Artículos
AComparative Study of Ketofol and Thiopental Sodium in Patients undergoing Dilation and Curettage by General Anesthesia
Un estudio comparativo de Ketofol y sodio tiopental en pacientes sometidos a dilatación y curetaje por anestesia general
AComparative Study of Ketofol and Thiopental Sodium in Patients undergoing Dilation and Curettage by General Anesthesia
Revista Latinoamericana de Hipertensión, vol. 13, no. 6, pp. 515-519, 2018
Sociedad Latinoamericana de Hipertensión

This work is licensed under Creative Commons Attribution-NoDerivs 4.0 International.
Abstract: Considering that the combined drug, Ketofol has been used and its efficacy observed in patients, we have aimed to compare the effects of ketofol and thiopental sodium on patients who are undergoing dilatation and curettage. This study was conducted as a randomized controlled clinical trial. In this study, 150 patients undergoing dilatation and curettage after classification were randomly selected and enrolled. The first group received ketofol, while thiopental sodium was administered to the second group. Any change in hemodynamics or respiratory distress, including the occurrence of apnea or hypotension, desaturation and the need for respiratory support were recorded in both groups. Finally, after the completion of the surgery and transfer to the recovery room, the recovery rate of each group was recorded, and once they were conscious and alert, were questioned about their satisfaction. All of the patient information was entered into the SPSS v18 software, and the data were analyzed. This study was conducted on 150 patients undergoing curettage; the mean ages in the first and second groups were 31.82 ± 9.18 and 33.64 ± 11.39 years, respectively. Ninety two percent of patients in the ketofol group and 100% of the patients in the thiopental sodium group experienced apnea and needed respiratory support. About 25.3% of patients in the ketofol group and 44% of patients in the thiopental group required a re-dose of the drug for the anesthetic process. The duration of recovery in the ketofol group was lower than the other group. About 2.7% of the patients in the ketofol group and 12% of the patients in the thiopental group had hallucinations and delusions at the end of the operation Six patients in the thiopental group also had hiccups. The results of the present study showed that ketofol is a better drug than thiopental because of the duration of anesthesia, reducing the need for medication, the incidence of apnea, and the complications of anesthesia
Keywords: General anesthesia, Ketofol, Thiopental sodium, Dilatation, Curettage.
Resumen: Teniendo en cuenta que el fármaco combinado, Ketofol se ha utilizado y su eficacia se ha observado en pacientes, el objetivo fue comparar los efectos del ketofol y el sodio tiopental en pacientes que están en proceso de dilatación y legrado. Este estudio se realizó como un ensayo clínico aleatorizado controlado. En este estudio, 150 pacientes sometidos a dilatación y legrado después de la clasificación fueron seleccionados al azar y se inscribieron. El primer grupo recibió ketofol, mientras que el tiopental sódico se administró al segundo grupo. Cualquier cambio en la hemodinámica o dificultad respiratoria, incluida la aparición de apnea o hipotensión, la desaturación y la necesidad de asistencia respiratoria se registraron en ambos grupos. Finalmente, después de la finalización de la cirugía y el traslado a la sala de recuperación, se registró la tasa de recuperación de cada grupo, y una vez que estuvieron conscientes y alertas, se les preguntó acerca de su satisfacción. Toda la información del paciente se ingresó en el software SPSS v18 y los datos se analizaron. Este estudio se realizó en 150 pacientes sometidos a curetaje; Las edades medias en el primer y segundo grupo fueron 31.82 ± 9.18 y 33.64 ± 11.39 años, respectivamente. Noventa y dos por ciento de los pacientes en el grupo de ketofol y el 100% de los pacientes en el grupo de sodio tiopental experimentaron apnea y necesitaron asistencia respiratoria. Alrededor del 25,3% de los pacientes en el grupo de ketofol y el 44% de los pacientes en el grupo de tiopental requirieron una nueva dosis del fármaco para el proceso anestésico. La duración de la recuperación en el grupo de ketofol fue menor que en el otro grupo. Alrededor del 2,7% de los pacientes en el grupo de ketofol y el 12% de los pacientes en el grupo de tiopental tuvieron alucinaciones y delirios al final de la operación Seis pacientes en el grupo de tiopental también tuvieron hipo. Los resultados del presente estudio mostraron que el ketofol es un fármaco mejor que el tiopental debido a la duración de la anestesia, lo que reduce la necesidad de medicación, la incidencia de apnea y las complicaciones de la anestesia.
Palabras clave: Anestesia general, Ketofol, Thiopental sodium, Dilatación, Curetaje.
Introduction
About 211 million pregnancies occur annually all over the world, of which, 46 million lead to abortion1. Common abortion therapies include pharmaceutical and mechanical therapies.
Dilatation and curettage (D & C) is one of the mechanical methods used for abortion. In this operation, opening the cervix or dilatation is far more painful than curettage2.The anesthetic method for this operation can be general (GA) or regional, GA is the most common anesthetic approach based on the surgeon and patients’ wish. Because bleeding is common in this operation, maintaining the hemodynamic during anesthesia is very important. The duration of the stay in the hospital is often short, and the patient can be discharged if they do not develop any complications3. So, it's best to use a method to get the patient to wake up and recover faster. Therefore, the choice type of drug in the general anesthesia should be carefully investigated and the best medicine be chosen4. Thiopental induces anesthesia by bonding to the position of ionophore chloride in the Gaba aminobutiric acid receptor (GABA) and inhibiting this receptor about 30 seconds after injection. It has no analgesic effect, but its effect on the cardiovascular system and the reduction of vascular resistance leads to hypotension and sometimes, reflex tachycardia5. Propofol is a drug with rapid onset and hepatic clearance after intravenous administration. It has direct antinociceptive effects but no analgesic effect. On the other hand, Ketamine acts on the NMDA via antagonistic effects, which increases the systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR). Ketamine has dose-dependent effects of inaccuracy and analgesia6. Ketofol is a combination of two drugs (propofol and ketamine) and is used in anesthesia.
Considering that ketofol and its efficacy has been observed among patients, we have aimed to compare the effects of ketofol and thiopental sodium on the patients undergoing dilation and curettage.
Methods and Materials
This study was approved by ethical committee of Ardabil University of medical sciences (1395.88) and written informed consent was obtained from all subjects, a legal surrogate, or the requirement for written informed consent was waived by ethical committee. The clinical trial with the IRCT2017031923559N9 code (Somaiyeh Matin, 2017.4.24) was registered before patient enrollment authors. This randomized controlled clinical trial was conducted before on patients with missed or incomplete abortion undergoing dilatation and curettage. In this study, 150 patients aged over 16 years and candidates for dilation and curettage with ASA class 1 and 2 were enrolled after obtaining informed consent. Patients with a history of susceptibility to propofol and other intravenous anesthetic drugs, patients with substance abuse, alcohol and psychotropic drugs, as well as patients with gastrointestinal ulcers, kidney disease or hypertension, and hypertension, osteopenia and osteoporosis, and uncontrolled hypertension were excluded. The patients were randomly classified into two groups and placed in two blocks
A and B. Group A or Group 1 were the ketofol group and group B or Group 2 were the thiopental sodium group. The preparation of the drugs was carried out by the anesthesia nurses, and after delivery of the syringes, they were covered with a white label. The drugs were administered by an anesthesiologist who did not know the drug content. In both groups, the patients in the operating room underwent cardiopulmonary monitoring. Then, the appropriate intravenous route was established, and the patients were hydrated, and received oxygen by facemask. Midazolam 0.05 mg / kg, fentanyl 1 μg / kg, and lidocaine 1 mg / kg for each patient were administered.
Subsequently, the first group received ketofol (which was mixed with 2: 1 propofol and ketamine in a syringe), and the second group received thiopental sodium 3 mg / kg body weight. The medication injection rate was 10 mg / sec. Any change in the hemodynamics or respiratory distress including the occurrence of apnea or hypotension, desaturation and the need for respiratory support were recorded in both groups. Eventually, after completion of surgery and transfer to the recovery room, the patients were questioned about satisfaction and anesthesia. All patient information was completed by the anesthesiologist. Finally, all the data was entered into the SPSS v18 statistical program and the data was analyzed. In this study, the t-test and chi-square test were used and P value less than 0.05 was considered significant.
Results
In this study, 150 patients were evaluated in two groups (the first group receiving the ketofol and the second group receiving the thiopental sodium). The mean age of the patients in the first group was 31.82 ± 9.18 years and in the second group was 33.64 ± 11.36 years (P = 0.258).
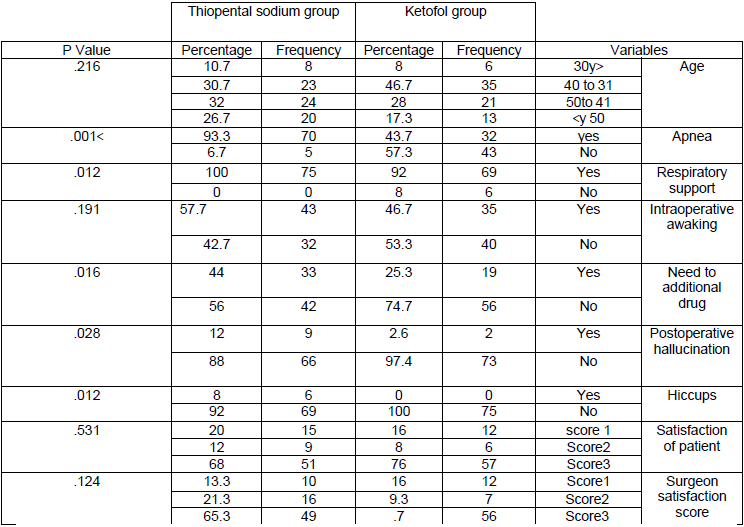
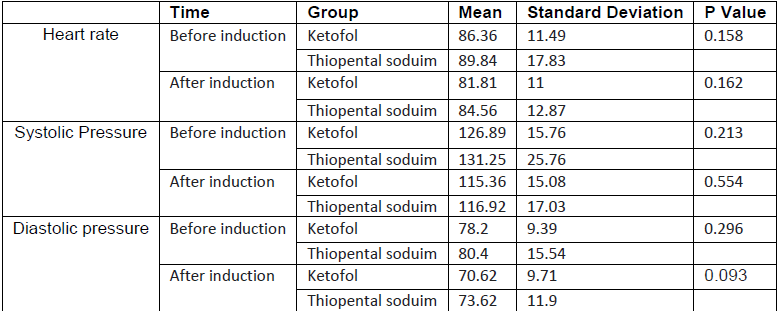
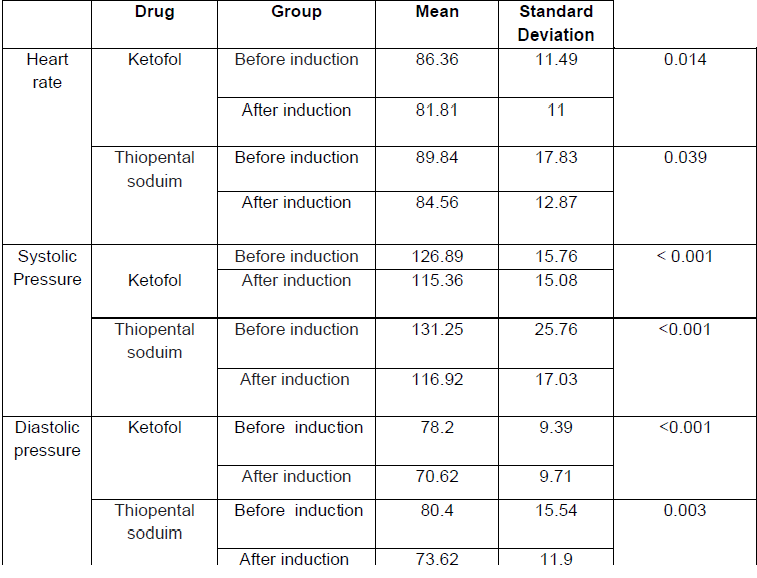
The incidence of apnea and the need for respiratory support in the thiopental sodium group were higher than the ketofol group (Table 1). Also, the mean duration of apnea in the first and second groups were 50.75 ± 27.77 and 99.22 ± 58.17 seconds, respectively (P <0.001). After recording the systolic, diastolic blood pressure and heart rate before and after induction did not show significant differences in the two groups (Table 2), but in each group, there were significant differences in the vital signs (Table 3). In this study, no cases of hypotension and bradycardia were reported. Awakening during anesthesia showed no significant difference in the two groups, but the amount of drug re-administration during anesthesia was significantly lower in the ketofol group than in the other group (P = 0.016) (Table 1). The mean arrival time of the Aldrete score was 9 and recovery in the ketofol, and thiopental sodium groups were 13.21 ± 3.13 and 19.12 ± 21.5 minutes, respectively (P <0.001). Drug complications in Group A were higher than Group B, but the satisfaction of patient and surgeon for the anesthetic level did not show any significant difference in the two groups (Table 1).
Discussion
Various studies have demonstrated that the effect of the combination of propofol and ketamine for the induction of anesthesia is different when injected by a syringe due to different kinetic effects on each other, and the combined drug (Ketofol) produces more effective sedative effects7.
In the study by Sawas et al., 52% of the recipients of ketofol and 73% of the propofol recipients experienced respiratory supplements (P = 0.035) 8. In a study by Goh et al., the incidence of apnea in propofol (3.3%) was lower than ketofol, and in ketofol (6.3%) was less than fentanyl + propofol (23.1%)9. Frey et al. reported respiratory suppression in propofol recipients more than cofactor recipients10. Jalili, in his meta-analysis study also stated that ketofol can significantly reduce respiratory complications, including depression of the respiratory system11. However, in the study by David and colleagues, there was no significant difference in the incidence of apnea in propofol and ketofol12. In this study, it was found that the incidence of apnea and the need for respiratory support in the thiopental sodium recipients was higher than that of ketofol. Its incidence in this study was more than other studies, which is probably due to the definition of apnea (respiratory discontinuation of 10 seconds) in this study and its difference with other studies. In their study, Ustun et al. studied the effects of ketofol (0.5 mg/kg) and thiopental (3 mg / kg) on MRI candidates; they observed that the heart rate decreased in both groups. However, there was no significant difference between the two groups in relation to each other13. Gholipour et al. also stated that ketofol produces a more stable hemodynamic than the other two groups (etomidated, thiopental + ketamine)14. Also, Garg et al. reported the ketamine and propofol combination as the best combination for the hemodynamic stability of patients during anesthesia15. Saleem et al. reported the hemodynamic stability in ketofol as more than in propofol and thiopental16. The combination of propofol and ketamine has a high degree of hemodynamic stability in other studies by Furuya et al., Ghatak et al., Goh et al., and Ozgul et al. In this study, despite the fact that there was a decrease in blood pressure and heart rate in both groups, no hemodynamic instability was reported, and all patients had stable hemodynamic parameters9,17,18,19. Like the previous studies, the two drugs, ketofol and thiopental, showed decreased but stable vital signs.
In a study by Ustun et al., the duration of sedation was 36.2 minutes for ketofol recipients and 24.24 minutes for the thiopental sodium patients, which was statistically significant13. The duration of hospital stay was 20.4 minutes in the ketofol group and 4.9 minutes in the thiopental group, respectively. In a study by Del Pizzo et al., the duration of sedation was 20 minutes in the propofol group (propofol + ketamine with separate infusion) and recovery time was 18 minutes. In the ketamine group, it was 19 minutes (P = 0.469) and the recovery time was 11, 9, and 12 minutes (P = 0.704)20. A study by Coulter et al. compared proportions of ketamine and propofol in the ketofol drug and reported that a ratio of 1 to 3 ketamine to propofol was appropriate in short procedures (5 to 20 minutes), and by administration of this drug can be prevented from multiple injections with a ratio of 1 to 4. But the injection of ketofol with a ratio of 1 to 4 can increase recovery time to over 20 minutes21. In a study by Frey et al., the sedation time in recipients of ketofol and propofol was 164 and 235 seconds, respectively. In this study as in other studies, the need for re-administration of ketofol was less than thiopental. On the other hand, the ketofol recipients had a shorter duration of recovery10.
Regarding side effects, Sawas et al. reported that ketofol has fewer side effects than propofol, and it is generally accepted as a better anesthetic drug8. Gholipur et al. also reported that 15% of recipients had muscle contractions, and 27.5% had nausea and vomiting while receiving ketamine + thiopental (with separate infusion), 20% had muscle contractions, and 7.5% had nausea and vomiting during surgery, while the patients receiving ketofol did not have any side effects14. Jalili et al. reported that ketofol had significantly fewer complications than other anesthetic drugs, including hallucinations, muscle rigidity, nausea, and vomiting11. A review of other studies has found that propofol in patients reduces nausea and vomiting; the mechanism of this event is not well understood22, but its adjuvant effects or its weak antagonistic effects on the subcortical route can be considered23.
Conclusion
The results of this study showed that ketofol is a better drug than thiopental for the induction of anesthesia, reducing the need for medication, the incidence of apnea, and the complications of anesthesia.
References
1. World Health Organization. The world health report 2005: Make every mother and child count. Geneva: World Health Organization; 2005.
2. Mehdizadeh A, Akbarian A, Ghasemi A, Ardjomand F. Comparison of lidocaine and salin effect in cervical anesthesia on level of pain during curtage. RJMS. 2000; 7 (21):220-222(Persian).
3. Sahin L, Sahin M, Aktas O, Kilic E, Mandollu E. Comparison of propofol/ketamine versus propofol/alfentanil for dilatation and curettage. Clin Exp Obstet Gynecol. 2012;39 (1):72-5.
4. MacKay HT, Schulz KF, Grimes DA. Safety of local versus general anesthesia for second-trimester dilatation and evacuation abortion. Obstet Gynecol. 1985 Nov; 66 (5):661-5.
5. Liu H, Yao S. Effect of thiopental sodium on the release of glutamate and gamma-aminobutyric acid from rats prefrontal cortical synaptosomes. J Huazhong Univ Sci Technolog Med Sci. 2004;24(6):602-4.
6. Miller R, Eriksson L, Fleisher L, Wiener-Kronish J, Cohen N, Young W. Miller's Anesthesia. 8th ed, Elsevier Health Sciences. p 920.
7. Yan JW, McLeod SL, Iansavitchene A. Ketamine-Propofol Versus Propofol Alone for Procedural Sedation in the Emergency Department: A Systematic Review and Meta-analysis. Acad Emerg Med. 2015 Sep;22(9):1003-13.
8. Sawas A, Youngquist ST, Madsen TE, Davis VW. Combined ketamine and propofol sedation vs propofol sedation for emergency department procedures: a prospective randomized trial. Acad Emerg Med 2013;62:S1.
9. Goh PK, Chiu CL, Wang CY, Chan YK, Loo PL. Randomized double-blind comparison of ketaminepropofol, fentanyl-propofol and propofol-saline on haemodynamics and laryngeal mask airway insertion conditions. Anaesth Intensive Care. 2005 Apr;33(2):223-8.
10. Frey K, Sukhani R, Pawlowski J. Propofol versus propofol-ketamine sedation for retrobulbar nerve block: omparison of sedation quality, intraocular pressure changes, and recovery profiles. Anesth Analg. 1999; 89:317–321.
11. Jalili M, Bahreini M, Doosti-Irani A, Masoomi R, Arbab M, Mirfazaelian H. Ketamine-propofol combination (ketofol) vs propofol for procedural sedation and analgesia: systematic review and metaanalysis. Am J Emerg Med. 2016 Mar;34(3):558-69.
12. David H, Shipp J. A randomized controlled trial of ketamine/propofol versus propofol alone for emergency department procedural sedation. Ann Emerg Med. 2011 May;57(5):435-41.
13. Ustun YB, Atalay YO, Koksal E, Kaya C, Ozkan F, Sener EB, et al. Thiopental versus ketofol in paediatric sedation for magnetic resonance imaging: A randomized trial. J Pak Med Assoc. 2017 Feb;67(2):247-251.
14. Gholipour Baradari A, Firouzian A, Zamani Kiasari A, Aarabi M, Emadi SA, Davanlou A, et al. Effect of Etomidate Versus Combination of Propofol-Ketamine and Thiopental-Ketamine on Hemodynamic Response to Laryngoscopy and Intubation: A Randomized Double Blind Clinical Trial. Anesth Pain Med. 2016 Jan 10;6(1):e30071.
15. Garg K, Grewal G, Grewal A, Singh A, Mishra A, Nar AS, Bawa A. Hemodynamic responses with different dose of ketamine and propofol in day care gynecological surgeries. J Clin Diagn Res. 2013 Nov; 7(11):2548-50.
16. Saleem S, Board DI, Naaman K. An interventional comparative study of haemodynamic effects of induction doses of propofolthiopentone and propofol-ketamine combinations. Anaesth Pain Intens Care. 2010;14(2):82–87.
17. Furuya A, Matsukawa T, Ozaki M, Nishiyama T, Kume M, Kumazawa T. Intravenous ketamine attenuates arterial pressure changes during the induction of anaesthesia with propofol. Eur J Anaesthesiol. 2001;18 (2):88–92.
18. Ghatak T, Singh D, Kapoor R, Bogra J. Effects of addition of ketamine, fentanyl and saline with Propofol induction on hemodynamics and laryngeal mask airway insertion conditions in oral clonidine premedicated children. Saudi J Anaesth. 2012;6(2):140–4.
19. Ozgul U, Begec Z, Karahan K, Ali Erdogan M, Said Aydogan M, Colak C, et al. Comparison of Propofol and Ketamine-Propofol Mixture (Ketofol) on Laryngeal Tube-Suction II Conditions and Hemodynamics: A Randomized, Prospective, Double-Blind Trial. Curr Ther Res Clin Exp. 2013;75:39–43.
20. Del Pizzo J, Agha BS, Downes K, Mularoni P. Efficiency in sedation for forearm fracture reduction in children: propofol vs. ketamine-propofol vs. ketofol. Pediatric Emergency Care Conference: American Academy of Pediatrics, AAP Section on Emergency Medicine National Conference and Exhibition. 2011;27:10.
21. Coulter FL, Hannam JA, Anderson BJ.Ketofol dosing simulations for procedural sedation. Pediatr Emerg Care. 2014 Sep;30(9):621-30.
22. Sümer C, Erhan ÖL, Özer AB, Yildiz F. Effects of etomidate on blood cortisol, insulin, and glucose levels and PONV rates in smokers. Turkish J Med Sci. 2012;42(5):810–5.
23. Unal Y, Ozsoylar O, Arslan M, Sariguney D, Akcabay M. Comparison of the efficacy of propofol and metoclopramide in preventing postoperative nausea and vomiting after middle ear surgery. Saudi Med J. 2009;30(6):778–82.