Artículos
AComparison of the Effects of Anesthesia with Ketamin-Sevoflurane and Ketamin-Propofol on Cardiorespiratory Variables in Patients Undergoing Diagnostic Cardiac Angiography at Children’s Medical Center in 2014
Una comparación de los efectos de la anestesia con ketamina-sevoflurano y ketamina-propofol en variables cardio-respiratorias en pacientes sometidos a angiografía cardíaca diagnóstica en el Centro médico infantil en 2014
AComparison of the Effects of Anesthesia with Ketamin-Sevoflurane and Ketamin-Propofol on Cardiorespiratory Variables in Patients Undergoing Diagnostic Cardiac Angiography at Children’s Medical Center in 2014
Revista Latinoamericana de Hipertensión, vol. 13, no. 3, pp. 236-241, 2018
Sociedad Latinoamericana de Hipertensión

This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International.
Abstract:
Pediatric patients undergoing cardiac catheterization need general anesthesia with the least alteration in hemodynamic status. The aim of this study was to compare the effects of ketamine-propofol and ketamine-sevoflurane on hemodynamic changes in pediatric patients undergoing cardiac catheterization. In this randomized double-blinded clinical trial, sixty 2-8 year-old patients met the inclusion criteria and were randomly divided into two equal groups (n=30): the KS group (1 mg/kg intravenous ketamine and 2.5 minimum alveolar concentration (MAC) volatile sevoflurane for induction followed by 1.5 MAC sevoflurane which was reduced to 1 MAC after 10 min) and the KP group (0.1 ml/kg of premixed solution of 80 mg/ml ketamine and propofol for induction followed by a maintenance solution of 0.01 mg/kg min). Heart rate (HR), blood pressure, and arterial oxygen saturation were recorded and compared prior to and after the induction of anesthesia, prior to and after catheter insertion, and together with the measurement of systemic and pulmonary atrial blood pressure during angiography. Pain was recorded using Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) immediately after surgery and every 10 min until recovery and discharge. None of the patients had significant changes in blood pressure and heart rate. There was no significant difference in cardiopulmonary assessment using angiography. The mean of CHEOPS in the KS group was significantly lower than that in the KP group 40 and 50 min after surgery. There was no significant difference between the groups in terms of mean CHEOPS trend. Patients in the KS group recovered and were discharged from the recovery room faster than patients in the KP group. Based on our result, the ketamine-sevoflurane combination has no significant advantages over ketamine-propofol combination. However, its shorter recovery time has made it the preferred method of general anesthesia.
Keywords: Angiography, ketamine, pediatric, propofol, sevoflurane, hemodynamics.
Resumen:
Los pacientes pediátricos sometidos a cateterismo cardíaco necesitan anestesia general con la menor alteración en el estado hemodinámico. El objetivo de este estudio fue comparar los efectos de la ketamina-propofol y la ketamina-sevoflurano en los cambios hemodinámicos en pacientes pediátricos sometidos a cateterismo cardíaco. En este ensayo clínico aleatorizado a doble ciego, 60 pacientes de 2 a 8 años cumplieron los criterios de inclusión y se dividieron aleatoriamente en dos grupos iguales (n = 30): el grupo KS (1 mg / kg de ketamina intravenosa y 2,5 concentración alveolar mínima (MAC) sevoflurano volátil para la inducción seguido por 1.5 MAC sevoflurano que se redujo a 1 MAC después de 10 min) y el grupo KP (0.1 ml / kg de solución premezclada de 80 mg / ml de ketamina y propofol para la inducción seguido de una solución de mantenimiento de 0.01 mg / kg min). La frecuencia cardíaca (FC), la presión arterial y la saturación arterial de oxígeno se registraron y compararon antes y después de la inducción de la anestesia, antes y después de la inserción del catéter, y junto con la medición de la presión arterial sistémica y pulmonar durante la angiografía. El dolor se registró usando la escala de dolor del Hospital de Niños de Ontario del Este (CHEOPS) inmediatamente después de la cirugía y cada 10 minutos hasta la recuperación y el alta. Ninguno de los pacientes presentó cambios significativos en la presión arterial y la frecuencia cardíaca. No hubo diferencias significativas en la evaluación cardiopulmonar con angiografía. La media de CHEOPS en el grupo de KS fue significativamente menor que en el grupo de KP 40 y 50 minutos después de la cirugía. No hubo diferencias significativas entre los grupos en cuanto a la tendencia media de CHEOPS. Los pacientes en el grupo KS se recuperaron y fueron dados de alta de la sala de recuperación más rápido que los pacientes en el grupo KP. En base a nuestro resultado, la combinación ketamina-sevoflurano no tiene ventajas significativas sobre la combinación ketamina-propofol. Sin embargo, su menor tiempo de recuperación lo ha convertido en el método preferido de anestesia general.
Palabras clave: angiografía, ketamina, pediatría, propofol, sevoflurano, hemodinámica.
Introduction
eneral anesthesia for pediatric cardiac catheterization is usually necessary to prevent pain, movement, and hemodynamic response to the noxious stimuli used to increase procedure effectiveness1. In addition, there is a growing body of knowledge that precise sedation monitoring is associated with improved safety and post-surgical pain control2.
Diagnostic angiographic catheterization in pediatric patients is provided to assess the physiologic and hemodynamic status of cardiac chambers, systemic and pulmonary blood pressure, vascular resistance, and cardiac contractility1.
In general anesthesia, reduced threshold of apnea and respiratory depression lead to the increase of arterial carbon dioxide tension, pulmonary vascular resistance, and the following pulmonary hypertension1. These alterations on pulmonary/systemic blood flow ratio can affect angiographic findings; therefore, anesthetic medications that cause less hemodynamic alteration are preferable.
Few studies have been conducted on the effect of anesthetic method on hemodynamic variables in the pediatric population. Ketamine is a hypnotic/sedative medication preferred by many in pediatric catheterization suites due to its benefits in airway management with minimal alteration in respiration and preservation of cardiac function. Ketamine can increase the sympathetic effect; however, its effect on pulmonary vascular resistance is not fully understood3.
Propofol is another anesthetic agent in pediatric units with many advantages such as predictable onset of action, short half-life, and rapid recovery time. Propofol has no analgesic effect and is associated with respiratory depression4,5. Ketamine and propofol have opposing effects on blood pressure, heart rate, and systemic vascular resistance. These combinations were used in some studies.
Akin compared the effect of low-dose ketamine and propofol combination and propofol alone on hemodynamic changes in pediatric catheterization. He concluded that the ketamine and propofol combination preserves mean atrial blood pressure better than propofol alone without a significant effect on recovery time.
Sevoflurane is a volatile liquid used as an inhalational anesthetic that has a significantly slower onset of action, lower incidence of apnea, and a shorter time to re-establishment of spontaneous ventilation compared with propofol. Induction complications are uncommon with sevoflurane.
In the study of Potocnik9, the effect of sevoflurane vs. propofol on hemodynamic changes in patients undergoing thoracotomy was compared. He revealed more circulatory stability and a lower dose of ephedrine consumption in the sevoflurane group.
Few studies have compared the effect of propofol, ketamine, and sevoflurane on hemodynamic status in pediatric patients. The aim of the present study was to investigate the effect of ketamine-propofol and ketamine-sevoflurane combination on hemodynamic changes in pediatric patients undergoing cardiac catheterization.
Materials and methods
Following the approval by the Tehran University of Medical Sciences (Tehran, Iran) and the signing of written informed consent forms, patients undergoing diagnostic cardiac angiography (ASA class I-II) in Children’s Medical Center were considered eligible for the study. Patients with underlying pulmonary, hepatic, renal, and metabolic diseases; patients with a history of cardiac or thoracic surgery; and patients who needed more airway support and pulmonary care were all excluded from the study. Sixty 2-8 year-old patients who met the inclusion criteria were enrolled in the study.
Patients were randomly divided into two equal groups (n=30). Premedication was done by oral midazolam (0.5 mg/kg) after electrode placement for electrocardiography (ECG) monitoring, pulse oximetry, and non-invasive blood pressure monitoring.
In the KS group, induction of anesthesia was performed using 1 mg/kg of intravenous ketamine and 2.5 minimum alveolar concentration (MAC) of volatile sevoflurane. All patients received 100% oxygen via mask oxygenation using the Bain Circuit system. After 3 min, Laryngeal Mask Airway (LMA) was inserted and fixed in patients with desirable spontaneous breathing. Anesthesia was maintained using 1.5 MAC sevoflurane and 21% oxygen. Sevoflurane was reduced to 1 MAC after 10 min (after insertion of angiographic catheter). In patients who needed a second attempt of catheter insertion or change in position, 0.5 mg/kg of intravenous ketamine was administered.
In the KP group, a mixture of 20 ml propofol 1% (200 mg) + 4 ml ketamine (200 mg) and D5%W (1 ml) was prepared. This solution includes 8 mg/ml ketamine and 8 mg/ml propofol. In this group, 0.1 ml/kg of the prepared KP solution (0.8 mg/kg of each anesthetic) was administered for induction, and 0.01 ml/kg/min (80 µg/kg/min of both ketamine and propofol) was administered for maintenance of anesthesia. Airway support in this group was similar to the KS group and LMA was inserted in the same manner. After insertion of the angiographic catheter (10 min after the induction), the dose of KP solution was reduced to 60 µg/kg/min and 10 min later, it was reduced to 40 µg/kg/min. In patients who needed a second attempt of catheter insertion or change in position, 0.4 mg/kg of both ketamine and propofol bolus dose were injected intravenously.
Demographic data such as age, gender, and weight of all participants were recorded. Heart rate (HR), blood pressure, and peripheral oxygen saturation (SPO2) were recorded and compared prior to and after induction of anesthesia, prior to and after catheter insertion, and together with the measurement of systemic and pulmonary atrial blood pressure during angiography. PaO2 and PaCO2 in arterial blood gas sample were measured during catheterization. Aortic, left and right ventricular pressure, pulmonary artery systolic and diastolic blood pressure, the incidence and severity of nausea and vomiting (0: without nausea, 1: with nausea, 2: with nausea and vomiting), pain and agitation (0: without pain or agitation, 1: with pain or agitation), and recovery time (time needed to achieve an Aldrete Score of 9 out of 10) were recorded and compared between the groups.
Pain in participants was recorded as a qualitative nominal variable (0: without pain, 1: with pain) and quantitative variables using Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS)10 and Pediatric Anesthesia Emergence Delirium (PAED) Scale11 immediately after surgery and every 10 min after surgery, until recovery and discharge.
In this clinical trial, the anesthesiologist who was responsible for administration of medications and recording of the data and the person who was responsible for data analysis were blinded.
All statistical analyses were performed using SPSS 12 software package and statistical significance was determined as P≤0.05.
This randomized controlled trial (RCT) was registered in the Iranian Registry of Clinical Trials (IRCT2015013012642N12).
Results
There were no significant difference between the two groups in terms of age (4.20 ± 2.28 and 4.20 ±2.28 years in KS and KP groups, respectively), gender (16/14 and 15/15 in the KS and KP groups, respectively) and weight (14.83 ± 6.26 and 17.83 ± 8.26 in the KS and KP groups, respectively). Baseline heart rate, diastolic blood pressure (DBP), PaO2, PaCO2, and SPO2 in both groups were similar (Table 1).
| Table 1: cardiovascular variables in both groups in five evaluations. | ||||
| Variables | Time of evaluation | KS group (n=30) | KP group (n=30) | P value |
| Heart rate (beat /minute) | Prior to induction | 116.5 (16.81) | 110.3 (13.92) | 0.108 |
| After induction | 116.53 (18.62) | 109.33 (15.22) | 0.107 | |
| Prior to catheterization | 116.77 (18.89) | 111.00 (17.06) | 0.224 | |
| After catheterization | 115.63 (18.42) | 107.60 (16.22) | 0.078 | |
| Along with angiography | 116.77 (16.24) | 111.80 (15.36) | 0.229 | |
| Systolic blood pressure (mmHg) | Prior to induction | 92.13 (10.28) | 97.73 (9.48) | 0.032* |
| After induction | 90.06 (12.20) | 94.63 (11.07) | 0.134 | |
| Prior to catheterization | 91.27 (10.95) | 96.21 (9.37) | 0.068 | |
| After catheterization | 88.40 (11.80) | 94.14 (9.24) | 0.043* | |
| Along with angiography | 90.30 (10.01) | 96.53 (8.41) | 0.011* | |
| Diastolic blood pressure (mmHg) | Prior to induction | 60.77 (9.13) | 59.96 (9.00) | 0.734 |
| After induction | 58.50 (8.92) | 58.23 (10.08) | 0.914 | |
| Prior to catheterization | 59.27 (8.85) | 58.89 (9.10) | 0.875 | |
| After catheterization | 57.00 (9.38) | 57.10 (9.05) | 0.966 | |
| Along with angiography | 57.40 (9.33) | 59.00 (8.50) | 0.490 | |
| peripheral oxygen saturation (SpO2) | Prior to induction | 92.80 (6.39) | 92.67 (5.47) | 0.931 |
| After induction | 93.60 (6.05) | 93.53 (6.26) | 0.967 | |
| Prior to catheterization | 93.77 (5.21) | 92.48 (7.29) | 0.438 | |
| After catheterization | 93.33 (6.36) | 93.70 (5.13) | 0.807 | |
| Along with angiography | 94.07 (5.08) | 94.43 (4.67) | 0.772 | |
There was no recorded case of more than 5% change in these parameters in either group.
All variables across the KS and KP groups were assessed based on underlying cyanotic or non-cyanotic diseases. The heart rate and systolic blood pressure of the non-cyanotic group were insignificantly lower in the KP group (p=0.06 and 0.055, respectively).
None of the patients had significant changes in systolic and diastolic blood pressure and heart rate (changes of over 20% with respect to baseline evaluation).
There was no significant difference in cardiopulmonary evaluation using angiography and arterial blood gas (ABG) variables except for bicarbonate concentration, which was significantly lower in the KS group. Pulmonary systolic blood pressure in cyanotic patients of the KS group was significantly lower than that in the KP group (14.28±2.36 vs. 35.85±25.73, respectively, p=0.047). PaO2 in non-cyanotic patients of the KS group (129.1±83.45 vs. 88.1±21.02, respectively, p=0.045) and cyanotic patients of the KP group (67.7±13.66 vs. 54.11±5.30, respectively, p=0.013) was significantly higher than the other group. Table 2 summarizes the comparison of the two groups.
| Table 2: cardiopulmonary pressure during angiography in both groups | |||
| Variables | The KS group | The KP group | P value |
| Aortic blood pressure (mmHg) | 90.67 (11.07) | 94.97 (10.16) | 0.123 |
| Left ventricular pressure (mmHg) | 94.00 (16.29) | 100.41 (13.51) | 0.111 |
| Right ventricular pressure (mmHg) | 46.00 (27.12) | 49.85 (35.76) | 0.647 |
| Pulmonary systolic blood pressure (mmHg) | 27.04 (15.11) | 33.32 (19.32) | 0.191 |
| Pulmonary diastolic blood pressure (mmHg) | 13.11 (6.88) | 16.64 (9.32) | 0.125 |
| PO2 (mmHg) | 105.83 (77.33) | 81.30 (21.05) | 0.099 |
| PCO2 (mmHg) | 43.47 (6.47) | 41.67 (3.99) | 0.200 |
| HCO3 | 20.27 (2.26) | 21.43 (2.04) | 0.044* |
Nausea and vomiting was reported in one patient in the KS group. Pain was reported in 3 and 2 patients and agitation was reported in 3 and 1 patients of the KS group and KP, respectively, which was not different between the groups (p>0.05).
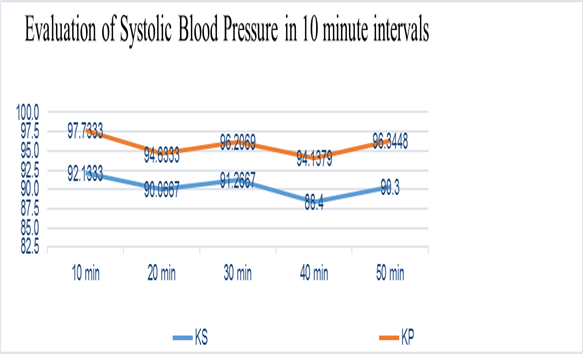
Figure 1:
The mean of systemic systolic blood pressure in 10 minute intervals. KS: ketamine-sevoflurane; KP: ketamine-propofol
CHEOPS in groups KS and KP is as shown in Figure 2. The mean of CHEOPS in the KS group was significantly lower than that in the KP group in 40 and 50 min after surgery. There was no significant difference between groups in mean of CHEOPS trend in six evaluations (p= 0.6).
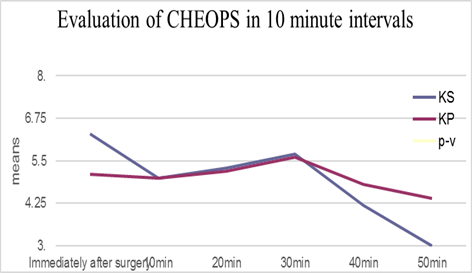
Figure 2
The mean of CHEOPS in both groups in 10 minute intervals. KS: ketamine-sevoflurane; KP: ketamine-propofol; CHEOPS: Children’s Hospital of Eastern Ontario Pain Scale
The mean of CHEOPS in non-cyanotic patients of the KS group was significantly lower than that in the KP group (4.75±2.21 vs. 7.33±2.43, respectively, p=0.001). This difference in cyanotic patients was not significant.
PAED in groups KS and KP is shown in Figure 3. It was significantly lower in the KS group 10 minutes after surgery. Both groups had similar PAED trends. The mean of PAED in non-cyanotic patients of the KS group was significantly lower than in the KP group (4.92±2.09 vs. 6.31±2.23, respectively; p=0.04). This difference in cyanotic patients was not significant.
Patients in the KS group recovered and were discharged from the recovery room faster than patients in the KP group (12 vs. 3; p=0.007), 30 (18 vs. 10; p=0.03), 40 (24 vs. 16; p=0.02) and 50 (29 vs. 18; p=0.005) minutes after surgery. Recovery time in non-cyanotic patients of the KS group was significantly faster than in the KP group (28.33 vs. 51.75; p=0.000).
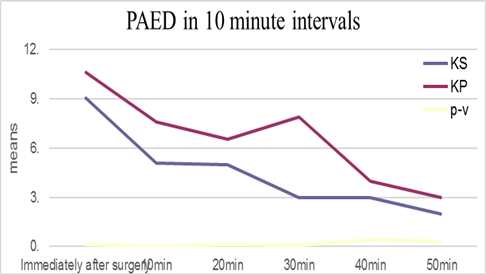
Figure 3
The mean of PAED in both groups in 10 minute intervals. KS: ketamine-sevoflurane; KP: ketamine-propofol; PAED: Pediatric Anesthesia Emergence Delirium Scale
Discussion
This study compared the effects of the two different anesthesia methods of ketamine-propofol and ketamine-sevoflurane on the hemodynamic stability of pediatric patients undergoing cardiac catheterization. There are many different anesthetic methods for cardiac catheterization in children. Ketamine is an injectable anesthetic medication that has adequate analgesic and sedative effect and no significant alteration of airway reflexes and respiratory drive; however, it has a prolonged recovery period12. Propofol, a short-acting anesthetic medication with insufficient analgesic effect, is another drug commonly used in pediatric cardiac procedures. The mixture of ketamine-propofol was reported as a safe and practical alternative for general anesthesia in pediatric cardiac catheterization7.
Sevoflurane, a volatile liquid anesthetic with slower onset of action, lower incidence of apnea, and a shorter time to re-establishment of spontaneous ventilation compared to propofol, is another anesthetic option with uncommon induction complications.
The results of the present study showed lower systolic blood pressure, CHEOPS and PAED in the KS group when compared with the KP group. Recovery time in the KS group was significantly shorter than in the KP group. The score of pain, agitation, nausea and vomiting was not different between the two groups. There was no significant difference in left and right ventricular, aortic and pulmonary blood pressure between the two groups.
Potocnik et al.9 compared the effects of sevoflurane vs. propofol on hemodynamic changes in patients undergoing thoracotomy in their study. The results of their study showed a greater circulatory stability and a lower dose of ephedrine consumption in the sevoflurane group. Our findings showed a lower systolic blood pressure in the KS group compared to the KP group.
In their study, Kanaya et al.13 showed the different effects of propofol and sevoflurane on heart rate. They concluded that induction with propofol can decrease blood pressure and heart rate depending on the different depths of hypnosis. Sevoflurane, however, was found to have little or no effect on hemodynamics. The depth of hypnosis was not evaluated in that study. Contrary to the study of Kanaya et al., the present study found no significant difference in heart rate between the groups. There are evidences of negative inotropic and chronotropic effects of propofol; however, the present study found no significant change in heart rate in either group. There was no significant difference in the left and right ventricular, aortic, and pulmonary blood pressure between the groups.
In their study, Bharti et al.15 compared the hemodynamic effects of sevoflurane- and propofol-based anesthesia and showed the advantages of sevoflurane over propofol in cardiovascular stability and recovery time. In our study, patients in the KS group recovered and were discharged from the recovery room faster than the patients in the KP group. However, the results of the study conducted by Glaisyer and Sury16 showed that recovery time in the propofol-remifentanil group was 19 minutes shorter, and the patients in this group were discharge-ready 19 minutes earlier, than the propofol-sevoflurane and nitrous oxide group16.
Based on the results of the present study, PaO2, PaCO2 and SpO2 were similar in both groups with no significant changes (more than 5% from the baseline evaluation) in any of the patients. Simsek et al.12 designed a study to compare four different anesthetic methods used in pediatric cardiac catheterization: propofol-ketamine, propofol-dexmedetomidine, dexmedetomidine-ketamine, and midazolam-ketamine. They recorded hemodynamic variables every 5 min for half an hour. The significant reduction of SpO2 was recorded 16 times (11.4%) in ketamine-propofol groups, which was significantly higher than the other groups12.
The respiratory rate data in this study was missing, so no conclusion could be made regarding anesthesia-induced changes in respiratory rate, which is the limitation of the present study. Recovery and discharge time were not directly recorded; however, the number of patients in the recovery room was recorded every 10 min after surgery.
There was no significant difference in CHEOPS and PAED between the KS and KP groups. The score of pain, agitation, nausea and vomiting was also not different between the two groups.
Conclusion: Anesthesia in pediatrics is of paramount importance due to the unique physiology and anatomy of the population. Administration of the best anesthetic method with the fewest side effects and shorter recovery time is preferable. Based on our result, the ketamine-sevoflurane combination has no significant advantage over the ketamine-propofol combination; however, because of its shorter recovery time and lower CHEOPS and PAED, it can be the preferred anesthetic method in pediatric patients undergoing cardiac catheterization.
References
1. Bernard PA, Ballard H, Schneider D (2011). Current approaches to pediatric heart catheterizations. Pediatric Reports. 3, e23.
2. Cravero JP, Blike GT (2004). Review of pediatric sedation. Anesth Analg. 99, 1355-64.
3. Berman W, Fripp R, Rubler M, Alderete L (1990). Hemodynamic effects of ketamine in children undergoing cardiac catheterization. Pediatr Cardiol , 11(2), 72-76.
4. Hertzog JH1, Campbell JK, Dalton HJ, Hauser GJ (1999). Propofol anesthesia for invasive procedures in ambulatory and hospitalized children: experience in the pediatric intensive care unit. Pediatrics. 103, E30.
5. Oklü E, Bulutcu FS, Yalçin Y, Ozbek U, Cakali E, Bayindir O (2003) . Which anesthetic agent alters the hemodynamic status during pediatric catheterization? Comparison of propofol versus ketamine. J Cardiothorac Vasc Anesth. 17(6), 686-90.
6. Gayatri P, Suneel PR, Sinha PK (2007). Evaluation of Propofol-Ketamine anesthesia for children undergoing cardiac catheterization procedures. J Interv Cardiol. 20, 158- 63.
7. Kogan A, Efrat R, Katz J, Vidne BA (2003). Propofol-ketamine mixture for anesthesia in pediatric patients undergoing cardiac catheterization. J Cardiothorac Vasc Anesth. 17(6), 691-3.
8. Akin A, Esmaoglu A, Guler G, Demircioglu R, Narin N, Boyaci A (2005). Propofol and propofol-ketamine in pediatric patients undergoing cardiac catheterization. Pediatr Cardiol. 26(5), 553-7.
9. Potocnic I, Jankovic VN, Stupnil T and Kremzar B (2011). Haemodynamic changes after induction of anesthesia with sevoflurane vs. propofol. SIGNAL VITAE. 6(2), 52-57.
10. Cohen LL, Lemanek K, Blount RL, Dahlquist LM, Lim CS, Palermo TM (2008). Evidence-based Assessment of Pediatric Pain. J Pediatr Psychol. 33(9), 939-955.
11. Sikich N and Lerman J (2004). Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology. 100 (5), 1138-45.
12. Simsek M, Bulut MO, Ozel D, Yucel IK, Aykac Z (2016). Comparison of sedation method in pediatrics cardiac catheterization. Eur Rev Med Pharmacol Sci. 20(8), 1490-4.
13. Kanaya N, Hirata N, Kurosawa S, Nakayama M and Namiki A (2003). Differential effect of propofol and sevoflurane on heart rate variability. Anesthesiology. 98, 34-40.
14. Dewhirst E, Lancaster C, Tobias JD (2013). Hemodynamic changes following the administration of propofol to facilitate endotracheal intubation during sevoflurane anesthesia. Int J Clin Exp Med. 6(1), 26-29.
15. Neerja Bharti, Promila Chari, and Parag Kumar (2012). Effect of sevoflurane versus propofol-based anesthesia on the hemodynamic response and recovery characteristics in patients undergoing microlaryngeal surgery. Saudi J Anaesth. 6(4), 380–384.
16. Glaisyer HR, Sury MR (2005). Recovery after anesthesia for short pediatric oncology procedures: propofol and remifentanil compared with propofol, nitrous oxide, and sevoflurane.Anesth Analg. 100(4), 959-63.
Author notes
bnooralishahi@gmail.com