Abstract:
Peripheral vascular injuries are uncommon in civilian trauma but can threaten the patient’s life or the viability of the limb. The definitive control of the vascular injury represents a surgical challenge, especially if the patient is hemodynamically unstable. This article proposes the management of peripheral vascular trauma following damage control surgery principles. It is essential to rapidly identify vascular injury signs and perform temporary bleeding control maneuvers. The surgical approaches according to the anatomical injured region should be selected. We propose two novel approaches to access the axillary and popliteal zones. The priority should be to reestablish limb perfusion via primary repair or damage control techniques (vascular shunt or endovascular approach). Major vascular surgeries should be managed post-operatively in the intensive care unit, which will allow correction of physiological derangement and identification of those developing compartmental syndrome. All permanent or temporary vascular procedures should be followed by a definitive repair within the first 8 hours. An early diagnosis and opportune intervention are fundamental to preserve the function and perfusion of the extremity.
Key Words: Peripheral vascular traumaPeripheral vascular trauma,vascular trauma of the extremitiesvascular trauma of the extremities,hemodynamically unstablehemodynamically unstable,damage control surgerydamage control surgery,Vascular System InjuriesVascular System Injuries,Popliteal ArteryPopliteal Artery,Femoral ArteryFemoral Artery,Advanced Trauma Life Support CareAdvanced Trauma Life Support Care,Axillary ArteryAxillary Artery,TourniquetsTourniquets,FasciotomyFasciotomy,Ankle Brachial IndexAnkle Brachial Index,Endovascular ProceduresEndovascular Procedures.
Resumen:
El trauma vascular periférico no es común en el contexto civil, pero representa una amenaza para la vida del paciente o de la extremidad. El control definitivo de la lesión vascular representa un desafío quirúrgico, especialmente en pacientes con inestabilidad hemodinámica. Este artículo describe la propuesta de manejo del trauma vascular periférico de acuerdo con los principios de la cirugía de control de daños. Se debe identificar los signos sugestivos de lesión vascular y realizar oportunamente maniobras temporales para el control del sangrado. Se debe elegir el abordaje quirúrgico dependiendo del área anatómica lesionada. Se proponen dos nuevas incisiones para acceder a la región axilar y poplítea. La prioridad es restablecer la perfusión de la extremidad mediante el reparo primario o técnicas de control de daños (shunt vascular o abordaje endovascular). Los pacientes sometidos a cirugías vasculares mayores deben ser manejados postoperatoriamente en la unidad de cuidados intensivos para corregir las alteraciones fisiológicas e identificar aquellos que desarrollen un síndrome compartimental. Todos los procedimientos vasculares permanentes o temporales deben contar con un reparo definitivo en las primeras 8 horas. El diagnóstico temprano e intervención oportuna son fundamentales para salvaguardar la perfusión y funcionalidad de la extremidad.
Palabras clave: Trauma vascular periférico, trauma vascular de las extremidades, inestabilidad hemodinámica, hemodinámicamente inestable, control de daños en cirugia, daños del sistema vascular, arteria poplitea, arteria femoral, atención de soporte vital avanzado para traumatismo, arteria axilar, torniquete, fasciotomia, indice tobillo brazo, procedimientos endovasculares.
Carátula del artículo
Damage control of peripheral vascular trauma - Don’t be afraid of axillary or popliteal fosses
Control de daños del trauma vascular periférico - No le tema a la fosa axilar o poplítea
 Mario Alain Herrera
Mario Alain Herrera
Hospital Universitario del Valle, Colombia
Universidad del Valle, Colombia
Mauricio Millán
Universidad Icesi, Colombia
Fundación Valle del Lili, Colombia
Ana Milena del Valle
Hospital Felix Bulness, Chile
Mateo Betancourt-Cajiao
Universidad del Valle, Colombia
Yaset Caicedo
Fundación Valle del Lili, Colombia
Isabella Caicedo
Fundación Valle del Lili, Colombia
Linda M. Gallego
Universidad Icesi, Colombia
Diego Rivera
Centro Médico Imbanaco, Colombia
Michael W. Parra
Broward College, USA
Carlos A. Ordoñez
Universidad del Valle, Colombia
Universidad Icesi, Colombia
Fundación Valle del Lili, Colombia
Colombia Médica, vol. 52, no. 2, e4074735, 2021
Universidad del Valle
Received: 15 February 2021
Revised document received: 05 March 2021
Accepted: 05 April 2021
Introduction
Vascular injuries of the extremities are uncommon in civilian trauma. With a prevalence of 2% in blunt trauma and 4% in penetrating, their management remains a surgical and clinical challenge given the need for prompt hemorrhage control. A delay in intervention can lead to a patient´s exsanguination or can be associated with ischemic complications threatening the patient’s life and/or the viability of the limb. These types of injuries are typically prone to external compression in the prehospital care setting. Nevertheless, achieving definitive control of the vascular injury represents a surgical challenge, especially if the patient is hemodynamically unstable. This article proposes the management of peripheral vascular trauma following damage control surgery principles.
This article is a consensus that synthesizes the experience earned during the past 30 years in trauma critical care management of the severely injured patient from the Trauma and Emergency Surgery Group (CTE) of Cali, Colombia which is made up of experts from the University Hospital del Valle "Evaristo García", the University Hospital Fundación Valle del Lili, the Universidad del Valle and Universidad Icesi, the Asociación Colombiana de Cirugía, the Pan-American Trauma Society and the collaboration of international specialists of the United States of America, Europe, Japan, South Africa, and Latin America.
Epidemiology
Peripheral vascular trauma is more prevalent in the military than in civilian trauma 1-3. Falls from great heights, work-related accidents, and motorcycle crashes are common causes of vascular injury in blunt trauma 2-4. Penetrating trauma by gunshot or stab wounds prevails in developing countries such as Latin-America 5. A 30-year review study conducted by Mattox et al found 5,760 patients with vascular injuries with an overall prevalence of 19% involving the lower extremities and 14% involving the upper. The most common injured vessel of the lower extremity was the femoral artery in 45% , the femoral vein in 25% and the popliteal artery in 14%. Meanwhile, vascular injuries of the upper extremities involved the brachial artery in 52% and the radial or cubital artery in 30% 6,7. These results did not vary much from those reported previously in North America, Europe or Latin-America 8-12. Complete or partial transection of the vessel was the predominant type of injury 12.
The Prospective Observational Vascular Injury Treatment (PROOVIT) registry collected information on 542 vascular trauma patients, in which 241 presented with peripheral vascular injuries. They reported conservative management in 47% (66/141) of the lower extremity injuries and 33% (30/92) in the uppers. An initial open surgical approach was performed in 51% (72/141) in the lower extremity injuries and 71% (65/92) in the uppers. The primary repair rate was 78% (56/72) in the lower extremity vascular injuries and 78% (51/65) in the uppers. Prehospital tourniquet placement was used in 20% (47/233) of all peripheral vascular injury cases and prophylactic fasciotomy was performed in 33 and decompressive fasciotomy in 19 12. Similarly, D’Alessio et al reported a series of 56 patients from Milan, Italy, in which 75% of peripheral vascular trauma had associated orthopedic and/or neurological injuries. The open surgical approach was performed in 85%, while the remaining 15% underwent an endovascular repair with an overall limb preservation rate of 90.4%. Inferior limb amputation was required in 5 cases, three patients had prosthetic graft infection, two patients suffered graft rejection and the overall post-operative mortality was 5.7% 13.
Initial Approach
All efforts must be directed towards stabilizing the patient. Advanced Trauma Life Support - ATLS guidelines, the ABCDE mnemonic and damage control resuscitation principles should be followed and applied vigorously 14. Peripheral vascular trauma can be diagnosed in the initial evaluation if the presence of hard signs of injury are present or suspected in cases where soft signs exist (Table 1). Additionally, perfusion of the extremity distal to the injury site must be assessed and associated orthopedic, muscular and neurologic involvement must be ruled out. In cases where the patient is hemodynamically unstable, an emergency surgical approach is necessary. Otherwise, patients who are hemodynamically stable should undergo an ankle-brachial index and Doppler examination in the Trauma Bay. If positive, then a computed tomographic angiography (CT-Angio) to better delineate the injury 15.
Table 1
Hard and Soft Signs of Peripheral Vascular Injury

The American Association for the Surgery of Trauma (AAST) has developed a grading scale for peripheral vascular injuries (Table 2) 16.
Table 2
American Association for the Surgery of Trauma (AAST) Classification of Peripheral Vascular Trauma. AAST Peripheral Vascular Trauma Classification

Surgical Approach
Step 1: Attention should be directed towards identifying all immediate life-threatening injuries following the ABCDE approach of ATLS. Both femoral arterial and venous lines should be placed immediately for blood pressure monitoring and intravenous access. In hemodynamically unstable patients, damage control resuscitation via activation of the institution’s massive transfusion protocol should be initiated 17.
Step 2: Prompt identification of all hard and/or soft vascular injury signs. Orthopedic, muscular and/or soft tissue associated injuries should be considered. Temporary bleeding control maneuvers should be performed which include: wound packing, direct manual pressure or tourniquet placement 18. If the patient remains hemodynamically unstable despite initial resuscitation efforts, the placement of a Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) should be considered and placed as an adjuvant 19,20. The patient should then be transferred to the operating/hybrid room immediately.
Step 3: The surgical approach depends on the anatomical region:
- 1.
For axillary artery injuries, the patient must be placed in the supine position with the injured extremity taped to the forehead, exposing the axillary fossa. The access to the axillary artery can be achieved through an inverted “S” shaped incision starting at the pectoralis major muscle curving in the axillary fossa and ending in the arm between the bicep and tricep muscles. This incision prevents future scar retraction and functional limitation of the shoulder joint (Figure 1).
- 2.
The brachial artery lies in the bicipital groove that extends from the axillary fossa to the center of the ante-cubital fossa. It´s bifurcation can be approached by an “S” incision starting from the medial border of the arm, crossing through the ante-cubital fossa and ending in the lateral border of the proximal forearm.
- 3.
The radial and ulnar arteries are accessed via direct vertical incisions.
- 1.
The femoral artery is accessed via a vertical incision over the sartorius muscle before identifying a palpable pulse or ultrasound guidance in a pulseless artery.
- 2.
The popliteal artery can be accessed via a posterior “S” shaped incision starting in the postero-medial region of the thigh, crossing parallel in the mid popliteal fossa and ending vertically in the postero-lateral region of the leg. After skin incision, the subcutaneous tissue is dissected down the midline until the popliteal vessels are exposed. Be aware of both the tibial and peroneal nerves that are in the vicinity (Figure 2).
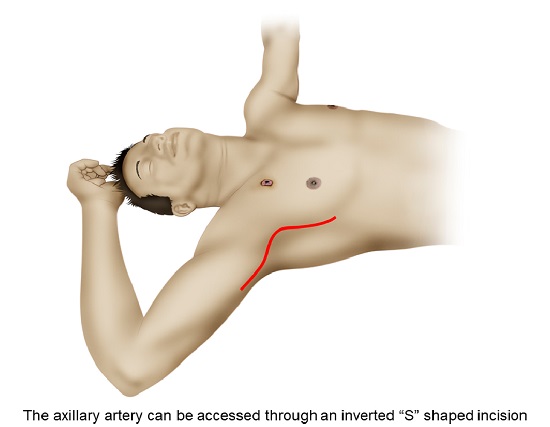 Figure 1
Surgical approach to the axillary artery. The axillary artery can be accessed through an inverted “S” shaped incision starting at the pectoralis major muscle, curving in the axillary fossa and ending in the arm between the bicep and tricep muscles. This incision prevents future scar retraction and functional limitation of the shoulder joint.
Figure 1
Surgical approach to the axillary artery. The axillary artery can be accessed through an inverted “S” shaped incision starting at the pectoralis major muscle, curving in the axillary fossa and ending in the arm between the bicep and tricep muscles. This incision prevents future scar retraction and functional limitation of the shoulder joint.
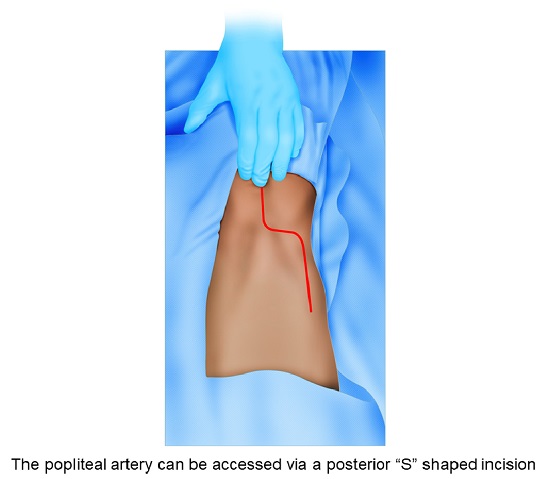 Figure 2
Surgical approach to the popliteal artery. The popliteal artery can be accessed via a posterior “S” shaped incision starting in the posteromedial region of the thigh, crossing parallel in the mid popliteal fossa and ending vertically in the postero-lateral region of the leg. Afterward, subcutaneous tissue should be dissected down the midline until the popliteal vessels are exposed, carefully not injuring the tibial and/or peroneal nerves.
Figure 2
Surgical approach to the popliteal artery. The popliteal artery can be accessed via a posterior “S” shaped incision starting in the posteromedial region of the thigh, crossing parallel in the mid popliteal fossa and ending vertically in the postero-lateral region of the leg. Afterward, subcutaneous tissue should be dissected down the midline until the popliteal vessels are exposed, carefully not injuring the tibial and/or peroneal nerves.
Step 4: Both proximal and distal control of the injury should be performed. Perform thrombectomy/embolectomy of the injured vessel routinely before definitive repair.
Step 5: Primary vascular repair is indicated if the patient is hemodynamically stable. Nevertheless, if the injured vessel requires partial resection, a primary repair can still be performed, only if the anastomosis is not under excessive tension. If the tension is excessive, an interposition graft with an autologous vein or synthetic graft can be performed. In cases of an isolated radial or cubital arterial injury and a patent palmar arch, the vessel can be ligated.
In complex vascular injuries, the persistence of hemodynamic instability or prolonged ischemia, a vascular shunt should be placed initially after proximal and distal control of the injury is obtained. The purpose of the shunt is to reperfuse the limb and limit the ischemic damage.
In cases where venous injuries cannot be primarily repaired, then the vessel should be ligated. Prophylactic fasciotomies are indicated in patients with compartment hypertension and/or impending compartment syndrome.
An endovascular approach can be performed in hemodynamically stable patients. Options include stent placement and/or thrombo-embolectomy of the injured vessel. Long-term patency rates are equivalent to those managed by open repair for proximal arterial injuries of the extremities 21,22.
Step 6: All permanent or temporary vascular procedures should have soft tissue coverage; all significant unstable fractures should be stabilized, and the wound should be packed or have a negative pressure dressing placed. All major vascular procedures should be managed postoperatively in the intensive care unit (ICU) for correction of the lethal diamond 23, serial vascular pulse checks and active clinical bedside surveillance of signs developing compartmental syndrome in cases where prophylactic fasciotomies were not performed.
Step 7: All shunted patients must return to the operating room within the first 8 hours to perform the definitive repair of the injury.
Complications
Complications include compartment syndrome, reperfusion injury and limb amputation. The amputation rate of upper extremity vascular injuries is around 1%. However, ligating the brachial artery has an amputation risk of 18 to 55%. Lower extremity vascular injuries have an overall amputation rate of 11%. Injuries of the popliteal or femoral arteries have an amputation risk of 28 to 37%, increasing up to 70% when there is a delay in presentation 24-28.
Conclusion
Peripheral vascular trauma becomes a surgical challenge for a well-trained surgeon aiming to preserve the function and perfusion of the extremity. A prompt and early intervention is required to improve outcomes and avoid complications. When facing hemodynamically unstable patients, control of hemorrhage becomes paramount, followed by reestablishing limb perfusion via primary repair or damage control techniques, if required and indicated.
References
White JM, Stannard A, Burkhardt GE, Eastridge BJ, Blackbourne LH, Rasmussen TE. The epidemiology of vascular injury in the wars in Iraq and Afghanistan. Ann Surg. 2011;253:1184-9. doi: 10.1097/SLA.0b013e31820752e3.
Muckart DJJ, Pillay B, Hardcastle TC, Skinner DL. Vascular injuries following blunt polytrauma. Eur J Trauma Emerg Surg. 2014;40:315-22. doi: 10.1007/s00068-014-0382-y.
Friend J, Rao S, Sieunarine K, Woodroof P. Vascular trauma in Western Australia: A comparison of two study periods over 15 years. ANZ J Surg. 2016;86:173-8. doi: 10.1111/ans.12309.
Konstantinidis A, Inaba K, Dubose J, Barmparas G, Lam L, Plurad D, et al. Vascular trauma in geriatric patients: A National Trauma Databank review. J Trauma. 2011;71:909-16. doi: 10.1097/TA.0b013e318204104e.
Sonneborn R, Andrade R, Bello F, Morales-Uribe CH, Razuk A, Soria A, et al. Vascular trauma in Latin America: A regional survey. Surg Clin North Am. 2002;82:189-94. doi: 10.1016/S0039-6109(03)00148-8.
Mattox KL, Feliciano DV, Burch J, Beall AC, Jordan GL, Debakey ME. Five thousand seven hundred sixty cardiovascular injuries in 4459 patients: Epidemiologic evolution 1958 to 1987. Ann Surg. 1989;209:698-707. doi: 10.1097/00000658-198906000-00007.
Baker AC, Clouse WD. Upper extremity and junctional zone injuries. In: Rasmussen TE, Nigel RM. Rich's Vascular Trauma. Elsevier; 2016. 149-67. doi: 10.1016/B978-1-4557-1261-8.00014-X.
Espinoza E, Castañeda E. Caracteristicas clinicas de los traumas vasculares perifericos en pacientes atendidos en un hospital general de Lima, Peru. Rev Medica Hered. 2014;25:122-8.
Montoya-Reales DA, Ochoa J. Características clínicas del trauma vascular periférico en pacientes atendidos en el Hospital Escuela Universitario, Honduras. Rev Méd Hondur. 2015; 83: 33-7.
Ockert S, Winkler M, Richter A, Palma P, Post S. Gefäßverletzungen nach extremitätentrauma. Zentralbl Chir. 2002;127:689-93. doi: 10.1055/s-2002-33575.
Diamond S, Gaspard D, Katz S. Vascular injuries to the extremities in a suburban trauma center. Am Surg. 2003; 69: 848-51.
DuBose JJ, Savage SA, Fabian TC, Menaker J, Scalea T, Holcomb JB, et al. The American association for the surgery of trauma prospective observational vascular injury treatment (PROOVIT) registry: Multicenter data on modern vascular injury diagnosis, management, and outcomes. J Trauma Acute Care Surg. 2015; 78: 215-23. doi: 10.1097/TA.0000000000000520.
D'Alessio I, Domanin M, Bissacco D, Romagnoli S, Rimoldi P, Sammartano F, et al. Operative treatment and clinical outcomes in peripheral vascular trauma: the combined experience of two centers in the endovascular era. Ann Vasc Surg. 2020; 62:342-8. doi: 10.1016/j.avsg.2019.06.037.
The Comittee on Trauma. Advanced Trauma Life Support. Student Course Manual. American College of Surgeon. 10th Edition; 2018. doi: 10.1111/j.1365-2044.1993.tb07026.x.
Kobayashi L, Coimbra R, Goes AMOJ, Reva V, Santorelli J, Moore EE, et al. AAST - WSES guidelines on diagnosis and management of peripheral vascular injuries. J Trauma Acute Care Surg. 2020; 89(6):1183-1196. doi: 10.1097/TA.0000000000002967.
Moore EE, Cogbill TH, Jurkovich GJ, McAninch JW, Champion HR, Gennarelli TA, et al. Organ injury scaling. III: Chest wall, abdominal vascular, ureter, bladder, and urethra. J Trauma. 1992;33:337-9.
Salamea JC, Himmler A, Valencia-Angel LI, Ordoñez CA, Parra M, Caicedo Y, et al. Whole Blood for Blood Loss: Hemostatic Resuscitation in Damage Control. Colomb Med (Cali). 2020; 51(4): e4044511. doi: 10.25100/cm.v51i4.4511.
Melendez JJ, Caicedo Y, Guzman M, Serna JJ, Ordoñez J, Angamarca E, et al. Prehospital Damage Control: The Management of Volume, Temperature...and Bleeding! Colomb Med (Cali). 2020; 51(4):e4024486. doi: 10.25100/cm.v51i4.4486.
Ordoñez CA, Parra M, Caicedo Y, Padilla N, Rodriguez F, Serna JJ, et al. REBOA as a New Damage Control Component in Hemodynamically Unstable NTCH patients. Colomb Med (Cali). 2020; 51(4): e4064506. Doi: 10.25100/cm.v51i4.4506
Ordoñez CA, Parra MW, Serna JJ, Rodríguez H F, García AF, Salcedo A, et al. Damage Control Resuscitation : REBOA as the New Fourth pillar. Colomb Med (Cali). 2020; 51(4): e4014353. doi: 10.25100/cm.v51i4.4353.
Liu JL, Li JY, Jiang P, Jia W, Tian X, Cheng ZY, et al. Literature review of peripheral vascular trauma: Is the era of intervention coming?. Chinese J Traumatol. 2020;23:5-9. doi: 10.1016/j.cjtee.2019.11.003.
Ganapathy A, Khouqeer AF, Todd SR, Mills JL, Gilani R. Endovascular management for peripheral arterial trauma: The new norm?. Injury. 2017;48:1025-30. doi: 10.1016/j.injury.2017.02.002.
Ditzel RM, Anderson JL, Eisenhart WJ, Rankin CJ, DeFeo DR, Oak S, et al. A review of transfusion- And trauma-induced hypocalcemia: Is it time to change the lethal triad to the lethal diamond?. J Trauma Acute Care Surg. 2020;88:434-9. doi: 10.1097/TA.0000000000002570.
Mullenix PS, Steele SR, Andersen CA, Starnes BW, Salim A, Martin MJ. Limb salvage and outcomes among patients with traumatic popliteal vascular injury: An analysis of the National Trauma Data Bank. J Vasc Surg. 2006; 44: 94-100. doi: 10.1016/j.jvs.2006.02.052.
Ratnayake A, Samarasinghe B, Bala M. Outcomes of popliteal vascular injuries at Sri Lankan war-front military hospital: Case series of 44 cases. Injury. 2014;45:879-84. doi: 10.1016/j.injury.2014.01.003.
Pourzand A, Fakhri BA, Azhough R, Hassanzadeh MA, Hashemzadeh S, Bayat AM. Management of high-risk popliteal vascular blunt trauma: Clinical experience with 62 cases. Vasc Health Risk Manag. 2010;6:613-8. doi: 10.2147/vhrm.s11733.
Fortuna G, DuBose JJ, Mendelsberg R, Inaba K, Haider A, Joseph B, et al. Contemporary outcomes of lower extremity vascular repairs extending below the knee: A multicenter retrospective study. J. Trauma Acute Care Surg. 2016; 81: 63-9. doi: 10.1097/TA.0000000000000996.
Gopinathan N, Santhanam S, Saibaba B, Dhillon M. Epidemiology of lower limb musculoskeletal trauma with associated vascular injuries in a tertiary care institute in India. Indian J Orthop. 2017;51:199-204. doi: 10.4103/0019-5413.201702.
Notes
Author notes
Corresponding author: Carlos A. Ordonez, MD, FACS. Division of Trauma and Acute Care Surgery, Department of Surgery. Fundación Valle del Lili. Cali, Colombia; Division of Trauma and Acute Care Surgery, Department of Surgery, Universidad del Valle, Cali, Colombia; Universidad Icesi, Cali, Colombia. Email: ordonezcarlosa@gmail.com, carlos.ordonez@fvl.org.co

