We hypothesize possible variables related to the concomitant presence of DVT in cellulitis, but additional prospective studies are needed to validate these findings.
Acknowledgements
The authors thank Hospital Pablo Tobón Uribe and IPS Universitaria Medellin for allowing this study to be performed.
References
Kahn S, Lim W, Dunn A, Cushman M, Dentali F, Akl E. Et al. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl): e195S-e226S
Di Nisio M, van Es N, Büller H. Deep vein thrombosis and pulmonary embolism. Lancet. 2016;388(10063):3060-3073
Heit J, Spencer F, White R. The epidemiology of venous thromboembolism. J Thromb Thrombolysis. 2016;41(1):3-14.
Afzal M, Saleh M, Razvi S, Hashmi H, Lampen R. Utility of Lower Extremity Doppler in Patients with Lower Extremity Cellulitis: A Need to Change the Practice? South Med J 2015 Jul;108(7):439-44
Bersier D, Bounameaux H. Cellulitis and deep vein thrombosis: a controversial association. J Thromb Haemost 2003;1:867Y868
Bendick P. Cellulitis and the prevalence of deep vein thrombosis. J Diagn Med Sonog 1996; 12:170-74
Maze M, Skea S, Pithie A, et al. Prevalence of concurrent deep vein thrombosis in patients with lower limb cellulitis: a prospective cohort study. BMC Infect Dis 2013; 13:141.
Gunderson C, Chang J. Risk of deep vein thrombosis in patients with cellulitis and erysipelas: a systematic review and meta-analysis. Thromb Res. 2013;132(3):336-40.
Author notes
* Correspondencia: Mónica Zuluaga-Quintero. Medellín (Colombia). E-Mail: mzulu28@hotmail.com
