Abstract: The COVID-19 pandemic has caused great psychological distress in healthcare workers, especially among nurses. The main objective of this study was to evaluate the impact of the COVID-19 crisis on a large sample of Spanish nurses in the public health system in terms of anxiety, depression, perceived stress, fear of COVID-19, compassion fatigue, burnout, and demand for psychological help, as well as the possible effect of preventive confinements on these variables. A cross-sectional descriptive study design was developed in December 2020 among 439 registered nurses from the Public Health Service of the Principality of Asturias. Psychological variables were measured by using the Hospital Anxiety and Depression Scale (HADS), the Perceived Stress Scale (PSS), the Fear of COVID-19 Scale (FCV-19S), and the compassion fatigue and burnout subscales from the Professional Quality of Life Questionnaire (ProQoL). The study found 37.6 % of nurses with anxiety and 17.1 % with depression. Perceived stress and compassion fatigue levels were medium/high. Also, burnout level was high in 50.6 % of participants. Being a woman (medium/large effect size), working with COVID-19 patients (medium effect size) and previous quarantines (small/medium effect size) were associated with higher psychological distress. Preventive quarantines increase anxiety and fear of COVID-19 (medium effect size), depression and compassion fatigue (small effect size). The COVID-19 infection does not have a significant impact in terms of psychological distress or professional quality of life among nursing professionals. Given the high proportion of professionals at risk of developing emotional disorders, the implementation of mental health preventive programs is needed.
Keywords: COVID-19, quarantine, psychological distress, anxiety, depression, burnout, nurses.
Resumen: La pandemia de COVID-19 ha causado un gran distrés psicológico en forma de estrés, ansiedad y depresión en los profesionales sanitarios de todo el mundo, y especialmente en las enfermeras, que afectaron su calidad de vida profesional. El objetivo principal de este estudio fue evaluar el impacto de la crisis del COVID-19 en una amplia muestra de enfermeras españolas del sistema sanitario público, en términos de ansiedad, depresión, estrés percibido, miedo al COVID-19, fatiga por compasión, burnout y demanda de ayuda psicológica, así como el posible efecto de los confinamientos sobre estas variables. A tal fin, se llevó a cabo una comparación entre profesionales que habían realizado o no confinamientos preventivos por contacto estrecho y entre aquellos profesionales que habían sufrido o no la infección por COVID-19. Se realizó un estudio descriptivo transversal en el que participaron 439 enfermeras y enfermeros del Servicio Público de Salud del Principado de Asturias, España, en diciembre de 2020. Para la medida de las variables de interés se utilizaron las versiones adaptadas y validadas en el contexto español de la Escala Hospitalaria de Ansiedad y Depresión (HADS), la escala de estrés percibido (PSS), la escala de miedo a la COVID-19 (FCV-19S), y las subescalas de fatiga por compasión y burnout del Cuestionario de Calidad de Vida Profesional (ProQoL). De acuerdo a los puntos de corte establecidos para la detección de casos, se identificaron un 37.6 % de casos de ansiedad, sin diferencias entre ambos sexos, así como un 17.1 % de casos de depresión, con una incidencia prácticamente duplicada en las mujeres. Los niveles de estrés psicológico fueron medios/altos en la muestra, y se observó una correspondencia completa entre el porcentaje de casos detectados de depresión y el porcentaje de participantes con un nivel alto de estrés percibido, que fue asimismo del 17.1 %. Del mismo modo, se observaron niveles altos de estrés percibido en el doble de mujeres que de hombres. Respecto a la fatiga por compasión, constructo que en el contexto sanitario refleja el coste psicológico de cuidar a los pacientes y acompañarlos en su sufrimiento con el deseo de aliviarlo, sus niveles fueron medios/altos en la muestra, pero resultaron más altos entre las mujeres. Finalmente, el 50.6 % de los participantes presentó altos niveles de burnout. Las puntuaciones en todas las variables fueron mayores en mujeres (tamaño de efecto medio/grande) y en profesionales con alta exposición a pacientes COVID-19 (tamaño de efecto medio). El 38.5 % de los participantes estimó necesario recibir ayuda psicológica para afrontar la situación, y hasta el 86 % consideró que hubiera sido útil recibir este tipo de ayuda profesional en el propio lugar de trabajo. Como dato relevante, los participantes que habían realizado confinamientos preventivos por contacto estrecho con personas infectadas mostraron un mayor impacto psicológico, con mayor ansiedad y miedo a la COVID-19 (tamaño de efecto medio), así como una mayor depresión y fatiga por compasión (tamaño de efecto pequeño). La infección por COVID-19 no produjo un mayor impacto en la salud mental ni en la calidad de vida profesional. En definitiva, ser mujer, trabajar con pacientes COVID-19, y la realización de confinamientos preventivos asociaron un mayor distrés psicológico en la muestra. Los confinamientos preventivos incrementaron la ansiedad y el miedo a la COVID-19, la depresión y la fatiga por compasión, mientras que la infección por COVID-19 no produjo un impacto significativo en el distrés psicológico de las enfermeras y enfermeros durante la crisis pandémica. Dada la alta proporción de profesionales en riesgo de presentar trastornos emocionales como ansiedad y depresión, es necesario implementar programas preventivos y de promoción del bienestar psicológico.
Palabras clave: COVID-19, confinamiento, distrés psicológico, ansiedad, depresión, burnout, enfermería.
Artículos
Nurses´ mental health and professional quality of life during the COVID‑19 crisis: Effects of preventive quarantines
Salud mental y calidad de vida profesional de las enfermeras durante la crisis COVID‑19: Efectos de los confinamientos preventivos
Centro Interamericano de Investigaciones Psicológicas y Ciencias Afines

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-CompartirIgual 4.0 Internacional.
Recepción: 23 Junio 2022
Aprobación: 12 Octubre 2022
The COVID-19 crisis has been the biggest global public health problem in decades and for many healthcare professionals it will represent the greatest professional challenge of their lives. For them, the crisis has resulted in high exposure to occupational stressors that can lead to psychopathological symptoms (Bettinsoli et al., 2020; Chen et al., 2020; Lai et al., 2020). In addition to the high care pressure caused by successive waves of the pandemic, there are also concerns such as the fear of becoming infected or infecting one's family (Wang et al., 2020). Among other factors, physical exhaustion, uncertainty, fear of not providing competent care, or lack of support have been linked to mental health problems (Pappa et al., 2020).
Numerous studies have found significant levels of anxiety, depression, and psychological distress in healthcare professionals since the beginning of the health crisis (Alonso et al., 2020; Lai et al., 2020; Pappa et al., 2020), as well as a negative impact on the quality of professional life in terms of burnout (BO) and compassion fatigue (CF; Dosil-Santamaría et al., 2021; Ruiz-Fernández et al., 2020). These effects are more intense in front-line professionals, women and young professionals (Lai et al., 2020; Pappa et al., 2020; Romero et al., 2020).
Physicians and nurses are the professionals most vulnerable to the crisis (García-Fernández et al., 2020; Rodríguez-Rey et al., 2020), and this vulnerability would be greater in nurses as they present higher levels of stress during the pandemic (Mo et al., 2020). In addition, greater stress is a risk factor for emotional disorders such as anxiety or depression, which are also more prevalent in women (Pérez-Martínez & Gabiña, 2019). These reasons, and especially the CF or personal cost of the helping relationship with the patient, lead us to consider nurses as a group particularly vulnerable to the psychological impact of the current crisis (García-Fernández et al., 2020; Rodríguez-Rey et al., 2020).
Despite the enormous amount of research that has been produced, to our knowledge there are no studies that evaluate the effect of close-contact preventive confinement or the experience of COVID-19 infection on both mental health and professional quality of life in Spanish healthcare professionals, and none that investigate the effect of these experiences on fear of infection.
The main objective of this study was to evaluate the impact of the COVID-19 crisis on a large sample of Spanish nurses in the public health system in terms of anxiety, depression, perceived stress, fear of COVID-19, CF, BO and demand for psychological help, as well as the possible effect of preventive confinements on these variables.
A descriptive cross-sectional study was conducted on a convenience sample of 439 nurses from 9 hospitals and 15 health centers of the public health system of the Principality of Asturias, an autonomous community located in the north of Spain. This public system has a network of 14 hospitals and more than 60 health centers that provide primary and specialized healthcare to a population of one million people. From the beginning of the current crisis, all COVID-19 patients in Asturias were diagnosed and cared by this network, including those with very severe symptoms that required admission to intensive care units.
A minimum required sample size of 355 was calculated considering a population of 4,550 nurses working in the public health service of the Principality of Asturias, with an error margin of 5 % and a 95 % confidence interval.
All registered professionals in the autonomous community were invited to participate by means of an e-mail sent from the Official College of Nursing of the Principality of Asturias. This email informed of the objectives of the study, warning that only those who met the inclusion and exclusion criteria could participate: being over 18 years, working as a nurse in the Public Health Services of the Principality of Asturias, working uninterruptedly during the months of September to December 2020 corresponding to the second pandemic wave of COVID-19 in Spain, and not having presented at any time sick leave due to temporary disability during that period.
For the collection of sociodemographic and labor data, an ad hoc questionnaire was designed, including age, sex, marital and work setting.
Hospital Anxiety and Depression Scale (HADS)
Anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS; Terol-Cantero et al., 2015). This tool consists of 14 items divided into two independent subscales of the same length. Each item is evaluated on a 4-point Likert scale from 0 (low frequency) to 3 (high frequency). It is an instrument that, despite its name, allows the assessment of anxiety and depression in the general population in terms of "cases", "probable cases" and "non-cases". High scores on each subscale indicate higher levels of anxiety or depression. The psychometric properties of this scale are optimal (Terol-Cantero et al., 2015). In our sample, a Cronbach's alpha of .87 was obtained for the anxiety subscale and .85 for the depression subscale.
Perceived Stress Scale (PSS)
Stress was assessed using the Spanish version of the Perceived Stress Scale (PSS; Remor, 2006). The instrument consists of fourteen 4-point Likert scale items ranging from 0 (never) to 4 (very often), with high scores indicate high levels of perceived stress. The scale has good reliability, with a Cronbach's alpha of .81 (Remor, 2006). Excellent reliability was obtained in our sample, with a Cronbach's alpha of .90.
Fear of COVID-19 Scale (FCV-19S)
Fear of COVID-19 was assessed using the Spanish version of the Fear of COVID-19 Scale (FCV-19S). This instrument consists of 7 five-point Likert scale items ranging from 1 (total disagreement) to 5 (total agreement). The Spanish validation reports robust psychometric properties (Martínez-Lorca et al., 2020). In our sample a Cronbach's alpha of .89 was obtained.
Professional Quality of Life (ProQoL)
ProQoL (Morante-Benadero et al., 2006) was used to assess BO and CF. This tool also allows to assess the compassion satisfaction, but this subscale was not used in this study according to the purpose of evaluate the negative costs of caring others during the pandemic. Each of BO and CF subscales includes ten 6-point Likert items from 0 (never) to 5 (always). High scores on each subscale indicate high levels in BO and CF respectively. The Spanish version of the ProQoL has a Cronbach's alpha of .54 for BO and .78 for CF. In this study was obtained an alpha of .57 for BO and .86 for CF.
Need for psychological help and COVID-19 diagnostic
The need for psychological help and the perceived usefulness of receiving such help in the workplace itself was assessed by two questions. The first was "Do you think you will need psychological help during the COVID-19 crisis?" whose response options were "I don't think I need it"; "I think I will need it"; "I need it and have already requested it" and "I am receiving psychological help". The second question was "Do you think it would be useful to receive psychological help in the workplace itself during the crisis?" whose response options were "Not at all"; "Hardly useful"; "Not sure"; "Useful" and "Very useful".
Finally, the questionnaire included two dichotomous yes/no response questions:
"Have you ever received a medical diagnosis, or a positive COVID-19 test?" and "Have you ever been preemptively confined by close contact with an infected person?"
Data collection was carried out by means of an online Google Forms questionnaire whose link, disseminated through the same mailing, was available between December 2 and 24, 2020. Participants who did not expressly acknowledge strict compliance with the inclusion and exclusion criteria were automatically excluded by the tool itself, as well those who did not provide informed consent to participate voluntarily in the study. It is interesting to note that during the second pandemic wave in Spain, the Principality of Asturias recorded the highest incidence of cases, the highest mortality due to COVID-19 and the greatest healthcare pressure to date.
In order to assess the clarity, comprehension and accessibility of the tool, before starting the dissemination of the questionnaire, it was piloted on December 1, 2020 in 40 professionals (10 % of the sample). Completion time of the questionnaire, which was anonymous, took 20 minutes. No incentives were offered for participation.
The study was approved by the Research Ethics Committee of the Principality of Asturias (563/2020). The ethical principles of the Declaration of Helsinki were respected at all times. The confidentiality of the data and the anonymity of the participants were preserved in accordance with the Organic Law 3/2018 of 5 December on the Protection of Personal Data and Guarantee of Digital Rights.
For data analysis, the sample was first divided into two categories according to high or low exposure to COVID-19 patients. In accordance with previous studies (Alharbi et al., 2020; Trumello et al., 2020) professionals with high exposure were considered to be those working in emergency departments, intensive care units for COVID-19 patients and hospital units equipped for these patients (n = 161). The rest of the professionals, including primary care, conventional hospital units and others, were considered to have low exposure (n = 278).
A descriptive analysis of frequencies and percentages of the variables anxiety, depression, perceived stress, BO and CF was performed, taking into account low, medium and high levels of these variables according to the cut-off points of the tools used. The percentages of professionals who considered psychological help necessary were calculated. Differences in anxiety, depression, perceived stress, BO, CF, and fear of COVID-19 were analyzed by comparing between different groups. The comparison groups were: men and women; professionals with high and low exposure to COVID-19 patients; professionals who did or did not consider psychological help necessary, professionals who had or had not been infected by COVID-19, and finally those who had or had not performed preventive close-contact confinement. All these comparisons were performed using Student's t-test for independent samples. Finally, the effect size was calculated using Cohen's d, considering small values from 0.1 to 0.3, medium values from 0.3 to 0.5 and large values from 0.5 and above.
All statistical analyses were performed with SPSS v. 24.0.
A total of 439 professionals with an age range of 22 to 64 years (M = 41.53; SD = 11.38) participated. All sociodemographic and occupational data of the sample can be seen in Table 1.
Table 1.
Descriptive data on socio-demographic and labor variables
shows the percentages of professionals grouped into low, medium and high levels of perceived stress, anxiety, depression, BO and CF, as well as the cut-off points for each of the instruments used. These levels are presented according to sex and high or low exposure to COVID-19 patients.
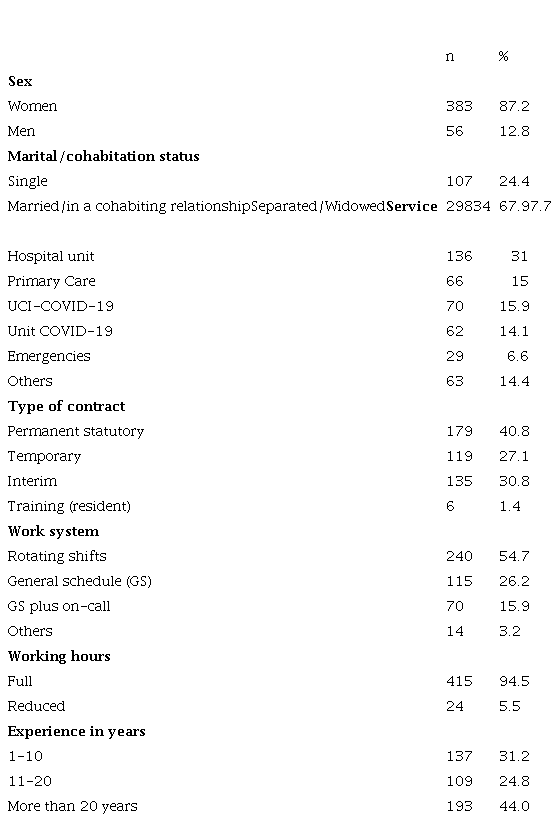
Table 2 shows the percentages of professionals grouped into low, medium and high levels of perceived stress, anxiety, depression, BO and CF, as well as the cut-off points for each of the instruments used. These levels are presented according to sex and high or low exposure to COVID-19 patients.
Perceived stress levels were moderate in 65.4 % of the sample and high in 17.1 %. Cases of anxiety and depression were detected in 37.6 % and 17.1 % of participants, while 24.8 % and 28 % of the sample were identified as probable or at-risk cases of anxiety and depression, respectively. BO levels were medium in 11.4 % of the sample and high in 50.6 %, while CF levels were medium in 27.1 % and high in 59.7 %. Only 1.4 % and 13.2 % of the participants had low levels of BO or CF, respectively. Scores according to the percentages exposed tend to be higher for women and nurses with high exposure. Next, it will be tested whether these differences are statistically significant.
Table 2.
Frequencies and percentages of nurses at different levels of perceived stress, anxiety, depression, burnout, and compassion fatigue as a function of sex and high or low exposure to COVID-19 patients (N = 439)
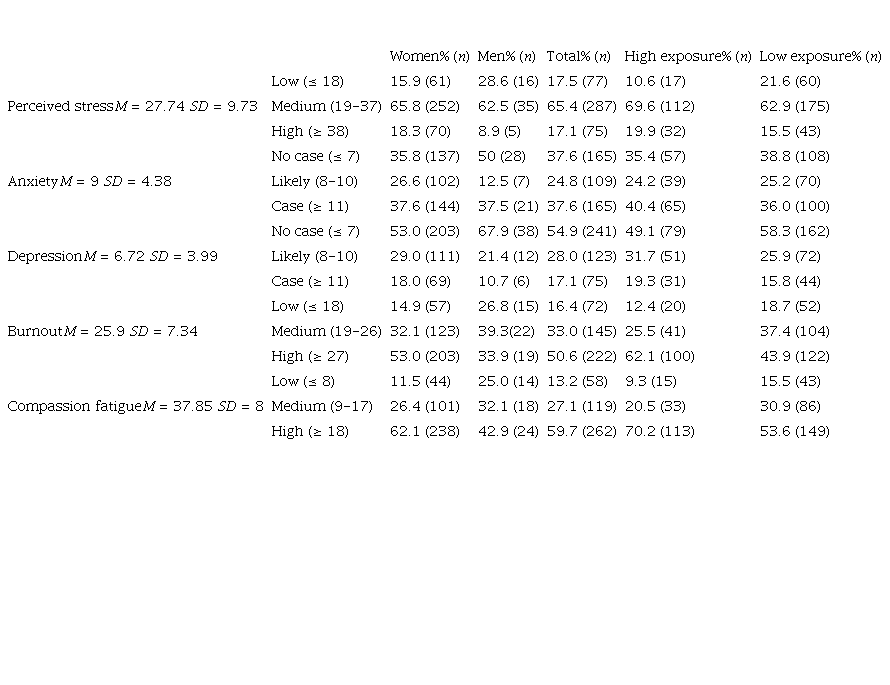
Note: The cut-off points used to form the groups are indicated in parentheses.
Perceived stress was higher in professionals with high exposure (M = 29.17) with respect to the rest (M = 26.91, p = .019) with a small effect size (d = .23). The same was observed for the anxiety variable, with higher levels in first-line nurses (M = 9.63) than in the rest of the professionals (M = 8.65, p = .023) with an effect size also small (d = .23). However, no differences were found between professionals with high and low exposure to infected patients in fear of COVID-19 and in depression. On the other hand, differences in BO were found between professionals with high exposure to COVID-19 patients (n = 161) and low exposure (n = 278), with BO being higher in the nurses with high exposure (M = 27.36) with respect to the nurses with low exposure (M = 25.06, p = .001) with an intermediate effect size (d = .32). Similarly, significant differences in CF were observed between professionals with high exposure (M = 22.54) versus low exposure (M = 19.73, p = .004) with a small effect size (d = .29).
Finally, statistically significant differences were found between men and women in all psychological variables, as shown in Table 3.
Table 3
T-test for the difference in means between women and men
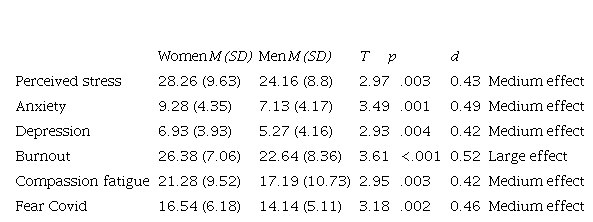
Note: T: value of the t-statistic; p: p-value of the t-test for the mean difference; d: effect size according to Cohen's d.
Regarding the demand for psychological help, 38.5 % of the sample considered this help necessary, while 7.7 % were already receiving it. Eighty-six percent of the participants considered that it would have been useful to receive this type of intervention in the workplace. Between those who considered psychological help necessary or were already receiving it (n = 169) and those who did not consider it necessary (n = 270), statistically significant differences were found in all the psychological impact variables analyzed. Thus, nurses who considered it necessary to receive psychological help obtained higher scores on all these variables with a large effect size, as shown in Table 4.
Table 4.
T-test for the difference in means between nurses who considered psychological help necessary or not on different variables (N = 439)
Note: T: value of the t-statistic; p: p-value of the t-test for the mean difference; d: effect size according to Cohen's d
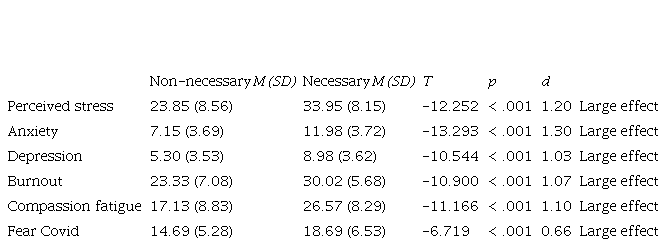
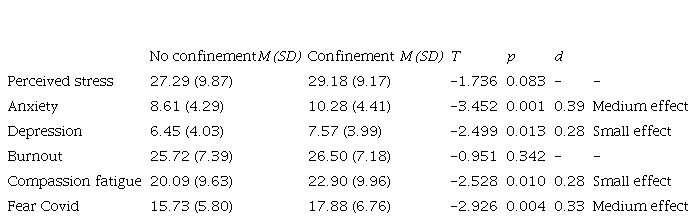
No statistically significant differences were found between those who had received a diagnosis of COVID-19 or positive test (n = 40) and the rest of the professionals (n = 399) in perceived stress (p = .939), anxiety (p = .580), depression (p = .891), BO (p = .354), CF (p = .766) or fear of COVID-19 (p = .337). However, significant differences were observed between those who had performed preventive quarantines (n = 104) and those who had not (n = 335), with levels of anxiety, depression, CF and fear of COVID-19 being higher in the former, as shown in Table 5.
Table 5.
T-test for the difference in means between nurses with and without preventive quarantines
Note: T: value of the t-statistic; p: p-value of the t-test for the mean difference; d: effect size according to Cohen's d
The results of the present study reveal a significant impact on the mental health of nurses during the COVID-19 crisis, with percentages of "cases" and "probable cases" of anxiety and depression high for a sample of active workers. The study shows a high number of cases of depression, anxiety, perceived stress and burnout among nursing staff. Also, being a woman, working with COVID-19 patients, and previous quarantines were associated with higher psychological distress. On the other hand, the COVID-19 infection among nurses does not have a significant impact in terms of their psychological distress or professional quality of life. However, it is important to note that the HADS is only a screening tool used to assess the intensity of anxiety and depression symptoms. Thus, although this scale allows participants to be grouped in terms of "cases", "probable cases" or at-risk cases and "non-cases", it should be emphasized that no score obtained implies a clinical diagnosis of anxiety or depression, and that no score on this scale is a necessary or sufficient condition for diagnosis. The results of our study are similar to others carried out both in Spain (Alonso et al., 2020; Dosil-Santamaría et al., 2021; Erquicia et al., 2020; Lobos-Peña et al., 2021;Londoño-Ramírez et al., 2021; Luceño-Moreno et al., 2020) and in other countries (AlAteeq et al., 2020; Xiong & Peng, 2020). Thus, with respect to depression, the sum of "cases" and "at-risk cases" detected by Luceño-Moreno et al. (2020) yields 51.3 %, slightly higher than our 45.1 %. In their study, the percentage of professionals above the cut-off point for the identification of anxiety risk cases is 79.3 %, also higher than our 62.4 %. Erquicia et al. (2020) found 71.6 % of healthcare professionals with symptoms of anxiety, while Alonso et al. (2020) concluded that 45.7 % of Spanish healthcare professionals present some emotional disorder, a percentage that rises to 50.4 % among nurses. In other countries, Xiong and Peng (2020) found symptoms of anxiety in 40.8 % of nurses, as well as depression in 26.4 %, while Azoulay et al. (2020) identified a prevalence of these symptoms of 50.4 % and 30.4 %, respectively. For their part, Simonetti et al. (2021) observed moderate anxiety levels in 33.23 % of the nurses. In summary, being a nurse during the present crisis is associated with psychopathological symptoms of anxiety and depression (Luceño-Moreno et al., 2020).
There are differences in the results of the studies cited, and these may be due to different reasons such as the use of different samples and assessment instruments. In addition, it is important to consider that environmental conditions have changed over time, so that some shortcomings of the first months of the pandemic, such as the lack of personal protective equipment or less scientific evidence to guide the clinical approach to patients, have improved substantially.
In our study, those professionals who had performed preventive quarantines by close-contact to COVID-19 cases show a greater negative impact on their mental health in terms of anxiety and depression, in coherence with previous studies (Alonso et al., 2020). Our work also reveals that quarantines increase CF and fear of COVID-19, and to the best of our knowledge, this is an unexplored effect in the literature. However, the COVID-19 infection of the own professionals would be a less important variable to consider, or even irrelevant, as it has not been shown to increase the impact on the mental health of nurses or their professional quality of life in terms of BO and CF.
The BO levels is a issue of great concern. A study conducted during the first months of the pandemic in Spain (Ruiz-Fernández et al., 2020) found medium/high levels of both CF and BO in healthcare professionals, as well as perceived stress, especially in front-line workers. However, while the percentage of workers with high levels of CF in that study and ours is practically the same (60.5 % and 59.7 %, respectively), this research found a substantial increase in the percentage of professionals with high levels of BO, which rises from 36 % to 50.6 %. This finding implies that while CF and perceived stress have remained stable, BO could have increased in nurses during the pandemic. Given this scenario and considering the high proportion of nurses at risk of presenting emotional disorders, the need to implement preventive programs aimed at strengthening resilience is justified.
The responsibility of the institutions is fundamental because we will continue to need nurses to face the crisis we are experiencing. Unfortunately, protocolized psychological interventions in healthcare professionals have been scarce during the crisis, with great variations in format and objectives (Priede et al., 2021), despite the reduction in psychological distress and the positive impact on patient care and on the healthcare system itself that they produce (Forner-Puntonet et al., 2021). In this regard, it is important to consider that 86% of the participants in our study considered it useful or very useful to receive psychological interventions in the workplace. This is important because physicians and nurses are generally reluctant to participate in psychological interventions, and that they prefer a face-to-face format as opposed to online (Shechter et al., 2020).
In the interpretation of our results, one aspect to take into account is the context of the lack of nurses in the Spanish healthcare system. This situation has led many professionals with little experience and without advanced training to perform their functions in special services such as the ICU or the emergency room. This situation may have led to greater psychological distress. Especially in young professionals, the absence of consolidated technical skills leads more frequently to experiences of overwhelm and greater perceived stress.
Some limitations of our work should be noted. First, the non-probability sampling used should be considered, which does not fully guarantee that the participants represent the population studied. Secondly, the voluntary nature of the study and the context of the health crisis may have introduced a response bias. In addition, the online evaluation may have discouraged participants from the older age group, as they are less familiar with new technologies. Finally, another limitation is the cross-sectional design used, since the effects of the pandemic are dynamic and their variations cannot be captured in this type of design, requiring longitudinal studies. All these reasons lead us to interpret the results with caution, especially with regard to their generalizability. In conclusion, this study finds a high number of cases of depression, anxiety, perceived stress and burnout among nursing staff. These levels of anxiety, depression, and perceived stress are higher in women and in front-line professionals. Having received a diagnosis of COVID-19 or a positive test is not associated with a greater psychological impact, but having performed preventive quarantines implies higher levels of anxiety, depression, CF and fear.
Healthcare institutions should implement psychological interventions aimed at reducing symptoms of anxiety and depression in healthcare professionals, as well as reducing BO and promoting psychological well-being and resilience. Future research should be directed at assessing the long-term psychological effects of the pandemic on health care workers, especially BO, the current levels of which are of great concern. It would also be timely to evaluate the effectiveness of protocolized interventions to prevent deterioration of mental health and professional quality of life. Deliberate evidence-based interventions are needed to protect the mental health and well-being of healthcare professionals. Implementing prevention and mental health promotion is important for these professionals to enable them to continue caring for patients with the quality of care they deserve.
redalyc-journal-id: 180
shows the percentages of professionals grouped into low, medium and high levels of perceived stress, anxiety, depression, BO and CF, as well as the cut-off points for each of the instruments used. These levels are presented according to sex and high or low exposure to COVID-19 patients.
