Artículos
Full Mouth Reconstruction in a Patient with Severely Worn Dentition by Restoring the Vertical Dimension of Occlusion: A Case Report
Reconstrucción bucal completa en un paciente con dentición gravemente desgastada al restaurar la dimensión vertical de la oclusión: reporte de un caso
Full Mouth Reconstruction in a Patient with Severely Worn Dentition by Restoring the Vertical Dimension of Occlusion: A Case Report
Revista Latinoamericana de Hipertensión, vol. 13, no. 6, pp. 544-546, 2018
Sociedad Latinoamericana de Hipertensión

This work is licensed under Creative Commons Attribution-NoDerivs 4.0 International.
Abstract: This clinical report describes the full mouth reconstruction in a patient with severely worn dentition. The treatment plan involved the metal-ceramic complete cast crowns and partial removable dental prostheses. The patient had a loss of vertical dimension of occlusion (VDO) because of severe attrition. We restored the VDO. During the recall sessions, the treatment plan was successful.
Keywords: Worn dentition, Tooth relationship, Vertical dimension of occlusion, Full mouth reconstruction.
Resumen: Este informe clínico describe la reconstrucción bucal completa en un paciente con dentición severamente desgastada. El plan de tratamiento incluía coronas completas de metal-cerámica y prótesis dentales removibles parciales. El paciente tuvo una pérdida de la dimensión vertical de la oclusión (VDO) debido a un desgaste severo. Hemos restaurado el VDO. Durante las sesiones de retiro, el plan de tratamiento fue exitoso.
Palabras clave: dentición desgastada, relación dental, dimensión vertical de la oclusión, reconstrucción bucal completa.
Introduction:
The restoration of severely worn dentition presents one of the greatest challenges in dentistry1. Tooth wear is a multifactorial condition that is affected by several factors that altered chewing pattern due to teeth loss or lack of dental prosthesis is one of these factors2. If tooth wear is caused by attrition, all worn surfaces are in contact with the opposing teeth, during centric occlusion and lateral excursions. When the enamel is worn off a tooth, the soft underlying dentin may wear more rapidly, which may allow the overeruption of the opposing tooth with sound enamel. This can cause occlusal problems3.
The loss of posterior occlusal support, as well as posterior occlusal pre-maturities, may cause the increased use of the anterior teeth, which results in their wear4. When the rate of tooth wear exceeds the compensatory mechanisms, such as tooth eruption and the development of associated alveolar bone, a loss of vertical dimension of occlusion (VDO) is observed5
In this paper, we report on a patient with severely worn dentition. We then present our treatment plan for restoring the patient’s occlusion and improving their appearance.
Clinical report: A 52-year-old man was presented to our department complaining that he was not satisfied with the appearance of his teeth; his teeth showed progressive wear and he had problems speaking and chewing (Fig.1).

Fig. 1
Smile view of the patient
The patient reported that he had previous pocket surgery in both jaws and that some of his teeth had been extracted because of extensive caries and periodontitis. He also mentioned that he had endodontic treatment and amalgam and composite restorations in some teeth because of caries or attrition (Figs. 2 and 3).

Fig.2:
Pre-treatment panoramic radiograph
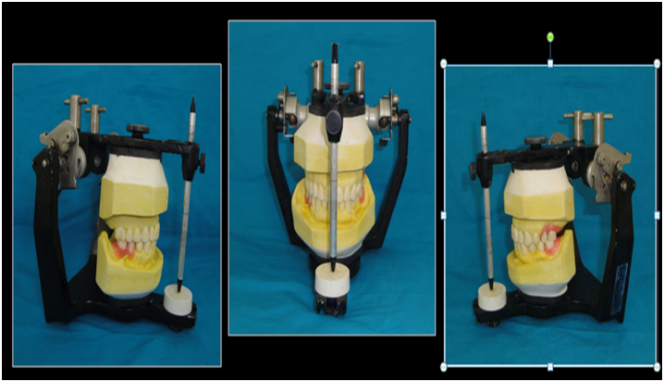
Fig. 3.
Diagnostic wax-up
The clinical examination revealed attritional facets on the anterior teeth and premolars in both jaws. There were multiple abfractions and caries in cervical surface of the remaining teeth. The patient had a loss of VDO because of severe attrition. The maxillary left second premolar and molar teeth had an unfavorable crown–root ratio and furcation involvement (Fig.4).

Fig. 4.
Smile view with interim restorations in new VD
The anterior and posterior occlusal planes were uneven because of supra-eruption and the drifting of the remaining teeth into the edentulous areas. The occlusal examination revealed destructive non-working side contacts.
The severe wear was attributed to long-term posterior edentulism, supra-eruption, and the drifting of teeth into the adjacent and opposing edentulous areas, which resulted in premature contact and bruxism. The wear was intensified following the exposure of dentin and the progression of periodontal disease. Tooth mobility further aggravated the malocclusion. The poor oral hygiene practices resulted in multiple cervical caries. Our patient was assigned to the third category in the Turner and Missirlian6 classification for patients with extensively worn dentition (Table 1).
| Category No. 1 | Excessive wear Loss of the occlusal vertical dimension |
| Category No. 2 | Excessive wear No loss of the occlusal vertical dimension Space available for the placement of restorations because of continuous eruption of the teeth Adequate posterior support Long history of bruxism |
| Category No. 3 | Excessive wear No loss of the occlusal vertical dimension Limited space for the placement of restorations Increase in the occlusal vertical dimension is needed |
First, the mandibular anterior occlusal plane, in the rest position, was determined based on phonetics and smile esthetics. The posterior occlusal planes were determined using intraoral landmarks and the Broadrick occlusal plane analyzer. A diagnostic wax-up was produced in these planes (Fig.5).

Fig. 5.
Smile view with final restorati
Interim restorations were fabricated after caries removal and primary preparation. The VDO was estimated using several methods, such as phonetics, inter-occlusal distance, and swallowing5. The restorations were cemented with non-eugenol zinc-oxide cement (DentoTemp, ITENA, France, Paris). A removable interim prosthesis was fabricated for the mandibular edentulous areas (Figs.6).

Fig. 6.
Hard occlusal splint to prevent nocturnal parafunctional occlusal wear
The patient used them for 3 months to adapt to it.
During the 3-month follow-up after the interim restorations, the available treatment options were thoroughly explained to the patient. Because of financial concerns, the patient could not afford the placement of dental implants in the edentulous areas. Therefore, the agreed treatment plan included the metal-ceramic complete cast crown of the teeth and the preparation of partial removable dental prostheses for the edentulous areas; the plan was that the patient would be able to financially afford the dental implants at a later date.
Initially, the PI decreased to 20 percent due to oral hygiene practice. The maxillary second premolar and molar teeth were extracted because of an improper crown–root ratio. An impression was made from the interim restorations using hydrocolloid impression material; stone casts were made from the impression. The anterior guide table was then fabricated.
The final impression was made with a two-stage putty-wash method (Panasil, Kettenbach, Germany, Eschenburg) using a prefabricated metal tray. The final casts were mounted on an articulator using a cross-mounting technique. Initially a full contour wax-up was done for the metal–ceramic restorations.
Guide planes were created using a surveyor and the rest seats were carved. The cut-back was done using the putty indexes, and non-precious metal frameworks (VeraBond II, Aalba Dent, Fairfield, CA) were fabricated. The fit, retention, stability, and occlusion of the frameworks were checked intraorally and radiographically. The porcelain (Kuraray Noritake Dental Inc., Japan, Tokyo) veneering was then applied. Porcelain fused to the metal restorations was cemented with non-eugenol cement.
For the fabrication of partial removable dental prostheses, primary impressions were made of both jaws and custom acrylic trays were fabricated. The final impressions, after border molding, were made using medium-body addition silicone (Panasil, Kettenbach, Germany, Eschenburg). The frameworks were cast in a nickel–chromium alloy (Vera PDI, Aalba Dent Inc., Fairfield, CA) and the fit was checked intraorally. Finally, it was delivered to the patient. A hard occlusal splint was made to prevent nocturnal parafunctional occlusal wear
Follow-up: After 3 months, the temporary cement was replaced with glass ionomer cement (Luting and Lining Cement, GC Corp., Japan, Tokyo). The patient was followed up for 6 months, 1 year, and 3 years. During the recall sessions, there was no evidence of temporomandibular joint problems or tooth or crown fracture. The patient was satisfied and had no complaints.
Conclusion:
In this clinical report, the patient presented with excessive tooth wear and uneven anterior and posterior occlusal planes. The treatment plan included correcting the anterior and posterior occlusal planes and restoring the VDO. The patient indicated no problems and the treatment plan was considered to be successful. In full-mouth rehabilitation, if the centric and eccentric occlusions are corrected, the treatment will be successful even if the VDO has been restored.
References
1. Dawson P. Functional Occlusion: From TMJ to Smile Design. Philadelphia, Mosby, 2006:430-52.
2. Katsoulis J, Nikitovic SG, Spreng S, Neuhaus K, Mericske-Stern R. Prosthetic rehabilitation and treatment outcome of partially edentulous patients with severe tooth wear: 3-years results. J Dent.2011; 39(10):662-71.
3. Crothers AJ. Tooth wear and facial morphology. J Dent.1992; 20(6): 333-41.
4. Moslehifard E, Nikzad S, Geraminpanah F, Mahboub F. Full-mouth rehabilitation of a patient with severely worn dentition and uneven occlusal plane: A clinical report. J Prosthodont.2012; 21(1): 56-64.
5. Moshaverinia A, Kar K, Aalam AA, Takanashi K, Kim JW, Chee WW. A multidisciplinary approach for the rehabilitation of a patient with an excessively worn dentition: A clinical report. J Prosthet Dent.2014; 111(4): 259-63.
6. Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent.1984; 52(4): 467-74.
Author notes
mahboubi.sh@muk.ac.ir