Abstract:
Subjective memory complaints (SMC) refer to verbalizations of memory decline perception. They can be a sign of a correct perception of decline or reflect the prelude to mild cognitive impairment and dementia. Due to the perception of memory deficit, older adults, often implement memory compensation strategies (MCS) to maximize performance in daily life. Quantitative, observational, cross-sectional design. The sample consisted in 121 non-institutionalized older adults between 60 and 92 (M = 71.7; SD = 7.8), from Buenos Aires city (63.6 % women). A weak negative correlation was observed between SMC and semantic fluency. There was a negative weak correlation between the educational level and the Success factor, indicative that more educated elderly perceived less necessity or motivation to compensate memory deficits. As for gender, women used more Internal Time, Effort and Change strategies. The elderly´s score in the SMCQ was correlated with various compensation strategies, founding that the greater the SMC, the more Time, Effort, Reliance and Change strategies were used. Older adults who perceived more SMC use different compensation strategies than those with low SMC. Our findings are consistent with previous studies that affirm that, as older adults perceive deficits in their memory, they need more aids and, therefore, set forth compensatory mechanisms that allow them to adapt better to daily life. These strategies can be taught and trained.
Keywords: older adults, memory, memory forgetting, strategies, cognitive aging.
Resumen:
El deterioro cognitivo y su percepción son un aspecto fundamental en la población de adultos mayores, ya que la memoria y otras funciones cognitivas tienden a disminuir. La queja subjetiva de memoria (QSM) refiere a las verbalizaciones de la percepción del deterioro de la memoria que pueden expresarse en olvidos constantes. Estas pueden ser signo de una percepción correcta del declive o reflejar el preludio de un posterior deterioro cognitivo leve o una demencia. Debido a la apreciación del déficit de memoria, los adultos mayores, a menudo implementan estrategias de compensación de la memoria (ECM) para maximizar el rendimiento en la vida diaria. Estas se suelen categorizar por estrategias de remediación (subescala Tiempo y Esfuerzo), de substitución (Externas, Internas y Confianza), y complementarias (Éxito y Cambio). Aunque las quejas subjetivas de memoria son comunes entre los adultos mayores sanos, aún no se ha determinado si utilizan las mismas estrategias de compensación que los adultos mayores con una alta queja subjetiva de memoria. Por tanto, el objetivo de este estudio es comparar las estrategias de compensación de memoria implementadas por personas mayores sanas, con y sin quejas de memoria. El presente trabajo tuvo un diseño cuantitativo, observacional y transversal. La muestra consistió en 121 adultos mayores sanos no institucionalizados de entre 60 y 92 años (M = 71.7; DE = 7.8), de la Ciudad Autónoma de Buenos Aires (63.6 % mujeres). Todos los participantes presentaron puntuaciones en el screening cognitivo acordes a una trayectoria de envejecimiento saludable. No se encontró relación entre las quejas subjetivas de memoria y las variables sociodemográficas (edad, sexo y nivel educativo). Se observó una correlación negativa débil entre la QSM y la prueba de fluidez semántica. Por otro lado, hubo una correlación negativa débil entre el nivel educativo y el factor de éxito, lo que indica que los adultos mayores más educados perciben menos necesidad o motivación para compensar los déficits de memoria. En cuanto al género, las mujeres utilizaron más las estrategias de tiempo [t (118) = 1.66; p = .03], interno [t (117) = 1.93; p = .05], esfuerzo [t (117) = 1.94; p = .05] y cambio [t (116) = 3.22; p = .002] en comparación con los hombres. La puntuación total de los adultos mayores en la escala de QSM se correlacionó con diversas estrategias de compensación, y se constató que, cuanto mayor es la QSM, mayor es el uso de las siguiente estrategias: tiempo (r = .22, p = .01), esfuerzo (r = .37; p < .001), confianza (r = .36; p < .001) y cambio (r = .26; p = .004). Al comparar al grupo de alta queja subjetiva de memoria con el grupo de baja queja, se encontraron diferencias significativas (p < .000) en los tipos de olvidos reportados. En conclusión, los adultos mayores que perciben más problemas de quejas de memoria utilizan diferentes estrategias de compensación que aquellos con baja queja de memoria. Estos hallazgos son consistentes con estudios anteriores que afirman que, a medida que los adultos mayores perciben déficits en su memoria, necesitan más ayudas y, por tanto, ponen en marcha mecanismos compensatorios que les permiten adaptarse mejor a la vida cotidiana. Estas estrategias se pueden enseñar y entrenar. En el futuro, será importante aumentar el número de hombres al momento de investigar estas variables, además de profundizar en qué medida los aspectos psicológicos (como podrían ser la depresión, las estrategias de afrontamiento, la ansiedad) están relacionados con la presencia de QSM y el uso de estrategias de compensación de memoria.
Palabras clave: adulto mayor, memoria, pérdida de memoria, estrategias de compensación, envejecimiento cognitivo.
Artículos
Subjective memory complaints and compensation strategies in healthy older adults
Quejas subjetivas de memoria y estrategias de compensación en adultos mayores sanos
Centro Interamericano de Investigaciones Psicológicas y Ciencias Afines

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-CompartirIgual 4.0 Internacional.
Recepción: 21 Junio 2022
Aprobación: 16 Mayo 2023
Cognitive changes and its perception are a fundamental aspect in the elderly, as memory and other cognitive functions tend to decline. These changes are heterogeneous among older adults and may vary due to genetic and environmental factors, as well as being manifested as complaints that may represent better or worse cognitive performance (Maroof et al., 2016). Aging trajectories are heterogeneous in this population, and the boundary between the normal cognitive impairment expected for age, and the cognitive impairment that could imply the existence of a disease, is not yet clear or defined (Borrás Blasco & Viña Ribes, 2016). Ageing is not necessarily an equivalent to pathological cognitive impairment but continues to be one of the most relevant non-modifiable risk factors in the onset of neurodegenerative diseases (Aguilar Agudo et al., 2022; Paredes Arturo et al., 2021). The normal ageing process brings with it certain mild cognitive changes (such as occasional forgetfulness), so evaluating performance in memory tests is a fundamental aspect for the prevention of neurodegenerative diseases (Lin et al., 2020).
In recent studies, the focus is not only on cognitive changes but also on the perception of them. Subjective cognitive decline (SCD) refers to the self-perception of a decline in some cognitive domain and the worsening of certain cognitive capacity (Jessen et al., 2014; Rabin et al., 2015). Older adults with SCD refer to increased frequency of “never” and “always” verbalizations, increased worry in various aspects of their lives, lapses, relative absence of space-time orientation, compensation and coping strategies to losses, attention fluctuation, dependency, and affective influences on memory (Ellis et al., 2015). SCD is also related to various aspects of personality and objective cognitive performance (Jessen et al., 2014).
Subjective memory complaint (SMC) refers to the verbalizations of memory decline perception which can be expressed in consistent forgetfulness (Ellis et al., 2015; Mías et al., 2015; Mías & Causse, 2021). They can occur in a variety of ways and, altogether with SCD, could be a sign of a correct perception of decline or reflect the prelude to mild cognitive impairment and dementia (Bazán et al., 2018; Lin et al., 2019; Smith & Peterson, 1997).
Within the cognitive impairment that exceeds the expected decline (due to age), can be find the Mild Cognitive Impairment (MCI) and dementia, being Alzheimer´s type dementia the most frequent. SMC is the main symptom for the diagnosis of MCI, defined as a clinical entity which is intermediate between normal aging and dementia. MCI is a known risk factor and a prodromal marker of dementia where one perceives the cognitive changes and has a low performance in certain neuropsychological tests, without a significant interference in the functionality in daily and instrumental living activities (Lin et al., 2019; Paredes, 2019; Petersen et al., 2018). Compared to Alzheimer´s dementia, where difficulties with daily skills are seriously altered, patients with MCI may begin to perceive trouble in money management, in several executive functions such as planning, managing and organizing daily tasks and recalling where some item was left (Schmitter Edgecombe & Dyck, 2014).
Even though the first symptoms of dementia are not restricted only to the memory domain, memory losses are frequently the first reason why patients ask for medical help. Both, SCD and SMC are symptomatic indicators not only at a preclinical stage of Alzheimer's disease, but also of other dementias. Some manifestation may even appear 15 years before significant impairment manifests (Rabin et al., 2015).
Due to the perception of memory deficit, older adults often use different mechanisms and implement MCS to maximize performance in daily life (Dixon et al., 2001; Frias et al., 2003). By activating the use of different compensatory aids, older adults can improve their functional activities. It is relevant to mention that patients with healthy ageing or MCI, by perceiving their cognitive decline, would activate and implement more MCS than those with dementia (who will not even, probably, recognize the need of them) (Schmitter Edgecombe & Dyck, 2014). The use of MCS is related to a slower functional decline and to a better cognitive performance (Farias et al., 2020).
These mechanisms can be evaluated by the Memory Compensation Strategies Questionnaire (MCSQ) (Dixon et al., 2001; Meléndez et al., 2013). The MCS are usually categorized into four components: remediation (using more time to perform a compensatory strategy), substitution (developing or implementing latent tools that compensate), accommodation (adjusting goals and criteria in line with one’s abilities), and assimilation (modifying the demands or requirements of the environment). In the MCSQ the remediation mechanism is represented by the Time and Effort scales (time and effort invested to mitigate losses). The External (use of notes, agendas), Internal (mnemonic strategies) and Reliance (rely on others) scales represent the substitution component. Finally, the MCSQ has two complementary subscales: Success (a person's motivation and commitment to optimally maintain the memory performance) and Change (a perception of changes in the use of compensation strategies in the last 5-10 years) (Dixon et al., 2001; Melendez et al., 2013).
Previous studies have reported that MCS may vary according to age, gender, educational level, and cognitive performance. External memory strategies increased with age, while the Internal strategies decreased (Bouazzaoui et al., 2010; Hertzog et al., 2019; Pizzonia & Suhr, 2022). Men used Reliance strategies more than women, (they primarily turned to their spouses) and less External strategies (Martin et al., 2014; Mayordomo et al., 2015; Pizzonia & Suhr, 2022). Women, as well, scored higher in Internal and Time scales, and reported an increase in the use of all MCS compared to men (Martin et al., 2014). In addition, older adults with higher educational level used the Effort strategies less.
Cognitive healthy older adults frequently use memory compensation strategies. Typically, they tend to use more often External and Time compensation strategies, while adults with Mild Cognitive Impairment often use more Reliance type strategies (Domínguez Chávez et al., 2021; Farias et al., 2020; Meléndez et al., 2012). In addition, frequent use of Reliance type strategy was related with higher SMC, poorer objective memory, and less verbal learning (Lin et al., 2020). Regarding cognitive impairment, several studies have found that a higher level of SMC is associated with more use of MCS, but not necessarily increases with objective memory performance (Frankenmolen et al., 2017; Hertzog et al., 2019).
Although SMC are common among the healthy elderly, it has not been yet determined whether they use the same MCS as older adults with a high SMC. As older adults with higher SMC fulfill the main risk factor for cognitive decline in MCI, it is important to investigate which MCS they spontaneously use, and if they may help them maintain an independent functioning in daily living activities. Studying these differences will provide useful information to improve cognitive rehabilitation to prevent or retard the onset of the Alzheimer´s type dementia.
The general purpose of this study is to describe and compare MCS implemented by cognitive healthy older people with and without SMC. In order to better address this general purpose, the following specific objectives were proposed: (1) describe the types of forgetfulness and compare the SMC level according to sociodemographic data (gender, age, educational level and cognitive performance); (2) describe the MCS implemented by older adults and compare them according to sociodemographic data (gender, age and educational level). The hypothesis regarding these objectives was that the SMC would be less, and the MCS would be more effective in women, younger, with higher educational level and better performance in cognitive tests. When comparing groups, those with higher SMC would use more MCS that would not necessarily be more efficient or adaptive.
An exploratory, observational, cross-sectional, and quantitative study was carried out. The target and accessible population were elderly people who lived in their homes and/or attended centers for the elderly in CABA (Autonomous City of Buenos Aires). In these centers, older people carry out different sociocultural activities programmed to strengthen the well-being of older people. Data collected in the centers for elderly, were provided by the Government of the City of Buenos Aires (Subsecretaría de la Tercera Edad del Gobierno de la Ciudad), in the framework of the study and approved procedures on Healthy Longevity conducted between UCA (Argentine Catholic University) and ILSI (International Life Sciences Institute) (agreement Res n°: 01-17 CNV, year 2017-2019).
A non-probabilistic sampling was carried out for convenience. The sample was collected between March 2018 and February 2020. An individual interview was carried out in which, firstly, the inclusion/exclusion criteria were evaluated: absence of alterations in cognitive status and symptoms of severe depression. For this, the Mini Mental State Examination (MMSE), the Clock Test and the Yesavage Geriatric Depression Scale (GDS) were used (see cut off scores at Instruments section). Secondly, the Subjective memory complaints and Memory compensation strategies questionnaires were administered. The cognitive screening and interviews were individual, and lasted between 30 and 40 minutes, carried out in a single date.
The inclusion criteria were being over 60 years old both sexes, non-institutionalized, and self-sufficient (able to move and manage for themselves). The exclusion criteria were major cognitive impairment (determined in an assessment interview, neurocognitive test) and presence of auto-reported symptoms of severe depression. The exclusion of these aforementioned factors was to ensure that the participants could remember details of daily life, which would allow the evaluation instruments to be implemented.
All the participants included in the sample agreed to participate voluntarily and signed the informed consent. Each participant was informed about the objectives, purpose and importance of the study, as well as about the possible inconveniences associated with their participation. The freedom to participate and to be able to withdraw from the study at any time was emphasized. The confidentiality of the data was explained and guaranteed. The informed consent form was prepared according to the guidelines of the Human Health Research Guide (2016) and Law 25326 on the Protection of Personal Data.
Among the 121 older adults evaluated, there were 63.6 % women (n = 77) and 36.4 % men (n = 44). The average age was 71.7 ± 7.8 years, with a minimum of 60 and a maximum of 92 years. The majority of the adults evaluated finished high school (M = 13.23; SD = 3.16).
A cognitive screening was conducted to complete the inclusion/exclusion criteria including the following tests in the order as follows:
Mini Mental State Examination (MMSE) (Butman et al., 2001). A widely used screening instrument in clinical neuropsychology. It evaluates different functions: time-space orientation (assessed by asking the participant to indicate the date, the season and location); fixation and immediate memory (evaluated by asking to repeat three words); attention and working memory (tested by asking to perform a series of subtractions); long-term memory (tested by asking to recall the three words mentioned above) and a series of tests to probe language, naming, writing and praxis. Depending on the participant's performance, each item carries a given score, with a maximum score of 30. The internationally recommended cut-off score for geriatric patients is 24, reporting a specificity of 75 % and sensitivity of 89 %.
Clock Drawing Test (CDT) (López et al., 2014). This screening test evaluates visuospatial and motor functions, as well as auditory comprehension, memory, planning and attention. The task consists of asking the participant to draw a round clock on a blank page, with all the numbers in order and the hands indicating a certain time. It is scored on a scale of 0 to 10, considering the sphere (0 to 2 points), the numbers (0 to 4 points) and the clock hands (0 to 4 points). The cut-off score for mild grade dementia is ≤ 6 points, demonstrating a sensitivity of 92.8 % and a specificity of 93.5 %.
Yesavage Geriatric Depression Scale – GDS (Tartaglini et al., 2017): scale for the assessment of depressive symptoms in older adults; scores less than four indicate no depression, between four and six indicate mild depression, and scores greater than seven indicate severe depression.
The following neuropsychological tests were used to acknowledge the cognitive performance of the older adults:
Frontal Assessment Battery (FAB) (Dubois et al., 2000). It is a screening used to detect the presence and/or severity of dis-executive syndromes. It has six tests that are scored from 0 to 3 and evaluate conceptualization, mental flexibility, motor programming, sensitivity to interference, inhibitory control and environmental autonomy. The total score is 18 points, and the cut-off score is 16, with a sensibility of 89 %.
Semantic Fluency Test (Butman et al., 2000). It is a verbal recall test that evaluates executive functions and the ability to store, retrieve and recall information. For this test, the participant is asked to say, in the limited time of one minute, as many animals as he can think of. The local scales are stratified according to age and educational level, which makes it possible to identify whether or not the participant falls within an expected performance.
In addition, the participants filled the following self-reported questionnaires:
Subjective Memory Complaint Questionnaire (SMCQ) (Mías, 2007). It consists of a self-report questionnaire inquiring about the type and frequency of different types of forgetfulness. It inquiries about daily forgetfulness, use of inappropriate words, language forgetfulness, involuntary acts or distractions, the manipulation of everyday objects, the meaning of known words and forgetting that he had to remember something. It is made up of 20 items ranging from 1 to 10, asking the frequency of forgetfulness in the last month: almost never (1-2), sometimes (3-4-5), frequently (6-7-8) and almost always (9-10). The total score is obtained by adding all the values (maximum 200 and minimum 20) and then dividing by the total number of items (20). Thus, a value ranging between 1 and 10 is obtained, where a score higher than 5 would be accounting for a subjective complaint of increasing and considerable frequency.
The Memory Compensation Strategies Questionnaire (MCQ) (Meléndez et al., 2013) is a self-report questionnaire which inquiries about the compensation strategies the person sets in play to undergo the cognitive challenges throughout life. It consists of 45 items with a Likert-type response, from 1 (never) to 5 (always) for frequency, and from 1 (much less) to 5 (much more) for items where the person is asked to compare him/herself with 5-10 years ago. It consists of five main scales: external, internal, time, effort, trust, success and change.
Percentages, means, and frequency were used for descriptive analyses. To answer the inferential objectives, it was used Pearson's r test and Student's t-test as appropriate. SPSS 25 software was used.
According to the cognitive screening, all participants belonged to a healthy aging confirmed by the scores (see cut-off scores in the Instruments section) in the MMSE (M = 28.33; SD = 1.76), the CDT (M = 8.97; SD = 1.37) and the FAB (M = 17.01; SD = 1.28).
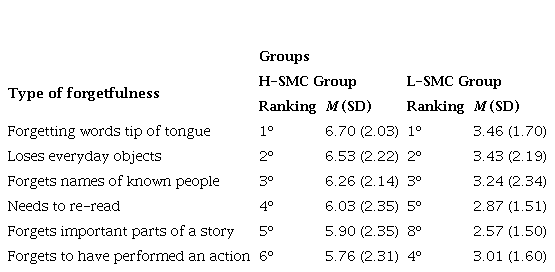
To begin with, following the first specific objective, participants were divided into two groups, with low score in the SMCQ (L-SMC) (≤ 3.69) and with high score in the SMCQ (H-SMC) (≥ 3.70). These scores were obtained, according to their performance in the 75 and 25 percentiles, respectively. Later, descriptive analysis were carried out regarding the frequency of forgetfulness among groups. Table 1 shows the top 6 types of forgetfulness reported by both groups (Table 1). These six types of forgetfulness, in addition with the other 14 of the SMCQ, showed significant differences (p < .000) when analyzing between H-SMC group and L-SMC group.
Table 1.
Types of forgetfulness. Differences in frequencies between groups
Note:
Student’s t test was carried out and showed significant differences in all types of forgetfulness between both groups.
H-SMC: High subjective memory complaints; L-SMC: Low subjective memory complaints
As detailed in Table 1, both groups reported similar frequencies in the first three types of forgetfulness ("forgetting words or having them on the tip of the tongue", "loses everyday objects” and “forgets names of known people”) but a greater frequency (almost twice as high) was reported in the H-SMC group.
Moreover, it was compared the SMC level according to sociodemographic data. In this sample of healthy older adults, there was no correlation between SMC and sociodemographic variables such as age, education or sex. Regarding cognitive performance, only a significant weak negative correlation was observed with the semantic fluency test (r = -.257; p < .001), since this is one of the most sensitive tests to detect cognitive decline in older adults.
Further, analysis compared the MCS implemented by the older adults according to sociodemographic data. In this case, the sociodemographic analysis of the compensation strategies components revealed no correlations between the type of compensation strategy and age. Regarding years of education, there was a negative weak correlation between the educational level and the Success factor (r = -.23; .011), indicative that more educated elderly perceived less necessity or motivation to compensate memory deficits. As for gender, women used more Internal [t (117) = 1.93; p = .05; d = .38], Time [t(118) = 1.66; p = .03; d = .39], Effort [t(117) = 1.94; p = .05; d = .37] and Change strategies [t(116) = 3.22; p = .002; d = .62] in contrast to men according to the same age. It is important to note in these that the effect size of the Internal, Time and Effort strategies is small; while the effect size of the Change strategy is moderate, indicating a greater difference.
To achieve the general purpose of the present study, several analyses were carried out to compare the SMC and the MCS. In the first place, while taking into account the total sample, the elderly´s score in the SMCQ was correlated with various compensation strategies, founding that the greater the subjective memory complaint, the more Time (r = .22, p = .01), Effort (r = .37; p < .001), Reliance (r = .36; p < .001) and Change (r = .26; p = .004) strategies were used.
Considering these previous results, further analysis were carried out comparing both groups (L-SMC vs. H-SMC). It is important to affirm that no significant differences in age, educational level and cognitive performance between groups were found. Moreover, results comparing both groups, showed differences between sex in the use of Time compensation strategy [t(118) = 2.08; p = .039; female M = 2.65; male M = 2.30; d = .39] and Change [t(116) = 3.02; p = .002; female M = 2.91; male M = 2.50; d = .62]. This last subscale (Change) presented a moderate effect size.
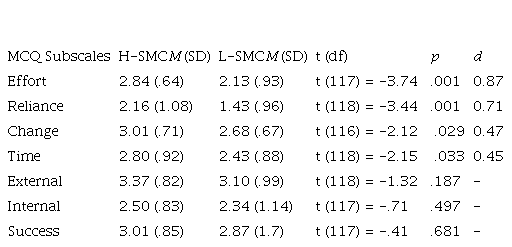
Finally, when analyzing the compensation strategies used by this group (H-SMC), results have showed that they scored significantly higher in the following MCQ subscales: Time (M = 2.80; SD = .92; p < .03), Effort (M = 2.84; SD = .64; p < .000), Reliance (M = 2.16; SD = 1.08; p < .001) and Change (M = 3.01; SD = .71; p = .029). Effect sizes were calculated accordingly (see Table 2), showing meaningful differences between groups.
Table 2.
Compensation strategies used by H-SMC and L-SMC groups
Note:
MCQ: Memory compensation questionnaire; H-SMC: High subjective memory complaints; L-SMC: Low subjective memory complaints.
t: Student’s t test score; df: degrees of freedom; p: significance level.
The purpose of this study was to compare the subjective memory complaints with the compensation strategies implemented by healthy older adults. Its relevance lies in the fact that these subjective memory complaints may be the prelude to a major neurodegenerative pathology or dementia and the way of compensating them indicates a greater or lesser degree of adaptation to them.
Initially, it is important to state that, in the sample selected for the present study, where there are a higher proportion of women than men, it can be observed that their cognitive performance coincides with a normal one, without cognitive impairment. This allows to think that all the conclusions reached are oriented to a population without clinical pathology.
As a descriptive measure, the group of elderly who reported a higher frequency of forgetfulness and H-SMC was analyzed. This group showed the same type of forgetfulness ("forgetting words or having them on the tip of the tongue", "loses everyday objects” and “forgets names of known people”) as the L-SMC group, although with a higher intensity. The complaint “loses everyday objects” was found to be related to forgetfulness reported by patients with lower cognitive performance (Mías, 2007; Schmitter Edgecombe & Dyck, 2014). “Forgetting word or having them on the tip of the tongue” is related to the tendency found, where these participants scored lower in the verbal fluency test.
Furthermore, in the overall sample, no differences were found according to sex, age and educational level. However, a relationship was found between high SMC and a decrease in semantic verbal fluency. This could be found to be related to the type of complaint, which is more frequently mentioned by participants (“forgetting words or having them on the tip of the tongue”). This could indicate that the older adult, who perceives more deficits in his memory, would present greater difficulties in his speech to produce a fluent spontaneous speech without excessive pauses or failures in the search for the right word (Butman et al., 2000).
In addition, the MCS used by the elderly were also analyzed and no changes were found with age, related to the fact that this was a controlled variable for the inclusion of the participants in the study (adults over 60). Regarding gender, in the general sample, our results agree with the fact that women use more MCS in general (Farias et al., 2020; Martin et al., 2014), especially Internal, Time and Change (Mayordomo et al., 2015; Pizzonia & Suhr, 2022).
Besides, when analyzing differences between men and women, separating groups (L-SMC vs. H-SMC) these results agree with previous studies, and with the general sample, where women tended to use more compensation strategies than men (Farias et al., 2020). However, men tend to rely more on their spouses how live more and better (Pizzonia & Suhr, 2022). These results show no significant differences in the use of the Reliance strategy between the sexes. A possible explanation for these findings would be that by segmenting the sample into two groups according to the perception of complaints (L-SMC vs. H-SMC), the size of the sample decreased considerably and with it, the proportion of men in the sample also diminished.
The main objective of this research was to study whether there were differences between the MCS used by healthy older adults with H-SMC and those with L-SMC. To fulfill this aim, the implementation of MCS chosen by those who have a subjective perception or experience of daily forgetfulness was sought to distinguish. Thus, it was corroborated that the greater the perception of SMC, the greater the use of MCS in general.
When dividing groups according to their performance in the SMC Questionnaire, this hypothesis was proven, and it was found that older adults who perceived more memory complaints problems (H-SMC) use different compensation strategies than those with L-SMC. These findings are consistent with previous studies, that affirm that these compensatory mechanisms represent the need, for both internal and external aids, that older people who perceive some decline have (Farias et al., 2020; Schmitter Edgecombe & Dyck, 2014). As they perceive deficits in their memory, they need more aids and, therefore, set forth compensatory mechanisms that allow them to adapt better to daily life (Mayordomo et al., 2015; Schmitter Edgecombe & Dyck, 2014).
Additionally, the results indicate that older people with H-SMC use more of the following compensation strategies: Time, Effort, Reliance and Change. In previous studies, it was pointed out that Effort and Time were remediation strategies, which refer to the energy disposed by the elderly in using resources to mitigate their memory loss (Dixon et al., 2001; Mayordomo et al., 2015). Nevertheless, those with H-SMC use more of the Reliance strategy, that responds to a substitution mechanism characterized by using support from another person to compensate for their perceived loss and can be the prelude of a greater decline (Mayordomo et al., 2015). This mechanism may not necessarily represent a compensation strategy as much as a decline in their independence (Farias et al., 2020). That is why it is important to take it into consideration as a preventive measure to anticipate further decline (Schmitter Edgecombe & Dyck, 2014). Furthermore, in this study, older adults with H-SMC presented a higher score on the complementary Change strategy scale, since they refer to an increase in the use of these strategies over time.
Finally, participants with H-SMC were also the ones with higher use of memory compensation strategies altogether. Besides, the greater the use of compensation strategies is strongly associated with better cognitive ability (better memory and executive function) and functional independence, regardless of the cognitive status (Farias et al., 2020). The present participants were all healthy, cognitively normal and independent in their daily life activities, so further research should include different life-trajectories and diagnosis such as mild cognitive impairment and dementia. Knowing which compensatory strategies exactly help in the maintenance of the daily activities, can prevent independence, and mitigate the cognitive changes and decline due to age.
In addition, preliminary analysis would suggest that the group with H-SMC scored higher in depression and presented greater symptoms of psychological distress. It will be important in the future to investigate the extent to which psychological aspects are related to the presence of SMC and the use of MCS.
The conclusions reached in this study may present, in part, certain limitations and should be considered in the evaluated context. A greater proportion of the sample (63.6 %) were women. Although this is the available sample, given that women consult and frequent more social meetings, it would be appropriate to delve deeper into the male population. Besides, most of the sample evaluated concluded high school, so further research should be held for a less educated population. In turn, the scales were self-administered, and this not only caused the loss of many cases, because they were incomplete, but may also have presented some reading errors. Further research on a diverse sample is required to generalize the previous findings.
In conclusion, emerging evidence suggests that a greater and proper use of MCS can mitigate cognitive decline and that these strategies can be taught and trained. This information is critical because prolonging patients’ independence can be related to a better quality of life and healthier aging, so further therapeutic interventions should include this preventive technique by teaching MCS.
redalyc-journal-id: 180
