Case presentation
Sporadic lymphangioleiomyomatosis
Linfangioleiomiomatosis esporádica
Sporadic lymphangioleiomyomatosis
Acta Medica Colombiana, vol. 48, no. 3, e10, 2023
Asociacion Colombiana de Medicina Interna
Received: 21 December 2022
Accepted: 01 April 2023
Abstract:
Lymphangioleiomyomatosis is a rare multisystemic disease which mainly affects women of reproductive age and is distinguished by diffuse cystic pulmonary involvement. It may present sporadically or in association with tuberous sclerosis complex. Lymphangioleiomyomatosis is also characterized by the presence of extrapulmonary angiomyolipomas, lymphatic tumors, chylothorax and pneumothorax. We present the case of a 39-year-old patient who had had signs and symptoms of pulmonary disease since adolescence, predominantly cough and progressive dyspnea, in addition to fatigue. She had multiple hospitalizations and various diagnoses and treatments without improvement. The clinical history and a high-resolution tomography of the lungs led to a suspicion of the disease, and measurement of vascular endothelial growth factor-D contributed to the diagnosis, with no need for a lung biopsy. (Acta Med Colomb 2022; 48. DOI:https://doi.org/10.36104/amc.2023.2815).
Keywords: Lymphangioleiomyomatosis, tuberous sclerosis complex, pulmonary cysts, pulmonary hypertension, vascular endothelial growth factor-D.
Resumen:
La linfangioleiomiomatosis es una enfermedad rara multisistémica, que afecta principalmente a mujeres en edad reproductiva y tiene como distintivo un compromiso pulmonar quístico difuso. Se puede presentar de forma esporádica o asociada con el complejo de la esclerosis tuberosa. La linfangioleiomiomatosis se caracteriza además por la presencia de angiomiolipomas extrapulmonares, tumores linfáticos, quilotórax y neumotórax. Se presenta el caso de una paciente de 39 años, que desde su adolescencia viene presentando signos y síntomas de enfermedad pulmonar dados principalmente por tos y disnea progresiva, además de fatiga. Múltiples hospitalizaciones y diversos diagnósticos y tratamientos sin mejoría. Por la historia clínica y la tomografía de alta resolución pulmonar se sospechó la enfermedad, y la determinación del factor de crecimiento endotelial vascular-D contribuyó en el diagnóstico sin nece sidad de biopsia pulmonar. (Acta Med Colomb 2022; 48. DOI:https://doi.org/10.36104/amc.2023.2815).
Palabras clave: Linfangiomiomatosis, complejo de esclerosis tuberosa, quistes pulmonares, hipertensión pulmonar, factor de crecimiento endotelial vascular-D.
Introduction
The term sporadic lymphangioleiomyomatosis (S-LAM) is used for patients with LAM which is not associated with the tuberous sclerosis complex (TSC), while TSC-LAM refers to LAM associated with TSC. This rare disorder is part of the perivascular epithelioid cell neoplasms, or PEComas, which are mesenchymal neoplasms made up of histologi cally and immunohistochemically distinctive epithelioid or fusiform cells and are immunoreactive for smooth muscle and melanocyte markers 1.
The diagnosis of LAM is often overlooked and, therefore, there is a significant delay between the onset of the disease and its definitive diagnosis. Any disease showing cysts in the lungs may look like LAM, which is why a lung biopsy has been essential for accurate diagnosis 2.
In the past, biopsies were a common approach to diag nosing LAM; now, there has been a paradigm shift toward less invasive methods that circumvent this procedure, es pecially for S-LAM with no extrapulmonary involvement, as in our case.
Our patient was diagnosed using her medical history, imaging and, mainly, by measuring vascular endothelial growth factor-D (VEGF-D). As far as we know, this is the first time in our country that this factor has been measured for this purpose.
Case presentation
This was a 39-year-old woman from the rural area of the city of Florencia (Caquetá). She was married, with no miscarriages, no children, and no contraceptives; she was a non-smoker and did not use psychoactive substances.
She had a SARS-CoV-2 infection in 2021. She had had difficulty breathing and an occasional cough since the age of 12. She had been hospitalized on several occasions for suspected tuberculosis, but repeated microscopy tests and tuberculin tests were nonreactive, with negative cultures. She was hospitalized several times in Florencia and the city of Neiva. A bronchoscopy with aspirate analysis was not relevant. She reported episodes of pneumonia and one episode of left pneumothorax. She had never had a lung biopsy. She was left with a diagnosis of pulmonary fibrosis of unknown etiology. She was on home oxygen at 2 L/min.
She was admitted with respiratory difficulty and inter costal retractions, low oxygen saturation (88% on 2 L/min of oxygen), oriented and conscious. She had an mMRC 4 dyspnea score, WHO-FC III, with cough and purulent spu tum; on auscultation, she had decreased breath sounds and diffuse crackles; she was afebrile and tachycardic at 124 bpm, with mild nail clubbing (Figure 1).

Figure 1
Signs of nail clubbing.
Laboratory tests were within normal limits, including the following: antinuclear antibodies, extractable nuclear anti-bodies, antineutrophil cytoplasmic antibodies, complement C3 and C4, rheumatoid factor, HIV, CA 125, VDRL, HBsAg, and anti-HCV. Abnormal laboratory tests included the leuko cyte count: 17,800 per microliter with 80.8% nuetrophilia; proBNP: 1,020 pg/mL; and hemoglobin and hematocrit 16.3 g/dL and 54.1%, respectively. The initial arterial blood gases showed: pH 7.31, pCO2 80, pO2 61, HCO3- 40.3, and SaO2 88. The sputum culture grew multisensitive Pseudomonas aeruginosa. Spirometry showed a mixed pattern.
The following tests were not performed: diffusing capacity of the lungs for carbon monoxide (DLCO), serum protein electrophoresis and free light chain quantification, as they are not available in our setting.
Pulmonary hypertension was documented through a suggestive echocardiogram (LV: septal flattening, D sign; RV: dilated chambers, pulmonary artery dilation at 32 mm, PASP 53 mmHg) and proven with a right catheterization (pulmonary artery systolic pressure 52 mmHg, right atrial pressure 12 mmHg, wedge pressure 11 mmHg, generalized hypokinesia and 27% RVEF).
An abdominal-pelvic computed axial tomography (CAT) and head CAT were normal. The chest CAT is shown in Figure 2.
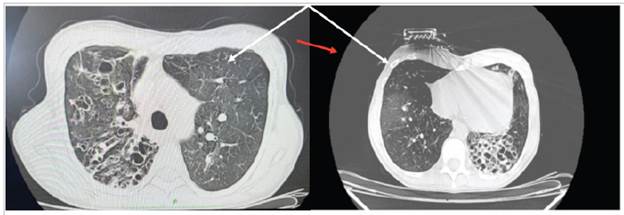
Figure 2
A high-resolution CAT without contrast. Axial plane. Different-sized cystic images. The cysts tend to be round or oval but may be polygonal (red arrow) when there is severe paren chymal involvement. Septal thickening, fibrous scar tracts, bronchiectasis, nodules and ground glass (white arrow) can be seen.
In light of suspected LAM, VEGF-D was ordered at an out-of-town laboratory (Synlab). The value reported was 155.3 pg/mL (verified with the laboratory), which was not significant; therefore, the sample was sent to the Translational Trial Development and Support Laboratory (TTDSL) at Cincinnati Children's Hospital, Ohio (USA), in collabo ration with the LAM Foundation and taking into account the proper sample transport instructions. The new report indicated 1,533 pg/mL (diagnosis > 800 pg/mL). Sirolimus 1 mg/day was added to the usual treatment.
Discussion
The most common signs and symptoms of the disease are caused by pulmonary involvement in S-LAM. Neurocutaneous findings (angiofibromas, shagreen patches, cortical tubercles, seizures and cognitive impairment, among others) are typical of TSC-LAM and are not found in S-LAM 3.
The true incidence and prevalence of S-LAM are unknown, as the available epidemiological data are observational and often include patients with TSC. Consequently, clinical experience and most studies confirm that the sporadic LAM variant is rare and almost exclusively affects women, but many have not yet been diagnosed 4. Previous estimates suggested a rate of one per million in the general population; however, more recent data indicate higher rates, which may reflect advances in recognizing and diagnosing the disease. For example, the LAM Foundation estimated a prevalence of 3-5 per million women, but approximately 10-15% of the patients registered in the foundation report having TSC 5.
The main histopathological abnormality in LAM is prolif eration of atypical smooth muscle-like cells (LAM cells). In the lungs, LAM cells are associated with multiple cysts 2.
Dyspnea on exertion is the most common presenting symptom in LAM. As dyspnea is nonspecific and common, and LAM is rare, women are often labeled with a different diagnosis before suspecting LAM.
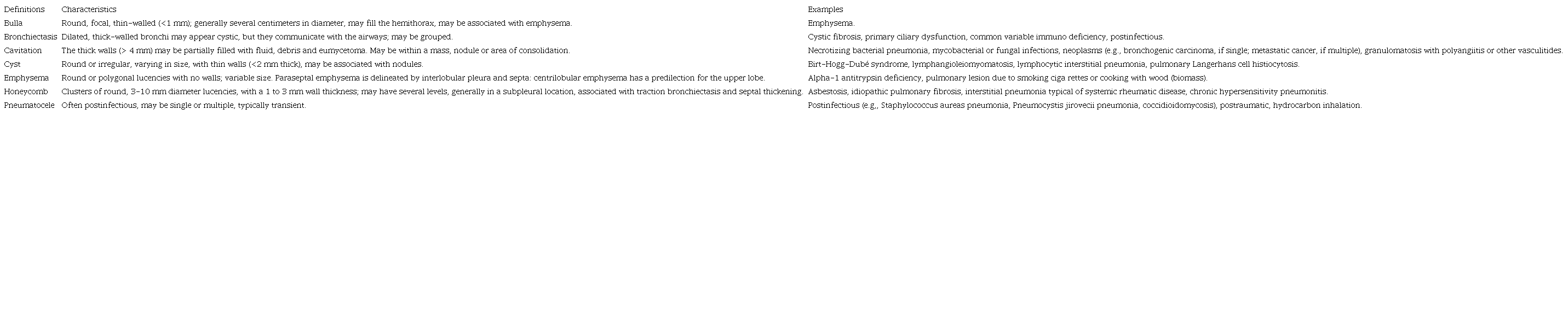
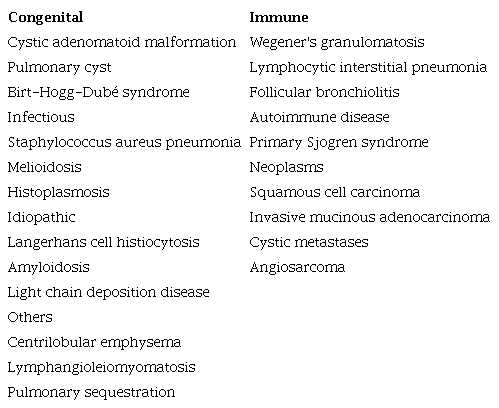
There are a variety of pulmonary diseases whose predominant CAT finding is cysts. A cyst is a "round parenchymal transparency or a low attenuation area with a well-defined interface with the normal lung" (6, translated). The differential diagnosis of these diseases is based on the number, size, shape and distribution of these cysts, as well as other associated findings. The characteristic LAM cysts are thin-walled, diffuse, rounded, well-defined, bilateral and with no lobe predominance. The cysts are generally 2-5 mm large but may be larger. They may be round or oval but may become polygonal with severe parenchymal involvement. Small centrilobular nodules have been reported, correspond ing to hyperplastic muscle or pneumocyte hyperplasia. Focal ground-glass opacities may be due to smooth muscle proliferation, and lymphatic obstruction may cause septal thickening 6,7. In the Japanese study, the frequency of pulmonary nodules was higher than in previous reports 8. In our case, we did not find what is typically described; there was more structural disorganization. While the accuracy of a LAM diagnosis based on high-resolution CAT is high for LAM experts 7, we believe that basing the diagnosis solely on the CAT is inadvisable for clinical decision making. A reliable clinical diagnosis of S-LAM is possible when the cystic changes on the CAT are typical for LAM. But we must remember that not all cystic lung diseases are LAM, but all LAM, with time, develops pulmonary cysts. However, we must also be prudent, because not all pulmonary parenchymal transparencies are cysts; there are certain conditions which mimic them (Table 1). Table 2 shows some of the main causes of cystic lung lesions.
Given the serum VEGF-D biomarker' s good performance and taking the recommended diagnostic threshold (>800 pg/mL) for its sensitivity and specificity of 73-100%, respectively, rules out other pulmonary cystic lung diseases which are commonly considered in the differential diagnosis, as they do not significantly elevate the VEGF-D, and this avoids 70% of biopsies 9. Studies so far have not found false positives, but a negative result does not rule out the diagnosis 9,10.
The following are notable in this case:
- 1. The chest CAT does not show the typical images found in these patients, but sometimes what is typical is not what is usual in the real world. We believe that we should not rule out the disease if we do not have the so-called "typical" images, especially if we do not have a radi ologist who is an expert in pulmonary cysts or LAM. When in doubt, a biomarker should be ordered before performing a biopsy. In our case, we had atypical images with typical VEGF-D levels from a LAM sensitivity and specificity perspective 10. In patients with S-LAM, like our patient, and with no other manifestation like renal angiomyolipomas, chylous fluid accumulation or TSC, a diagnosis cannot be made using high-resolution CAT, because the precision is estimated to be < 80% with expert radiologists 11.
- 2. The finding of Group 3 pulmonary hypertension. It has been described as precapillary and is generally an uncommon finding in people with LAM, < 7%, and, when found, is mild 12, unlike our case, which is why the di agnosis was questioned before obtaining the VEGF-D. A lung biopsy was proposed, which the patient refused after learning the benefits and risks of the procedure. Pulmo nary involvement has been reported to be more severe in S-LAM 12. Our patient's pulmonary hypertension was likely due to hypoxic pulmonary vasoconstriction with pulmonary vascular bed remodeling, along with vascular involvement due to inflammatory parenchymal fibrosis caused by repetitive infections, together with bronchial damage due to LAM cell and lymphatic proliferation, in which chronic inflammation tends to complicate the disease. Keeping in mind that LAM patients show pro gressive cystic destruction of the lung parenchyma.
- 3. Nail clubbing is not generally one of the physical findings in LAM 13; however, it may have been found in our patient due to chronic cardiopulmonary involvement.
- 4. A mixed pattern on spirometry. This is not usual, either; it only occurs in less than one-fourth of cases. Most are obstructive, followed by normal 13.
- 5. Two different VEGF-D results. In the first test, we do not know if correct sample packaging and processing pro cedures were followed. This is why another report was sought from a more sophisticated laboratory specialized in these areas, given the persistent clinical suspicion.
- 6. Recurrent pneumothorax, according to different authors, is characteristic of LAM, with an incidence of 61 to 81% 13. This was not a finding in our case, either; according to her history, she had only had one episode of pneumothorax.
In conclusion, we have a patient with S-LAM diagnosed by high VEGF-D levels, but who does not have the usual clinical and tomographic characteristics reported in the literature. Therefore, the disease should not be ruled out in patients who do not have the described characteristics, until the diagnostic tools have been exhausted, especially the serum biomarker. In appropriate clinical situations, the VEGF-D test is a significant advance in diagnosis and current effective treatment, and may make a lung biopsy unnecessary for diagnosing LAM. While there is no cure, living with the disease is very different today than in the past; where there was anxiety and fear there is now hope - it is no longer a death sentence.
What exists today is an unmet need for additional bio-markers of disease activity and/or response to treatment. These biomarkers would allow personalized and precision clinical care in the future.
Ethical aspects
For this article, informed consent was obtained from the patient according to the ethical principles contained in the Declaration of Helsinki. The article was also approved by the Ethics Committee at Clínica Mediláser, Florencia branch, Florencia, Colombia.
References
Thway K, Fisher C. PEComa: morphology and genetics of a complex tumor fami ly. AnnDiagnPathol. 2015;19(5):359-68. doi: 10.1016/j.anndiagpath.2015.06.003.
Kalassian K, Doyle R, Kao P, Ruoss S, Raffin T. Lymphangioleiomyomatosis: new insights. Am J Respir Crit Care Med. 1997;155(4):1183-1186.
Matsui K, Tatsuguchi A, Valencia J, Zu-xi Y, Bechtle J, Beasley MB, et al. Extrapulmonary lymphangioleiomyomatosis (LAM): clinicopathologic features in 22 cases. Hum Pathol. 2000; 31(10):1242-8. doi: 10.1053/hupa.2000.18500.
Harknett E, Chang W, Byrnes S, Johnson J, Lazor R, Cohen M, et al. Use of variability in national and regional data to estimate the prevalence of lymphangioleiomyomatosis. QJM: An International Journal of Medicine. 2011; 104(11): 971-979. doi.org/10.1093/qjmed/hcr116
The LAM Foundation. https://www.thelamfoundation.org/Newly-Diagnosed/Learning-About-Lam/About-LAM (Consultado el 8 de noviembre de 2022).
Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697-722. doi: 10.1148/radiol.2462070712.
Seaman DM, Meyer CA, Gilman MD, McCormack FX. Diffuse cystic lung disease at high-resolution CT. AJR Am J Roentgenol. 2011;196(6):1305-11. doi: 10.2214/AJR.10.4420.
Tobino K, Johkoh T, Fujimoto K, Sakai F, Arakawa H, Kurihara M, et al. Computed tomographic features of lymphangioleiomyomatosis: evaluation in 138 patients. Eur J Radiol. 2015;84(3):534-541. doi: 10.1016/j.ejrad.2014.12.008.
Young LR, Vandyke R, Gulleman PM, Inoue Y, Brown KK, Schmidt LS, et al. Serum vascular endothelial growth factor-D prospectively distinguishes lymphangioleiomyomatosis from other diseases. Chest. 2010; 138(3):674-81. doi: 10.1378/chest.10-0573.
McCormack FX, Gupta N, Finlay GR, Young LR, Taveira-DaSilva AM, Glasgow CG, et al. ATS/JRS Committee on Lymphangioleiomyomatosis. Of ficial American Thoracic Society/Japanese Respiratory Society Clinical Practice Guidelines: Lymphangioleiomyomatosis Diagnosis and Management. Am J Respir Crit Care Med. 2016; 194(6):748-61. doi: 10.1164/rccm.201607-1384ST.
Gupta N, Meraj R, Tanase D, James LE, Seyama K, Lynch DA, et al. Accuracy of chest high-resolution computed tomography in diagnosing diffuse cystic lung diseases. Eur Respir J. 2015;46(4):1196-9. doi: 10.1183/13993003.00570-2015
Freitas CSG, Baldi BG, Jardim C, Araujo MS, Sobral JB, Heiden GI, et al. Pulmonary hypertension in lymphangioleiomyomatosis: prevalence, severity and the role of carbon monoxide diffusion capacity as a screening method. Orphanet J Rare Dis. 2017;12(1):74. doi: 10.1186/s13023-017-0626-0.
Ryu JH, Moss J, Beck GJ, Lee JC, Brown KK, Chapman JT, et al. NHLBI LAM Registry Group. The NHLBI lymphangioleiomyomatosis registry: character istics of 230 patients at enrollment. Am J Respir Crit Care Med. 2006;173(1):105-11. doi: 10.1164/rccm.200409-1298OC
Author notes
* Correspondencia: Santiago Campbell-Silva. Florencia (Colombia). E-Mail: santiago.campbell@gmail.com