Artículos
Symptoms of psychological burden on health care providers regarding Covid-19
Sintomas de carga psicológica en los proveedores de atención médica respecto al Covid-19
 M.M AL-MERAB MMALmreab@pnu.edu.sa
A.M HAMZA
M.M AL-MERAB MMALmreab@pnu.edu.sa
A.M HAMZA
Symptoms of psychological burden on health care providers regarding Covid-19
Utopía y Praxis Latinoamericana, vol. 26, no. Esp.2, pp. 244-253, 2021
Universidad del Zulia

This work is licensed under Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International.
Received: 27 February 2021
Accepted: 24 March 2021
Abstract: The COVID-19 pandemic has affected an increasing number of healthcare providers. However, they face vast physical and psychological challenges. Therefore, we assessed healthcare providers’ symptoms of psychological burden concerning their response to the COVID-19 pandemic. A sample of healthcare providers completed the Depression Anxiety Stress Scale online. Analyses were performed on participants ’psychological burden symptoms since the COVID-19 outbreak. COVID-19 caused a relatively significant level of psychological burden among healthcare providers. Analyses showed that academic qualification was the main factor affecting this burden. Applying the online program could reduce the psychological burden on healthcare providers.
Keywords: Healthcare providers, psychological burden, coronavirus, stress, depression..
Resumen: La pandemia de COVID-19 ha afectado a un número creciente de proveedores de atención médica. sin embargo, enfrentan grandes desafíos físicos y psicológicos. Por lo tanto, evaluamos los síntomas de carga psicológica de los proveedores de atención médica con respecto a su respuesta a la pandemia de COVID-19. Una muestra de proveedores de atención médica completó la Escala de estrés, ansiedad y depresión en línea. Se realizaron análisis de los síntomas de carga psicológica de los participantes desde el brote de COVID-19 que causó un nivel relativamente significativo de carga psicológica entre los proveedores de atención médica. Los análisis mostraron que la calificación académica fue el principal factor que incidió en esta carga. La aplicación del programa en línea podría reducir la carga psicológica en los proveedores de atención médica.
Palabras clave: Proveedores de atención médica, carga psicológica, coronavirus, estrés, depresión..
INTRODUCTION
Since the first case of the novel coronavirus, SARS‐CoV‐2, also known as coronavirus disease 2019(COVID-2019), was detected at the end of 2019 in Wuhan, Hubei Province, China, the number of new casesout of China has increased rapidly. The World Health Organization (WHO) Emergency Committee declared COVID-19 a global pandemic on March 11, 2020, and it has affected all countries worldwide. To date, there have been 1,918,138 confirmed COVID-19 cases and 123,126 deaths globally.
Hospital workers, especially physicians and nurses, were more susceptible to psychological disorders after treating patients with SARS more than a decade ago (Verma et al.: 2004, pp. 743-748).
Hence, knowledge of healthcare workers’ current psychological state is vital (Lu et al.: 2020, pp. 33-40). Healthcare Providers specifically involved in the diagnosis, treatment, and care of patients infected with COVID- 19 are at noteworthy risk of contracting the virus and possibly spreading it to their family or friends. (Neto et al.: 2020). In addition, working in tight spaces, having to wear personal protective equipment, and attending to anxious patients adds to the burdens placed on healthcare providers (Wang et al.: 2020, p.1729).
Healthcare providers’ mental health is the foundation of a well-functioning health care system. As a result of the coronavirus pandemic, healthcare providers are under immense strain from heavy workload coupled with increased healthcare expenditures (Moazzami et al.: 2020). Thus, the enormous challenge of COVID-19 could lead to healthcare providers’ psychological burden (Lu et al.: 2020, p.33-40).
The most common reasons of psychological burden among healthcare providers include long hours of work, sleep disturbances, physical fatigue, lack of personal protective equipment, patients with negative emotions, confusion, isolation, discrimination, and the fear of becoming infected and infecting their family (Conversano et al.: 2020, p. 1900; Du et al.:2020; Kang et al.: 2020, p.14). The more obstacles they face, the greater the chance that pressure may be internalized, causing mental health problems such as stress, anxiety, and depression (Chen et al.: 2020, pp.198-204; Liu et al.: 2019, p. 22-27; Moore et al.: 2020, pp. 1-8; Wu et al.: 2020, pp.3-6). Healthcare providers’ psychological burden also has serious consequences for patients and could cause a devastating collapse of the medical system (Patel et al.: 2018, pp. 76-89).
Considering these risks, it is important to reflect on the experiences of healthcare providers, identify the similarities and discrepancies between the experiences of various groups of healthcare providers, implement tailored interventions and provide consistent and comprehensive support to healthcare providers to attend to their physical and healthcare needs during the COVID-19 pandemic COVID-19 (Xiong and Pen: 2020, pp. e740- e741). Healthcare providers can experience stress, depression, and anxiety when faced with COVID-19 infected patients (Moore et al.: 2020, pp. 1-8; Wu et al.: 2020, pp. 3-6). The present study aimed to investigate the psychological burden levels of healthcare providers during the Covid-19 outbreak.
METHODOLOGY
Study Aim
This study aimed to determine the effect of the COVID-19 outbreak on healthcare providers’psychological burden.
Participants And Procedures
A cross-sectional survey was designed to analyze the psychological responses of healthcare workers and related factors during the COVID-19 outbreak. We used an online survey to reduce face to face encounters and to promote the involvement of busy healthcare workers who were working in hospitals in Riyadh, Saudi Arabia. The survey was shared among various social network groups of healthcare providers from varied specialties. At the beginning of the survey, all respondents indicated their willingness to participate. Data were collected from August to September 2020. The response rate was 87.8%, which resulted in a sample of 310 healthcare providers.
The total number of participants in Riyadh hospitals was 1500, which was calculated using Epi Info (version 6.04) computer software. With an expected frequency of 50% and a confidence level of 95%, the estimated sample size was 310. Statistical analyses were performed using SPSS version 25.0. Data are presented using descriptive statistics in the form of means and standard deviation for quantitative variables.
Ethical Considerations
The research proposal was approved by the Institutional Review Board of Princess Norah Bint Abdul Rahman University (no. RO2020-P-009). Participants faced no risks owing to participation, and the study followed the common ethical principles associated with clinical research. Written consent was obtained from participating healthcare providers after we explained the nature and purpose of the study, that confidentiality and anonymity would be assured, and that they had the right to withdraw from the study at any time.
Survey Instrument
Sociodemographic data were collected, including age, specialty, years of experience, academic qualification, shift type, and daily working hours since the outbreak.
The Depression Anxiety Stress Scale (Lovibond and Lovibond: 1995) was used to assess the status of participants’ psychological burden. A scale is a self-report tool containing 21 items that assess three constructs: depression, anxiety, and stress (seven items each). Items consist of statements referring to the previous week, and participants are asked to report the most appropriate option: “0” = it is not suitable for me, “1” = it is a little bit suitable for me, “2” = it is usually suitable for me, and “3” = it is completely suitable for me. A score of 5-6 indicates minor depression, 7-10 indicates moderate depression, 11-13 indicates acute depression, and ≥ 14 indicates very acute depression. Scores were added for each scale to produce a total score, and higher scores indicated a more severe psychological burden.
Cronbach’s alpha was used to measure reliability: αs = .91 for depression, .81 for anxiety, and .85 forstress. An explanatory factor analysis was conducted to assess construct validity.
The correlations between sub-dimensions were .39 for depression-anxiety, .32 for anxiety -stress, and .48 for depression-stress.
RESULTS
Participants’ Characteristics and DASS-21 Scores
Table (1) shows participants’ characteristics. Table (2) shows participants’ scores on the DASS-21.
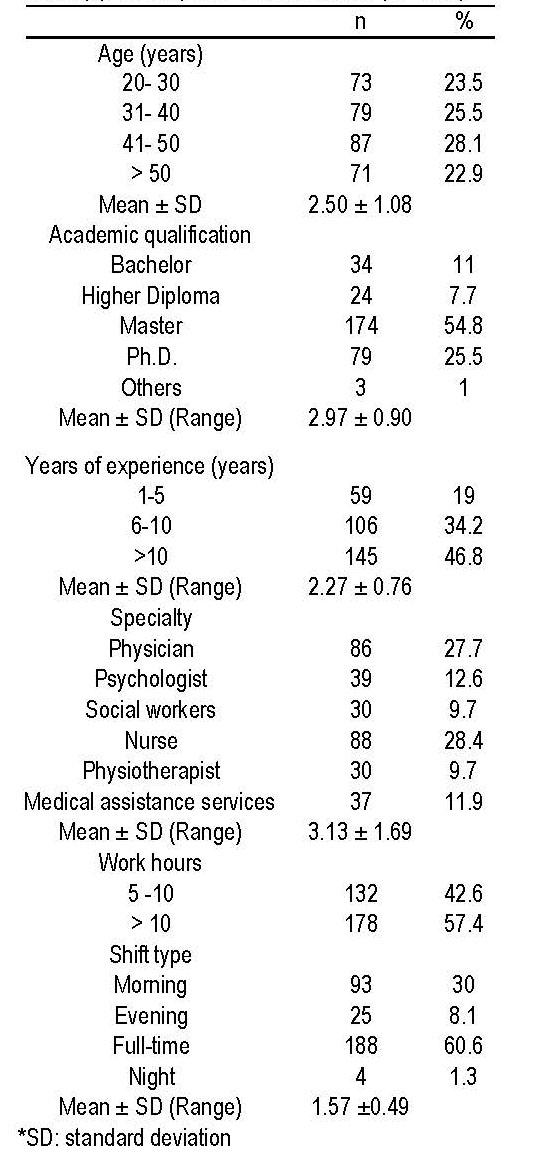
Table (1).: This table shows that 28.1% of the study sample age ranging from 41-50 years 2.50 ± 1.08. More than half of the study sample was a master’s degree, 54.8%. 2.97 ± 0.901. According to specialty, 28.4% of the study sample was nurses 3.132 ± 1.69. In relation to the year of experience was more than ten years with 46.8% of the study sample 2.27 ± 0.763. Nearly more than half of the 57.4 work more than 10 hours. The majority of them were working full time (60.6 %), with 1.57 ±0.49.
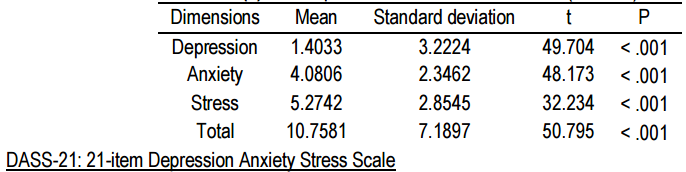
Table (2). Looking at the above table, we find that the general characteristic of all dimensions (depression, anxiety, stress) was a function of a low degree, as well as the total sum of the dimensions, where the number of the sample = 310, and the value of (T) test for all dimensions and the total came respectively = (-49.704, - 48.173, -32.234, -50.795) at the level of significance = 0.000, which is a statistically significant difference in correlation between depression, stress, and anxiety among the study sample.
Table (3) shows the results of analyses of variance and Mann-Whitney U tests concerning various sociodemographic characteristics and their association with depression, stress, and anxiety scores. Depression was significantly associated with participants’ age, specialty, academic qualification, years ofexperience, working hours, and shift type. Stress was significantly associated with participants’ age andacademic qualification, and years of experience.
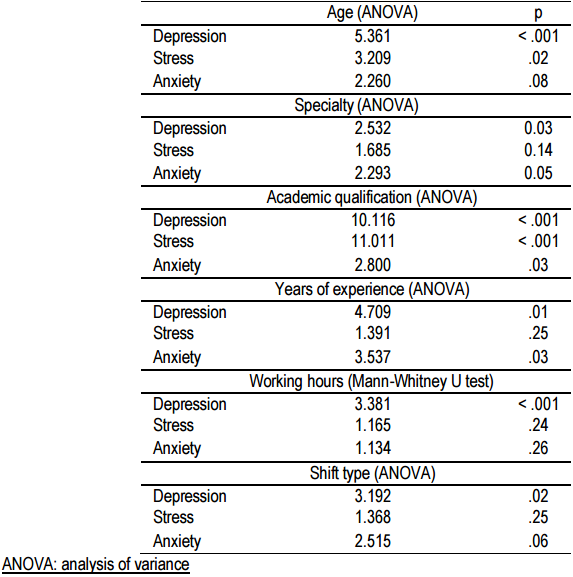
Looking at the above table, we find that there are statistically significant differences in the dimension of depression and stress, while there are no differences in the dimension of anxiety and the total sum of the dimensions, where the value of (P) for the dimension of depression = 5.361 at a significance level = 0.00, which is a statistical function in favor of age from 20-30 Years, we also find the value (q) for the stress dimension = 3.209 at a significance level = 0.00, which is a statistical function in favor of age from 51 and over. In contrast, there are no statistically significant differences in the dimension of anxiety and the total sum of the dimensions, where the value of (P) for the dimension of anxiety = 2.260 at the level of significance = 0.08, which is not a statistical function. It is a statistical function. For specialty, we find that there are statistically significant differences in the dimension of depression and anxiety, while there are no differences in the dimension of stress and the total sum of the dimensions, where the value of (P) for the dimension of depression= 2.532 came at a significance level = 0.03, which is a statistical function in favor of medical services. We also find the value (q) for the anxiety dimension = 2.293 at a significance level = 0.05, which is a statistical function in favor of a psychologist. While there are no statistically significant differences in the dimension of pressures and the total sum of the dimensions, where the value of (P) for the dimension of pressures = 1.685 at the level of significance = 0.14, which is not a statistical function, we also find the value of (P) for the total sum of the dimensions = 2.174 at the level of significance = 0.06 which is Is a statistical function.
We also find that there are statistically significant differences in all dimensions (depression, anxiety, stress) as well as the total sum of the dimensions, where the value of (P) for three dimensions, respectively,= (10.116, 2.800, 11.011, 7.987) at the level of significance = ( 0.00 and 0.03) which is a statistical function, so there are statistically significant differences in depression in favor of others, and there are also statistically significant differences in anxiety in favor of a bachelor’s, and also there are statistically significant differences in pressures in favor of a higher diploma, as well as there are statistically significant differences in the total number of dimensions in favor of a diploma. For the year of experience, we find that there are statistically significant differences in the dimension (depression, anxiety, as well as the total number of dimensions), where the value of (q) came to them, respectively = (4.709, 3.537, 3.709) at the level of significance = (0.01 and 0.03), which is Statistical function, then there are statistically significant differences in depression in favor of 1-5 years, and there are also statistically significant differences in anxiety in favor of 1-5 years, and there are also statistically significant differences in the total number of dimensions in favor of 1-5 years. While there are no statistically significant differences in pressures attributed to years of experience, where the value of (P) for the stress dimension = 1.391 at a significance level = 0.25, which is not a statistical function.
There are statistically significant differences in the total depression dimension, while there are no differences in the anxiety and stress dimension, as the Mann Whitney value for the depression dimension = 9364,000 At significance level = 0.00, which is a statistical function in favor of 5-10 hours, we also find the Man-Whitney value for the total = 10108,000 at significance level = 0.03, which is a statistical function in favor of 5-10 hours. While there are no statistically significant differences in the dimension of anxiety and stress, as the value of Mann Whitney for the dimension of anxiety = 10928.500 at a significance level = 0.26, which is not a statistical function, we also find the value of Mann Whitney for the dimension of stress = 10860,000 at a significance level = 0.24 which is not a statistical function.
In relation to shifting type, we find that there are statistically significant differences in the dimension (depression, the total sum of dimensions), where the value of (q) for them, respectively, = (3.192, 2.859) at the level of significance = (0.02 and 0.04), which is a statistical function, then there are statistically significant differences in depression in favor of the evening period, and there are also statistically significant differences in the total in favor of the evening period. In contrast, there are no statistically significant differences in the two dimensions of anxiety and stress due to the working period, where the value of (q) for the dimension of anxiety= 2.515 at a significance level = 0.06 and the value for (q) for the dimension of stress = 1.368 at the level of significance = 0.25, which is not a statistical function.
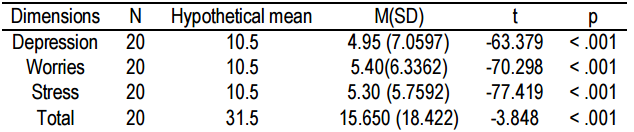
Looking at the above table, we find that the general characteristic of all dimensions (depression, anxiety, stress) was a function of a low degree, as well as the total sum of the dimensions, where the number of the sample was = 20, and the value of (t) test for all dimensions and the total respectively = -63.379 70.298, -77.419, -3.848) at the level of significance = 0.000 which is a statistically significant function.
Consequently, through a comparison between the spoken value and the arithmetic mean of eachdisorder, it becomes clear to the researcher that there is a clear reduction in the mean of all disorders than its spoken value, which indicates that the treatment program is effective in reducing these disorders that were measured.
The researchers explain from this result that the online therapeutic program was effective in treating the disorders to which the program was applied.
DISCUSSION
Although primary care providers are exposed to clinical burnout, prolonged stress, trauma, and physical and mental fatigue, those who are treating patients with COVID-19 face ethical tension that can lead to continued emotional stress, likely resulting in excessive fatigue (Moloney et al.: 2020, pp.1-13). The current results of the DASS-21 scores showed significant correlations between all three dimensions: depression, anxiety, and stress. These findings were in accordance with those of Elbay et al.: (2020, pp. 25-39), who indicated that 64.7 % of physicians had depressive symptoms, 51.6% had anxiety, and 41.2 % had stress- related symptoms in the early period of the outbreak in Turkey. In addition, in accordance with Wu et al.: (2020, pp. 3-6), frontline healthcare professionals experience psychological distress owing to an increased risk of COVID-19 infection and working in high-risk primary care medical settings.
Regarding age, our results revealed significant differences in the dimensions of depression and stress but not anxiety or total DASS-21 score. Specifically, those who were aged 20-30 years were more depressed than their counterparts. These results coincide with those of Elbay et al.: (2020, pp. 25-39), who found that age was associated with the DASS-21 subscales. Further, those who were aged > 50 years were more stressed than their counterparts.
Regarding specialty, our results revealed significant differences in the dimensions of depression and anxiety but not stress or total DASS-21 score. Specifically, those who specialized in medical services were more depressed than their counterparts. Further, psychologists had more anxiety than did their counterparts. These findings were in accordance with Alkhamees et al.: (2020, pp. 42-63), who found that 27.9% of medical providers had higher scores on the stress, anxiety, and depression subscales.
Regarding academic qualification, our results revealed significant differences in all three dimensions and total DASS-21 score. Specifically, those who reported “other,” “a bachelor’s degree,” and “a higher diploma” in medical services were more depressed, anxious, and stressed than their counterparts, respectively. Further, those who held “a diploma” scored higher on the DASS-21 than did their counterparts. In accordance with Olum et al.: (2020, p.181), 62% were medical doctors, and 92% had at least a bachelor’s degree. Overall, 69% had sufficient knowledge to experienced depression, stress, and anxiety.
Regarding working hours, our results revealed significant differences only for depression. Specifically, those who worked 5-10 hours a day were more depressed than their counterparts. In accordance with Kunaviktikul et al.: (2015, pp. 386-393), DASS-21 total and subscale scores in frontline workers were associated with increased weekly working hours.
Regarding shift type, our results revealed significant differences for depression and total DASS-21 score. Specifically, those who worked in the evening were more depressed than their counterparts. In accordance with Elbay et al.: (2020, pp. 113-130), DASS-21 total and subscale scores in frontline workers were associated with increased weekly working hours, and providers’ shift-type was associated with DASS-21 total scores.
Limitations
Our cross-sectional design limits our ability to follow-up with participants. The data collection phase of the study was completed within 30 days. The data collection phase of the study was completed within six days. Given the time-sensitivity of this emergency situation, we analyzed the psychological symptoms and related causes of healthcare providers promptly. Furthermore, selection bias is a possibility, and the results should be generalized with caution.
CONCLUSION
Worldwide, COVID-19 poses a major public health problem as it is very complex and contagious. Researchers should focus on healthcare providers’ psychological burden, including the key factor that is associated with their stress, anxiety, and depression: academic qualification. Notably, shift type, working hours, age, and specialty were also associated with increased depression.
ACKNOWLEDGMENT
The authors extend their appreciation to the Deputyship for Research& Innovation, Ministry of Education in Saudi Arabia for funding this research work through the project )number (PNU-DRI-Targeted-20-018)
BIODATA
MONEERAH MOHAMMAD AL MERAB: Associate Professor of Psychology at Princess Noura Bint Abdul Rahman University, former Dean of Girls' Colleges at the University of Hail, Deputy Director of Pre-University Education at Princess Noura Bint Abdul Rahman University, Former Head of Field Training in the Department of Psychology, Chairman of the Department's Scientific Research Committee, Member of the Scientific Society Saudi Arabia for Psychological Counseling, a member of more than one society serving the community, a member of the Women and Autism Spectrum Committee, a member of the committee to create a postgraduate program in the department. My interests are scientific research in the field of mental abilities. Website: www.//faculty.uoh.edu.sa/m.almerab. Email: MMALmreab@pnu.edu.sa. drmoneera@ hotmail.com
A. M. HAMZA: Ahmed Hamza (PhD) is currently an Associate Professor of Psychology, King Salman Institute for Studies and Consulting Services, Majmaah University. Princess Nourah bint Abdulrahman, Saudi Arabia. Her research interests include DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS ,DSM- 5 , and psychological measures. Her research has appeared in the Journal of Religion and Health (2018) International Journal of Innovation, Creativity and Change(2020).
H. M. AL-SAYED: Hala Abd Ellatif Elsayed received her B.Sc. degree in Education from Suez Canal University, Egypt, in 1995 and Ph.D. degree in Clinical Psychology from Suez Canal University, Egypt, and University of Cincinnati (Channel) in 2010. She had published papers in Egypt and international Journals in the field of Clinical Psychology, presently; She is Associate Professor in Clinical Psychology Program / College of Health and Rehabilitation Sciences / University of Princess Nourah Bint Abdulrahman
Z. A. MOHAMED: Zamzam Ahmed Ahmed received his B.Sc degree in psychiatric and mental health nursing from Assiut university Egypt, in 2000 and M.Sc. degree in psychiatric and mental health nursing from Assiut university Egypt, in 2005. He had published papers in international Journals of nursing science in the field of mental health nursing, presently; received PhD degree in psychiatric and mental health nursing child psychology in 2013 and received Assisstant professor degree in 2018 now assistant professor in psychiatric and mental health nursing and work in clinical psychology in health and rehabilitation science in princess noura bint Abdulrahman university.
BIBLIOGRAPHY
ALKHAMEES, A, A, ALRASHED, S, A, ALZUNAYDI, A, A, ALMOHIMEED, A, S, & ALJOHANI, M, S, (2020).“The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia”. Comprehensive Psychiatry, 102, pp. 42-63.
CHEN, Y, LIU, J, LI, Z, LIU, B, JI, Y, JU, Y, ... & LI, L, (2020). “The Tendency of Modified Electroconvulsive Therapy–Related Working Memory and Subjective Memory Deficits in Depression: A Prospective Follow-up Study”. The Journal of ECT, 36(3), pp. 198-204.
CONVERSANO, C, DI GIUSEPPE, M, MICCOLI, M, CIACCHINI, R, GEMIGNANI, A, & ORRÙ, G, (2020).“Mindfulness, age and gender as protective factors against psychological distress during Covid-19 pandemic”.Frontiers in Psychology, 11, p.1900.
DU, J, DONG, L, WANG, T, YUAN, C, Fu, R, ZHANG, L, ... & LI, X, (2020). “Psychological symptoms amongfrontline healthcare workers during COVID-19 outbreak in Wuhan". General Hospital Psychiatry, p.112412
ELBAY, R, Y, KURTULMUŞ, A, ARPACIOĞLU, S, & KARADERE, E, (2020). “Depression, Anxiety, StressLevels of Physicians and Associated Factors in Covid-19 Pandemics". Psychiatry Research, pp. 25-39.
KANG, L, LI, Y, HU, S, CHEN, M, YANG, C, YANG, B, X, ... & LIU, Z, (2020). “The mental health of medicalworkers in Wuhan, China dealing with the 2019 novel coronavirus”. The Lancet Psychiatry, 7(3), p. e14.
KUNAVIKTIKUL, W, WICHAIKHUM, O, NANTSUPAWAT, A, NANTSUPAWAT, R, CHONTAWAN, R,KLUNKLIN, A, ... & SIRAKAMON, S, (2015). “Nurses' extended work hours: patient, nurse and organizationaloutcomes”. International Nursing Review, 62(3), pp. 386-393.
LIU, Y, ZHANG, J, HENNESSY, D, A, ZHAO, S, & JI, H, (2019). “Psychological strains, depressive symptoms, and suicidal ideation among medical and non-medical staff in urban china”. Journal of Affective Disorders, 245, pp. 22-27.
LOVIBOND, S, H, & LOVIBOND, P, F, (1995). “Depression anxiety stress scale-21 (DASS-21)". Manual for The Depression Anxiety & Stress Scales.
LU, L, QUE, J, LE SHI, J, D, LIU, J, ZHANG, L, WU, S, ... & GONG, Y, (2020). “Psychological impact of theCOVID-19 pandemic on healthcare workers: a cross-sectional study in China”. General Psychiatry, 33(3), pp. 33-54.
MOAZZAMI, B, RAZAVI-KHORASANI, N, MOGHADAM, A, D, FAROKHI, E, & REZAEI, N, (2020). “COVID-19 and telemedicine: Immediate action required for maintaining healthcare providers well-being”. Journal of Clinical Virology, p.104345.
MOLONEY, K, SCHEUER, H, ENGSTROM, A, SCHREIBER, M, WHITESIDE, L, NEHRA, D, ... & ZATZICK,D, (2020). “Experiences and insights from the early US COVID-19 epicenter: A rapid assessment procedureinformed clinical ethnography case series”. Psychiatry, pp.1-13.
MOORE, T, M, BARZILAY, R, GREENBERG, D, M, DIDOMENICO, G, E, BROWN, L, A, WHITE, L, K, ... &GUR, R, E, (2020).” Resilience, COVID-19-related stress, anxiety and depression during the pandemic in alarge population enriched for healthcare providers”. Translational Psychiatry, 10(1), pp.1-8.
NETO, M, L, R, ALMEIDA, H, G, ESMERALDO, J, D, A, NOBRE, C, B, PINHEIRO, W, R, DE OLIVEIRA, C, R,T, ... & DA SILVA, C, G, L, (2020). “When health professionals look death in the eye: the mental health ofprofessionals who deal daily with the 2019 coronavirus outbreak”. Psychiatry Research, p.112972.
OLUM, R, CHEKWECH, G, WEKHA, G, NASSOZI, D, R, & BONGOMIN, F, (2020). “Coronavirus Disease-2019: Knowledge, attitude, and practices of health care workers at Makerere university teaching hospitals,Uganda”. Frontiers in Public Health, 8, p. 181
PATEL, V, BURNS, J, K, DHINGRA, M, TARVER, L, KOHRT, B, A, & LUND, C, (2018). “Income inequalityand depression: a systematic review and meta‐analysis of the association and a scoping review ofmechanisms”. World Psychiatry, 17(1), pp. 76-89.
VERMA, S, MYTHILY, S, CHAN, Y, H, DESLYPERE, J, P, TEO, E, K, CHONG, S, A, (2004). “Post- SARSpsychological morbidity and stigma among general practitioners and traditional Chinese medicine practitioners in Singapore”. Ann. Acad. Med. Singap, 33 (6), pp. 743–748.
WANG, C, PAN, R, WAN, X, TAN, Y, XU, L, HO, C, S, & HO, R, C, (2020). “Immediate psychologicalresponses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China”. International Journal of Environmental Research and Public Health, 17(5), p.1729.
WU, Y, WANG, J, LUO, C, HU, S, LIN, X, ANDERSON, A, E, ... & QIAN, Y, (2020). “A comparison of burnoutfrequency among oncology physicians and nurses working on the front lines and usual wards during the COVID-19 epidemic in Wuhan, China”. Journal of Pain and Symptom Management, pp. 3-6.
XIONG, Y, & PENG, L, (2020). “Focusing on health-care providers' experiences in the COVID-19 crisis". The Lancet Global Health, 8(6), pp. e740-e741.