Artículos Reportes de Caso
Received: 05 October 2018
Corrected: 01 March 2019
Accepted: 12 March 2019
DOI: https://doi.org/10.30554/archmed.19.1.2618.2019
Abstract: Introduction: chronic non-bacterial osteomyelitis (CNO) is a non-infectious inflammatory of unknown etiology. Case description: ABA, female, 16 years old, was admitted with a pain in her left thigh. At the time, it was suspected to be caused by a tumor, and a bone scintigraphy was requested, which evidenced a focal area of increased uptake in the distal metadiaphyseal area of the left femur. A bone biopsy was performed, and its result was compatible with chronic osteomyelitis. The patient started taking pamidronate (withdrawn due to treatment failure) and methotrexate (subsequently suspended due to urticarial reaction). After some years of clinical stability, a new focal area of osteomyelitis appeared, in the distal right femur. The use of anti-TNF (infliximab) was chosen, resulting in an improvement of the algic state. Discussion: the diagnosis of CNO is made by process of elimination and is based on clinical, laboratorial, radiological, bacteriological and histological data. Non-hormonal anti-inflammatory and bisphosphonate drugs are recommended as initial therapy. Disease-modifying drugs, steroids and anti-TNFα have been used in severe and recurring cases. Conclusion: the authors present a CNO case with good response to anti-TNFα after treatment failure with bisphosphonates
Keywords: osteomyelitis, scintigraphy, methotrexate, infliximab.
Resumen: Introducción: la osteomielitis crónica no bacteriana (OMNB) es una enfermedad inflamatoria no infecciosa de etiología desconocida. Descripción del caso: ABA, mujer, 16 años, ingresó con dolor en muslo izquierdo. En ese momento, se sospechaba que era causado por un tumor, y se solicitó una gammagrafía ósea, que evidenció un área focal de captación aumentada en el área metadiafisaria distal del fémur izquierdo. Se realizó una biopsia de hueso, y su resultado fue compatible con osteomielitis crónica. El paciente comenzó a tomar pamidronato (retirado debido a una falla en el tratamiento) y metotrexato (posteriormente suspendido debido a una reacción urticarial). Después de algunos años de estabilidad clínica, apareció una nueva área focal de osteomielitis en el fémur derecho distal. Se eligió el uso de anti-TNF (infliximab), lo que resultó en una mejora del estado álgico. Discusión: el diagnóstico de CNO se realiza por proceso de eliminación y se basa en datos clínicos, de laboratorio, radiológicos, bacteriológicos e histológicos. Se recomiendan los fármacos antiinflamatorios y bifosfonatos no hormonales como terapia inicial. Se han usado fármacos modificadores de la enfermedad, esteroides y anti-TNFα en casos graves y recurrentes. Conclusión: los autores presentan un caso de CNO con buena respuesta a anti-TNFα después del fracaso del tratamiento con bisfosfonatos.
Palabras clave: osteomielitis, cintilografia, metotrexato, infliximab.
Introduction
Chronic non-bacterial osteomyelitis (CNO) is a non-infectious inflammatory of unknown etiology [1]. Its bone lesions can be unifocal of multifocal, initially osteolytic, and posteriorly sclerotic or hyperostotic [2]. The primary targets of the primary disease are children, in which it mainly attacks metaphyses of long bones, but may occur anywhere in the skeleton [1,3,4]. Skin, eyes and lungs may also be affected by inflammation [1,3]. Complications include vertebral fracture and severe bone lesions [2]. The first description of the disease was in 1972 by Giedion et al., such as symmetrical multifocal osseous lesions [5]. Subsequently, in new descriptions of the literature, the recurrent and chronic character of aseptic osteomyelitis was discovered. In the pathophysiology of the disease there are data demonstrating an imbalance of pro-inflammatory and anti-inflammatory interleukins, represented by IL-1β, IL-6, Anti-TNF and IL-10, respectively [5]. The discovery of the pathophysiology of the disease reinforces a hypothesis of possible autoinflammatory disease [4]. Current evidence shows that chronic aseptic osteomyelitis has a relevant genetic component. Mutations in LPIN2, PSTPIP2 and FBL1M1 genes have been found in mice and human studies [6].
CNO remains a diagnosis of exclusion. The presence of bone pain associated with edema, local heat, fractures, cutaneous lesions (including palmoplantar pustulosis, psoriasis and acne), peripheral arthritis, and discrete elevations of evidence of inflammatory activity suggest the diagnosis [7].
The first-line treatment remains the use of non-steroidal anti-inflammatory drugs [1,3,4,7]. For patients not responding to initial therapy, there are no comparative studies that provide a basis for a flowchart. The use of synthetic DMARDS such as methotrexate or sulfasalazine, use of anti-TNF or the use of bisphosphonates appear in reports as drugs with potential for disease control, as reported by Taddio et.al. and other authors [4,6,7]. There are recent reports of IL-1 antagonists, with variable results [7]. The objective with this report is to present a case to the literature regarding the response to the use of anti-TNF (infliximab) after failure with the use of anti-inflammatory drugs, methotrexate and bisphosphonates.
Case description
ABA, female, 16 years old, presented pre-existing bilateral hearing loss of unknown etiology, and asthma. The patient was admitted for examination due to a pain in her left thigh. Facing the need to rule out a neoplasia diagnosis, a bone scintigraphy was requested, which evidenced a focal area of increased uptake in the distal metadiaphyseal area of the left femur, with a highly aggressive osteoblastic lesion (Figure 1). A bone biopsy was performed, and its result evidenced medullary fibrosis, chronic inflammation with multinucleated of giant cells and areas fusocellular proliferation, compatible with chronic osteomyelitis. Cultivations of matter, serological investigation, autoantibodies and metabolic alterations were negative. In face of the clinical picture, the CNO diagnosis was performed, and treatment was initiated with pamidronate and prednisone, with partial improvement. Bisphosphonate was administered for 22 months (withdrawn due to treatment failure), and then, methotrexate was administered for 6 months, when it was suspended due to urticarial reaction. In January 2016, the patient presented a new pain episode, this time, in the right distal thigh and knee, which raised a suspicion of an additional focus of osteomyelitis during disease activity, which was confirmed by a new scintigraphy. In accordance with the reviewed literature and bearing in mind a refractory case to the usual therapy, it was decided to administer an anti-TNFα (infliximab), at a dose of 200mg per infusion (3.5 mg / kg), with applications every 8 weeks, with important clinical improvement in 4 months of evaluation until this moment, with recovery from the pain, besides standardization of inflammatory activity tests and new scintigraphic improvement. It is important to highlight that during the applications the patient did not present any side effects to the medication use, nor did she present infectious pictures in the period.
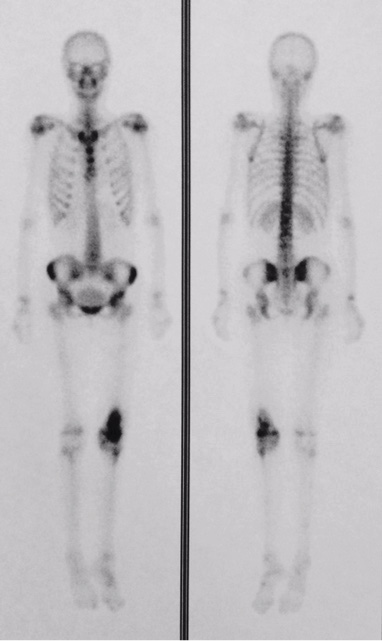
Figure 1
Bone scintigraphy – focal area of increased heterogeneous uptake in the distal metadiaphyseal area of the left femur with a highly aggressive osteoblastic lesion
Authors personal archives
Discussion
CNO is a rare inflammatory bone disease with intermittent course [8], characterized by recurring multifocal bone lesions [9]. The literature describes a female 5:1 predominance [5]. The most commonly affected age group is 8-12 years old, with peak incidence at 10 years old [9]. The diagnosis of CNO is made by process of elimination and is based on clinical, laboratorial, radiological, bacteriological and histological data [1]. Evidence of inflammatory activity is heightened during phases of disease activity, with normalization in periods of clinic remission [8]. Bone biopsy shows nonspecific inflammation, fibrotic or hyperostotic regeneration, and cultures are negative [10]. The scintigraphy reveals increased uptake in the affected areas, and helps perform diagnosis, which is done by process of elimination [8]. There are descriptions of association with other inflammatory diseases, such as Crhon’s disease, palmoplantar pustulosis, psoriasis, Sweet’s syndrome, among others [9]. Nonsteroidal anti-inflammatory and bisphosphonate drugs are recommended as initial treatment [1,3,7,10]. Bisphosphonates appear to be beneficial in reducing the expansion of the bone lesion due to the antiosteoclastic activity and its anti-inflammatory effect, which can contribute to pain control [9]. Disease-modifying drugs, steroids and anti-TNFα have been used in severe and recurring cases [1,3,7,10,11,12]. Despite reports of a variable response to the use of anti-TNF [11,12], in this case the clinical and laboratory response had been sustained to date, with about 4 months of use of the biological medication, corroborating the reports of clinical and image improvement with the use of anti-TNF.
Conclusion
The authors present a CNO case with good response to anti-TNFα after treatment failure with bisphosphonates and anti-inflammatory drugs.
Conflict of interest: none.
Source of funding: none
Literature cited
Beck C, Morbach H, Beer M, Stenze M, Tappe D, Gat- tenlohner S, et al. Chronic nonbacterial osteomyelitis in child: prospective follow-up during the first year of anti-inflammatory treatment. Arthritis Res Ther 2010; 12(2):R74. DOI: 10.1186/ar2992.
Jansson AF, Müller TH, Gliera L, Ankerst DP, Win- tergerst U, Belohradsky BH, et al. Clinical score for nonbacterial osteitis in children and adults.Arthritis Rheum 2009; 60(4):1152-9. DOI: 10.1002/ art.24402.
Girschick HJ, Zimmer C, Klaus G, Darge K, Dick A, Morbach H. Chronic recurrent multifocal os- teomyelitis: what is it and how should it be treated?Nat Clin Pract Rheumatol 2007; 3:733-738. DOI: 10.1038/ncprheum0653.
Taddio A, Ferrara G, Insalaco A, Pardeo M, Gregori M, Finetti M, et al. Dealing with Chronic Non-Bacterial Osteomyelitis: a practical approach.Pediatr Rheumatol Online J 2017; 15(1):87. DOI:10.1186/ s12969-017-0216-7.
Giedion A, Holthusen W, Masel LF, Vischer D. Sub- acute and chronic “symmetrical” osteomyelitis. Ann Radiol (Paris) 1972; 15(3):329-42.
Cox AJ, Zhao Y, Ferguson PJ. Chronic RecurrentMultifocal Osteomyelitis and Related Diseases–Update on Pathogenesis.Curr Rheumatol Rep 2017; 19:18. DOI:10.1007/s11926-017-0645-9
Hofmann SR, Kapplusch F, Girschick HJ, Morbach H, Pablik J, Ferguson PJ, et al. Chronic Recurrent Multifocal Osteomyelitis (CRMO): Presentation, Pathogenesis, and Treatment.Curr Osteoporos Rep. 2017; 15(6):542-54. DOI:10.1007/s11914-017-0405-9.
Paim LB, Liphaus BL, Rocha AC, Castellanos ALZ, Silva CAA. Osteomielite crônica multifocal recorrente da mandibular: relato de 3 casos. J Pediatr (Rio J.) 2003; 79(5):467-70. DOI: 10.1590/ S0021-75572003000500016.
Ferraria N, Marques JG, Ramos F, Lopes G, Fonseca JE, Neves MC. Osteomielite crônica multifocal recorrente: série de quatro casos clínicos tratados com bifosfonados. Acta Reumatol Port 2014; 39:38-45.
Jansson A, Renner ED, Ramser J, Mayer A, Haban M, Meindl A, et al. Classification of Non-Bacterial Osteitis. Reumatology 2007; 46:154-160. DOI: 10.1093/rheumatology/kel190.
Girschick H, Finetti M, Orlando F, Schalm S, Insalaco A, Ganser G, et al. The multifaceted presentation of chronic recurrent multifocal osteomyelitis: a series of 486 cases from the Eurofever international registry.Rheumatology (Oxford) 2018; DOI: 10.1093/rheumatology/key058.
Moussa T, Bhat V, Kini V, Fathalla BM. Clinical and genetic association, radiological findings and response to biological therapy in seven children from Qatar with non-bacterial osteomyelitis. Int J Rheum Dis 2017; 20(9):1286-1296. DOI: 10.1111/1756-185X.12940.
Alternative link
http://revistasum.umanizales.edu.co/ojs/index.php/archivosmedicina/article/view/2618 (html)
