Original research
Safety and clinical outcomes of obstetric hysterectomies in patients treated at a tertiary hospital in Chile
Seguridad y desenlaces clínicos de las histerectomías obstétricas en pacientes atendidas en un hospital de atención terciaria en Chile
 Benjamín Moraga-Arias
Fernanda Muñoz-Baeza
Sebastián Cifuentes-Espinoza
Benjamín Moraga-Arias
Fernanda Muñoz-Baeza
Sebastián Cifuentes-Espinoza
Safety and clinical outcomes of obstetric hysterectomies in patients treated at a tertiary hospital in Chile
Revista Colombiana de Obstetricia y Ginecología, vol. 76, no. 2, 4349, 2025
Federación Colombiana de Obstetricia y Ginecología; Revista Colombiana de Obstetricia y Ginecología
Received: 17 November 2024
Accepted: 18 June 2025
ABSTRACT
Objective: To describe the incidence, clinical characteristics, and complications of obstetric hysterectomy in a tertiary hospital in Chile from 2021 to 2023.
Methods: Retrospective descriptive cohort study including all women with a gestational age ≥20 weeks or up to six weeks postpartum who underwent obstetric hysterectomy at Santiago Oriente Dr. Luis Tisné Brousse Hospital. Clinical and surgical data were collected from institutional records. Descriptive statistics were performed.
Results: Twenty-five obstetric hysterectomies were performed during the study period. Incidence per 1,000 live births decreased from 3.22 in 2021 to 1.81 in 2023. Postpartum hemorrhage was the main indication (52%), followed by placenta accreta spectrum (32%), infection (12%), and uterine rupture (4%). Supracervical hysterectomy was performed in 52% of cases, and total hysterectomy in 48%; 68% were emergencies. One intraoperative complication (bladder injury) was reported. Postoperative complications occurred in 84% of cases, the most frequent being anemia (84%) and hemorrhagic shock (36%). No significant associations were found between baseline characteristics and complications.
Conclusion: Although its incidence is declining, obstetric hysterectomy remains associated with high morbidity. Strengthening prevention, early detection, and timely multidisciplinary care is essential. Further prospective, multicenter studies are needed to inform strategies to improve maternal outcomes.
Keywords: Hysterectomy+ postpartum hemorrhage+ cesarean section+ placenta accreta+ postoperative complications.
RESUMEN
Objetivos: Describir la incidencia, características clínicas y complicaciones de la histerectomía obstétrica (HO) en un hospital terciario en Chile entre 2021 y 2023.
Métodos: Estudio descriptivo de cohorte retrospectivo que incluyó a todas las mujeres con una edad gestacional ≥20 semanas o hasta seis semanas posparto que se sometieron a HO en el Hospital Santiago Oriente, Dr. Luis Tisné Brousse. Se recolectaron datos clínicos y quirúrgicos a partir los registros institucionales. Se realizó un análisis estadístico descriptivo.
Resultados: Se realizaron 25 HO durante el período de estudio. La incidencia disminuyó de 3,22 en 2021 a 1,81 en 2023 por cada 1.000 nacidos vivos. La indicación principal fue hemorragia posparto (52%), seguida de espectro de acretismo placentario (32%), infección (12%) y ruptura uterina (4%). Se realizó histerectomía supracervical en el 52% y total en el 48%; el 68% fueron de urgencia. Se registró una complicación intraoperatoria (lesión vesical). Las complicaciones posoperatorias ocurrieron en el 84% de los casos, siendo las más frecuentes la anemia (84%) y el shock hipovolémico (36%). No se encontraron asociaciones significativas entre las características basales y las complicaciones.
Conclusión: Aunque su incidencia ha disminuido, la HO sigue asociada a una alta morbilidad. Es fundamental fortalecer la prevención, detección precoz y atención multidisciplinaria oportuna. Se requieren estudios prospectivos y multicéntricos para mejorar los resultados maternos.
Palabras clave: Histerectomía, hemorragia posparto, cesárea, placenta accreta, complicaciones posoperatorias.
INTRODUCTION
Obstetric hysterectomy refers to the surgical removal of the uterus during pregnancy, childbirth, or within the first six weeks postpartum. This definition includes both total and supracervical hysterectomies, performed either electively or as an emergency procedure following cesarean section or vaginal delivery. Obstetric hysterectomy is typically reserved for cases of severe obstetric hemorrhage that do not respond to more conservative treatments.
Globally, the incidence of obstetric hysterectomy is estimated at approximately 1.1 per 1,000 births 1. The most common indications include severe obstetric hemorrhage and uterine infections, such as myometritis. The procedure is technically demanding due to altered pelvic anatomy, increased uterine vascularization and size, and the urgency associated with controlling life-threatening bleeding. As a result, it is associated with a high risk of complications, including intraoperative hemorrhage, infections, urinary or gastrointestinal tract injuries, and even maternal death 2.
Severe obstetric hemorrhage, defined as blood loss exceeding 1,500 mL 3 is one of the leading obstetric emergencies and a major cause of maternal morbidity and mortality worldwide 4. Its most frequent etiologies include placenta previa, placenta accreta spectrum, uterine rupture, placental abruption, and uterine atony 2,5. Risk factors associated with a higher incidence of severe hemorrhage include advanced maternal age, abnormal placentation, multiparity, multiple gestations, prior cesarean deliveries, preeclampsia, and coagulation disorders 6. Certain causes, such as placenta accreta spectrum -with or without placenta previa- can be diagnosed antenatally, allowing for better prenatal counseling, multidisciplinary planning, and potentially avoiding the need for emergency procedures 7.
Management of obstetric hemorrhage follows a stepwise approach, beginning with medical therapy and supportive measures, and escalating to surgical interventions like uterine artery ligation, B-Lynch sutures, and Bakri balloon placement. Obstetric hysterectomy remains the final option when bleeding cannot be controlled. In cases involving severe uterine infection, such as septic abortion or chorioamnionitis, the use of antibiotics is essential, but surgical intervention, including hysterectomy, may be required to control infection 8.
Understanding the incidence and complications associated with obstetric hysterectomy is critical when evaluating the quality and safety of maternal healthcare services 9. However, there is limited literature on this subject in Chile and Latin America. Both specialized maternal centers as well as general hospitals must be equipped with trained teams capable of performing these procedures, particularly in emergency situations. Moreover, it is essential to generate local data to benchmark outcomes against those reported in comparable institutions.
Therefore, the objective of this study is to describe the safety profile -based on complications and clinical characteristics- of patients undergoing obstetric hysterectomy in a tertiary care hospital in Chile.
MATERIALS AND METHODS
Study Design and Setting: This was a retrospective descriptive cohort study conducted at the Santiago Oriente Dr. Luis Tisné Brousse Hospital, a public Level III referral center for high-risk obstetric care in Santiago, Chile. The hospital provides emergency obstetric services and manages complex maternal- fetal cases. We included all women with a gestational age of ≥20 weeks or up to six weeks postpartum who underwent any type of hysterectomy (total or supracervical) between January 2021 and December 2023. No exclusion criteria were applied. A strict consecutive census sampling method was used.
Procedure: Eligible cases were identified through a review of the hospital’s electronic medical records of all obstetric discharges during the study period. A filter was applied using surgical procedure codes relevant to obstetric hysterectomy, including cesarean section + hysterectomy and hysterectomy alone. Cases were confirmed through cross-verification of operative reports and clinical documentation. Data collection was carried out by trained researchers using a standardized extraction form to ensure data quality. Information was anonymized and stored securely in the institutional database. Quality control was performed via random double-checking of 10% of records. To minimize information bias, variables were predefined and collected systematically. Missing data were explicitly noted in the dataset and considered in the analysis.
Variables: Baseline variables included maternal age, weight, height, body mass index (BMI), parity, gestational age, comorbidities, and a history of prior cesarean section.
Intraoperative variables included hysterectomy type and indication, surgical duration, use of preventive interventions (e.g., tranexamic acid, uterine artery ligation, B-Lynch sutures, Bakri balloon), estimated blood loss, transfusions, and other procedures.
Postoperative outcomes included intensive care unit (ICU) admission, hospital length of stay, complications (e.g., anemia, hemorrhage, infection, shock, thromboembolism), reoperation, and maternal mortality. Follow-up extended to 42 days postpartum.
Statistical Analysis: Data were analyzed using the Jamovi software. Descriptive statistics were applied. Variables are reported as frequencies, means ± standard deviations (SD), or medians with interquartile ranges (IQR), as appropriate. Normality was tested using the Shapiro-Wilk test. The incidence of obstetric hysterectomy was calculated annually per 1,000 live births, based on official birth data, to enable comparisons across settings.
Ethical Considerations: This study was approved by the Scientific Ethics Committee of the Servicio de Salud Metropolitano Oriente. All data were anonymized prior to analysis to ensure patient confidentiality.
RESULTS
Study Population and Incidence of Obstetric Hysterectomy
A total of 25 cases of obstetric hysterectomy were identified between January 2021 and December 2023: 10 in 2021, 9 in 2022, and 6 in 2023. All patients who met the inclusion criteria were included in the analysis. During the same period, 9,694 live births occurred at the institution: 3,109 in 2021, 3,262 in 2022, and 3,323 in 2023. The incidence of obstetric hysterectomy showed a downward trend over the study period: 3.22 per 1,000 live births in 2021, 2.76 in 2022, and 1.81 in 2023, representing an overall reduction of 43.8%.
Baseline Characteristics and Pre-Hysterectomy Interventions. The mean maternal age was 34.2 ± 4.76 years, and the mean BMI was 33 ± 5.85 kg/m2. The median gestational age at delivery was 37 weeks (IQR: 27.6-37.4), and the median parity was 2 (IQR: 1-2). The mean neonatal birth weight was 2,733 ± 931 g. Comorbidities were present in 56% of the patients. Regarding delivery mode, cesarean section accounted for 84% of cases. In terms of previous cesarean sections, 44% of women had none, 32% had one, and 24% had two or more. In the subset of patients with postpartum hemorrhage (n=13), tranexamic acid was administered in 30% of cases, and uterine artery ligation was performed in 46%. A B-Lynch suture was used in only one case (8%), and Bakri balloons were employed in two patients-one after vaginal delivery and one after cesarean section. No cases involved hypogastric artery ligation.
Indication and Type of Hysterectomy, Surgical Details. The leading indication for hysterectomy was uterine atony (52%), followed by placenta accreta spectrum (32%), uterine infection (12%), and uterine rupture (4%). A total of 13 supracervical hysterectomies (52%) and 12 total hysterectomies (48%) were performed. Eight procedures (32%) were elective, and 17 (68%) performed as surgical emergency. The median operative time was 105 minutes (IQR: 90-115), and 13 patients required admission to the ICU. The median ICU stay was 1 day (IQR: 1-3), with a maximum of 32 days. (Table 1)
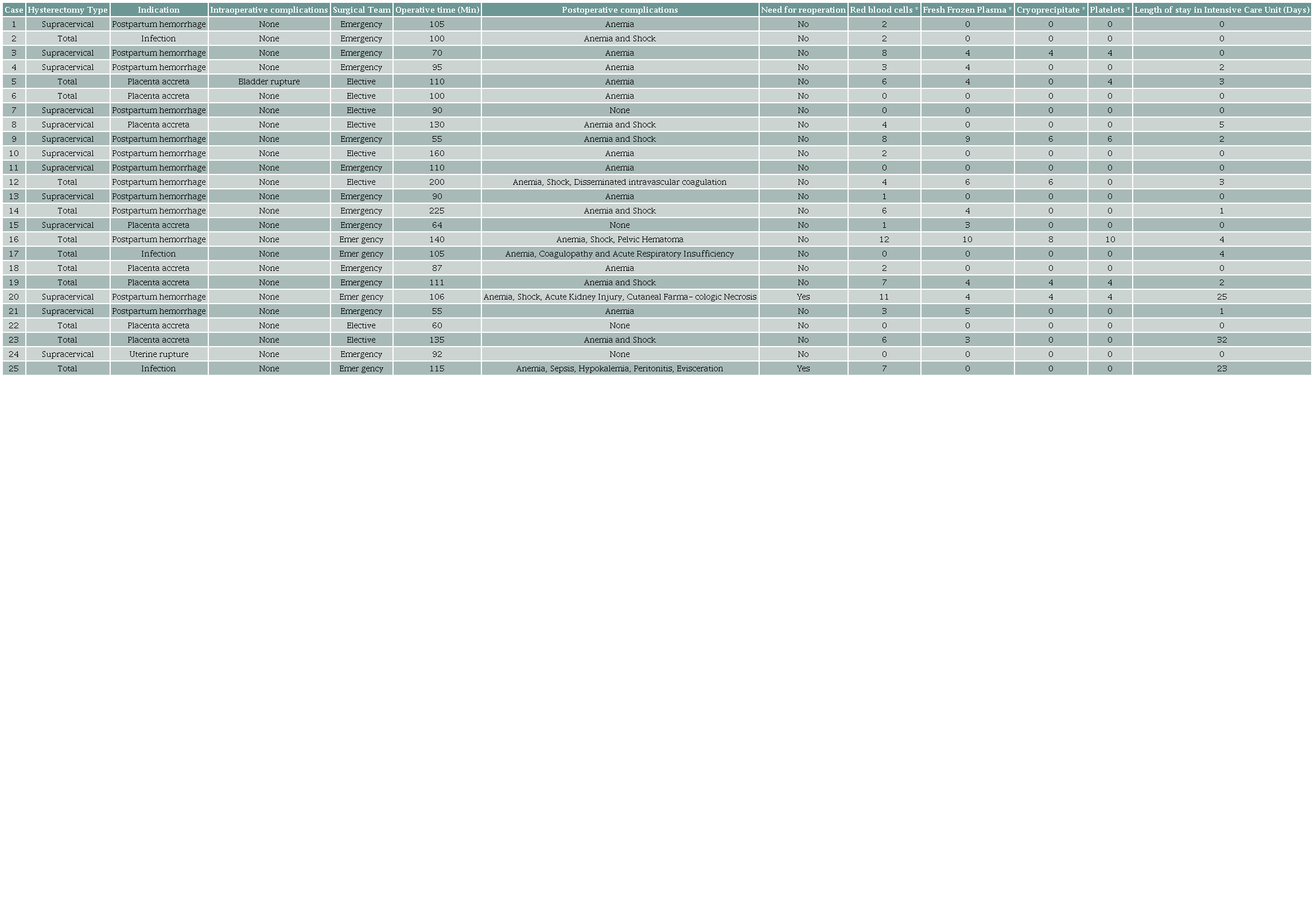
* Transfusion of (Units). Source: Authors.
Intraoperative and Postoperative Complications. Only one intraoperative complication was documented (4%), corresponding to a bladder injury during a total hysterectomy. Postoperative complications were common, with 21 cases of anemia and 9 cases of shock. Other complications included coagulopathy, disseminated intravascular coagulation, acute kidney injury, pharmacologic skin necrosis, pelvic hematoma, respiratory failure, sepsis, hypokalemia, peritonitis, and evisceration. Four patients (16%) had no recorded postoperative complications (see Table 1). When stratified by hysterectomy type, supracervical hysterectomies were associated mainly with anemia (10 cases) and shock (3 cases), along with isolated cases of acute kidney injury and skin necrosis. Among total hysterectomies, anemia was also frequent (11 cases), along with more severe complications such as shock (6 cases), disseminated intravascular coagulation, and sepsis.
Exploratory Analyses. No statistically significant associations were found between demographic characteristics and the occurrence of complications (Table 2). There was no significant difference in complication rates based on the mode of delivery (p = 0.171). However, patients who underwent vaginal delivery had a higher relative risk of developing shock (RR = 3.00; 95% CI: 1.56-5.77). The most frequently transfused blood product was red blood cells, with a median of 3 units. Median transfusion requirements for fresh frozen plasma, cryoprecipitate, and platelets were zero.
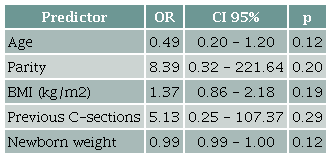
Source: Authors.
DISCUSSION
This study provides updated data on obstetric hysterectomy at a tertiary-level referral hospital in Chile over a three-year period. The incidence of obstetric hysterectomy decreased from 3.22 in 2021 to 1.81 per 1,000 live births in 2023, representing a 43.8% reduction. The most frequent indication was postpartum hemorrhage (52%), followed by placenta accreta spectrum disorders (32%), uterine infections (12%), and uterine rupture (4%). Supracervical hysterectomies were more frequently associated with postpartum hemorrhage (67%), while total hysterectomies were more often performed in cases of placenta accreta (46%). Complications, most of them postoperative, occurred in 84% of cases. Anemia and hemorrhagic shock were the most common complications. Only one intraoperative complication (bladder injury) was documented.
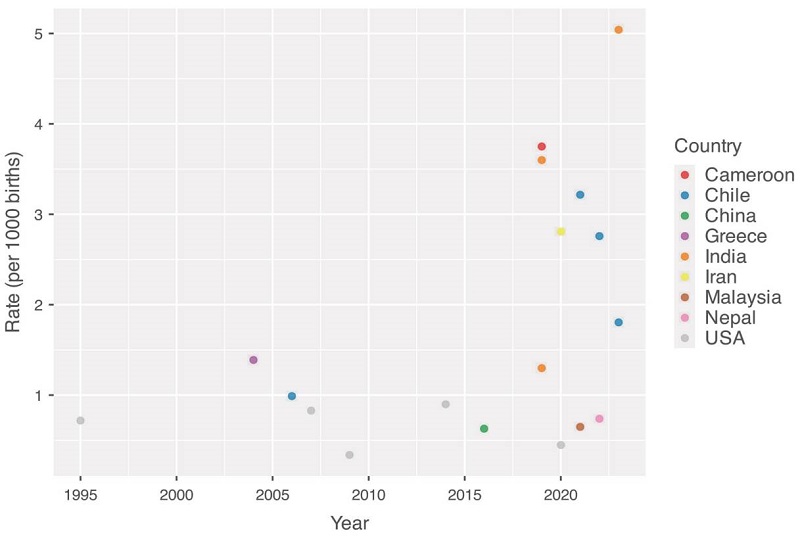
The incidence of obstetric hysterectomy observed in our study exceeds previously reported rates at the same institution. In 2006, a local study reported an incidence of 1 per 1,000 births, consistent with findings from high-income countries 5. While our current rate shows a downward trend, it remains higher than rates reported in many high-income countries where improved prenatal diagnosis and hemorrhage management protocols have reduced the need for hysterectomy, but lower than rates reported in low -and middle- income countries 2,5,10-19 (Figure 1). Our complication incidence (84%) is considerably higher than that reported in China with a postoperative complication incidence of 43.8% 19 and in Peru, where the cumultive incidence was 18.8% 20, but they are similar to repors form Mexico (96.9%) 21, Uruguay (83%) 22, and Colombia (76.3%) 23. It is important to highlight that the definition of "complication" varies across studies, which may influence reported frequencies. These discrepancies could be explained by the heterogeneity in access to specialized obstetric care, availability of blood products, and the capability to respond to obstetric emergencies.
Strengths and Limitations. A key strength of this study is its comprehensive inclusion of all obstetric hysterectomy cases at a national tertiary referral center over a defined three-year period. This ensures that the sample accurately reflects clinical practice in a high-complexity obstetric setting. The use of detailed institutional records provided robust data on surgical characteristics and outcomes. Nonetheless, several limitations must be acknowledged. First, the retrospective and descriptive design restricts the ability to assess causal relationships or evaluate intervention effectiveness. The small sample size limits statistical power and generalizability, and the lack of a control group precludes analysis of potential risks or protective factors. In addition, there is an inherent selection bias: as a tertiary referral center, our hospital receives more complex cases, potentially overestimating the rate of complications. Finally, classifying anemia as a postoperative complication may be misleading, as it can result from the underlying hemorrhage rather than the surgery itself, introducing a potential measurement bias.
CONCLUSIONS
Although its incidence is declining, obstetric hysterectomy remains associated with high morbidity. Strengthening prevention, early detection, and timely multidisciplinary care is essential. Further prospective, multicenter studies are needed to inform strategies designed to improve maternal outcomes.
REFERENCES
Kallianidis A, Rijntjes D, Brobbel C, Dekkers O, Bloemenkamp K, van den Akker T. Incidence, Indications, Risk Factors, and Outcomes of Emergency Peripartum Hysterectomy Worldwide: A Systematic Review and Meta-analysis. Obstet Gynecol. 2023;141(1):35-48. http://www.doi.org/10.1097/AOG.0000000000005022.
Daskalakis G, Anastasakis E, Papantoniou N, Mesogitis S, Theodora M, Antsaklis A. Emergency obstetric hysterectomy. Acta Obstet Gynecol Scand. 2007;86(2):223-7. http://www.doi.org/10.1080/00016340601088448.
Hellstern P, Haubelt H. Indications for plasma in massive transfusion. Thromb Res. 2002;107 Suppl 1:S19-22. http://www.doi.org/10.1016/s0049-3848(02)00147-0.
Mercier F, Van de Velde M. Major obstetric hemorrhage. Anesthesiol Clin. 2008;26(1):53-66, vi. http://www.doi.org/10.1016/j.anclin.2007.11.008.
Aguilera B, Sepúlveda K, Lattus J, Pantoja V, Moscoso F, Guichard C, et al. Histerectomía obstétrica de emergencia. Experiencia en el Hospital Santiago Oriente Dr. Luis Tisné Brousse. Revista de Obstetricia y Ginecología - Hospital Santiago Oriente Dr Luis Tisné Brousse. 2006;1:39-44.
van den Akker T, Brobbel C, Dekkers O, Bloemenkamp K. Prevalence, Indications, Risk Indicators, and Outcomes of Emergency Peripartum Hysterectomy Worldwide: A Systematic Review and Meta-analysis. Obstet Gynecol. 2016;128(6):1281-94. http://www.doi.org/10.1097/AOG.0000000000001736.
Nieto-Calvache A, Sanin-Blair J, Buitrago-Leal H, Benavides-Serralde J, Maya-Castro J, Rozo-Rangel A, et al. Colombian Consensus on the Treatment of Placenta Accreta Spectrum (PAS). Rev Colomb Obstet Ginecol. 2022;73(3):283-316. http://www.doi.org/10.18597/rcog.3877.
Coccolini F, Sartelli M, Sawyer R, Rasa K, Viaggi B, Abu-Zidan F, et al. Source control in emergency general surgery: WSES, GAIS, SIS-E, SIS-A guidelines. World J Emerg Surg. 2023;18(1):41. http://www.doi.org/10.1186/s13017-023-00509-4.
Schaap T, Bloemenkamp K, Deneux-Tharaux C, Knight M, Langhoff-Roos J, Sullivan E, et al. Defining definitions: a Delphi study to develop a core outcome set for conditions of severe maternal morbidity. BJOG. 2019;126(3):394-401. http://www.doi.org/10.1111/1471-0528.14833.
Anju, Sibia P, Kaur P. Emergency obstetric hysterectomy: A clinical study. International Journal of Clinical Obstetrics and Gynaecology. 2020;4(2):432-5. http://www.doi.org/10.33545/gynae.2020.v4.i2g.564.
Bateman B, Mhyre J, Callaghan W, Kuklina E. Peripartum hysterectomy in the United States: nationwide 14 year experience. Am J Obstet Gynecol. 2012;206(1):63. e1-8. http://www.doi.org/10.1016/j.ajog.2011.07.030.
Givens M, Einerson B, Allshouse A, Bruno A, Hammad I, Debbink M, et al. Trends in Unplanned Peripartum Hysterectomy in the United States, 2009-2020. Obstet Gynecol. 2022;139(3):449-51. http://www.doi.org/10.1097/AOG.0000000000004673.
Kalyankar V, Nimbalkar R, Kalyankar B, Gadappa S. A comprehensive study of obstetric hysterectomy. The New Indian Journal of OBGYN. 2023;10(1):88-92. http://www.doi.org/10.21276/obgyn.2023.10.1.15.
Lawson S, Chou B, Martin K, Ryan I, Eke A, Martin K. The association between race/ethnicity and peripartum hysterectomy and the risk of perioperative complications. Int J Gynaecol Obstet. 2020;151(1):57-66. Epub 20200806. http://www.doi.org/10.1002/ijgo.13304.
Mbakwa M, Tendongfor N, Ngunyi Y, Ngek E, Alemkia F, Egbe T. Indications and outcomes of emergency obstetric hysterectomy; a 5-year review at the Bafoussam Regional Hospital, Cameroon. BMC Pregnancy Childbirth. 2021;21(1). http://www.doi.org/10.1186/s12884-021-03797-3.
Nor A, Jagdeesh K, Mohd F, Kamraul A, Yusmadi A, Noraslawati R, et al. Peripartum hysterectomy clinical characteristics and outcomes- a hospital based retrospective audit study. Med J Malaysia. 2023;78(6):756-62.
Peivandi S, Peivandi S, Habibi A, Atarod Z, Moosazadeh M, Fallah S. Prevalence and Factors Associated with Peripartum Hysterectomy among Iranian Pregnant Women: A Retrospective Study. Ethiop J Health Sci. 2022;32(2):289-96. http://www.doi.org/10.4314/ejhs.v32i2.9.
Verma A, Sharma G, Kashyap M. A Retrospective Analysis of Emergency Obstetric Hysterectomy: A LifeSaving Intervention. Cureus. 2023;15(10):e46758. http://www.doi.org/10.7759/cureus.46758.
Zhang Y, Yan J, Han Q, Yang T, Cai L, Fu Y, et al. Emergency obstetric hysterectomy for life-threatening postpartum hemorrhage: A 12-year review. Medicine (Baltimore). 2017;96(45):e8443. http://www.doi.org/10.1097/MD.0000000000008443.
Ramírez Cabrera J, Cabrera Ramos S, Campos Siccha G, Peláez Chomba M, Poma Morales C. Histerectomía obstétrica en el Hospital San Bartolomé, Lima, 2003 - 2015. Revista Peruana de Ginecología y Obstetricia. 2017;63:27-33. https://doi.org/10.31403/rpgo.v63i1961
Lima C, Bernés S, Quiroz A, Solís M, Carrillo E, Barragán R. Comportamientos de las incidencias, indicaciones y complicaciones de histerectomías obstétricas en un hospital público mexicano. South Florida Journal of Health. 2024;5(2). http://www.doi.org/10.46981/sfjhv5n2-003.
Tolosa V, Lambruschini C, Santos D, Nozar F. Análisis de las histerectomías obstétricas en el Centro Hospitalario Pereira Rossell 2017-2022. Rev Med Urug (Montev). 2024;40(4). http://www.doi.org/10.29193/rmu.40.4.1.
Casas-Peña R, Pérez-Varela I, Chicangana-Figueroa G. Frecuencia, indicaciones y complicaciones de la histerectomía obstétrica en el Hospital Universitario San José de Popayán, 2006-2010: Estudio de cohorte. Rev Colomb Obstet Ginecol. 2013;64:121-5. https://doi.org/10.18597/rcog.119
How to cite this article:
AUTHOR’S CONTRIBUTIONS
FUNDING
Author notes
*Correspondence: Ejército 141. Santiago, Chile. sebastian.lavanderos@mail.udp.cl
Conflict of interest declaration