Artículos

This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International.
Abstract: The purpose of current study was to compare different cognitive abilities, depression and anxiety of type II diabetic patients with healthy individuals in Isfahan province in 2015. The research method used for this research is a scientific-comparative method. Independent variable is defined in the healthy and type II diabetic patient groups and the dependent variables are defined by the participants’ scores in cognitive ability test and the scale of anxiety and depression. The statistical population consisted of two groups (type II diabetic group: included type II diabetic patients who were diagnosed with type II diabetes by their specialist physicians and the diagnosis metabolism for type II diabetes, and the healthy group: including companions of patients). The sample size for type II diabetes group consisted of 40 individuals and for the healthy group was consisted also of 40 individuals. Sampling had been done using random sampling method. The data were collected using cognitive abilities questionnaire and Hospital anxiety and depression scale (HADS). Data were analyzed using SPSS-20 software in two descriptive and inferential sections. The results indicated that in type II diabetic patients, there is a significant and direct relationship between sustained attentions with job status; there is a significant and reverse relationship between cognitive flexibility with marital status, and a significant and direct relationship between cognitive flexibility with educational status. The relationship between the mean scores of overall cognitive abilities and the mean of total mood changes in type II diabetic patients is confirmed. The mean scores of cognitive abilities in all subscales and the overall test in healthy subjects are higher than those with type II diabetes. The mean of mood changes in all subscales and the overall test in healthy subjects are lower and less than those with type II diabetes.
Keywords: Cognitive Abilities, Depression and Anxiety, Diabetes and Diabetic Patients.
Resumen: El objetivo del presente estudio fue comparar diferentes habilidades cognitivas, depresión y ansiedad de pacientes diabéticos tipo II con individuos sanos en la provincia de Isfahan en 2015. El método de investigación utilizado para esta investigación es un método científico-comparativo. La variable independiente se define en los grupos de pacientes diabéticos sanos y de tipo II y las variables dependientes se definen mediante las puntuaciones de los participantes en la prueba de capacidad cognitiva y la escala de ansiedad y depresión. La población estadística consistió en dos grupos (grupo diabético tipo II: pacientes diabéticos tipo II incluidos que fueron diagnosticados con diabetes tipo II por sus médicos especialistas y el diagnóstico de metabolismo para la diabetes tipo II, y el grupo saludable: incluidos los compañeros de los pacientes). El tamaño de muestra para el grupo de diabetes tipo II consistió en 40 individuos y para el grupo sano también consistió en 40 individuos. El muestreo se realizó con un método de muestreo aleatorio. Los datos fueron recolectados mediante el cuestionario de habilidades cognitivas y la escala de ansiedad y depresión del Hospital (HADS). Los datos se analizaron usando el software SPSS-20 en dos secciones descriptivas e inferenciales. Los resultados indicaron que en pacientes diabéticos tipo II, existe una relación significativa y directa entre las atenciones sostenidas con el estado laboral; hay una relación significativa e inversa entre la flexibilidad cognitiva con el estado civil y una relación significativa y directa entre la flexibilidad cognitiva y el estado educativo. Se confirma la relación entre las puntuaciones medias de las capacidades cognitivas generales y la media de los cambios de humor total en pacientes diabéticos tipo II. Los puntajes promedio de las habilidades cognitivas en todas las subescalas y la prueba general en sujetos sanos son más altos que aquellos con diabetes tipo II. La media de los cambios de humor en todas las subescalas y la prueba global en sujetos sanos son menores y menores que en aquellos con diabetes tipo II.
Palabras clave: Habilidades cognitivas, depresión y ansiedad, diabetes y pacientes diabéticos.
Introduction
Diabetes is a chronic and dangerous metabolic disorder that is divided into two types of I and II. Type I diabetes is insulin dependent, and Type II diabetes is non-insulin dependent diabetes (Aghamolayi et al., 2006). In other words, the diabetic patient either does not produce insulin or does not respond to insulin. Hence, glucose intolerance or increased blood glucose is the most common symptom of the disease, and the symptoms of this disease include short-term complications and long-term increased of blood glucose levels (Beghiani-Moghdam et al., 2006).
So that, diabetes is the fifth cause of death in the world and about 150 million people are affected worldwide (Schwendi et al., 2010). Moreover, diabetes also has serious and dangerous side effects that can reduce the health and life expectancy of patients. These complications include kidney failure, cardiovascular complications, blindness, bed sores and legs lesions (Vares et al., 2010).
In addition, diabetes has high health costs, which directly account for 1.5 to 2.5 percent of the total health budget and indirectly includes several times this amount. One of the important therapeutic goals of diabetic patients is to increase their quality of life, which today self-care program plays a major role in this matter. Depression is common in chronic diseases, and it is 3 times more common in diabetes comparing to other chronic diseases. The prevalence of depression in these patients is estimated to be 61.3%, and in Iran, this number is reported in type II diabetes up to 48.1%. Depression in addition to psychological and social complications associated with these patients, is a risk factor for disrupting self-care behaviors (Vares et al., 2010).
Depression is the most commonly diagnosed psychiatric disorder that has recently grown and is referred to as psychological common cold. Almost all humans in their lives experience at least mild depression or in the face of suffering and loss show some of the symptoms of depression. Feelings (meaningfulness, impatience, sadness, frustration, coldness and unpleasantness) are the most common experiences of depression. Over the past thirty years, significant advances have been made in recognizing this disease, and today, most people with this disease can be helped (Miligman and Rosenhan, 2004).
Depression is a common disorder, with a lifelong prevalence of about 15%, and in women, it may be as high as 25%. The prevalence of major depressive disorder is high in patients referred to general practitioners or hospital wards, so that it has been reported to be 10 to 15 percent (Saduk and Saduk, 2008).
Evidence suggests that depression increases the burden of diabetes and creates problems for glycemic control due to impairment in self-care behaviors. The risk factors for depression in diabetes are sex, body mass index, age of the patient, major stressful life events, status (unfavorable socioeconomic status and lack of social support) (Bay et al., 2008).
The prevalence of depression in our diabetic patients has been reported to be 41.9%, of which 24.7% have major depressive disorder, 9.3% have Dysthymia and 8% have two disorders. The prevalence of major depression was between the ages of 31-59 and dysthymia was above 60 years. Studies also show that depression was more common in sick women, in patients with uncontrolled blood glucose and in patients with systemic diabetes complications (Larijani et al., 2003).
The prevalence of diabetes, especially type II (middle-age onset of diabetes) is rising in the world and includes 90-95% of diabetic patients worldwide (Aghayi-Molayi et al., 2004). Therefore, the overlap effect of diabetes and depression on cognitive problems of these patients is indisputable and it is necessary to examine how it affects the life of diabetic patients. The current research attempts to evaluate the memory, attention, general intelligence, visual perception, spatial functions of the cognitive subsystems in these patients. Considering the importance of the research, different cognitive abilities, depression and anxiety among type II diabetic patients had been compared with healthy individuals in Isfahan province in 2015.
Materials and methods
The research method of the current study is scientific-comparative. Independent variable in healthy and patient group is defined as type II diabetes and the dependent variables are defined by the scores of the subjects in cognitive ability test and the hospital anxiety and depression scale. Coefficient of correlation of demographic variables was investigated and controlled with research variables. The statistical population included two groups:
Type II diabetes: Type II diabetic patients who have been diagnosed by their own specialist physician and the Metabolic Diagnosis test were included as patients group.
Healthy group: Includes patients’ companions. The sample size of type II diabetic group was 40 and the sample size for healthy group was also 40. Sampling had been done using random sampling method. The data were collected through cognitive abilities questionnaire and hospital anxiety and depression scale (HADS). In the current study independent variables are: being a member of healthy or patient groups and type II diabetes; dependent variables include the scores of subjects in the cognitive abilities and hospital tests.
In the stage of research implementation, after providing a preliminary description of the measurement tools and the purpose of the test, it was explained for participants how to respond to the tests in detail. In the case of ethical considerations, after obtaining consent from participants and providing the necessary information, they were assured that obtained information would be used only in this research and it would be protected from any misuse. The questionnaires contained questions that were able to measure variables of the research. The Response Scale is a 5-point Likert scale. The data were analyzed using SPSS-20 software in two descriptive and inferential sections.
Research Methods:
From September 24, 2015 the sample was selected randomly from type II diabetic patients. After obtaining consent from patient and their companions to participate in the research, descriptions had been provided and the tests had been implemented which took about 30 minutes for preparation; the healthy group consisted of the companions of these patients, and the procedure for type II diabetic group that was mentioned before was also implemented for the healthy group.
Results:
The report of the results of descriptive statistics in the research
Results of descriptive statistics of demographic characteristics in research
In the following section, the frequency, frequency percentage and frequency of aggregation of demographic characteristics in healthy and type II diabetic groups are discussed. Demographic characteristics include age, gender, educational status, occupational status and marital status. For this purpose, frequency, frequency percentage and frequency of aggregation of the study groups were initially reported for two groups of healthy and type II diabetic patients. Further, other characteristics of these two groups were investigated.
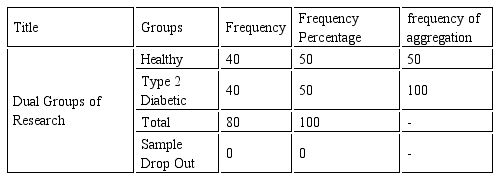
As shown in [Table 1], the total number of sample was 80, of which 40 were in the healthy group and 40 were in the type 2 diabetic group. The rate of drop out in the research was zero and all participants completed the questionnaire and cooperate at the end of the research.
Descriptive statistics of research sample groups based on dual groups
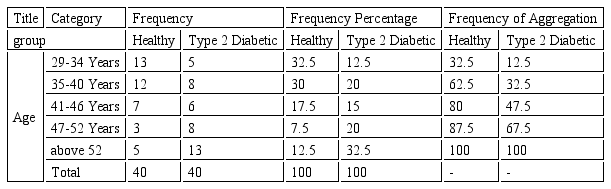
As shown in [Table 2], the highest frequency was seen in the age group of 29 to 34 years in the healthy group; and the highest frequency was also seen in the age group above 52 years in type II diabetic patients. The lowest frequency was reported in the age group of 47 to 52 years in the healthy group and in 29 to 34 years for the patient group.
Descriptive statistics of five age groups divided into two groups of healthy and patients
As shown in [Table 3], female gender in type II diabetic group with 29 individuals and in the healthy group with 34 individuals have the highest frequency and frequency percentage.
The descriptive statistics of gender groups in both healthy and patient groups

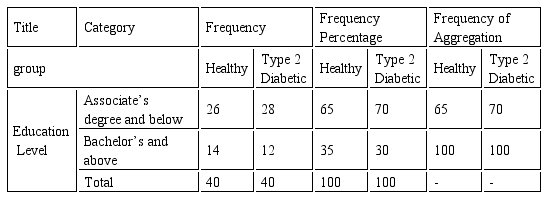
As shown in [Table 4], in educational groups, the lowest frequency is in bachelor's degree and higher group which only were 14 which are 35%; and 12 individuals in the diabetic patients which is 30%. The highest frequency in this area is seen in Associate’s degree and below group which includes 26 individuals in healthy group (equivalent to 65%) and 28 individuals in type II diabetic (equivalent to 70%).
Descriptive statistics of educational status in two healthy and patient groups
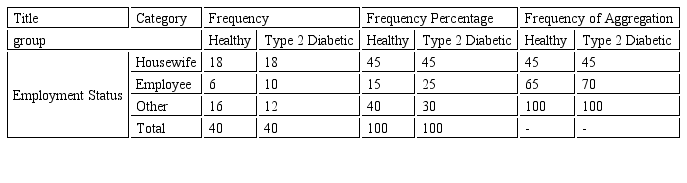
According to [Table 5], the highest prevalence of employment status is seen in the housewife group; its frequency is 18 in the healthy group and 18 in type 2 diabetic group. The lowest frequency is observed in the employee group, with only 6 members in the healthy group which is 15% of the healthy group and 10 individuals in type 2 diabetic patients which is 25%.
Descriptive statistics of employment status in two healthy and patient groups
According to [Table 6], 75% of the healthy group, that is 30 individuals and 85% of the type II diabetic patient which is 34 individuals were married.
Descriptive statistics of marital status in two healthy and patient groups

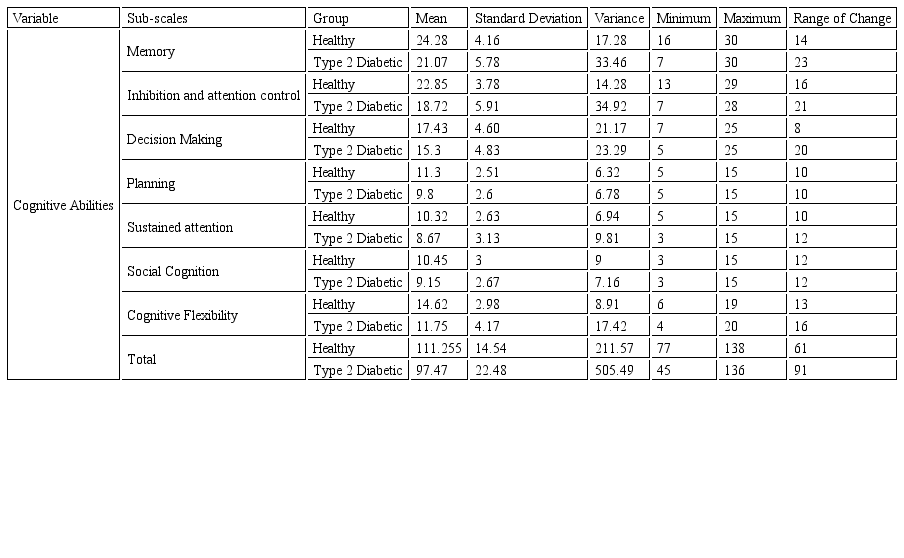
Reports of the results of descriptive statistics of the research variables In the following section, the mean, standard deviation, variance, minimum, maximum and range of research variables including cognitive abilities and mood changes are examined by healthy and type II diabetic groups Table 7.
In [Figure 1], the mean scores of cognitive abilities test and its subscales are categorized into healthy and patient groups.
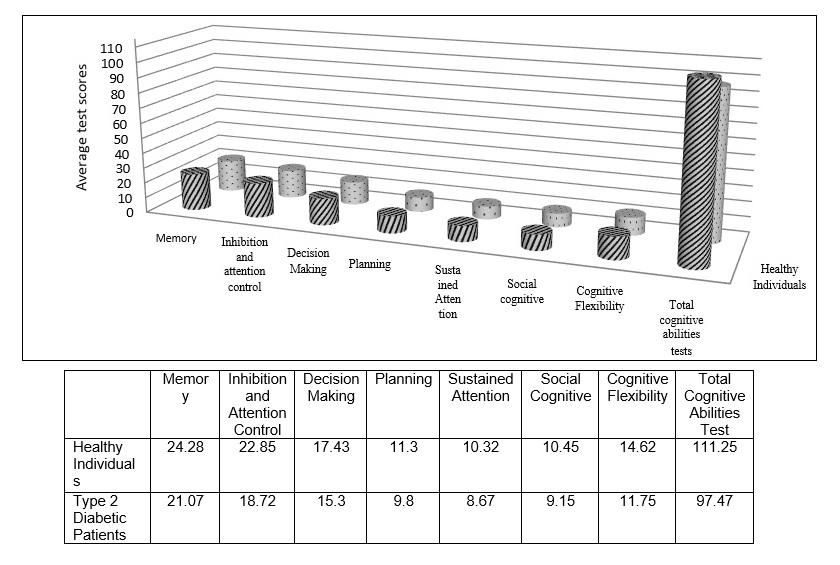
Figure 1
Descriptive statistics of cognitive abilities variables and its subscales
[Figure 2] shows the mean scores of cognitive ability test and its subscales divided into two groups of healthy and patient.
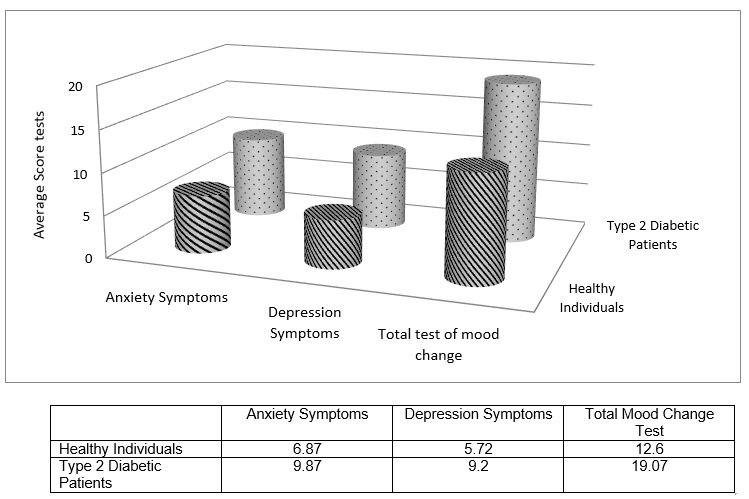
Figure 2
shows the mean scores of cognitive ability test and its subscales divided into two groups of healthy and patient
In the following, t-test results are used to test the hypotheses.
First hypothesis: There is a relationship between the demographic characteristics and cognitive problems in type II diabetic patients Table 8.
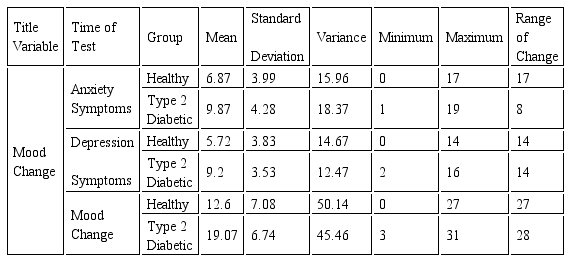
The descriptive statistics of mood changes in two healthy groups and type II diabetic patients
Based on the results reported in [Table 9], the first hypothesis is confirmed only in three relationships. According to the results, only the relationship between sustained attention with employment status (equal to 0.33), cognitive flexibility with marital status (equal to 0.38), and cognitive flexibility with educational status (equal to 0.33) are significant; the relationship between cognitive flexibility with marital status has been reported reversed and the other two relationships are direct. In other subscales of demographic characteristics, no significant relationships have been observed; the relationship between demographic characteristics and overall cognitive abilities are also not significant.
The Matrix of Correlation Coefficients of Cognitive Ability Variables in Patients and Type II Diabetes Groups
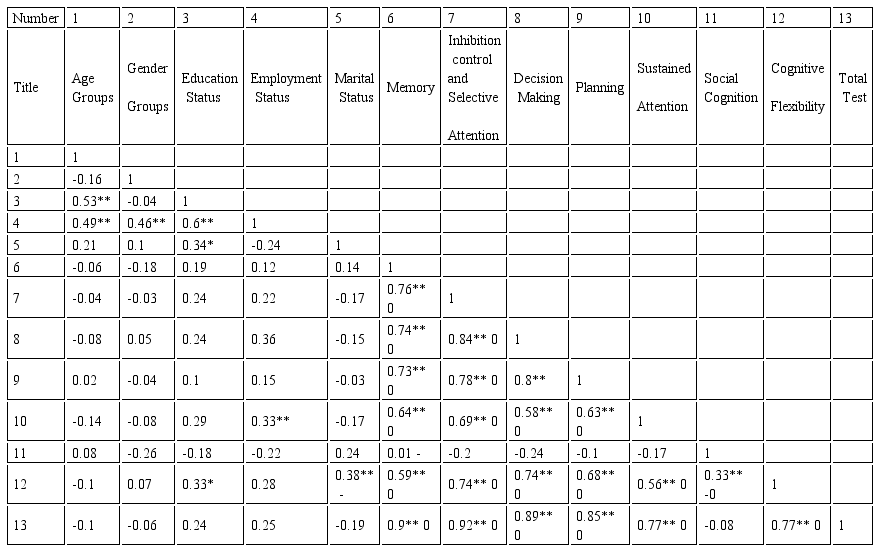
* <0.05** P<0.01
Second hypothesis: There is a relationship between demographic characteristics and mood changes in type II diabetic patients.
According to [Table 10], the second hypothesis of the research is rejected (P> 0.05), and none of the relationships between mood changes with demographic characteristics, either in the sub-scales or in the overall score is significant.
Matrix of Correlation Coefficients of mood changes in type II diabetic patient group
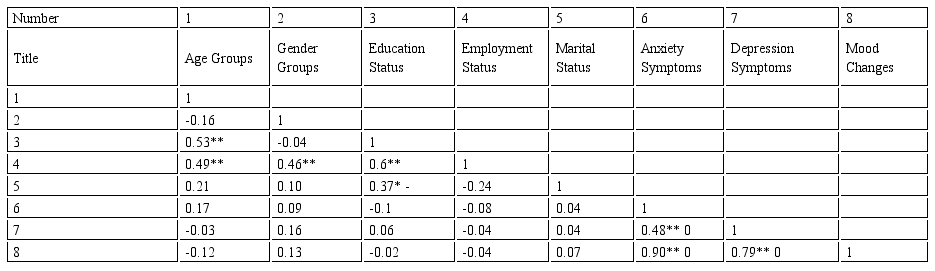
* <0.05** P<0.001
Third hypothesis of research: There is a relationship between cognitive abilities and mood changes in type II diabetic patients.
To test this hypothesis, correlation coefficient test has been used and the correlation coefficient matrix is reported in [Table 11].
According to [Table 11], the third hypothesis of the research regarding the relationship between cognitive abilities and mood changes in some relationships is significant and only in the context of all subscales of mood changes and total mood change, the relationships with social cognition, anxiety symptoms with decision making, planning, social cognition, and cognitive flexibility have been rejected. The relation between the mean scores for overall cognitive abilities and the average scores for total mood changes is confirmed (equal to -0.55); this relationship is considered to be inversely significant. Based on the findings, the relationship between anxiety symptoms and all subscales of cognitive abilities was significant except for social cognition (P> 0.05). The relationship between anxiety symptoms and the total test scores of cognitive abilities was significant (-0.56 at the level below 0.01). The relationship between depression symptoms and the total test scores of cognitive abilities is significant and is reported to be -0.36.
The overall score of mood change tests was not significant only with social cognition (P> 0.05); in other cases, this relationship was significant (P> 0.01). The correlation coefficient reported in this variable with planning had the smallest significant correlation coefficient which was 0.33 at the level below 0.05 that indicates the inverse relationship between the two variables.
Matrix of variables correlation coefficients of cognitive abilities and mood changes in the type II diabetic patient group
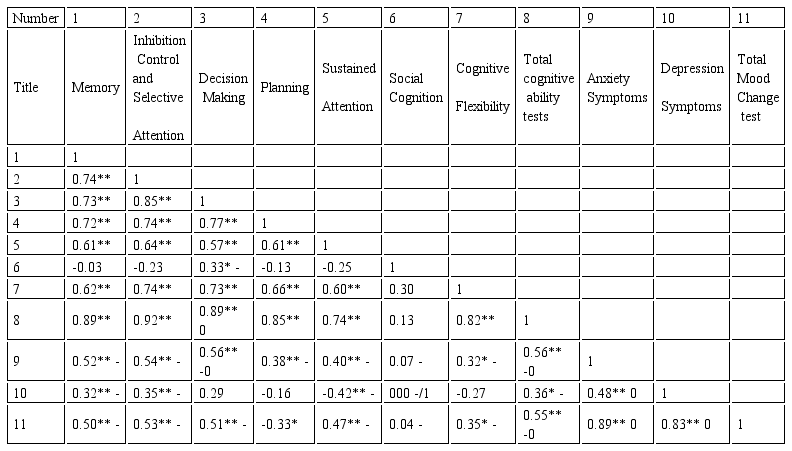
* P<0.05** P<0.01
Fourth hypothesis: There is a difference between the mean scores of cognitive abilities in type II diabetic patients and healthy subjects.
To test this hypothesis, t test of two independent groups has been used and the results are reported in [Table 12].
Based on the results of [Table 12], there is a difference between the mean scores of all subscales of cognitive abilities and overall cognitive ability in type II diabetic patients and healthy subjects (P˂0.05). According to this finding, the fourth hypothesis is confirmed. Accordingly, these abilities differ in healthy subjects and type II diabetic patients. In order to determine that in which group these abilities are higher, refer to descriptive statistics [tables 4-7] which are categorized by healthy and patient groups. Based on these tables, the mean scores of cognitive abilities in all subscales and the overall test in healthy subjects are higher and more than those in type II diabetic group. Accordingly, people with type II diabetes have a lower memory, inhibition control and selective attention, decision making, planning, sustained attention, social cognition, cognitive flexibility, and overall cognitive in comparison to healthy individuals.
Fifth hypothesis: There is a difference between the mean scores of mood changes in type II diabetic patients and healthy subjects.
To test this hypothesis, t test of two independent groups has been used and its results are reported in [Table 13]. To test this test, we must examine the homogeneity assumption of Lewin variance and then the results are reported accordingly, which is shown in the [table 12].
T-test of two independent groups in order to examine the differences between healthy groups and diabetic patients in cognitive abilities and its subscales
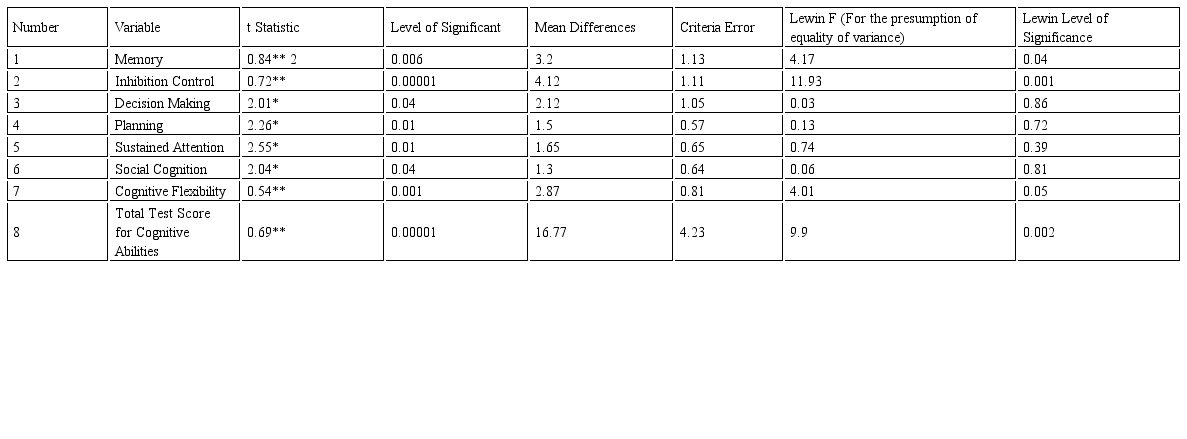
* P<0.05** P<0.01
Based on the results of [Table 13], there is a difference between the mean scores of all subscales of mood changes and overall mood changes in type II diabetic patients and healthy subjects (P < 0.01). According to this finding, the fifth hypothesis is confirmed; accordingly, these changes are different in healthy subjects and type II diabetic patients. In order to examine how these changes are in each group, refer to mean differences in the descriptive statistics [tables 4-7] which are categorized by healthy and patients groups. Based on the [table 8, 9], the mean of mood changes in all subscales and the overall test in healthy people is lower and less than those with type II diabetes. Accordingly, type 2 diabetic patients experience more symptoms of anxiety, depression and mood changes than healthy people.
Table for t-test of two independent groups in order to assess the differences between healthy groups and diabetic patients for mood changes and their subsamples
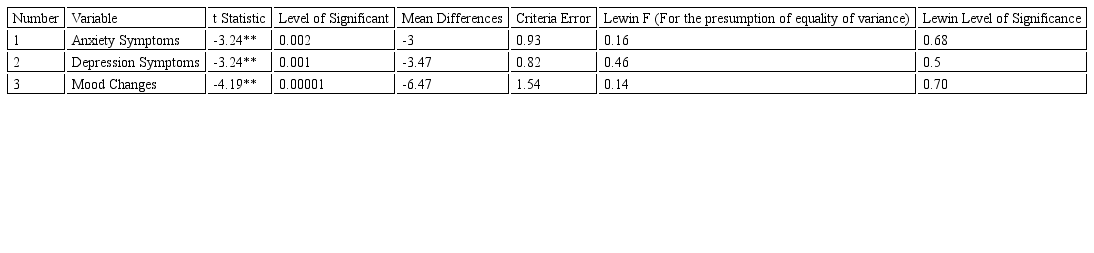
* P<0.05** P<0.001
Discussion
The purpose of this study was to compare the different cognitive abilities, depression and anxiety among type II diabetic patients and healthy individuals in Isfahan province in 2015. The results of the research were consistent with some of the research records that we will examine:
Based on the results of the first hypothesis, this hypothesis is confirmed only in three relationships. Based on the findings, the relationship between sustained attentions with employment status, cognitive flexibility with marital status and cognitive flexibility with educational status is significant; the relationship between cognitive flexibility and marital status is reported as inverse and two other relationships are reported to be direct. There are no significant relationships in other subscales with demographic characteristics; the relationship between demographic characteristics and overall cognitive abilities is also not significant. Regarding the second hypothesis, this hypothesis has been rejected in the present study. Based on the results of the research, none of the relationships between mood changes with demographic characteristics, whether in sub-scales and in the overall scores are not significant. This hypothesis has been reported significant in some relationships. Regarding the relationship between cognitive abilities and mood changes, some relationships are significant; regarding the relationships of all subscales of mood changes and total mood changes, these relationships with social cognition, anxiety symptoms with decision making, planning, social cognition and cognitive flexibility have been rejected. The relationship between the mean scores of overall cognitive abilities and the average of total mood changes are confirmed; this relationship is considered to be inversely significant. In the fourth hypothesis, there is a difference between the mean scores of all subscales of cognitive abilities and overall cognitive abilities in type II diabetic patients and healthy subjects. According to this finding, the fourth hypothesis is confirmed. Accordingly, these abilities differ in healthy subjects and type II diabetic patients. The mean scores of cognitive abilities in all subscales and the overall test in healthy subjects are higher and more than those with type II diabetes. Accordingly, people with type II diabetes have a lower overall memory, inhibition control and selective attention, decision making, planning, sustained attention, social cognition, cognitive flexibility, and overall cognitive abilities. The results of the current study are consistent with the study results of Berg et al. (2010), Chrisman et al. (2010), Elderen et al. (2010), Rubis et al. (2009), Ying et al (2009) outside the country and with the study results of Abadi et al (2008) inside the country. In the fifth hypothesis, there is a difference between the mean scores of all subscales of mood changes and overall mood changes in type 2 diabetic patients and healthy subjects. According to this finding, the fifth hypothesis is accepted; accordingly, these changes are different in healthy subjects and type 2 diabetic patients. The mean of mood changes in all subscales and the overall test in healthy subjects are lower and less than those with type II diabetes. Accordingly, type 2 diabetic patients experience more symptoms of anxiety, depression and mood changes than healthy people.
The overall results of the current research are as follows:
The results of the current study showed that in type II diabetic patients, only the relationship between sustained attention with employment status and cognitive flexibility with educational status are directly significant and the relationship between cognitive flexibility with marital status is inversely significant.
Conclusion
The relationship between the mean scores of overall cognitive abilities and the mean of total mood changes in type 2 diabetic patients is confirmed. The mean scores of cognitive abilities in all subscales and the overall test in healthy subjects are higher and more than those with type II diabetes. The mean of mood changes in all subscales and the overall test in healthy subjects are lower and less than those with type II diabetes.
Considering the impact of type II diabetes on cognitive abilities and mood changes, it is recommended that institutions and centers such as Welfare Organization, the Association of social Workers, Health Centers, and other centers in these areas provide Educational program workshops that aim to change cognitive ability and mood conditions.
References
1. Agha-Mollai, S.; Eftekhar, H.; Mohammad, K.; Sajani, A.; Shojaeizadeh; Nakhjavani, M.; Ghofranipour, F. (2004). The effect of educational intervention using interactive approaches on behavioral change, ALC hemoglobin and Health-related quality of life in diabetic patients. Journal of School of Public Health and the Institute of Health Research, 3 (4); 109.
2. Baghiyani Moghadam, M.; Afkhami Ardeghani, M.; Mazlomi, S.; and Saeedizadeh M. (2006). The study of Quality of life in type II diabetic patients in Yazd, Shahid Sadoughi University of Medical Sciences and Health Services of Yazd, 14 (4), 54-49.
3. Saduk W. A. and Saduk, B. (2008). Summary of Psychiatry (Volume II). Translation: Rezaei, F. Tehran: Arjomand.
4. Saduk B. and Saduk V. (2006). Summary of Psychiatry, Translation: Nusrat (Pourfakari, Volume II, Third Edition), Tehran: Shahr-e-Ab Publishing.
5. Shunde, N.; Shahr Jaray, Sh.; Sheikh Hosseini, R.; and Quorbayni, A. (2010). Effect of Heavy Strength Training and Metabolic Indicators, Quality of Life and Mental Health of Women with Type 2 Diabetes. Journal of Iranian Endocrine Sciences and Metabolism, 12 (3). 240 - 22.
6. Larijani, B.; Khorram Shahi Bayat, M.; Khalili Gorgani, M.; Bandarian, F.; Akhondzadeh, Sh. (2003). Relationship between diabetes and depression in diabetic patients referred to Shariati Hospital and Diabetes Association. Iranian Journal of Diabetes and Lipid, 3 (1): 77-82.
7. 2. Maligman M. P. and Rouznahan, V. (2004). Abnormal Psychology, Psychopathology. Seyyed Mohammad Salovan.
8. Vares, Z.; Zendegi, M.; Tabani, P.; Masoudi Alavi, N.; and Mir Baqer Ajriz, N. (2010). The study of Quality of Life and Its Related Factors in patients Referring to Diabetes Center in Kashan, Nursing Research Volume (178): 24-14.
9. Bai, Y, L . , Chiou, C, P, Change, Y,Y. , & L . Am, H .C (2008) correlates of depression in tipe 2 diabetic elderly patients; a correlational study. Enternational journal Nurs student, 45(4):571-90.
Author notes
rezapour.r@sbmu.ac.ir
