Monográfico
Monitoring the health environment in Ukrainian primary schools
Monitoring the health environment in Ukrainian primary schools
Monitoring the health environment in Ukrainian primary schools
Revista Interuniversitaria de Formación del Profesorado, vol. 34, núm. 1, pp. 115-132, 2020
Universidad de Zaragoza
Resumen: El artículo describe los resultados del monitoreo del ambiente de salud en las escuelas primarias de la región de Jarkiv (Ucrania), realizado en 2017 y 2018. En el estudio respondieron a unas preguntas las directores de 77 escuelas primarias, 42 inspectores de departamentos de educación (el número de distritos administrativos en la región de Jarkiv), 462 maestros y 847 padres de los niños. Mediante un modelo cualitativo construido sobre esta base, se evaluó la implementación del ambiente de salud en las escuelas. El modelo se construyó teniendo en cuenta aspectos organizativos, gerenciales, médicos, metodológicos, pedagógicos y familiares. Los resultados del monitoreo indican que los directores califican el estado del ambiente de salud en las escuelas primarias ligeramente más alto que los funcionarios. Al mismo tiempo, el indicador general se encuentra en los niveles promedio y suficiente. Con el desarrollo general del ambiente de salud, el análisis reveló un deterioro en el desarrollo de los aspectos familiares y pedagógicos (participación de los padres en eventos de salud, trabajo de la escuela de padres jóvenes, etc.). La disminución en el nivel de cooperación con los padres también se confirma por los resultados de las respuestas de los padres. El número más pequeño de participantes en el estudio caracterizó el sistema de monitoreo del ambiente de salud en las escuelas primarias de alto nivel. Reafirmamos la importancia de involucrar a todos los interesados en el contexto de la planificación, implementación, monitoreo y gestión del ambiente de salud.
Palabras clave: Monitoreo, Modelo cualitativo, Ambiente de salud, Escuelas primarias.
Abstract: The article describes the results of monitoring the health environment in primary schools in the Kharkiv region (Ukraine), which was carried out in 2017 and 2018. In the study, school principals of 77 primary schools, 42 (the number of administrative districts in the Kharkiv region) inspectors of educational departments, 462 teachers, and 847 parents of children answered the questions. Through a qualitative model built on this basis, the implementation of the health environment in the primary schools was evaluated. The model was built taking into account organizational, managerial, medical, methodological, pedagogical, and family aspects. Monitoring results indicate that school principals rate the state of the health environment in the primary schools slightly higher than officials. At the same time, the general indicator is at medium and sufficient levels. Together with the general development of the health environment, the analysis revealed a decrease in the development of family and pedagogical aspects (parental involvement in health events, school work of young parents, etc.). The decrease in the level of cooperation with parents is also confirmed by the results of the parents' responses. The smallest number of participants in the study characterized the health environment monitoring system in primary schools at a high-level. We reaffirm the importance of involving all stakeholders in the context of planning, implementation, monitoring, and management of the health environment.
Keywords: Monitoring, Qualitative model, Health environment, Primary schools.
Introduction
The health of the younger generation is an indicator of the health of the nation in the future. Public health is considered the main criterion for the prosperity of any country, and the problem of creating a safe health educational environment is a matter of the utmost importance. In accordance with the Dakar Framework for Action, in the World Educational Forum, participants confirmed a framework of actions aimed at creating a safe and psychologically comfortable learning environment. This framework was named FRESH (Focusing Resources on Effective School Health).
The state of the art in the field is full of theoretical and practical underpinnings. Schools are recognized as key settings for health promotion (Rowling & Jeffreys, 2000). Good monitoring and evaluation ensures adequate and optimal implementation of school health services (Chidiebere et al., 2016). Scientists from various fields consider the problem of the creation of a safe health education environment for primary schools and monitoring its effectiveness: monitoring the medical (Calmeiro, 2019;
Jourdan et al., 2018; Wahl, 2017) and sanitary (Chavan & Chavan, 2018; Madureira et al., 2015) provision of the educational environment; monitoring of school physical activity policies (Jordán, et al., 2017; Kohl et al., 2012; Taylor et al., 2011); remote health monitoring technologies (Toscos, Connelly, & Rogers, 2012) programs to measure the child's holistic development (Seema, 2019); monitoring as a primary information system in education (Lunyachek, 2011) etc.
It is well-known that healthier children are better learners (Basch, 2011), i.e. a favorable learning environment would enhance educational performance. Many aspects of educational monitoring are sufficiently developed at the theoretical level and the practical experience of planning and implementation of monitoring at educational institutions of various levels. An analysis of the scientific works on the preservation and development of the components of children's health shows that the problem is timely relevant and reflected in the research. However, researchers are mostly limited to assessing partial indicators of a safe, health-friendly educational environment. The process of filling monitoring systems with criteria and its systematization (Booth & Samdal, 1997) received little attention.
The main objective of the article is to substantiate the immense value of the process of filling and systematization of the health environment in primary schools, development and implementation of complex monitoring research at the level of the region and at the level of the school.
In Ukraine, the implementation of the state policy for preserving the health of the younger generation is based on the United Nations Concept on Sustainable Human Development as a program of action for the 21st century, and is reflected in such state documents as: the Constitution of Ukraine, the Law of Ukraine ―On Education‖, The Code of Civil Protection of Ukraine, the Concept of education in the field of ―Safety of life and human activity‖, etc.
The increase in child traumatism (The State Emergency Service of Ukraine, 2017) and the deterioration of children health sets the the task for educational institutions to work systematically and comprehensively for the creation of a healthier environment, education of young children a culture of health and safety, and the development of mechanisms for monitoring the development of the environment parameters.
Based on the Code of Safe Education, the main tasks of the creation of the health environment monitoring are: identifying factors that impede the safety of participants in the educational process; developing a system of agreed views and perceptions of educators, psychologists, and parents on the health educational environment; justification of the conditions of organization of the health educational environment and requirements (criteria) for its effective implementation (Tsyuman & Boichuk, 2018). Regulatory documents emphasize that the condition of holistic development of a school-aged child is the use of health-saving and health-forming
technologies in educational institutions. These approaches are implemented in a complex way through the creation of safe development environment, ecological and health science education, full medical care, safe nutrition, optimization of motor activity, formation of value attitude to one's own health and motivation for healthy lifestyle.
Planning, implementation, monitoring, management, and collaboration are the keys to the success of the developed health environment (Hens et al., 2010). Each of these elements is related to the other and has a corresponding impact. In the presented article, the proposed monitoring system is developed in collaboration with all stakeholders. The system influences the planning, management and implementation of activities to create the health environment in the primary schools.
Method
Design By analyzing the approaches of scientists and practitioners to the systems, indicators, components, and performance criteria for the safe health environment, the model of the health environment was developed. It takes into account the factors which influence the deterioration of the health of young children: the impact of adverse environmental factors, overheating, hypodynamia, depression, forced postures, the impact of closed spaces, and excessive obsession with methods of intellectual development etc. An important condition for the conscious implementation of the safe educational environment in a school is the formation of knowledge on the identified issue, which goes through the following stages: clarification of children's perceptions of safety rules, i.e. the personal experience; expansion of elementary children's ideas, accumulation of new knowledge about safety rules; consolidation of the acquired knowledge and formation of conscious attitude to observance of safety rules; developing a sense of responsibility; development of a school-aged child's sense of control and self-control.
Taking into account reviewed scientific sources (Booth & Samdal, 1997; Tsyuman & Boichuk, 2018), we developed criteria for the system of work of a primary school for the creation of the safe educational environment.
Organizational and managerial aspect:
- health and safety planning;
- infrastructure development;
- establishment of information and an organizational system;
- examination of the state of educational activities in the field of life and health, protection and prevention of all types of childhood traumas;
- health and safety visualization;
- control and analytical activities;
- organizing and conducting events such as Health and Safety Weeks, etc.
Medical aspect:
- sanitary and hygienic condition of a school;
- rational nutrition;
- analysis of the incidence;
- prevention of morbidity;
- health and rational daily regime control;
- medical and pedagogical control over the organization of physical activities, etc.
Pedagogical aspect:
- organization of safe motor activity of children;
- physical and health measures with regard to safety rules;
- compliance with program requirements;
- observation of child development milestones, diagnostic, correction, and development;
- preparation of training programs for individual work with children;
- cooperation with parents, assistance in maintaining a favorable psychological climate.
Methodical aspect:
- actualization of health and safety problems;
- creation of optimal conditions for organization of work on health and safety;
- constant enrichment of the development and game environment;
- methodological support of teachers in order to improve their professional skills in accordance with the requirements of modern education;
- space creation for effective interaction of methodical service and a teacher, teacher and child, teacher and parents, methodical service and parents;
- conducting methodological measures on health and safety, generalization of effective pedagogical experience;
- use of innovative methods and technologies;
- development of synopsis and scenarios of measures aimed at the protection of life and health, safety of life, etc.
Family aspect:
- work with parents' associations;
- actualization of the problem among parents;
- young parents' school;
- participation of parents in dedicated events;
- parents meetings;
- conducting interviews, consultations, and questionnaires;
- exhibitions of creative works of children and their parents, etc. This list is not exhaustive.
To carry out effective work with children, it is necessary to carry out systematic work with teachers and parents, which face the following tasks: create safe conditions for the life of the child, develop child’s ability to
anticipate the consequences of his actions, develop child’s skills of action during emergency situations.
At the level of a school, the monitoring suggests the following: the creation of a single information space; identifying the level and dynamics of the functioning of the health education environment by certain indicators; identifying factors that have a positive or negative impact on children's health; identifying the degree of implementation of the factors which influence on responsible attitude of children to their own health; forming a culture of health and promoting a healthy lifestyle; identification of the state and dynamics of the educational system; studying the effectiveness of interaction with parents and the government; predicting the development and effectiveness of a safe and health-conscious educational environment.
Qualimetry provides the possibility of measuring any qualitative phenomena based on the use of factor-criterion models and provides a comprehensive assessment of quality through a set of indicators using the appropriate mathematical model. The advantage of qualimetric technology is that its use makes it possible to measure results that capture a purpose at a particular point in time. The selection of identified factors is based on the expert (practitioners) evaluation. Information processing is performed on the basis of rapid analysis with the use of pair wise comparison and ranking technology.
When comparing qualimetry results, it is necessary to take into consideration dynamics of the indicators (increase or decrease) for a certain time rather than quantitative indicators per se. Dynamics characterizes the quality of education. Using the qualimetric approach, one of the most important principles of qualimetry is implemented: taking into account the relationship between complex and simple properties of an object by creating a standard, an appropriate model of the ideal state of an object. Decomposition of the object properties occurs by selecting the basic parameters of its development, factors and criteria for identifying factors. Thus, it creates a toolkit for assessing the condition of the object, called a qualimetric standard, which allows us to quantify how the object achieves a certain state of development.
In the first stage of the study, expert evaluation was carried out using the developed qualimetric models. School administration (Self-ranking) and inspectors (Ranking) acted as experts. In the second stage, the monitoring system was supplemented by the results of parents and teachers answers. These findings allow us to extend the continuous monitoring procedures, as well as to include into the monitoring direct contractors (teachers) and customers (parents) of the learning process.
Measures
When constructing a qualimetric model of health-saving educational environment, we rely on the following algorithm: determination of directions of activity – formation of groups by the number of directions – ranking one of the directions – generalization of indicators (components of activity) in a certain direction – determination of the importance of the directions.
Within the framework of the qualimetric model construction, experts who evaluate the directions according to their importance were involved: the highest score was given to the most important direction, the maximum rank of which corresponds to the number of the directions. For five directions, the maximum score of 5 is assigned to the most important direction.
The weighting coefficients are calculated as follows:
- sum of each row of coefficients;
- the total amount (column sum ∑);
- the weight is calculated as the ratio of the line amount to the total;
- the weighting coefficients are adjusted so that the sum is equal to one.
The calculation for each direction is done automatically by formulas, for example, in MS Excel:
- the product of the weight of the component × the degree of the components;
- the sum of products within each direction (∑ (weight of component × degree of the components));
- the product of the sum of each direction and the weight of the direction (weight of the direction × ∑ (weight of the component × degree of the components)).
The degree of the components for each indicator is rated.
Procedure
In 2017 and 2018, monitoring was carried out in the Kharkiv (Ukraine) region, the purpose of which was to obtain information on the state of health environment development in primary schools using the following indicators: condition of the territory and premises, compliance with sanitary and hygiene requirements, compliance with child safety requirements, system of internal monitoring, etc. Children aged 6–10 years study in the primary schools in Ukraine. The study was conducted as a part of a general regional monitoring of the quality of education (Kapustin et al., 2018).
In the first phase of the study, school principals of 77 primary schools (random sampling) in the Kharkiv region were involved. The number of the primary schools accounted for approximately 10% of the total number of such schools in the region. In accordance with the number of administrative districts in the Kharkiv region, 42 inspectors of educational departments that control the direction of health development in schools participated in the study. Respondents were asked to evaluate the degree of the health environment development in the primary schools in 2017 and 2018.
As part of this monitoring phase, indicators of a system for creating a
safe health education environment were being investigated. For example, indicators of dedicated infrastructure (sports and music classrooms) were ranked. According to the Indicative List the equipment should include equipment for physical education (gymnastic wall / ladder, cubes for exercises with balance and jumps, ladder with hooks, ladder rope suspended, gymnastic board, ribbed board, benches for gymnastics, cubes for exercises with balancers, logs, hinged targets / boards with targets, arches for lifting, rolling, soft sports module, fences, barriers, "mazes" with elements of various sizes, pit with sand for long and height jumps, ropes, gymnastic poles / rails, cloth tunnel, toys, games, game equipment for the development of movements, bolboka, kletsekid, serso, skittles, "Darts", board sports-motor games, dry pool with balls, skipping ropes).
Teachers of young children – 462 persons from 77 primary schools of Kharkiv region participated in the parallel evaluation. The study also included parents of young children – 847 persons.
We obtained data on the age of the parents. All the samples of the study are representative. The characteristics of the units from which they are formed are subject to the normal distribution law and can represent the opinion of the general population as a whole within 5% of the study error. Cronbach alpha is (> 0.8).
Results
Partial results of the qualitative modeling of the health environment are presented in Table 1 (in the model, two components of each direction are presented as an example).
We can compare the analysis of activities by defined aspects according to the answers of the schools' staff (Self-rating) and the examiners (Rating) (Fig. 1). Fig. 2 shows the percentage of the availability of equipment in sports and music classrooms according to the Ukrainian Indicative List for the Development of Motor Activity (Indicative List).
Out of the 77 schools, most (58,44%) are provided with 70–79% of equipment for sports and music classrooms according to the Indicative List. At the same time, a high percentage of providing the necessary equipment (from 80% and more) was found in 32,46% of the schools. Low level of providing the appropriate equipment (from 0% to 39%) was identified in 2,59% of the schools. It should be noted that almost every sixth school participated in the study is provided with 50–69% of equipment according to the Indicative List.


Figure 1
Histogram for comparing Self-rating and Rating in accordance with results of the health environment monitoring

Figure 2
Distribution of the number of the schools by the percentage of the availability of equipment in sports and music classrooms
In 2018, the percentage of the primary schools equipped with sports and music facilities in the ranges of 70%–79% and 80%–100% increased by 1,3%–2,6%.
Table 2 shows the study results regarding some other components of the health environment.
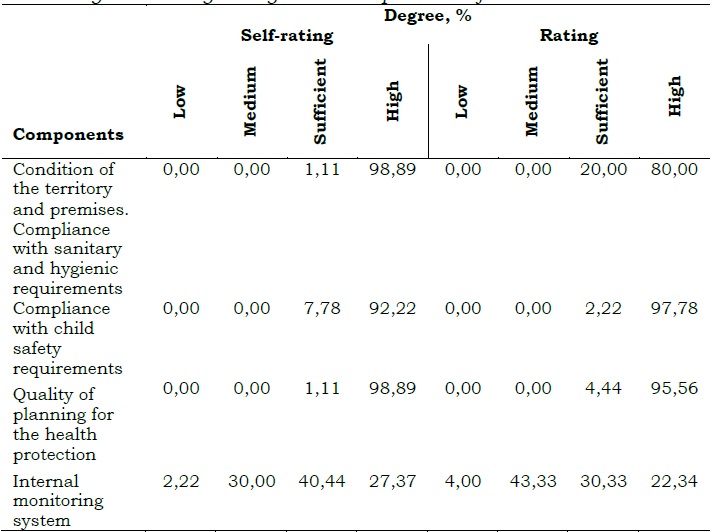
Managers of the schools described (Self-rating) all indicators mostly at high levels. At a high level, most school principals (98,89%) rated the condition of the territory and premises, compliance with sanitary and hygiene requirements and quality of planning; more than 90% – compliance with child safety requirements (92,22%). The smallest number of respondents (27,37%) gave a high-level assessment to the internal monitoring system. At the same time, a significant proportion of respondents described this indicator at low and medium levels. 7,78% of managers at a sufficient level described the compliance with child safety requirements, 40,44% – system of internal monitoring. A small number of the study participants rated the territory and premises as satisfactory, compliance with sanitary and hygienic requirements (1,11%) and the quality planning for the health protection (1,11%).
Responsible persons (inspectors) for the health education of young children in the district evaluated (Rating) almost all indicators (except the internal monitoring system) involved in the study at sufficient and high levels. They rated at a high level the condition of the territory and premises and compliance with sanitary and hygienic requirements; more than 95% – compliance with child safety requirements (97,78%) and quality of planning for the health protection (95,56%). Small number of the participants
(22,34%) characterized the system of internal monitoring at a high level. According to the responses of the inspectors, activities on the internal monitoring system (43,33%), the quality of planning of activities for the health protection (4,44%), and compliance with the requirements of child safety (2,22%) were rated at a sufficient level.
Similar to 2017, in 2018, the vast majority of school principals rated all components at a high level, except for the internal monitoring system. Compared to 2017, the number of school principals who gave such an assessment of compliance with child safety requirements (by 2,53%), the quality of planning for the health protection (by 10,23%), and the system of internal monitoring (by 15,22%) increased. At the same time, the number of respondents who characterized at a high level the condition of the territory and premises as well as compliance with sanitary and hygienic requirements at a high level decreased by 1,11%.
According to the information provided by the participants of the monitoring, it was found out that the majority (58%) of the schools are provided with equipment for sports and music classrooms within the range of 70–79%. 32% of the primary schools are provided with educational toys according to the Indicative List within the range of 80–100%. Managers of all educational institutions described the performance of the institution at sufficient and high levels. At the same time, most school principals (98%) rated the condition of the territory and premises as well as compliance with sanitary and hygienic requirements, and the quality of planning for the health protection at a high level.
Compared to 2017, the number of the managers who rated the compliance with child safety requirements at a high level increased by 3%, the quality of planning for the health protection increased by 10%, and the internal monitoring system increased by 15%. At the same time, the number of respondents who characterized the condition of the territory and premises and their compliance with sanitary and hygienic requirements at a high level decreased by 1%.
Inspectors rated almost all indicators of the activity of the primary schools at sufficient and high levels. They rated the condition of the territory and premises, and the compliance with sanitary and hygienic requirements at a high level. However, both the school principals and the inspectors characterized the internal monitoring at a high level at only 27% and 22% of the schools respectively.
The answers of the teachers showed that, in comparison with parents’ opinion, they were more fully satisfied with the attitude of teachers to children (by 10,17%), the activities of teachers (by 1,56%), the activities of the administration (by 12,19%), ensuring the safety at the schools (by 15.32%), and the organization of movement activity during the day (by 10,29%). Among teachers, there were also more persons who gave preference in the education on the child's social adaptation (by 18,17%), the ability to communicate (by 9,77%), physical development (by 13,92%), and the ability to manage their behavior (by 12,95%).
The majority of parents are satisfied with the activities of educators on the children health protection (on the average 76,60%), the attitude of teachers to the child (76,23%), the organization of physical activity during the day (66,89%), the activities of the administration of the primary schools (65,97 %), ensuring the safety at the schools (62,84%), the implementation of an individual approach to the child (60,20%), conditions for the development of the child (59,77%). But on the average 57,12% of parents rated the organization of their health education and their lack of cooperation activities on the issue at a low level. A small number of parents interviewed are dissatisfied with the administration's activities (2,70%), the implementation of an individual approach to the child (3,26%) and the conditions of the child's development in the schools (2,21%).
Discussion
For Ukraine, the problem of health care for young children is particularly urgent, due to the presence of a negative medical and demographic situation and an unfavorable trend in children injury rates. The study results show that the situation is not nearly as dire as it might appear, but primary schools should endeavor to uphold the high standards in this area. We revealed an overall high level rating of the monitoring indicators. The results are approximately equal, both in terms of self- ranking and ranking. The lowest is the internal monitoring score. Regarding this issue, we could discern the note of urgency in the answers of the study participants. Taking into account this fact, as well as taking into consideration the parents' specific view of building a monitoring system of the health environment in Ukrainian primary schools, we confirmed the importance of involving all stakeholders in the monitoring procedures.
An important characteristic of this study was the attraction of officials, administration, teachers, and parents. The practicability of involving officials and school principals in the study has been confirmed by various studies (Barjasteh, Rezaee, & Zibaee, 2016; Bezerra et al., 2017). Our study confirmed that in order to have a healthy and safe school, proper management and strict monitoring are required (Barjasteh, Rezaee, & Zibaee, 2016). The importance of involving parents in forming a healthy mindset is repeatedly mentioned in the scientific literature (Cachón-Zagalaz et al., 2019; Toscos, et al., 2012; Yu & Li, 2017). Schools, families and communities should work in partnership to reduce the gradient in health, well-being, and resilience of children and young people that are considered a priority among public health objectives (Marmot et al., 2010). The complex combination of feedback from all participants in the learning process (de Villiers et al., 2012) showed its effectiveness.
According to the obtained results, the overall score of the school principals' own work is at a high level – 0,79 in 2017 and 0,75 in 2018. The pinion of officials in 2017 was close to the self-ranking of the administration and was sufficient. In 2018, officials believed that the health environment in the primary schools in the Kharkiv region had dropped to a middle level.
Monitoring of the school system's indicators for creating a safe health educational environment involving parents showed that in comparative periods, the number of parents ranked the family aspect of the system at a low level (discussing the problem among parents, consultations, questionnaires, etc.) increased; the medical aspect of the environment (sanitary and hygienic condition of the schools, rational nutrition; prevention of morbidity; health and rational daily regime control, etc.) increased. However, the number of parents who appreciate this aspect of activity at a high level decreased by 3%. At the same time, taking into account the probabilistic error of the study, these results can be neglected. These indicia should be given further detailed treatment.
The analysis of indicators of the created qualimetric model, together with the general development of the health environment, the analysis revealed a decrease in the development of family and pedagogical aspects (work of parents' associations, participation of parents in health activities and events, work of young parents' schools, etc.), despite the fact that more than a half of the respondents (54%) aged between 30 and 40 years old and 37% of them were under 30 and had one child, which means a little experience in fostering a child's health culture. The decrease in the level of cooperation with parents is also confirmed by the results from the parents’ answers, in which the majority of parents (57,12%) indicated that their education on protection of the health of their child is low and there is the lack of cooperation in these questions. Greater inclusion of parents in the monitoring process would invigorate the creation of the health educational environment.
The smallest number of the participants in the study (22,34%) characterized the system of internal monitoring at a high level. These results indicate the need for the development and implementation at the regional level of educational measures for training all stakeholders on the issues of monitoring procedures and interpretation of the obtained results. The need to work together should stem from the nature of such an interaction.
The analysis of the components of the pedagogical aspect (organization of safe motor activity of children; physical and health measures with regard to safety rules; cooperation with parents, assistance in maintaining a favorable psychological climate, etc.) according to the parents’ point of view showed a general decrease by 16% at a high level. This point needs greater elaboration in subsequent monitoring procedures. Positive dynamics were observed in the monitoring of the methodological aspect.
Thus, we see that the results of the monitoring have some differences in which school principals and inspectors on the one hand, teachers and parents on the other, are the experts. Although the checkpoint list may differ from known studies (Booth & Samdal, 1997), an important feature is the adaptability of the system to new requirements. The formative findings of this study contribute to the methodology of creating the monitoring systems. With the involvement of all stakeholders, compliance with this criterion can be achieved. Also, we supplemented various national studies (Barjasteh et al., 2016; Bezerra et al., 2017; Hens et al., 2010; Wedderkopp et al., 2012, etc.) with the data from Ukraine.
Conclusion
In the study, a qualitative model for the health environment monitoring in Ukrainian primary schools was developed. The model made it possible to monitor the indicators (components of the directions) of the health environment through the implementation of a quality planning system, through the use of safe equipment and taking into account the physiological characteristics of children, through the implementation of effective forms and methods of an educational preventive work.
At the local level, we resolved the difficulty that lies in determining what is acceptable as evidence in the context of ―what are the most appropriate methods for collecting this evidence‖ (Rowling & Jeffreys, 2000). The developed internal monitoring system made it possible to determine the level of organization of safe motor activity of children, physical and health measures with regard to safety rules, infrastructure development of a health-friendly educational environment, etc.
The developed system reflects the multi-variant and dynamic nature of the processes involved (Rowling, & Jeffreys, 2000). Summarizing the salient points of the study, we affirmed the need to develop a comprehensive monitoring system as evidenced by the analysis of internal and external factors according to the study, and to increase the level of a family education through the education of parents on maintaining children's health and actively engaging them in the educational process.
In the organization of educational work on the safety of life of children, it is advisable to focus mainly on the fact that the maximum effect can be achieved when implementing a single strategy in the activities of administrative, pedagogical, and parents groups.
The implementation of a comprehensive internal monitoring system requires the implementation of the following algorithm for the development of a qualimetric model:
· Assessment of the quality of the health educational environment.
· Determination of all types of activities.
· Formation of groups according to the number of directions.
· Identifying components that can be evaluated in the each area.
· Generalization for each group of indicators (components of activities) in a particular direction.
· Determination of the importance of activities.
· Determination of the indicators weight within each direction.
· Comparison of results obtained from different expert groups; improvement of the monitoring system.
· After each evaluation, planning of future appropriate actions to develop a health-friendly educational environment.
Taking into account the views of scientists, we supplemented the toolkit of monitoring the quality of education with the technology of monitoring and supplementing indicators of the health educational environment. The educational environment is revealed through the system of principles for children's development organization and is a part of the general environment.
The study allows us to analyze the opinion of officials, administration, educators, and parents on particular health care issues that are mainly revealed at a high level. The investigated schools remain problematic issues – an educational work with parents on children's health care, a reduction in the attention of the schools to pedagogical aspect, and the organization of an internal monitoring system. In our view, achieving a "medium" and a "sufficient" level is not a marker of the success of the appropriate measures, especially when it concerns children. To achieve a "high" level, schools require a broader and more adaptive implementation of monitoring procedures and the appropriate corrective action.
References
Barjasteh, F., Rezaee, Z., & Zibaee, Z. (2016). Comparison of the environmental health and safety status of governmental and non- governmental primary schools in Kashmar in 2015-2016. Journal of Torbat Heydariyeh University of Medical Sciences, 4(3), 38–47.
Basch, C. E. (2011). Healthier students are better learners: high-quality, strategically planned, and effectively coordinated school health programs must be a fundamental mission of schools to help close the achievement gap. Journal of School Health, 81(10), 650–662. https://doi.org/10.1111/j.1746-1561.2011.00640.x
Bezerra, M. D. A., Carvalho, E. F. D., Oliveira, J. S., & Leal, V. S. (2017). Health and nutrition in public and private schools in the city of Recife. Revista Brasileira de Saúde Materno Infantil, 17(1), 191–200. http://dx.doi.org/10.1590/1806-930420170001000011
Booth, M. L. & Samdal, O. (1997). Health–promoting schools in Australia: models and measurement. Australian and New Zealand journal of public health, 21(4), 365–370. https://doi.org/10.1111/j.1467- 842X.1997.tb01716.x
Cachón-Zagalaz, J., Sánchez-Zafra, M., Lara-Sánchez, A., Zagalaz-Sánchez, M. L., & Shmatkov, D. (2019). Study on the relationship between physical activity and the development of professional competence: Findings from a study in Ukraine. Journal of Human Sport and Exercise, in press. doi: https://doi.org/10.14198/jhse.2020.153.10
Calmeiro, L., & Pereira, C. (2019). Healthy lifestyles and body mass index as correlates of body image dissatisfaction in primary schoolchildren. Acta Gymnica, 49(4), 189–196. https://doi.org/10.5507/ag.2019.016
Chavan, V. M., & Chavan, G. M. (2018). School health performance score: a comparative study between rural and urban school performance. International Journal of Community Medicine and Public Health, 5(6), 2421–2424. http://dx.doi.org/10.18203/2394-6040.ijcmph20182170/
Chidiebere, O. D., Thomas, U. O., Joy, E., Stanley, O. K., Ikenna, N. K., Uchenna, E., & Is, A. N. (2016). The status of school health services: a comparative study of primary schools in a developing country. Am J Public Health Res, 4(2), 42–46. DOI:10.12691/ajphr-4-2-1 de Villiers, A., Steyn, N.P., Draper, C.E. et al. (2012). ―HealthKick‖: Formative assessment of the health environment in low-resource primary schools in the Western Cape Province of South Africa. BMC Public Health 12, 794. doi:10.1186/1471-2458-12-794
Hens, L., Wiedemann, T., Raath, S., Stone, R., Renders, P., Craenhals, E., & Richter, B. (2010). Monitoring environmental management at primary schools in South Africa. Journal of Cleaner production, 18(7), 666–677. https://doi.org/10.1016/j.jclepro.2009.11.001
Jordán, O. R. C., del Campo, D. G. D., & Galarraga, S. A. (2017). Didáctica de la educación física por modelos para educación primaria. Síntesis.
Jourdan, D., Pironom, J., Simar, C., & Sormunen, M. (2018). Health education in schools: factors influencing parents’ views of the home– school relationship in France. International Journal of Health Promotion and Education, 56(1), 32–50. https://doi.org/10.1080/14635240.2017.1408419
Kapustin, I., Goltyai, S., Yevtushenko, V., Myroshnichenko, V., & Rudakova, O. (2018). Analysis of regional monitoring of preschool quality of education in 2017/2018 academic years [Аналіз результатів регіонального моніторингу якості дошкільної освіти в 2017/2018 н.р.] (Volyanska ed.). Ukraine, Kharkiv: Kharkiv Academy of Сontinuous Education. (In Ukrainian).
Kohl, H. W., Craig, C. L., Lambert, E. V., Inoue, S., Alkandari, J. R., Leetongin, G., & Kahlmeier, S. (2012). The pandemic of physical inactivity: global action for public health. The lancet, 380(9838), 294– 305. https://doi.org/10.1016/S0140-6736(12)60898-8
Lunyachek, V. (2011). Problems of the Education System Development of Ukraine in Times of Crisis. Public policy and administration, 10(1). 67– 79.
Madureira, J., Paciência, I., Ramos, E., Barros, H., Pereira, C., Teixeira, J. P., & Fernandes, E. D. O. (2015). Children’s health and indoor air quality in primary schools and homes in Portugal—Study design. Journal of Toxicology and Environmental Health, Part A, 78(13-14), 915– 930. https://doi.org/10.1080/15287394.2015.1048926
Marmot, M., Allen, J., Goldblatt, P., Boyce, T., McNeish, D., Grady, M., & Geddes, I. (2010). The Marmot review: Fair society, healthy lives. London: UCL.
Rowling, L. & Jeffreys, V. (2000). Challenges in the development and monitoring of Health Promoting Schools. Health Education, 100(3), 117– 123. https://doi.org/10.1108/09654280010320929
Seema, А. (2019). The Importance of Early Childhood Education for a Sustainable Society: A Sociological Analysis. Journal of Bank Management & Financial Strategies 2(3), 26–32.
Taylor, R. W., Farmer, V. L., Cameron, S. L. et al. (2011). School playgrounds and physical activity policies as predictors of school and home time activity. Int J Behav Nutr Phys Act 8, 38. doi:10.1186/1479- 5868-8-38
The State Emergency Service of Ukraine. Analytical report on the status of non-productive injury in Ukraine for the 12 months of 2017. Retrieved from https://www.dsns.gov.ua/files. (In Ukrainian).
Tsyuman, T. P. & Boichuk, Н. І. (2018). Code of Safe Educational Environment [Кодекс безпечного освітнього середовища]. Ukraine: Kiyiv, 2018. (In Ukrainian).
Wahl, G. (2017). Potential of public health service screenings in kindergartens and schools for prevention reporting. Journal of Health Monitoring, 2(S2). 33–36. DOI 10.17886/RKI-GBE-2017-093
Wedderkopp, N., Jespersen, E., Franz, C. et al. (2012). Study protocol. The Childhood Health, Activity, and Motor Performance School Study Denmark (The CHAMPS-study DK). BMC Pediatr 12, 128. doi:10.1186/1471-2431-12-128.
Yu, Y. & Li, Y. (2017, September). Physical Education in Primary and Middle Schools from the Perspective of Physical Fitness and Health Monitoring. In 2nd International Conference on Judicial, Administrative and Humanitarian Problems of State Structures and Economic Subjects (JAHP 2017). Atlantis Press. https://doi.org/10.2991/jahp-17.2017.20