Artículos
Effect of sleep hygiene on prosocial and antisocial behaviour
Efecto de la higiene del sueño en la conducta prosocial y antisocial
Effect of sleep hygiene on prosocial and antisocial behaviour
Interdisciplinaria, vol. 41, núm. 2, pp. 12-13, 2024
Centro Interamericano de Investigaciones Psicológicas y Ciencias Afines

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-CompartirIgual 4.0 Internacional.
Recepción: 01 Mayo 2022
Aprobación: 30 Noviembre 2022
Abstract: Sleep is an important factor influencing the balance between adaptive and maladaptive behaviours and is especially relevant in the adolescent and young adult population where there is an (ab)use of information and communication technologies (ICT) that can interfere with normal sleep needs. In turn, there is evidence that shows that education on more appropriate ways of sleeping improves sleep quality, but the effect that sleep hygiene education may have on social behaviour has not been studied. Therefore, the present study aims to observe the effect on prosocial and antisocial tendencies of improving sleep hygiene through an intervention. Participants are 121 young adults aged 18-25 years (83.5 % female) living in Spain. An improvement in sleep quality was expected in those who underwent the intervention and those who showed greater adherence were expected to show an increase in prosocial measures and a reduction in antisocial measures. To test the hypotheses, hypothesis testing was carried out between the groups in the pre-test, analysis of covariance to check for differences between the groups in the post-test and pairwise comparisons to study the differences. The results showed that there was no difference between the groups before starting the intervention and that the programme produced a reduction in certain variables associated with antisocial behaviour. Our findings imply that an improvement in sleep hygiene for a short period of time has the effect of a significant reduction in certain variables related to antisocial behaviour, so that interventions that promote an increase in sleep hygiene could have a positive impact on social interaction.
Keywords: sleep habits, social behaviour, young adults, sleep hygiene education, healthy sleep behaviours.
Resumen: Se entiende por conducta prosocial aquel comportamiento voluntario dirigido a ser beneficioso para los demás, y por conducta antisocial, cualquier comportamiento que refleje una infracción de las reglas o normas sociales, destacando la agresión. El sueño es un importante factor que influye en la balanza entre comportamientos adaptativos y desadaptativos. Además, el sueño tiene especial relevancia en adolescentes y adultos jóvenes, donde existe un (ab)uso de las tecnologías de la información y la comunicación (TIC), que puede interferir con las necesidades habituales de sueño. A su vez, existe evidencia que demuestra que una educación sobre maneras más adecuadas de dormir tiene mejoras sobre la calidad del sueño, pero no se ha estudiado el efecto que pueda tener una educación en higiene del sueño sobre la conducta social. Por ello, el presente estudio tiene por objetivo observar el efecto que puede tener sobre las tendencias prosociales y antisociales la mejora de la higiene del sueño a través de una intervención. El estudio consistió en una muestra de 121 adultos jóvenes de entre 18 y 25 años (83.5 % mujeres) residentes en España. Los participantes se distribuyeron en dos grupos: el grupo experimental, que recibió una formación en medidas de higiene del sueño -que pusieron en práctica-, y el grupo control. Se espera una mejora en la calidad del sueño en aquellas personas sometidas a la intervención en medidas de higiene del sueño (hipótesis 1), también se espera que aquellos participantes que muestren más adherencia a las recomendaciones sobre higiene del sueño presenten un aumento en la puntuación de las medidas prosociales (hipótesis 2), así como una reducción en las medidas relacionadas con la conducta antisocial (hipótesis 3a), en especial con la agresividad reactiva (hipótesis 3b), mientras que los participantes que no hayan seguido las recomendaciones sobre higiene del sueño no mostrarán diferencias significativas en ambas mediciones (hipótesis 4). Por último, se espera un mayor deterioro de la calidad del sueño en aquellos participantes con un mayor uso de pantallas digitales en las horas previas a acostarse (hipótesis 5). Para contrastar las hipótesis, se realizaron: 1) pruebas de contraste de hipótesis entre el grupo control y los experimentales, en el pretest, para comprobar la no existencia de diferencias entre ambos grupos antes de comenzar la aplicación de la intervención en el grupo experimental, 2) análisis de covarianza que permitieran comprobar si existen diferencias entre los grupos controles y experimentales en el post-test, pero eliminando la influencia de los niveles previos en el pretest y 3) comparaciones por pares para estudiar las diferencias entre el grupo control y los experimentales. Los resultados mostraron que antes de implementar la intervención no había diferencias significativas entre el grupo control y los experimentales en el conjunto de variables evaluadas, mientras que se observaron diferencias estadísticamente significativas pretest-postest entre los grupos experimentales y control; en concreto se observó que el programa produjo una reducción de ciertas variables asociadas a la conducta antisocial. El programa potenció un aumento de la calidad del sueño, aumentando la calidad de sueño en los participantes que se sometieron al programa de intervención. Aunque el programa potenció una mejoría de ciertas variables prosociales, donde más efecto tuvo fue en la reducción de las variables relacionadas con la conducta antisocial. Por lo tanto, estos hallazgos implican que una mejoría de la higiene del sueño durante un periodo corto de duración tiene como efecto una importante reducción de ciertas variables relacionadas con la conducta antisocial, por lo que intervenciones que permiten un aumento de la higiene del sueño podrían tener una repercusión positiva en la interacción social.
Palabras clave: hábitos de sueño, comportamiento social, adultos jóvenes, educación higiene sueño, comportamientos saludables sueño.
Introduction
Prosocial behaviour has been shown in numerous research studies to be a protective factor in childhood and adolescence as well as in early adulthood, as it inhibits antisocial behaviour while promoting personal and socially adaptive behaviours (Balabanian & Lemos, 2020; Carlo et al., 2014; Tur-Porcar et al., 2016). Prosocial behaviour is understood as voluntary behaviour aimed at being beneficial to others, involving sharing, caring, comforting and/or helping (Eisenberg et al., 2006). Furthermore, prosocial behaviour shows an inverse relationship with antisocial behaviour, understood as any behaviour that reflects an infraction of social rules or norms, highlighting aggression (Tur-Porcar et al., 2016), which has been conceptualised in a multitude of ways, but the proposal made by the research group of Kenneth Dodge et al. (Crick & Dodge, 1996) can be highlighted, which distinguishes, on the one hand, reactive aggression understood as those behaviours that occur as a reaction to a provocation or a perceived threat, real or imagined, and, on the other hand, proactive aggression, understood as those actions intentionally triggered to resolve conflicts or to achieve benefits, rewards or reinforcements valued by the aggressor (Andreu et al., 2009).
There are a number of factors that influence the balance between adaptive and maladaptive behaviours, one of them, which will be the subject of this study, being sleep (Dickinson & McElroy, 2017). Sleep plays a central role in the regulation of multiple psychological and biological processes, including the maintenance of immune and metabolic balance, the homeostasis of basic physiological processes, and the facilitation of learning and memory (Chee & Chuah, 2008; Dattilo et al., 2011). In both the short and medium term, sleep problems could lead to reduced work and/or academic productivity (Espie et al., 2012), increased likelihood of multiple psychopathologies (Soehner & Harvey., 2012), weight gain (Cizza, 2011), worsening muscle recovery (Dattilo et al., 2011), increased risk of developing diabetes (Vgontzas et al., 2009) or cardiovascular disease (Lao et al., 2018) and, in general, worsening physical and psychological health (Liu & Chen, 2019; Rappoport, 2019). In addition, multiple studies suggest that sleep, and specifically sleep deprivation, has a significant effect on social behaviour and aggression (Dickinson & McElroy, 2017; Solomon & Zeitzer, 2019).
There are a number of variables that have received greater attention in their relationship with prosociality, such as empathy, which has shown great importance in facilitating prosocial behaviour and inhibiting aggression, acting as a protective factor for the person. Empathy is understood as the emotional response that is made due to the understanding of the situation or state of another person, being this emotional response similar to what the other person is feeling (Ortiz et al., 2011; Tur-Porcar et al., 2016). Another variable that different studies show as a facilitator of prosocial behaviour is emotional self-efficacy, understood as a set of beliefs that a person holds regarding the effectiveness of their behaviour in facing or managing the different demands and challenges presented by the environment (Pereyra Girardi et al., 2019).
In turn, we find other variables associated with maladjusted or antisocial behaviour, such as emotional instability, understood as a person's difficulty in responding appropriately to the intensity or magnitude of a stimulus, or negative emotional states, which produce greater emotional reactivity to stress (Román et al., 2016). Along with emotional instability, another facilitating variable of aggression is anger, which has been classified into state and trait anger. Anger state refers to a temporary experience of feelings of rage and tension, and trait anger is a frequent behaviour that involves a series of facial expressions and physiological variations that can lead to aggression at all levels (García-Padilla, 2017).
The relationship between sleep and prosocial behaviour has not received much attention, yet the existing literature suggests that sleep deprivation may reduce prosocial behaviours (Anderson & Dickinson, 2010; Dickinson & McElroy, 2017; Rilling & Sanfey, 2011). Studies report that the prefrontal cortex (PFC), which develops later than other brain areas (Benenson et al., 2007), plays an important role in prosocial choices (Chee & Chuah, 2008), and is an area vulnerable to adverse sleep or circadian states (Dickinson & McElroy, 2012). Other authors, such as Dickinson and McElroy (2017) suggest that prosocial behaviour is affected by poor sleep hygiene due to reduced deliberative thinking.
In reference to aggression, it is found that research has not paid much attention between sleep and, on the one hand, reactive aggression (Kempes et al., 2005; Orobio de Castro et al., 2005) and, on the other hand, proactive aggression (Arsenio et al., 2009), which is why the understanding of the dynamics between sleep and aggression is limited (Barker et al., 2016). Nevertheless, pioneering studies in the 1980s suggested that aggression and impulsivity are correlated with the duration and frequency of the surface phases of sleep (Schubert, 1977) or highlighted irritability and emotional instability after an unsatisfactory period of sleep as mediators between aggression and sleep (Cutler & Cohen, 1979; Roth & Lutz, 1976). Such a relationship has been found in subjects with sleep apnoea (Bardwell et al., 1999; Flemons & Tsai, 1997) and prison populations (Barker et al., 2016; Elger, 2003), among others. More recent research indicates that hostility is the component of aggression most strongly associated with sleep quality (Ireland & Culpin, 2006).
As mentioned above, there is research that has pointed to the relationship between sleep and different facets of social behaviour such as prosociality and aggression (Anderson & Dickinson, 2010;Solomon & Zeitzer, 2019), but there is no research that delves into the effect that sleep habits may have on the different variables that favour or inhibit prosociality, such as empathy or emotional instability. In turn, there is evidence showing that education on more appropriate ways of sleeping, based on an increase in knowledge about sleep, improves the quality of sleep of individuals in populations as diverse as patients receiving chemotherapy (Zengin & Aylaz, 2019), elite athletes (O'Donnell & Driller, 2017) or young university students (Hershner & O'Brien, 2018), but the effect of sleep hygiene education on social behaviour has not been studied. Such education focuses on aspects such as sleeping at least seven hours and on a regular schedule throughout the week, having an active lifestyle and a healthy diet, avoiding caffeine, alcohol and nicotine, exposing oneself to sunlight during the day and avoiding artificial light in the hours before bedtime, among other measures (Walker, 2017).
This study has focused on a young adult population. With the onset of adolescence, a number of sleep alterations occur. There is an increased preference for the evening-type circadian phase (Carskadon et al., 1993), along with changes in sleep-wake homeostasis that favour late nights throughout adolescent development (Jenni et al., 2005; Taylor et al., 2005). The profound changes in sleep–wake regulation and circadian biology occurring during adolescence and other psychosocial factors can affect the quality and quantity of sleep in adolescents and young adults. These changes include school start times, which increase the prevalence of inadequate sleep (Dahl & Lewin, 2002; Owens et al., 2014). Furthermore, sleep is particularly relevant in adolescents and young adults, especially in our culture where there is an (ab)use of information and communication technologies (ICT) that can interfere with the usual sleep needs (Bruce et al., 2017; Lemola et al., 2015; Lupano Perugini & Castro Solano, 2021), especially due to the use of social networks by this population group, which has become a habitual experience, and which can influence their psychological and social development (Pertegal-Vega et al., 2019). In this regard, it is important to say that even though prosocial behaviour begins to emerge in childhood, it continues to develop during adolescence and early adulthood (Eisenberg et al., 2002). In turn, through online behaviour, antisocial behaviours can be shown due to problematic internet use, such as cyberaggression (Romera Félix et al., 2021). This is why the relationship between sleep quality loss and ICT abuse may be a facilitator of antisocial behaviour. Therefore, the need for interventions that promote healthy sleep behaviours is particularly relevant (Dietrich et al., 2016), especially at a critical age such as late adolescence and early adulthood, which will mark the subsequent development of the individual (Quan et al., 2018).
Therefore, the present study aims to observe the effect that improving sleep hygiene in a sample of young adults (18-25 years old) living in Spain may have on the prosocial and antisocial tendencies of the subjects. It is expected (hypothesis 1) an improvement in sleep quality in those who underwent the intervention on sleep hygiene measures, and (hypothesis 2) it is expected that those participants who show more adherence to the recommendations on sleep hygiene will present an increase in the score on prosocial measures, as well as a reduction in measures related to antisocial behaviour (hypothesis 3a), especially reactive aggression (hypothesis 3b), while participants in the different groups will not show significant differences before the intervention on sleep hygiene measures (hypothesis 4). Finally, a greater impairment of sleep quality is expected in those participants with a higher use of digital screens in the hours before bedtime (hypothesis 5).
Method
Participants
This research was carried out through a secure online platform, and participants accessed it through the presentation of the study to various classrooms at the Universitat de València, banners published on social networks (Facebook and Instagram) and/or through advertising posters. The inclusion criteria for accessing the survey were: (1) being older than 18 and younger than 25 years old and (2) being resident in Spain. Participants did not receive any compensation for their participation.
A total of 484 participants accessed the survey. The initial data derived from the online platform were filtered (screening I) to avoid duplicate, inconsistent and/or unreliable responses (e.g. participants claiming to be older than allowed). Only participants who completed both measurement phases of the survey were included (screening II). The final sample consisted of 121 participants (83.5 % female) aged 18-25 years (M = 20.21, SD = 1.67). All participants initially completed a battery of measures that included different ad hoc scales and standardised self-report measures. Table 1 lists the characteristics of the participants.
| % (n) | |
| Demographics | |
| Gender | |
| Man | 15.7 (19) |
| Woman | 83.5 (101) |
| Age (range: 18 to 25 years) M (SD) | 20.21 (1.78) |
| Civil status | |
| Single | 58.7 (71) |
| In a relationship (not married) | 40.5 (49) |
| In a relationship (married) | 0.8 (1) |
| Education | |
| Vocational training (intermediate/higher level) | 3.3 (4) |
| High school | 3.3 (4) |
| University studies | 93.4 (113) |
| Occupation | |
| Student | 99.2 (120) |
| Active worker | 13.2 (16) |
| Unemployed | 0.8 (1) |
All data are anonymous and confidential in accordance with the European General Data Protection Regulation (GDPR 2018 - Organic Law on the Protection of Personal Data and the Guarantee of Digital Rights). A common database was generated with the answers of all participants, so the cases were not analysed individually.
Participants provided written informed consent after being presented with the purpose of the study. Participation was voluntary and anonymous, taking into consideration all ethical principles of human research as set out in the Declaration of Helsinki, under current regulations.
Instruments
Socio-demographic data: participants were asked to indicate their gender, age, place of residence, marital status, level of education and professional status.
Sleep was measured with the Spanish version of the Pittsburgh Sleep Quality Index (PSQI, Macías Fernández & Royuela Rico, 1996). Consists of 19 self-administered questions and 5 questions that are assessed by the partner or roommate (if applicable). In this way, seven component scores are obtained, ranging from 0 (absence of difficulty) to 3 (severe difficulty) points: subjective sleep quality (SSQ), sleep latency (SL), sleep duration (SD), habitual sleep efficiency (HSE), sleep disturbances (SD), use of hypnotic medication (HM) and daytime dysfunction (DD). In turn, the seven components are summed to form an overall score in a range of 0 (no difficulties) to 21 (severe difficulties) points in the various areas studied. The components assessed are subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of hypnotic medication and daytime dysfunction. In our study,
Cronbach's alpha was .62 in the first measurement and .60 in the second measurement.
Additionally, participants were asked about their habitual patterns of behaviour related to sleep quality. They had to answer on a 3-point Likert scale ranging from 1 (never/almost never) to 5 (often) about the regularity of their sleep schedule, their behaviour in the hours before sleep, such as the use of digital screens, their behaviour while in bed, substance use, and sleep disruption due to the COVID-19 situation.
Empathy was measured by the Spanish version of the Interpersonal Reactivity Index (IRI, Mestre et al., 2004). We used two dimensions of empathy: perspective taking (PT) and empathic concern (EC). The items are rated on a 5-point Likert scale, ranging from 1 (does not describe me well) to 5 (describes me very well). In our study, Cronbach's alpha was .65 (PT) and .79 (EC), on the first measurement, and .73 (PT) and .81 (EC) at the second measurement.
Emotional self-efficacy was measured by the Spanish version of the Regulatory Emotional Self-efficacy (Caprara et al, 2008). Assesses three dimensions of self-efficacy: (a) positive (POS); (b) anger; and (c) despondency/anger (ANG). Items are rated on a 5-point Likert scale, ranging from 1 (unable) to 5 (completely able). In our study, Cronbach's alpha was .88 (positive), .81 (anger) and .79 (despondency/anger) on the first measurement and .88 (positive), .81 (anger) and .79 (despondency/anger) on the second measurement.
Prosocial tendencies were measured by the Spanish version of the Prosocial Tendencies Measure (PTM-R; Mestre et al., 2015). Assesses 6 dimensions of prosocial behaviour: (a) public (PUB); (b) emotional (EMO); (c) emergency (EME); (d) altruistic (ALT); (e) anonymous (ANO); and (f) compliant or obedient (OBE). The items are rated on a 5-point Likert scale, ranging from 1 (does not describe me at all) to 5 (describes me very well). In our study, Cronbach's alpha was .67 to .78 on the first measure and .68 to .82 on the second measure.
Emotional instability was measured by the Spanish version of the Emotional Instability Scale (IE; del Barrio et al., 2001). Its 15 items are rated on a 3-point Likert scale, ranging from 1 (Never) to 3 (Often). In this study, Cronbach's alpha was .72 and .82 at first and second measurement, respectively.
Aggressive behaviour was measured by the Spanish version of the Reactive-Proactive Aggression Questionnaire (RPQ; Andreu et al., 2009). Assesses two dimensions of aggression: (a) reactive (REA); and (b) proactive (PRO). The RPQ consists of 23 questions. Items are rated on a 3-point Likert scale, ranging from 1 (Never) to 3 (Often). In this study, Cronbach's alpha was .67 (reactive) and .47 (proactive) on the first measurement and .75 (reactive) and .54 (proactive) on the second measurement.
Anger was measured by the Spanish version of the State-Trait Anger Expression Inventory-2 (STAXI-2; Tobal et al., 2009). The STAXI-2 distinguishes the different components of anger: Experience, Expression and Control, as well as its facets as a State and as a Trait. Items are rated on a 3-point Likert scale, ranging from 1 (Not at all) to 3 (Very much). In this study, Cronbach's alpha was .75 (trait) and .79 (state) on the first measurement and .79 (trait) and .88 (state) on the second measurement.
Procedure
All participants initially completed a battery of measures that included different ad hoc scales and standardised self-report measures. Once completed, participants could choose to participate in either the experimental or control group. Regardless of which group was chosen, all participants received the instructions by email.
Experimental treatment
The experimental group first received a video explaining the procedure to be followed during the following 9 days, a video training on 10 sleep hygiene measures and a summary of these indications (see Supplementary Material). The control group only received a video explaining the procedure to be followed during the following 9 days (in which case they had to maintain their usual sleep patterns).
The procedure consisted of, once the videos had been viewed (day 1), putting into practice, as far as possible, from the following day (day 2) the 10 sleep hygiene instructions. Subsequently (day 3), they had to answer a short questionnaire in which they reported on whether or not they had followed the measures, their sleep schedule, as well as an assessment of their sleep quality. The follow-up measures were to be continued for 7 days (days 2-8), as well as the follow-up questionnaire (days 3-9).
After the end of the experimental procedure (day 9), both the experimental group and the control group (both received a reminder to respond in their email) had to answer the initial questionnaire again, in measurement phase II. (Figure 1).

Figure 1.
Experimental phases
Data analysis
An experimental design is proposed with two conditions: control and treatment. Due to the characteristics of a study of this nature, where, although there is a random selection for the assignment of subjects to the experimental and control groups, those in the first group have the option of not participating in it, the selected groups cannot be considered equal; therefore, the design proposed is quasi-experimental, since absolute control cannot be obtained in the randomisation of the participants.
Although there were initially two groups, the control and the experimental, because within the experimental group participants reported unequal follow-up to the intervention, participants were divided into two groups, the low adherence group (those participants who during the experimental period had the least adherence to the sleep hygiene instructions) and the high adherence group (those participants who during the experimental period had the least adherence to the sleep hygiene instructions). The cut-off was the 50th percentile on the follow-up measures (see Figure 2).
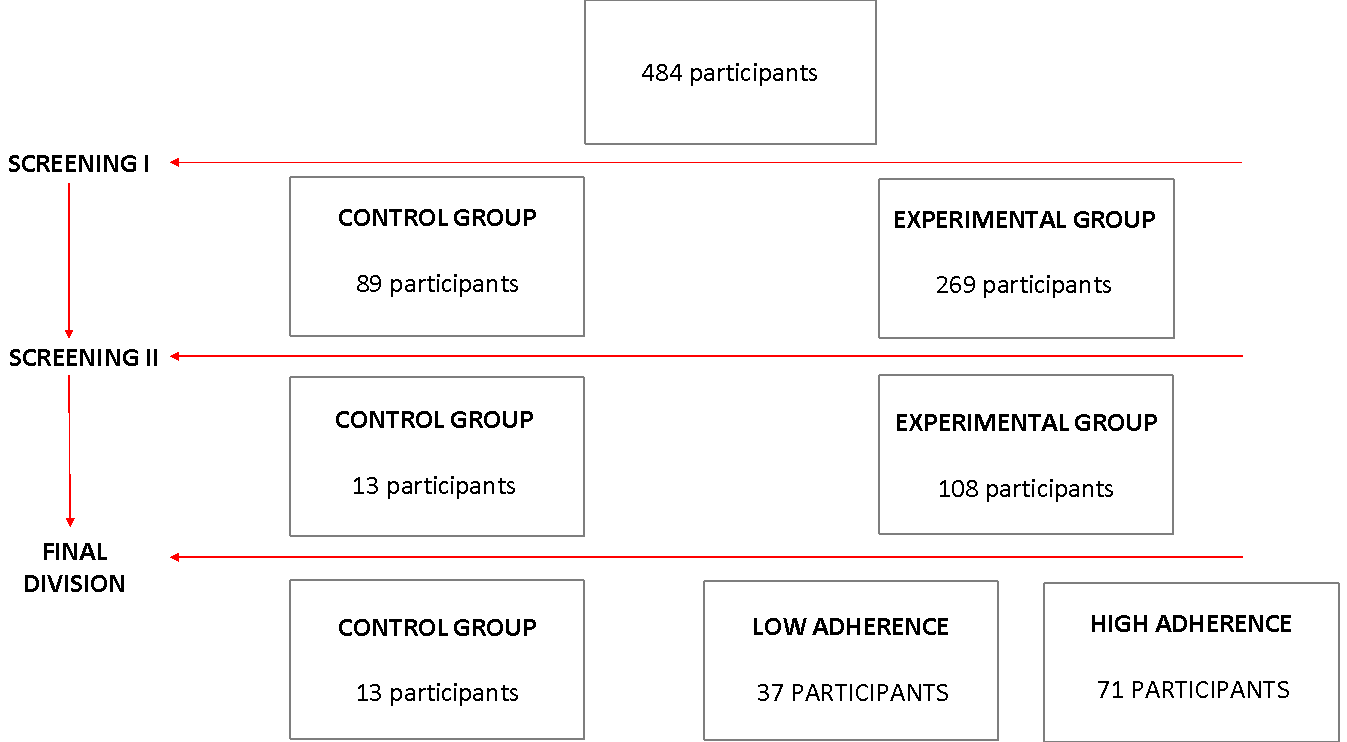
Figure 2.
Sample selection
Therefore, in order to test the hypotheses, the following analyses were carried out using the SPSS version 23 statistical package:
1) Hypothesis testing between the control and experimental groups, in the pre-test, to check for differences between the two groups before starting the application of the intervention in the experimental group. If there were differences between the groups before applying the programme, it would not be possible to ascertain whether the differences after the application of the programme are attributable to the program itself or to other reasons.
2) At the end of the programme, and once the equality between the control and experimental groups have been verified, the effectiveness of the programme will be tested. For this purpose, covariance analyses will be carried out, which allow us to check if there are differences between the control and experimental groups in the post-test, but eliminating the influence of the previous levels in the pre-test. This is important to bear in mind because it is not possible to verify the effectiveness of the programme in the same way if the levels of the variables considered are very high or very low in the pre-test. For example, if the levels of empathy and prosocial behaviour are high in the pre-test, it will be more difficult to verify the effectiveness of the programme because it will be difficult to increase even more the levels of the variables that are intended to be increased with the application of the programme.
3) Pairwise comparisons to study the differences between the control and experimental groups.
4) Bivariate correlation to test the relationship between sleep quality and digital screen use in the hours before bedtime.
Results
First, to assess the baseline in the different conditions before starting the intervention, ANOVA hypothesis testing was performed for each of the variables assessed from the instruments administered in the control group and in the experimental in the pre-test phase. The descriptive analyses (means and standard deviations) for each variable and the results of the pre-test ANOVA (Table 2) indicate that before implementing the intervention there were no significant differences between the control and experimental groups in the set of variables evaluated, which shows the high level of homogeneity between the different conditions.
| ControlN = 13 | LowN = 37 | HighN = 71 | F (2,118) | |||||
| M | SD | M | SD | M | SD | |||
| PSQI | 7.31 | 2.59 | 7.00 | 2.20 | 7.24 | 2.43 | .86 | |
| IRI | PT | 17.38 | 2.10 | 16.89 | 2.33 | 17.00 | 2.20 | .79 |
| EC | 13.38 | 1.26 | 13.68 | 1.60 | 13.38 | 1.61 | .64 | |
| SEE | POS | 15.92 | 2.40 | 16.92 | 2.79 | 16.27 | 3.00 | .07 |
| IRA | 10.31 | 3.20 | 12.32 | 3.61 | 11.03 | 3.08 | .13 | |
| ANG | 9.46 | 2.18 | 11.35 | 3.07 | 11.03 | 2.89 | ||
| IE | 1.69 | .27 | 1.69 | .36 | 1.69 | .28 | .99 | |
| STAXI I | 18.77 | 3.27 | 17.84 | 3.94 | 17.54 | 3.08 | .48 | |
| STAXI II | 11.38 | 3.84 | 10.72 | 1.49 | 10.94 | 1.80 | .60 | |
| PTM-R | PUB | 5.62 | 2.40 | 4.84 | 1.98 | 4.14 | 1.98 | .48 |
| EMO | 19.46 | 4.24 | 19.32 | 3.11 | 19.75 | 3.48 | .83 | |
| EME | 10.54 | 2.67 | 10.89 | 2.58 | 11.18 | 2.06 | .59 | |
| ANO | 11.46 | 2.22 | 9.54 | 3.50 | 10.82 | 3.69 | .12 | |
| ALT | 16.69 | 3.55 | 17.57 | 2.30 | 17.65 | 2.36 | .44 | |
| OBE | 5.62 | 2.40 | 4.84 | 1.98 | 5.14 | 1.98 | .48 | |
| RPQ | REA | 12.00 | 2.48 | 10.97 | 2.08 | 11.45 | 1.84 | .24 |
| PRO | 7.23 | 1.30 | 6.68 | .94 | 6.54 | .91 | .06 | |
*p < .05; **p < .01; ***p < .001
Secondly, to evaluate the effectiveness of the programme, analysis of covariance was carried out to observe the differences between the control and experimental groups in the post-test, but eliminating the influence of the previous levels in the pre-test. The results of the pretest-posttest ANCOVA (Table 3) confirm statistically significant differences in the pretest-posttest change between experimental and control groups, specifically a significant increase in the mean sleep scores of the different groups [F(3,117) = 9.75, p < .001], emotional instability [F(3,177) = 4.04, p < .05], state anger [F(3,117) = 4.13, p < .05], public prosocial tendencies [F(3,117) = 3.12, p = .05], anonymous prosocial tendencies [F(3,177) = 3.05, p = .05] and reactive aggression [F(3,117) = 21.32, p ≤ .001]. Effect sizes were large for sleep and reactive aggression, and medium for emotional instability and anger state.
| Pre-test | ControlN = 13 | LowN = 37 | HighN = 71 | F (1,117) | |||||
| M | SD | M | SD | M | SD | F | Sig. | n2p | |
| PSQI | 7.31 | 1.98 | 9.53 | 2.23 | 9.89 | 2.41 | 9.75 | .00*** | .31 |
| IRI PT | 16.93 | 2.04 | 17.56 | 2.34 | 17.10 | 2.29 | .85 | .43 | .01 |
| IRI EC | 13.56 | 1.26 | 13.73 | 1.48 | 13.98 | 1.82 | .54 | .58 | .01 |
| SEE POS | 16.01 | 2.76 | 16.11 | 3.13 | 16.49 | 2.88 | .69 | .50 | .01 |
| SEE IRA | 12.49 | 2.95 | 12.16 | 3.05 | 11.90 | 3.17 | .50 | .61 | .01 |
| SEE ANG | 11.74 | 1.50 | 11.54 | 2.90 | 11.20 | 3.00 | .71 | .50 | .01 |
| IE | 1.70 | .24 | 1.71 | .35 | 1.60 | .35 | 4.04 | .02* | .06 |
| STAXI I | 16.55 | 3.31 | 17.39 | 3.67 | 17.21 | 3.71 | .66 | .52 | .01 |
| STAXI II | 12.45 | 5.03 | 10.82 | 1.74 | 10.60 | 1.34 | 4.13 | .02* | .07 |
| PTM-R PUB | 5.55 | 2.99 | 5.54 | 2.38 | 4.73 | 2.07 | 3.12 | .05* | .05 |
| PTM-R EMO | 18.78 | 4.05 | 18.92 | 4.05 | 19.26 | 3.40 | .31 | .73 | .01 |
| PTM-R EME | 10.91 | 2.33 | 10.65 | 2.41 | 10.07 | 2.26 | .64 | .53 | .01 |
| PTM-R ANO | 12.16 | 2.67 | 10.20 | 3.21 | 10.18 | 4.04 | 3.05 | .05* | .05 |
| PTM-R ALT | 17.30 | 3.71 | 17.78 | 2.15 | 17.85 | 2.34 | .63 | .53 | .01 |
| PTM-R OBE | 10.39 | 2.67 | 10.97 | 2.58 | 11.17 | 2.06 | .69 | .50 | .01 |
| RPQ REA | 13.15 | 2.91 | 9.73 | 2.03 | 9.19 | 1.76 | 21.32 | .00*** | .27 |
| RPQ PRO | 6.51 | 1.04 | 6.55 | .76 | 6.73 | 1.14 | .41 | .02 | |
*p < .05; **p < .01; ***p < .001
Third, to study the differences between the control (Mc), low (Mb) and high (Ma) experimental groups, pairwise comparisons were made (Table 4). For sleep, statistically significant differences were observed between the control and low experimental group (Mc = 7.31, Mb = 9.53) and the control and high experimental group (Mc = 7.31, Ma = 9.89). For emotional instability, statistically significant differences were observed between the low experimental and high experimental groups (Mb = 1.71, Ma = 1.60). For state anger, statistically significant differences are observed between the control and low experimental group (Mc = 16.55, Mb = 17.39) and the control and high experimental group (Mc = 16.35, Ma = 17.2). For public prosocial tendencies, statistically significant differences were observed between the low experimental and high experimental groups (Mb = 5.54, Ma = 4.73). For anonymous prosocial tendencies, statistically significant differences are observed between the control and high experimental group (Mc = 5.03, Ma = 4.73). For reactive aggression, statistically significant differences were observed between the control and low experimental group (Mc = 13.15, Mb = 9.73) and the control and high experimental group (Mc = 12.15, Ma = 9.19).
| Post-test | Control | Low | High | |
| PSQI | Control | - | .00*** | .00** |
| Low | .00*** | - | 1 | |
| High | ||||
| IE | ControlLowHigh | - | .07 | .06 |
| .07 | - | .04* | ||
| .06 | .04* | - | ||
| STAXI II | ControlLowHigh | - | .02* | .01** |
| .02* | - | .62 | ||
| .01** | .62 | - | ||
| PTM-R PUB | ControlLowHigh | - | .98 | .12 |
| .98 | - | .03* | ||
| .12 | - | |||
| PTM-R ANO | Control | - | .08 | .05* |
| Low | .08 | - | 1 | |
| High | .05* | 1 | - | |
| RPQ REA | ControlLowHigh | - | .00*** | .00*** |
| .00*** | - | .192 | ||
| .00*** | .192 | - | ||
Finally, to observe the relationship between sleep quality and the use of digital screens before sleep, bivariate correlation analyses were performed between the PSQI, as well as the different subscales of the PSQI, and the use of digital screens in the hours before bedtime (Table 5).
| Screen | M (SD) | r |
| PSQI | 9.50 (2.42) | .004 |
| CSS | 1.21 (1.02) | .131 |
| LS | 1.13 (.50) | .270** |
| DS | 1.17 (.91) | .232* |
| ESH | 2.95 (.31) | -.076 |
| PS | .30 (.56) | .155 |
| HM | 2.02 (.58) | -.129 |
| DD | .23 (.65) | .055 |
It is observed that greater use of digital screens in the hours before bedtime is statistically significantly related to greater sleep disturbance (r = .270) and sleep dysfunction (r = .230).
Discussion
The study aimed to assess the effects of a sleep hygiene improvement programme on prosocial and antisocial tendencies. Specifically, an improvement in sleep quality was expected in those who underwent the intervention on sleep hygiene measures (hypothesis 1), and, on the other hand, it was expected that those participants who showed more adherence to the sleep hygiene recommendations would show an increase in scores on prosocial measures (hypothesis 2), as well as a reduction in measures related to antisocial behaviour (hypothesis 3a), especially reactive aggression (hypothesis 3b), while before the implementation of the sleep hygiene measures the control and experimental groups would show no significant differences (hypothesis 4). Finally, a greater impairment of sleep quality was expected in those participants with a higher use of digital screens in the hours before bedtime (hypothesis 5).
Firstly, the results showed that the programme significantly boosted sleep quality. Between the pre-test and the post-test, sleep quality increased in participants who underwent the intervention programme, with the effect being greater in participants with greater adherence. Therefore, hypothesis 1 has been confirmed, ratifying the results of other works, where informative sleep hygiene interventions promote an improvement in sleep quality (Hershner & O'Brien, 2018; O'Donnell & Driller, 2017; Zengin & Aylaz, 2019).
Secondly, and with respect to hypothesis 2, it can be observed that it is partially corroborated. The results showed that the programme significantly enhanced an improvement in certain prosocial variables. Specifically, between the pre-test and the post-test, those with greater adherence to the programme showed a reduction in public prosocial behaviour, that which is carried out with the aim of obtaining the approval of others (Carlo et al., 2003). In contrast, the other prosocial measures (empathy, emotional self-efficacy and prosocial tendencies) showed no variation between pre-test and post-test measures. One possible explanation is that prosocial behaviour depends on other variables in the family context (parenting styles), personal variables (empathy, self-control), school context (victimisation, peer group attachment and school performance), personality and other secondary socialising agents (television, video games, internet), which, in turn, are interrelated (Sarrionandia & Garaigordobil, 2014). In this equation that determines the final expression of prosocial behaviours, as already seen, sleep has some weight (Anderson & Dickinson, 2010; Dickinson & McElroy, 2017; Rilling & Sanfey, 2011), but for its effect to be manifested, a more extensive intervention may be necessary, allowing for long-term change, since prosocial behaviour is a very complex variable in development from childhood to adulthood, and producing significant change with a short-term informational intervention may have been insufficient.
Thirdly, in relation to hypothesis 3a, the results confirmed that the programme significantly reduced certain variables related to antisocial behaviour. Specifically, between the pre-test and the post-test, those with greater adherence to the programme showed a reduction in emotional instability. This is consistent with those studies that claim a relationship between sleep and emotional instability (Bardwell et al., 1999; Barker et al., 2016; Elger, 2003; Flemons & Tsai, 1997). However, there is little research on this relationship in a healthy young population, as well as on the possible effects of an intervention on the relationship between both variables, so our results provide new evidence that an improvement in sleep hygiene in a young population can lead to a reduction in emotional instability.
In turn, those participants who underwent the intervention programme, regardless of the degree of adherence, showed a reduction in state anger, a change that was not evident in trait anger. This is consistent with classic research linking the role of anger in aggressive behaviour (Cutler & Cohen, 1979; Roth & Lutz, 1976; Schubert, 1977) and with more recent research (Ireland & Culpin, 2006) claiming that sleep plays an important role in aggression. A significant reduction in reactive aggression has also been observed in participants who underwent the intervention programme, which was not evident in proactive aggression, being consistent with research in this regard (Kempes et al., 2005; Orobio de Castro et al., 2005), confirming hypothesis 3b. Therefore, although there is little research on the dynamics between sleep and aggression (Barker et al., 2016), the results have shown that improved sleep hygiene reduces emotional instability, anger state and reactive aggression, confirming hypothesis 3a in most variables related to antisocial behaviour.
Fourthly, those participants who have not undergone the intervention on hygiene measures have not shown statistically significant differences in any of the measures, thus corroborating hypothesis 4. In this way, it has been confirmed that the changes produced in the different prosocial variables and the variables related to antisocial behaviour have occurred only in those participants who have undergone the intervention programme.
Finally, a higher number of sleep disturbances and sleep dysfunctions were observed in those participants who used digital screens more before sleep, thus corroborating hypothesis 5. This is in line with the various studies that point to a delay in the onset of sleep, as well as a poorer quality of sleep due to the use of ICTs in the moments before sleep (Bruce et al., 2017; Lemola et al., 2015; Pertegal-Vega et al., 2019).
Our findings imply that an improvement in sleep hygiene over a short period of time has the effect of significantly reducing certain variables related to antisocial behaviour, such as reactive aggression, anger state and emotional instability. So, given the active role these variables play in the social behaviour of subjects, being predictors of poorer social adjustment, isolation and low social status among others (Chaux, 2003), interventions that allow for an increase in sleep hygiene could have a positive impact on social interaction, with special emphasis on prevention measures that educate in the correct use of ICTs. All of this, together with other benefits derived from optimal sleep quality, given its central role in the regulation of multiple psychological and biological processes, which has already been addressed previously (Chee & Chuah, 2008; Dattilo et al., 2011).
The study has some limitations. Firstly, the use of self-reports, with the social desirability biases they imply, suggesting that for future studies it would be relevant to replicate the research using observational methodology, such as EEG measures of sleep, or assessment instruments completed by impartial observers close to the participants that could be contrasted with the information provided by the participants themselves.
Secondly, the composition of the sample itself. The sample was mostly composed of women, which can be explained by the fact that the majority of the recruited population belongs to students of the Psychology Degree, which in turn is mostly composed of women. Another limitation is that there has been a large loss of the initial sample, which can be explained by the temporal extension of the experiment. Participants chose to participate in either the control group or the experimental group, so the sample was not randomised. Therefore, it would be interesting to replicate the intervention programme by increasing the size of the sample, randomly assigning the subjects to the different experimental groups, and increasing the representativeness of the population, as well as applying measures to encourage adherence to the experiment, especially in those participants assigned to the control group.
Finally, the health situation in which the participants live serves as a limitation of the study, given the potential emotional and physical effects it may have exerted on them, which we have not been able to control.
Funding: This study did not receive specific funding from public sector agencies, the commercial sector, or non-profit bodies.
References
Anderson, C., & Dickinson, D. L. (2010). Bargaining and trust: The effects of 36-h total sleep deprivation on socially interactive decisions. Journal of Sleep Research, 19(1 PART. 1), 54–63. https://doi.org/10.1111/j.1365-2869.2009.00767.x
Andreu, J. M., Fernández, M. E. P., & Ramírez, J. M. (2009). Cuestionario de agresión reactiva y proactiva: un instrumento de medida de la agresión en adolescentes. Revista de Psicopatología y Psicología Clínica, 14(1), 37–49. https://doi.org/10.5944/rppc.vol.14.num.1.2009.4065
Arsenio, W. F., Adams, E., & Gold, J. (2009). Social information processing, moral reasoning, and emotion attributions: Relations with adolescents reactive and proactive aggression. Child Development, 80(6), 1739-1755. https://doi.org/10.1111/j.1467-8624.2009.01365.x
Balabanian, C., & Lemos, V. (2020). El rol de la atribución en el comportamiento prosocial adolescente. Interdisciplinaria, Revista de Psicología y Ciencias Afines, 37(2), 129-142. http://doi.org/10.16888/interd.2020.37.2.8
Bardwell, W., Berry, C., Ancoli-Israel, S., & Dimsdale, J. (1999). Psychological correlates of sleep apnea. Journal of Psychosomatic Research, 47(6), 583–596. https://doi.org/10.1016/s0022-3999(99)00062-8
Barker, L. F., Ireland, J. L., Chu, S., & Ireland, C. A. (2016). Sleep and its association with aggression among prisoners: Quantity or quality? International Journal of Law and Psychiatry, 47, 115–121. https://doi.org/10.1016/j.ijlp.2016.02.014
Benenson, J. F., Pascoe, J., & Radmore, N. (2007). Children’s altruistic behavior in the dictator game. Evolution and Human Behavior, 28(3), 168–175. https://doi.org/10.1016/j.evolhumbehav.2006.10.003
Bruce, E. S., Lunt, L., & McDonagh, J. E. (2017). Sleep in adolescents and young adults. Clinical Medicine, 17(5), 424–428. https://doi.org/10.7861/clinmedicine.17-5-424
Caprara, G. V., Di Giunta, L., Eisenberg, N., Gerbino, M., Pastorelli, C., & Tramontano, C. (2008). Assessing regulatory emotional self-efficacy in three countries. Psychological Assessment, 20(3), 227–237. http://doi.org/10.1037/1040-3590.20.3.227
Carlo, G., Hausmann, A., Christiansen, S., & Randall, B. A. (2003). Sociocognitive and behavioral correlates of a measure of prosocial tendencies for adolescents. The Journal of Early Adolescence, 23(1), 107-134. https://doi.org/10.1177/0272431602239132
Carlo, G., Mestre, M. V., McGinley, M. M., Tur-Porcar, A., Samper, P., & Opal, D. (2014). The protective role of prosocial behaviors on antisocial behaviors: The mediating effects of deviant peer affiliation. Journal of Adolescence, 37(4), 359-366. http://doi.org/10.1016/j.adolescence.2014.02.009
Carskadon, M. A., Vieira, C., & Acebo, C. (1993). Association between puberty and delayed phase preference. Sleep, 16(3), 258-262. https://doi.org/10.1093/sleep/16.3.258
Chaux, E. (2003). Agresión reactiva, agresión instrumental y el ciclo de la violencia. Revista de Estudios Sociales, 15, 47-58. https://doi.org/10.7440/res15.2003.03
Chee, M. W. L., & Chuah, L. Y. M. (2008). Functional neuroimaging insights into how sleep and sleep deprivation affect memory and cognition. Current Opinion in Neurology, 21(4), 417–423. https://doi.org/10.1097/WCO.0b013e3283052cf7.
Cizza, G., Requena, M., Galli, G., & De Jonge, L. (2011). Chronic sleep deprivation and seasonality: Implications for the obesity epidemic. Journal of Endocrinological Investigation, 34(10), 793–800. https://doi.org/10.3275/7808
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences. Second Edition. LEA.
Crick, N. R., & Dodge, K. A. (1996). Social Information-Processing Mechanisms in Reactive and Proactive Aggression. Child Development, 67(3), 993–1002.
Cutler, N. R., & Cohen, H. B. (1979). The effect of one night's sleep loss on mood and memory in normal subjects. Comprehensive Psychiatry, 20(1), 61–66. https://doi.org/10.1016/0010-440X(79)90060-9
Dahl, R. E., & Lewin, D. S. (2002). Pathways to adolescent health sleep regulation and behavior. Journal of Adolescent Health, 31(6), 175-184. https://doi.org/10.1016/S1054-139X(02)00506-2
Dattilo, M., Antunes, H. K. M., Medeiros, A., Mônico Neto, M., Souza, H. S., Tufik, S., & De Mello, M. T. (2011). Sleep and muscle recovery: Endocrinological and molecular basis for a new and promising hypothesis. Medical Hypotheses, 77(2), 220–222. https://doi.org/10.1016/j.mehy.2011.04.017
Del Barrio, V., Moreno, C., & López, R. (2001). Evaluación de la agresión y la inestabilidad emocional en niños españoles: Su relación con la depresión. Clínica y Salud, 12(1), 33-50.
Dickinson, D. L., & McElroy, T. (2017). Sleep restriction and circadian effects on social decisions. European Economic Review, 97, 57-71. https://doi.org/10.1016/j.euroecorev.2017.05.002
Dietrich, S. K., Francis-Jimenez, C. M., Knibbs, M. D., Umali, I. L., & Truglio-Londrigan, M. (2016). Effectiveness of sleep education programs to improve sleep hygiene and/or sleep quality in college students: a systematic review. JBI Evidence Synthesis, 14(9), 108-134. https://doi.org/10.11124/JBISRIR-2016-003088
Eisenberg, N., Fabes, R. A., & Spinrad, T. L. (2006). Prosocial development. Handbook of Child Psychology, 3, 646–718. https://doi.org/10.1002/9780470147658.chpsy0311
Eisenberg, N., Guthrie, I. K., Cumberland, A., Murphy, B. C., Shepard, S. A., Zhou, Q., & Carlo, G. (2002). Prosocial development in early adulthood: A longitudinal study. Journal of Personality and Social Psychology, 82(6), 993–1006. https://doi.org/10.1037/0022-3514.82.6.993
Elger, B. (2003). Does insomnia in prison improve with time? Prospective study among remanded prisoners using the Pittsburgh Sleep Quality Index. Medicine, Science and the Law, 43(4), 334–344. https://doi.org/10.1258/rsmmsl.43.4.334
Espie, C. A., Kyle, S. D., Hames, P., Cyhlarova, E., & Benzeval, M. (2012). The daytime impact of DSM-5 insomnia disorder: Comparative analysis of insomnia subtypes from the Great British Sleep Survey. Journal of Clinical Psychiatry, 73(12), 1478–1484. https://doi.org/10.4088/JCP.12m07954
Flemons W., & Tsai, W. (1997). Quality of life consequences of sleep-disordered breathing. Journal of Allergy and Clinical Immunology, 99(2), 750–756. https://doi.org/10.1016/s0091-6749(97)70123-4
García-Padilla, A. K. (2017). Análisis Psicométrico del Staxi-2 Y Ml-Staxi en Adultos del Área Metropolitana de Bucaramanga. Cuadernos Hispanoamericanos de Psicología, 16(2), 33–44. https://doi.org/10.18270/chps..v16i2.1972
Hershner, S., & O’Brien, L. M. (2018). Sleep Education for College Students. Journal of Clinical Sleep Medicine, 14(7), 1271–1272. https://doi.org/10.5664/jcsm.7248
Ireland, J. L., & Culpin, V. (2006). The relationship between sleeping problems and aggression, anger, and impulsivity in a population of juvenile and young offenders. Journal of Adolescent Health, 38(6), 649-655. https://doi.org/10.1016/j.jadohealth.2005.05.027
Jenni, O. G., Achermann, P., & Carskadon, M. A. (2005). Homeostatic sleep regulation in adolescents. Sleep, 28(11), 1446-1454. https://doi.org/10.1093/sleep/28.11.1446
Kempes, M., Matthys, W., De Vries, H., & Van Engeland, H. (2005). Reactive and proactive aggression in children A review of theory, findings and the relevance for child and adolescent psychiatry. European Child & Adolescent Psychiatry, 14(1), 11-19. https://doi.org/10.1007/s00787-005-0432-4
Lao, X. Q., Liu, X., Deng, H. B., Chan, T. C., Ho, K. F., Wang, F., … Yeoh, E. K. (2018). Sleep quality, sleep duration, and the risk of coronary heart disease: A prospective cohort study with 60,586 adults. Journal of Clinical Sleep Medicine, 14(1), 109–117. https://doi.org/10.5664/jcsm.6894
Lemola, S., Perkinson-Gloor, N., Brand, S., Dewald-Kaufmann, J. F., & Grob, A. (2015). Adolescents’ electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age. Journal of Youth and Adolescence, 44(2), 405–418. https://doi.org/10.1007/s10964-014-0176-x
Liu, H., & Chen, A. (2019). Roles of sleep deprivation in cardiovascular dysfunctions. Life Sciences, 219(253), 231–237. https://doi.org/10.1016/j.lfs.2019.01.006
Lupano Perugini, M. L., & Castro Solano, A. (2021). Rasgos de personalidad, bienestar y malestar psicológico en usuarios de redes sociales que presentan conductas disruptivas online. Interdisciplinaria, Revista de Psicología y Ciencias Afines, 38(2), 7-23. https://doi.org/10.16888/interd.2021.38.2.1
Macías Fernández, J. A., & Royuela Rico, A. (1996). La versión española del Índice de Calidad de Sueño de Pittsburgh. Informaciones Psiquiátricas, 146, 465–472.
Mestre, V., Carlo, G., Samper, P., Tur-Porcar, A. M., & Llorca, A. (2015) Psychometric Evidence of a Multidimensional Measure of Prosocial Behaviors for Spanish Adolescents. The Journal of Genetic Psychology, 176(4), 260-271. https://doi.org/10.1080/00221325.2015.1052726
Mestre, V., Frías, M. D., & Samper, P. (2004). La medida de la empatía: análisis del Interpersonal Reactivity Index. Psicothema, 23(4), 824–831.
O’Donnell, S., & Driller, M. W. (2017). Sleep-hygiene Education improves Sleep Indices in Elite Female Athletes. International Journal of Exercise Science, 10(4), 522–530.
Orobio de Castro, B., Merk, W., Koops, W., Veerman, J. W., & Bosch, J. D. (2005). Emotions in social information processing and their relations with reactive and proactive aggression in referred aggressive boys. Journal of Clinical Child and Adolescent Psychology, 34(1), 105-116. https://doi.org/10.1207/s15374424jccp3401_10
Ortiz, M. A. C., Egido, B. D., García, M. I. B., Tello, F. P. H., & del Barrio Gándara, M. V. (2011). Propiedades psicométricas del interpersonal reactivity index (IRI) en población infantil y adolescente española. Psicothema, 23(4), 824–831.
Owens, J., Adolescent Sleep Working Group, Committee on Adolescence, Au, R., Carskadon, M., Millman, R., ... & O’Brien, R. F. (2014). Insufficient sleep in adolescents and young adults: an update on causes and consequences. Pediatrics, 134(3), e921-e932. https://doi.org/10.1542/peds.2014-1696
Pereyra Girardi, C. I., Páez Vargas, N., Ronchieri Pardo, C. del V., & Trueba, D. A. (2019). Validación de la Escala de Autoeficacia para el Afrontamiento del Estrés en estudiantes universitarios. Revista de Psicología, 37(2), 473–493. https://doi.org/10.18800/psico.201902.005
Pertegal Vega, M., Oliva Delgado, A., & Rodríguez Meirinhos, A. (2019). Revisión sistemática del panorama de la investigación sobre redes sociales: taxonomía sobre experiencias de uso. Comunicar: Revista Científica Iberoamericana de Comunicación y Educación, 60, 81–91. https://doi.org/10.3916/C60-2019-08
Quan, S. F., Ziporyn, P. S., & Czeisler, C. A. (2018). Sleep Education for College Students: The Time Is Now. Journal of Clinical Sleep Medicine, 14(7), 1269. https://doi.org/10.5664/jcsm.7246
Rappoport, A. (2019). A Complete Biological Theory of Sleep. (April), 1–31. https://doi.org/10.20944/preprints201904.0325.v1
Rilling, J. K., & Sanfey, A. G. (2011). The neuroscience of social decision-making. Annual Review of Psychology, 62, 23–48. https://doi.org/10.1146/annurev.psych.121208.131647
Román, D., Santibáñez, P., & Vinet, E.V. (2016). Uso de las Escalas de Depresión Ansiedad Estrés (DASS-21) como Instrumento de Tamizaje en Jóvenes con Problemas Clínicos. Acta de Investigación Psicológica, 6(1), 2325-2336. https://doi.org/10.1016/S2007-4719(16)30053-9
Romera Félix, E. M., Camacho, A., Ortega Ruiz, R., & Falla Fernández, D. (2021). Cibercotilleo, ciberagresión, uso problemático de Internet y comunicación con la familia. Comunicar: Revista Científica de Comunicación y Educación, 29(67), 61–71. https://doi.org/10.3916/C67-2021-05
Roth, T., Kramer, M., & Lutz, T. (1976). The effects of sleep deprivation on mood. Psychiatric Journal of the University of Ottawa, 1(3), 136–139.
Sarrionandia, A., & Garaigordobil, M. (2017). Efectos de un programa de inteligencia emocional en factores socioemocionales y síntomas psicosomáticos. Revista Latinoamericana de Psicología, 49(2), 110-118. https://doi.org/10.1016/j.rlp.2015.12.001
Soehner, A. M., & Harvey, A. G. (2012). Prevalence and functional consequences of severe insomnia symptoms in mood and anxiety disorders: Results from a nationally representative sample. Sleep, 35(10), 1367–1375. https://doi.org/10.5665/sleep.2116
Schubert, F.C. (1977). Personality traits and polygraphic sleep parameters: Correlations between personality factors and polygraphically recorded sleep in healthy subjects. Waking & Sleeping, 1(2), 165–170.
Solomon, N. L., & Zeitzer, J. M. (2019). The impact of chronotype on prosocial behavior. Plos One, 14(4), 1–11. https://doi.org/10.1371/journal.pone.0216309
Taylor, D. J., Jenni, O. G., Acebo, C., & Carskadon, M. A. (2005). Sleep tendency during extended wakefulness: insights into adolescent sleep regulation and behavior. Journal of Sleep Research, 14(3), 239-244. https://doi.org/10.1111/j.1365-2869.2005.00467.x
Tobal, J. J., Casado, M. I., Cano Vindel, A., & Spielberg, C. D. (2009). STAXI-2 Manual. Journal of Chemical Information and Modeling, 53(9), 1689–1699.
Tur-Porcar, A., Llorca, A., Malonda, E., Samper, P., & Mestre, M. V. (2016). Empathy in adolescence. Relations with prosocial moral reasoning, prosocial behavior and aggression. Acción Psicológica, 13(2), 3. https://doi.org/10.5944/ap.13.2.17802
Vgontzas, A. N., Liao, D., Pejovic, S., Calhoun, S., Karataraki, M., & Bixler, E. O. (2009). Insomnia with objective short sleep duration is associated with type 2 diabetes: A population-based study. Diabetes Care, 32(11), 1980–1985. https://doi.org/10.2337/dc09-0284
Walker, M. (2017). Why we sleep: The new science of sleep and dreams. Penguin Books.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Erlbaum.
Zengin, L., & Aylaz, R. (2019). The effects of sleep hygiene education and reflexology on sleep quality and fatigue in patients receiving chemotherapy. European Journal of Cancer Care, 28(3), 1–11. https://doi.org/10.1111/ecc.13020
Información adicional
redalyc-journal-id: 180