CASE REPORTS
Lingual frenotomy in a newborn, from diagnosis to surgery: a case report
Lingual frenotomy in a newborn, from diagnosis to surgery: a case report
Revista CEFAC, vol. 20, no. 2, pp. 258-262, 2018
ABRAMO Associação Brasileira de Motricidade Orofacial
Received: 23 August 2017
Accepted: 08 December 2017
ABSTRACT: This report describes the diagnostic approach and frenotomy in a newborn with breastfeeding difficulty, and the observation and analysis during the following 6 months. The patient was delivered normally and without complications, but showed breastfeeding difficulty during her first 5 days of life. The protocol proposed by Martinelli in 2013 was used to evaluate the lingual frenulum. After applying the protocol, the newborn was determined to require a frenotomy and the urgery was performed. The patient was reassessed using the protocol immediately after surgery and again 24 hours latter. There were improvements in the protocol scores at both reassessments. The newborn was observed and analyzed during the next six months by collecting monthly data from the vaccination card and by asking the mother for information. She was given no food supplements, pacifiers, nor sucked the thumbs, and was fed only breast milk and presented an age-appropriate weight gain. We conclude that the diagnosis using the Martinelli protocol is of fundamental importance to recognizing the need for early intervention and that the frenotomy helped improve the patient’s breastfeeding and swallowing capacity.
Keywords: Lingual Frenulum, Surgery, Pediatric Dentistry.
Introduction
Breastfeeding is directly related to sucking and swallowing, which should work in a coordinated way with breathing. Tongue movement plays a fundamental role in these actions. Any restriction of the free movement of the tongue may compromise these functions, contributing to early weaning, low weight, and impairment in the development of the baby.
Ankyloglossia, also known as tongue-tie, occurs when a part of the tissue in the sublingual region that should have undergone apoptosis during embryonic development remains, restricting lingual movement1.
Studies using ultrasonography have demonstrated the importance of tongue movement for milk flow during breastfeeding2.
Abnormal movement of the tongue during sucking has been indicated as a cause of persistent pain in the nipples, injuries, and difficulty in sustaining the baby’s hold during breastfeeding3.
Considering the importance of tongue movement for several functions of the stomatognathic system, the normal function of the tongue without restrictions is crucial for breastfeeding. We observed a clinical case in a newborn from diagnosis to surgery and followed-up the baby until her sixth month of life.
Case Presentation
We evaluated a healthy 5-day-old newborn female born vaginally. According to the mother's report, the patient was unable to breastfeed and required food supplementation, which the mother offered in a bottle (chuca) as the newborn was weeping, choking frequently, and wanting to suck constantly. This study was approved by the Research Ethics Committee of the Castelo Branco University, Unicastelo, number 32853505/10.
Lingual Frenulum Evaluation
The lingual frenulum was evaluated using the Lingual Frenulum Evaluation Protocol with scores for babies, proposed by Martinelli et al.4. The protocol consists of three parts: a clinical history; anatomical and functional evaluations; and nutritive and non-nutritive sucking evaluations. Each part has an independent score and can be applied separately.
Surgical Procedure
After screening according to the Lingual Frenulum Evaluation Protocol for babies5, we found that the frenulum interfered with tongue movement during breastfeeding, and surgery to release the frenulum was indicated.
The newborn was placed in a supine position and physically restrained with a sheet, immobilizing the elbows next to the body.
In the preoperative period, the frenulum was visualized using the inspection maneuver, and the baby was anesthetized with eye drop anesthetic (Figure 1).

Figure 1:
Clinical aspect of the lingual frenulum by means of digital evidence maneuver and anesthesia
The oral cavity of the newborn was opened by an assistant, and a surgical cannula was used for individualization and better visualization of the lingual frenulum (Figure 2).

Figure 2:
Section of the lingual frenulum with knife scalpel 15 using tentacanula
Subsequently, an incision was made from the free portion of the frenulum to the base of the tongue using a number 15 surgical scalpel. To facilitate hemostasis, the site was pressed with a gauze, contributing to tissue divulsion. Crying was observed only when the baby was under physical restraint. After the procedure, the baby was released and placed on the mother's chest (Figure 3). After 5 minutes of sucking, the patient was removed from the mother's chest for visualization.

Figure 3:
Newborn placed in the breast immediately after the surgical procedure
No bleeding was observed (Figure 4). The parents were advised that a whitish lesion resembling a cold sore might appear at the incision site early in the healing process; this was a normal part of the healing process. The baby was followed up weekly for a two-week period to visualize cicatrization, and then monthly until 6 months of age. Each month the newborn returned, the guidelines on breastfeeding were reinforced and the doubts raised by the parents were clarified.

Figure 4:
Postoperative clinical appearance after 5 minutes of breastfeeding
Results
The newborn scored a 9 on items 1, 2, 3, and 4 of the anatomical and functional evaluation of interference of the frenulum in tongue movement (Figure 5). The protocol was reapplied immediately after and 24 hours after the frenotomy. An improvement in the protocol scores was observed immediately after and again at 24 hours after surgery (Figures 5 and 6).
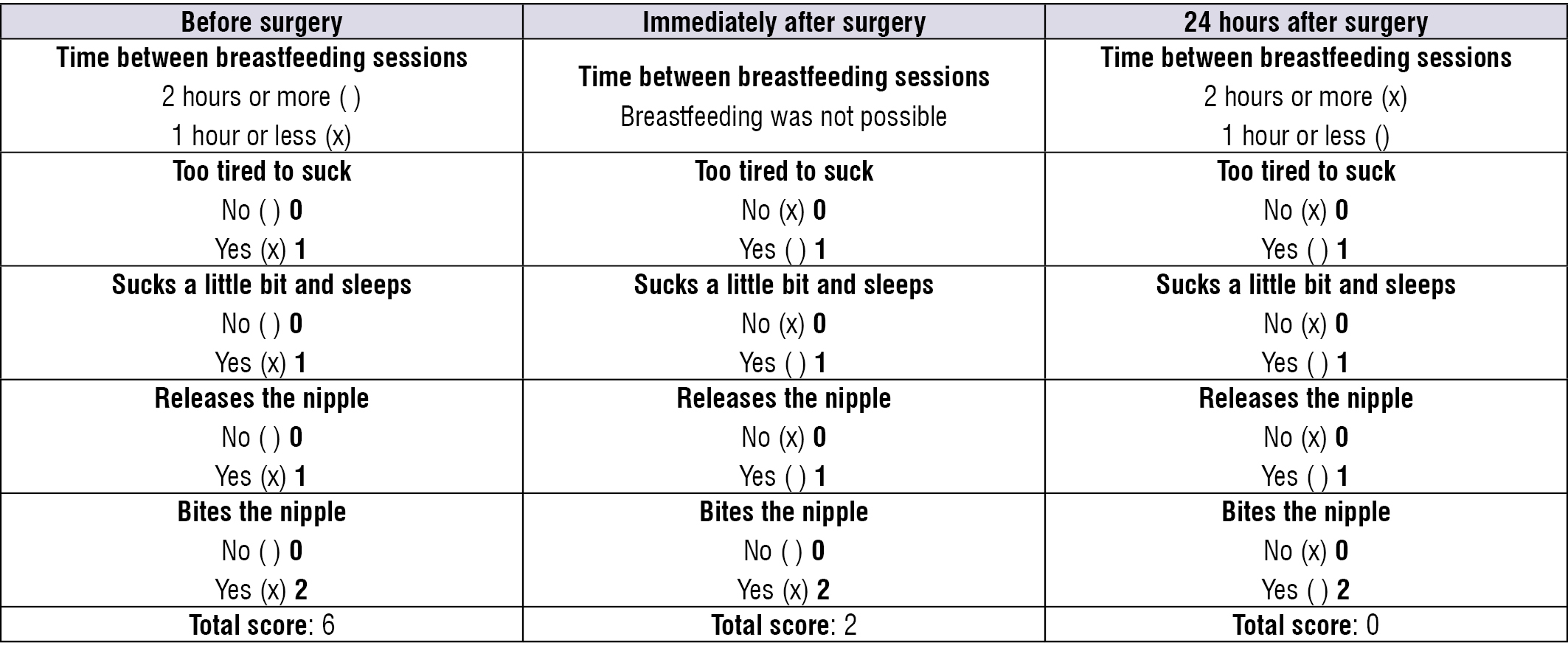
Figure 5:
Responses to the clinical history section of the protocol provided by the mother before, immediately after, and 24 hours after surgery
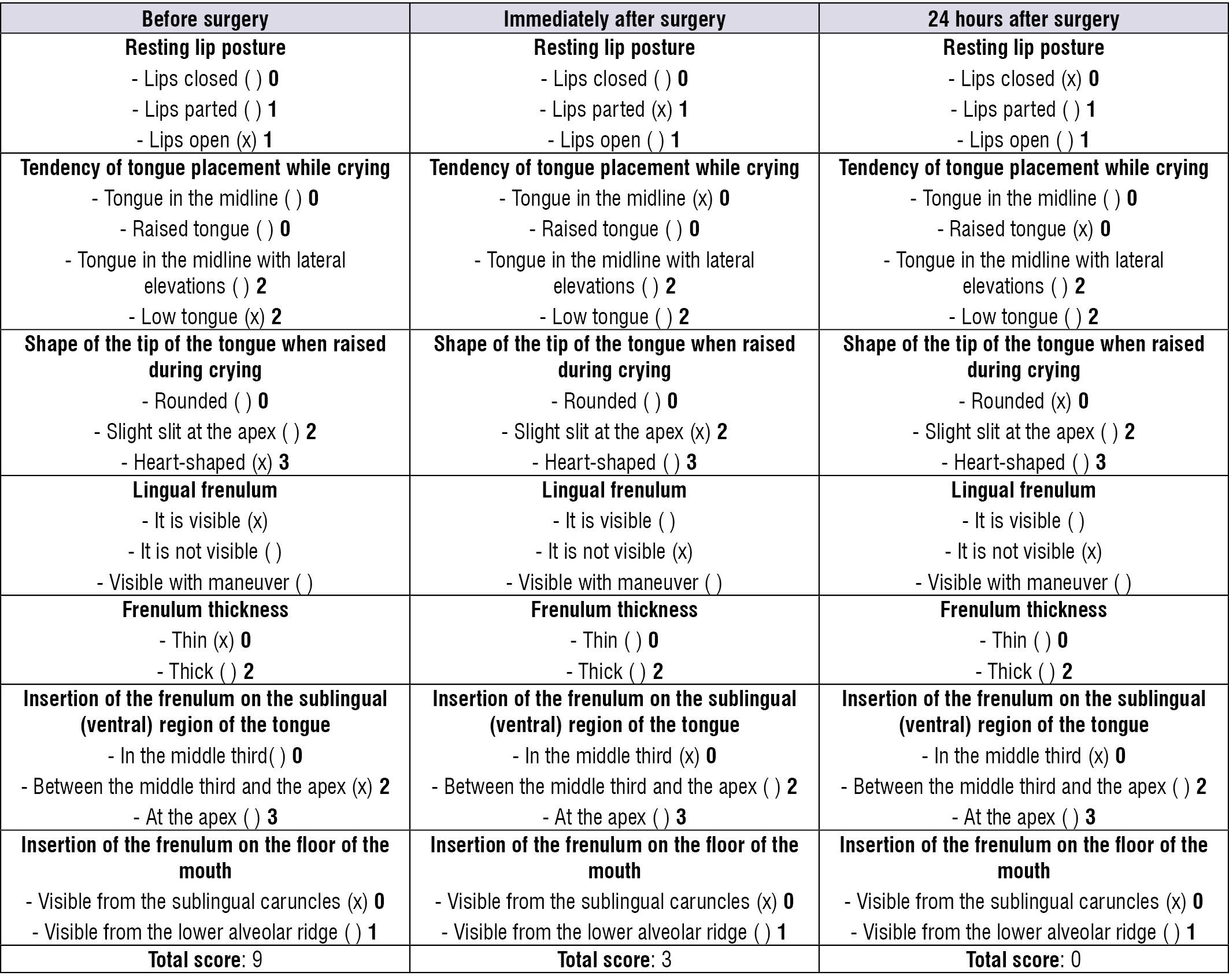
Figure 6:
Results of the anatomical and functional evaluation section of protocol items 1, 2, 3, and 4 before, immediately after, and 24 hours after surgery
The newborn was followed up monthly for six months; we collected data from the vaccination card and addressed questions to the mother. We observed that the patient did not use food supplements, pacifiers, and/or finger sucking, but was exclusively breast-fed and had a satisfactory weight gain for her age.
Discussion
The literature correlates ankyloglossia with breastfeeding difficulties reported by mothers, but no studies correlating sucking and swallowing functions (which require tongue movements) with the anatomical variations of the lingual frenulum4,5 were observed during the evaluation of the newborn using the protocol proposed by Martinelli et al.4 We observed the presence of ankyloglossia (also known as tongue-tie). It occurs when a part of the tissue in the sublingual region that should have undergone apoptosis during embryonic development remains, which restricts tongue movement1; the mothers’ complaints of being unable to breastfeed may be attributed to this restricted movement. According to Brookes and Bowley6, babies with changes in the tongue may have difficulty sucking, which can affect both the baby and the mother. The most often reported problems include difficulty holding (including signs of frustration, such as shaking the head), breast pain (including bleeding, cracked, or ulcerated nipples), and signs of dissatisfaction on the part of the baby, such as frequent or continuous breastfeeding and unrest. Francis et al.7 also report that ankyloglossia might interfere with the baby’s hold on the nipple, which makes breastfeeding difficult. Improvements were observed immediately after surgery and in the first 24 and 72 hours, as shown in Figures 5 and 6, which correlates with the results reported by Sakalidis et al.2 The study used ultrasonography and demonstrated the importance of tongue movement for milk flow during breastfeeding5.
After surgery, there was an improvement in holding and a decrease in nipple biting during breastfeeding, minimizing the mother's complaints of pain. These results agree with those of the study by McClellan et al.3, which reported that abnormal movement of the tongue during sucking has been indicated as a cause of persistent pain in the nipple, injuries, and difficulty sustaining the baby’s hold during breastfeeding3.
The Canadian Agency for Drugs and Technologies in Health8 reports that the benefits of surgical correction of ankyloglossia are uncertain regarding clinically relevant outcomes such as prevention of early weaning, increased duration of breastfeeding, and child growth and weight gain. However, in our study, it was possible to observe that, after 6 months, the patient was no longer using food supplements, pacifiers, or fingers; she was exclusively breast-fed. In addition, the patient had satisfactory weight gain for her age, which, in contrast to the aforementioned study, clearly demonstrates that frenotomy contributes to improved breastfeeding.
Conclusions
The diagnosis of ankyloglossia using a specific protocol is crucial, providing a safe indication of early intervention. In this study, the frenotomy improved holding and maintenance of breastfeeding as the only source of food for the patient.
References
1. Knox I. Tongue tie and frenotomy in the breastfeeding newborn. Neo Reviews. 2010;11(9):513-9.
2. Sakalidis VS, Williams TM, Garbin CP, Hepworth AR, Hartmann PE, Paech MJ et al. Ultrasound imaging of infant sucking dynamics during the establishment of lactation. J Hum Lact. 2013;29(2):205-13.
3. McClellan HL, Kent JC, Hepworth AR, Hartmann PE, Geddes DT. Persistent nipple pain in breastfeeding mothers associated with abnormal infant tongue movement. Int J Environ Res Public Health. 2015;12(9):10833-45.
4. Martinelli RLC. Relação entre as características anatômicas do frênulo lingual e as funções de sucção e deglutição em bebês. [Dissertação]. Bauru (SP): Faculdade de Odontologia de Bauru, Universidade de São Paulo; 2013.
5. Martinelli RLC, Marchesan IQ, Lauris JR, Honório HM, Gusmão RJ, Berretin-Felix G. Validity and reliability of screening: "tongue test". Rev. CEFAC. 2016;18(6):1323-31.
6. Brookes A, Bowley DM. Tongue tie: the evidence for frenotomy. Early Hum Dev. 2014;90(11):765-8.
7. Francis DO, Krishnaswami S, McPheeters M. Treatment of ankyloglossia and breastfeeding outcomes: a systematic review. Pediatrics. 2015;135(6):1458-66.
8. Canadian Agency for Drugs and Technologies in Health. Frenectomy for the correction of ankyloglossia: a review of clinical effectiveness and guidelines [online]. Ottawa: CADTH; 2016. Disponível em: http://www.ncbi.nlm.nih.gov/books/NBK373454/
Author notes
Mailing address: Kleber Rosa de Almeida, Rua Luiz Botta, 1209, CEP: 03959000 - São Paulo, São Paulo, Brasil, E-mail: kleberfono12@globo.com
Conflict of interest declaration