Original article
Religiosity, physical and functional health in older people in Chile
Religiosidad, salud física y funcional en personas mayores en Chile
 M Beatriz Fernández Lorca mrfernan@uc.cl
M Beatriz Fernández Lorca mrfernan@uc.cl
Religiosity, physical and functional health in older people in Chile
Colombia Médica, vol. 53, no. 2, e2004846, 2022
Universidad del Valle
Received: 27 April 2021
Revised document received: 01 June 2021
Accepted: 10 April 2022
Funding
Funding source: Agencia Nacional de Investigación y Desarrollo Programa Fondecyt Inicio
Contract number: N°11180287
Funding
Funding source: Iniciativa Científica Milenio
Contract number: ICS2019_024
Funding statement: Agencia Nacional de Investigación y Desarrollo Programa Fondecyt Inicio N°11180287 e Iniciativa Científica Milenio ICS2019_024
Abstract
Objective: To establish the association between different dimensions of religiosity - organizational, non-organizational and intrinsic - and physical and functional health indicators in older people in Chile.
Methods: Data from the Fifth Survey on Quality of Life in Old Age 2019 were used. Descriptive and explanatory analyses were performed using logistic, linear and multinomial regression models, with dependent variables being self-perception of health, functional dependence, number of chronic diseases and perception of health compared with other people of the same age. As predictors, indicators of the three dimensions of religiosity (DUREL Scale) were included, controlling for the MOS-SS Social Support Scale, Apgar Family Functioning Scale, educational level, gender, age, and living with a partner.
Results: Almost a third of older Chileans attend religious services frequently, and half of them pray frequently. On a range of 1 to 5, the mean intrinsic religiosity is 3.94. 46% perceive their health to be good/very good and about half perceive their health as better than their peers. On 0 to 5, the mean number of chronic diseases is 1.69. 6% are classified as functionally dependent. The only significant relationship observed was between religious attendance and a lower probability of presenting functional dependency; on the other hand, praying increases such probabilities and a relationship between attendance and a better perception of health compared with other people of the same age.
Conclusion: Organisational religiosity is a psychosocial resource that is positively associated with the process of successful aging
Keyword: Aged+ quality of life+ family relations+ functional status+ health promotion+ religion+ social support+ health behavior+ life expectancy.
Resumen
Objetivo: Establecer la asociación entre distintas dimensiones de religiosidad - organizacional, no organizacional e intrínseca- y diversos indicadores de salud física y funcional en personas mayores en Chile.
Métodos: Se utilizaron datos de la Quinta Encuesta de Calidad de Vida en la Vejez del 2019. Se realizaron análisis descriptivos y explicativos, utilizando modelos de regresión logística, lineal y multinomial, teniendo como variables dependientes autopercepción de salud, dependencia funcional, número de enfermedades crónicas y percepción de la salud en comparación con otras personas de la misma edad. Como predictores se incluyeron indicadores de las tres dimensiones de religiosidad considerada (Escala DUREL), controlando por Escala de Apoyo Social percibido MOS-SS, Escala de Funcionamiento Familiar de Apgar, nivel educativo, género, edad y vivir con una pareja.
Resultados: Casi un tercio de los mayores chilenos asiste de manera frecuente a servicios religiosos, y la mitad reza frecuentemente. En un rango de 1 a 5, la media de religiosidad intrínseca es de 3.94. Un 46% se percibe con buena/muy buena salud y cerca de la mitad se percibe con mejor salud que otras personas de la misma edad. En un rango de 0-5, la media de enfermedades crónicas es de 1.69 y un 6% es clasificado como dependiente funcional. Solo se encontró una relación significativa entre asistencia religiosa y una menor probabilidad de presentar dependencia funcional, mientras que por el contrario rezar aumenta dichas probabilidades; además de una relación entre asistencia y mejor percepción de salud en comparación con otras personas de la misma edad.
Conclusiones: la religiosidad organizacional es un recurso psicosocial que se asocia positivamente con el proceso del envejecimiento exitoso.
Palabras clave: envejecimiento, calidad de vida, relaciones familiares, estado funcional, promoción de salud, religión, apoyo social, comportamiento de salud, esperanza de vida.
Remark

Introduction
According to the latest Population Census, Chile is one of the countries in the most advanced stage of demographic transition in the region 1, with 16.2% of its population aged 60 and over and an average life expectancy of 80 years (2. This results in a higher prevalence of chronic diseases and social and health care needs, increasing the interest in studying modifiable factors that promote health at this stage of life (3.
In this context, religiosity appears as a psychosocial resource contributing to increased longevity (3,4. Religiosity is a multidimensional construct that primarily involves an organizational dimension (ORA), which refers to participation in religious services or other religious activities. However, it also has a non-organizational dimension (NORA), corresponding to a private expression such as praying, and a third dimension, known as intrinsic (IR), refers to the importance of religion in everyday life 5,6.
There is broad evidence on the link between religiosity and individual health. More specifically, religious people were found to have a lower prevalence of cardiovascular disease and certain types of cancer 7-9. They also have significantly lower mortality rates 9-11. Religious people were also found to have better self-perceived health (12, lower rates of functional impairment and disability (13, and less prevalent health-related behaviors such as smoking, alcohol use, and drug abuse (14,15. This is partially explained by the fact that religion imposes a set of rules not only associated with the ethical behavior of individuals but also with regard to food and drink intake, sexual activity, among other aspects, promoting healthy habits and lifestyles 3,16,17. With enhanced social support networks and a sense of certainty and stability, it is possible to cope effectively with the stressful events that occur throughout life 18, leading to better aging.
In this context, this study aims to establish the association between different dimensions of religiosity and various indicators of physical and functional health in older people in Chile, contributing to the scarce literature on this subject in the region.
Materials and Methods
The data for this study comes from the Fifth Survey on Quality of Life in Old Age 2019 of the Pontificia Universidad Católica de Chile and Caja Los Andes. This survey assesses different dimensions related to the quality of life of older people in Chile, such as physical and health conditions, working conditions, and social and family relationships. It also includes a specific module on religiosity.
The target population of the survey were Chileans aged 60 and over with no symptoms of cognitive impairment, residing in private households in urban localities of 10,000 inhabitants and over. The case selection was multistage, probabilistic, and stratified, with a total margin of error of +/- 2.4%, based on simple random sampling with maximum variance, and representative of about 86% of the total elderly population the country.
The final sample consists of 2,132 people. All respondents participated voluntarily, signing the informed consent form. The study was approved by the Ethics Committee of the Pontificia Universidad Católica de Chile (No. 190829005, 12 September 2019).
In terms of the hypotheses of this study, it is argued that those older people who have higher levels of religiosity in its organizational, non-organizational or intrinsic dimensions will have better physical health and a lower level of functional dependency. More specifically, the dependent variables of this study are the following: i) Perception of health, with responses dichotomised into poor/regular versus good/very good; ii) Perception of health compared to other people of the same age, categorised as worse, same and better; iii) Number of chronic diseases, generated from a checklist that queried the presence of the following diseases: hypertension, high cholesterol, diabetes, arthritis and osteoporosis; iv) Functional dependency; persons are classified as dependent if: a) they report extreme difficulty or inability to perform basic activities (eating, bathing, moving around the house, using the toilet, going to bed/getting out of bed, dressing) or instrumental activities of daily life (going out, shopping/going to the doctor, doing household chores, making/receiving calls), or b) they receive help with high frequency, or c) they present moderate or severe difficulties in at least one basic activity of daily life or two instrumental activities19,20.
Religiosity was measured using the Duke Religiosity Scale (21, which consists of five Likert-type items measuring the three dimensions of religiosity: (i) ORA: frequency of attendance to religious services or participate in other religious activities, dichotomized into infrequent (few times a year or less, never) and frequent (a few times a month, once a week or several times a week); ii) NORA: frequency of praying, studying scripture or meditating, dichotomized into infrequent (a few times a week, a few times a month, never) and frequent (daily or several times a day); iii) IR: How accurate or inaccurate is it for you to: experience the presence of the divine; allow religious beliefs to guide an approach to life; and carry religion into other areas of life, with responses ranging from 1= not true, 5= true. These three items were averaged to create one single indicator.
Additionally, other variables that may be associated with physical and functional health are included, such as i) 8-item MOS-SS (Medical Outcomes Study Social Support Survey) 22, with three possible responses (always= 1; sometimes= 2; never= 3), giving a range of 8 to 24 points (from least to most supportive); ii) Apgar Family Functioning Scale 23, which is a five-item scale with responses ranging from 0 (almost never), 1 (sometimes) and 2 (almost always), which were summed and recoded into two levels: severe or mild family dysfunction (0 to 6 points) and good family functioning (7 to 10 points); Educational level (1=Primary education or less; 2=Secondary education; 3= Higher education); Gender (1= Male; 2= Female); Age; and Living with a partner, where 1= not, and 2= yes.
In terms of the analysis strategy, univariate and bivariate descriptive statistics were first calculated for the variables mentioned above. Data was analyzed using STATA 14 software. Then, different regression models were estimated to examine which variables were most correlated with each of the dependent variables in the study. Based on the measurement level, logistic regression models were estimated for the variables health perception and functional dependence, while a linear regression model was estimated for chronic diseases. In the case of the health perception variable in comparison with other people of the same age, a multinomial logistic regression model was estimated. In all cases, and following the suggestions of the authors of the DUREL scale, the three religiosity subscales were included independently in separate regression models to avoid possible multiple collinearity problems24, followed by the rest of the predictors.
Results
Women account for 67% of the sample, with a mean age of 72 years (SD= 8.2). Almost half of them possess primary education or less versus only 19% with higher education. In addition. 48% of the older people surveyed are living with a partner. With regard to the health variables, 46% perceive themselves to be in good or very good health and about half perceive themselves to be in better health than other people of the same age. In a rank of 0-5, the mean number of chronic diseases is 1.69 (SD= 1.3), and 6% of the respondents are classified as functionally dependent.
As for the religiosity variables, almost a third of the elderly reported frequent attendance to religious services, while half of them reported praying frequently. On a rank of 1 to 5, the mean of intrinsic religiosity is 3.94 (SD= 1.01).
The MOS-SS scale has a mean of 21.65 (SD= 4.22), suggesting that respondents perceive high levels of social support, with four out of five reporting good family functioning.
Bivariate relationships (Table 1 and 2) show that frequent attendance to religious services is positively associated with a better perception of health when compared to people of the same age and with lower levels of functional dependency. Frequent praying is associated with a higher number of diseases and greater dependency and a better perception of health than others. The intrinsic dimension is negatively related to health perception and positively associated with the number of diseases, although it is positively associated with a better comparative perception of health.
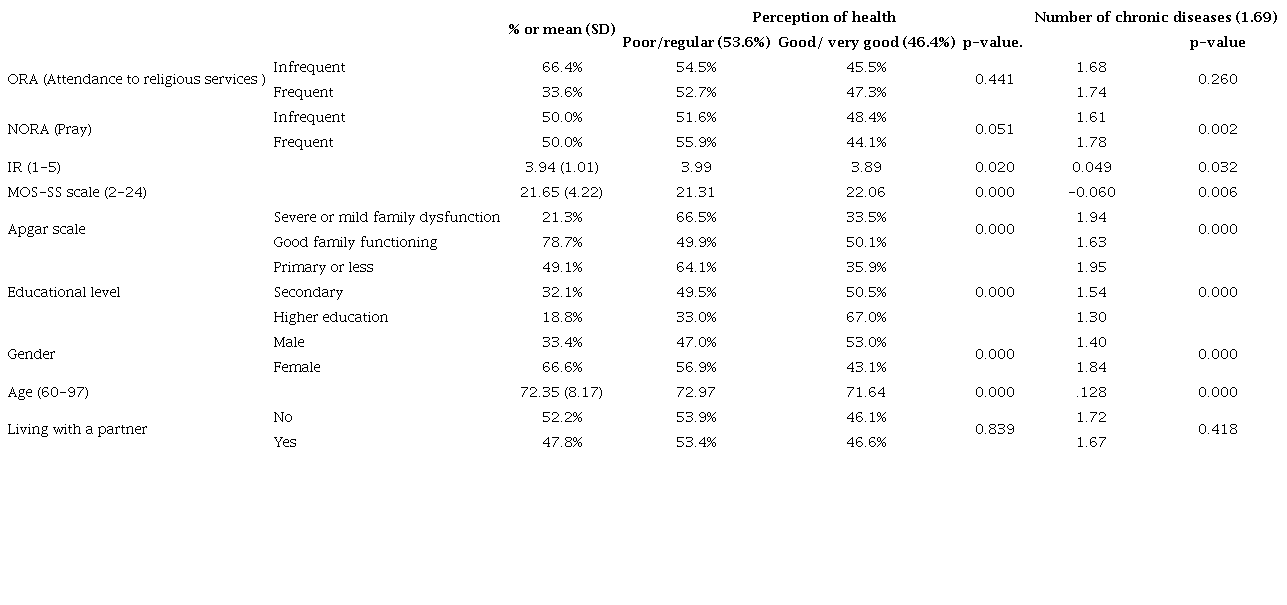
Note: The association between nominal variables was calculated using chi-square; association between nominal and scalar variable was calculated with the t test for independent samples; association between ordinal or scalar variables was calculated using the R-Pearson correlation.

Note: The association between nominal variables was calculated using chi-square; association between nominal and scalar variables was calculated with the t-test for independent samples; association between ordinal or scalar variables was calculated using the R-Pearson correlation.
The greater the social support and the better the family functioning, the better the perception of general and comparative health, as well as the lower the number of diseases. People with a higher level of education show better health conditions for all the variables included. On the contrary, being a woman is associated with worse health conditions, except for the dependency variable, which is not significant. In turn, the older the age, the worse the self-perception of health, the greater the number of diseases and the greater the dependency. As for living with a partner, is associated with lower levels of dependency at the bivariate level only.
Tables 3 y 4 shows the results of several estimated regression models. Once all predictor variables are controlled for in a single model, several previously noted bivariate relationships become weaker.
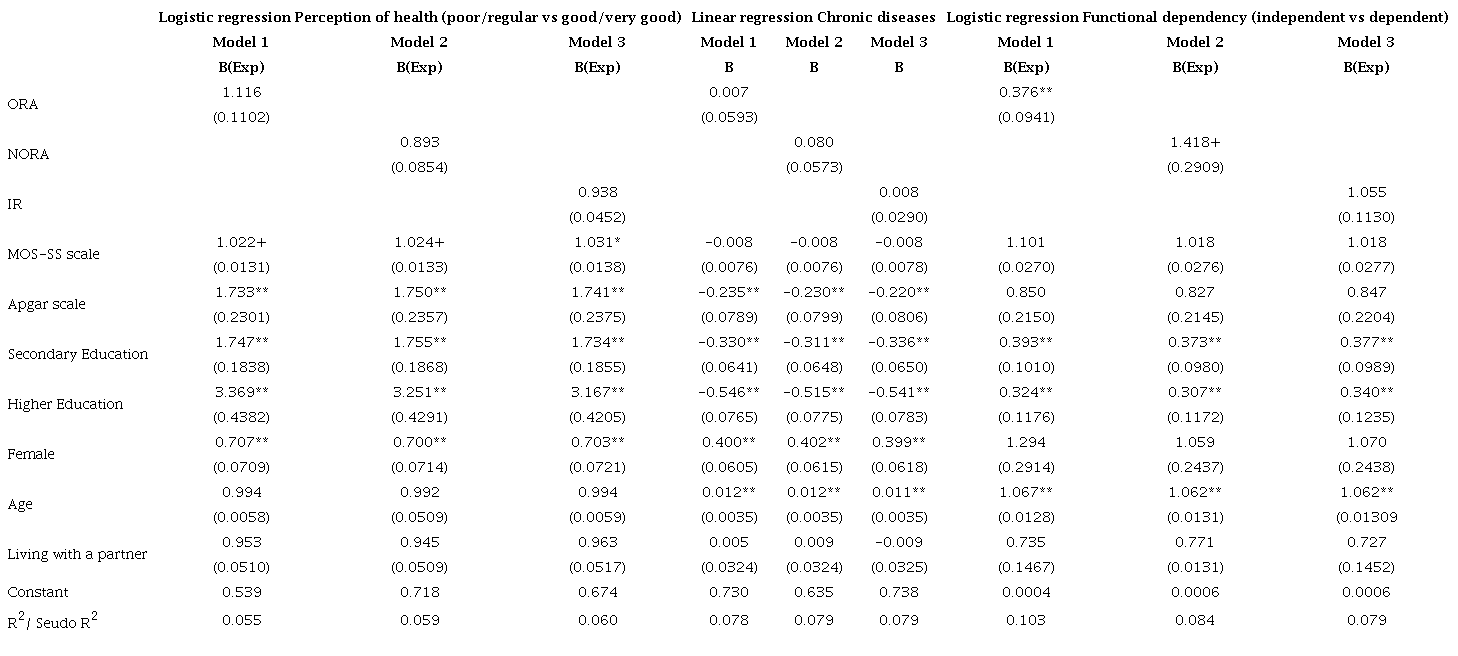
** p <0.01; *p <0.05; +p <0.10
** p <0.01; *p <0.05; +p <0.10
More precisely, in the logistic regressions of the Perception of health variable, it can be observed that none of the religiosity indicators are statistically significant. In these three models, it is found that having a good family functioning and having higher levels of education, increases the likelihood of perceiving oneself to be in good/very good health (Model 1: OR = 1.733, p <0.01, CI 95%: 1.336-2.248) and ORhigher_educ =3.369, p <0.01, CI 95%: 2.611-4.347); Model 2: OR= 1.750, p <0.01, CI 95%: 1.344-2.279 and ORhigher_educ= 3.251, p <0.01, CI 95%: 2.510-4.211; Model 3: OR = 1.741, p <0.01, CI 95%: 1.332-2.275 and ORhigher_educ= 3.167 p <0.01, CI 95%: 2.441-4.109). Being a woman, on the other hand, is associated with a lower likelihood of perceiving oneself to be healthy (Model 1: OR= 0.707, p <0.01, CI 95%: 0.581-0.861; Model 2: OR= 0.700, p <0.01, CI 95%: 0.573-0.855; Model 3: OR= 0.703, p <0.01, CI 95%: 0.575-0.860).
For the Chronic Diseases variable, neither are the religiosity variables significant. As for the other predictors, good family functioning and higher levels of education reduce the number of chronic diseases held (Model 1: B= -0.235, p <0.01, CI 95%: -0.390- -0.080 and Bhigher_educ= -0.546, p <0.01, CI 95%: -0.696- -0.396; Model 2: B= -0.230, p <0.01, CI 95%: -0.387- -0.073 and Bhigher_educ= -0.515, p <0.01, CI 95%: -0.667- -0.363; Model 3: B= -0.220, p <0.01, CI 95%: -0.378- -0.062 and Bhigher_educ= -0.541, p <0.01, CI 95%: -0.695- -0.387), while being a woman and being older increase this number (Model 1: B= 0.400, p <0.01, CI 95%: 0.281-0.519 and B= 0.012; p <0.01, CI 95%: 0.005-0.019; Model 2: B= 0.402, p <0.001, CI 95%: 0.282-0.523 and B= 0.012; p <0.01, CI 95%: 0.005-0.019; Model 3: B= 0.399, p <0.01, CI 95%: 0.272-0.521 and B= 0.011; p <0.01, CI 95%: 0.004-0.018).
For the Functional Dependence variable, the ORA indicator decreases the likelihood of presenting dependency, while NORA increases it to a lower level of statistical significance (Model 1: OR= 0.376, p <0.01, CI 95%: 0.230-0.614 and Model 2: OR= 1.418, p <0.10, CI 95%: 0.948-2.120). It is also observed that the higher the education, the lower the probability of presenting dependency (Model 1: ORhigher_educ= 0.324, p <0.01, CI 95%: 0.159-0.660; Model 2: ORhigher_educ= 0.307, p <0.01, CI 95%: 0.145-0.649; Model 3: ORhigher_educ= 0.340, p <0.01, CI 95%: 0.167-0.693), while the older the age, the greater such likelihood (Model 1: OR= 1.067, p <0.01, CI 95%: 1.042-1.093; Model 2: OR= 1.062, p <0.01, CI 95%: 1.037-1.088; Model 3: OR= 1.062, p <0.01, CI 95%: 1.037-1.088).
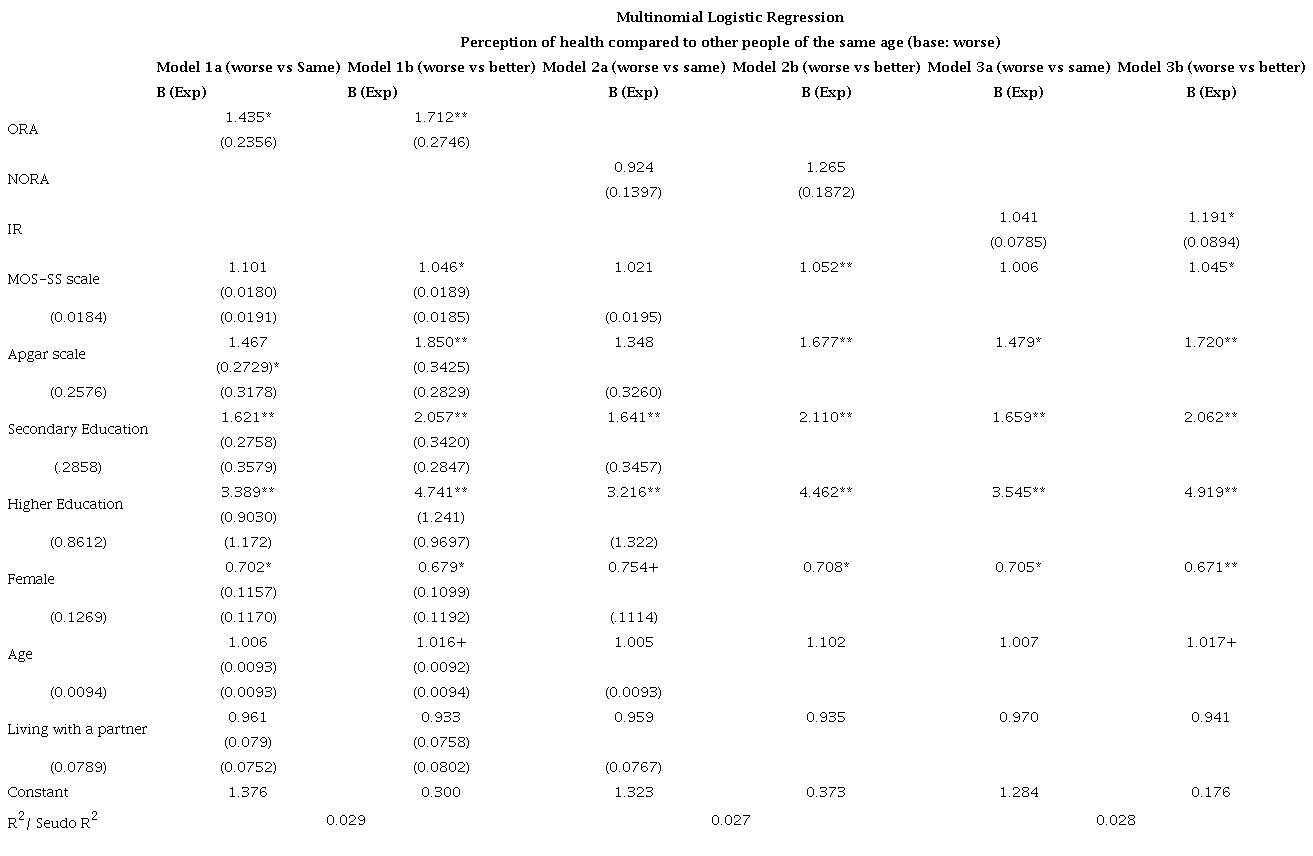
Finally, in relation to the model of Health Perception in Comparison with other people of the same age, it is found that ORA increases the likelihood of perceiving oneself to be in equal or better health (Model 1a: OR= 1.435, p <0.05, CI 95%: 1.040-1.979 and Model 1b: OR= 1.712, p <0.01, CI 95%: 1.250-2.344), while that IR increases the likelihood of perceiving oneself to be better health (Model 3b: OR= 1.191, p <0.05, CI 95%: 1.028-1.379). In the models of worse vs. better comparative health, the higher the social support, better family functioning and higher education, the higher the likelihood of perceiving oneself to be in better health than one's peers (Model 1b: OR= 1.046, p <0.05, CI 95%: 1.009-1.084; OR= 1.850, p <0.01, CI 95%: 1.287-2.660; ORhigher_educ= 4.741, p <0.05, CI 95%: 2.384-7.920; Model 2b: OR= 1.052, p <0.01, CI 95%: 1.016-1.091; OR= 1.677, p <0.01, CI 95%: 1.156-2.431; ORhigher_educ= 4.462, p <0.05, CI 95%: 2.667-7.467; Model 3b: OR= 1.045, p <0.05, CI 95%: 1.008-1.084; OR= 1.720, p <0.01, CI 95%: 1.186-2.494; ORhigher_educ= 4.919, p <0.01, CI 95%: 2.904-8.332), while being a woman is associated with a lower likelihood of being in better health than one's peers (Model 1b: OR= 0.679, p <0.05, CI 95%: 0.494-0.932; Model 2b: OR= 0.708, p <0.05, CI 95%: 0.512-0.979; Model 3b: OR= 0.671, p <0.01, CI 95%: 0.484-0.929).
Discussion
As stated by the World Health Organisation, psychosocial aspects of health and quality of life are relevant elements for assessing and promoting health. In this context, religiosity appears as a resource that could positively affect both the physical and mental health of the older population, thereby promoting successful ageing 14.
Thus, this study aimed to establish the association between religiosity - understood as a multidimensional concept - and various physical and functional health indicators in older people in Chile. The evidence suggests that the relationship between religiosity and health in the elderly population does indeed vary according to the dimension of religiosity being considered. It also varies according to the health indicator used, suggesting that the relationship between these variables is rather complex. The findings of this study, therefore, do not support the hypothesis that older people who are more religious in the organizational, non-organizational and intrinsic dimensions have better indicators of physical and functional health. Rather, the results show that this relationship is significant only for some of the dimensions of religiosity included and some of the health indicators measured.
More precisely, a significant relationship was found between ORA and a lower likelihood of functional dependency, while NORA increases the likelihood of functional dependence, which is consistent with other studies 13,16,25,26. The protective effect of religious attendance is explained by its association with better health practices, higher numbers of social contacts, and physical activity 27,28. This social support and physical engagement is ultimately associated with a delay in the onset and aggravation of disability (29.
In the case of NORA, the association with the dependency indicator can possibly be explained by the endogeneity effect between the two variables. In particular, as physical functioning worsens, praying becomes a coping and comfort-seeking resource 26. In doing so, people with greater functional limitations may be more likely to engage in private religious activities to cope with their disabling conditions 30. Conversely, declining health and increasing functional dependency would lead to a fall in attendance to religious services 3,25,31,32. Future studies may help to shed light on the directionality of these relationships.
Furthermore, this study also found a relationship between ORA and a better perception of health compared to other people of the same age. This could be explained by the fact that religious participation provides people with more regular opportunities to see their friends and to show others that they are physically well (28. Likewise, greater attendance is positively related to greater optimism, gratitude and better self-concept 33, which would imply a better comparative perception of one's health. Following this idea, it should also be noted a positive relationship was found between IR and a better perception of health compared to peers. Intrinsic religiosity involves the sincere and intentional integration of religion into one’s life24, acting as an organizing and motivating force, which in turn would allow for more optimistic life orientation34. People with higher levels of spirituality usually find greater meaning and one’s purpose of existence35, what it could better the auto perception of one´s own life conditions, included the health.
Finally, it should be noted that this study also confirms that having certain social and personal resources - in terms of availability of support, good quality of family relationships, and higher levels of education - predict better physical and functional health of older people. Similarly, being a woman and older is associated with poorer health conditions in old age, which is consistent with previous literature (36,37.
Conclusion
Organizational religiosity is a psychosocial resource that is positively associated with the process of successful ageing.
From the above, it becomes important to promote different actions to facilitate the religious participation of older people, considering the heterogeneity of this group, insofar as this - as well as other types of social participation - is a resource that protects better aging.
References
Huenchuan S. Envejecimiento, personas mayores y agenda 2030 para el desarrollo sostenible: perspectiva regional y de derechos humanos. Comisión Económica para América Latina y el Caribe (CEPAL); 2018. Available from: https://www.cepal.org/sites/default/files/publication/files/44369/S1800629_es.pdf
Comisión Económica para América Latina y el Caribe. Estimaciones y proyecciones de población total, urbana y rural, y económicamente activa. Comisión Económica para América Latina y el Caribe; 2019. Available from: https://www.cepal.org/es/temas/proyecciones-demograficas/america-latina-caribe-estimaciones-proyecciones-poblacion
Zimmer Z, Jagger C, Chiu C, Ofstedal M, Rojo F, Saito, Y. Spirituality, religiosity, aging and health in global perspective: A review. SSM Popul Health. 2016;2: 373-381. doi:10.1016/j.ssmph.2019.100441
Koenig H. Research on religion, spirituality, and mental health: a review. Can J Psychiatry. 2009;54(5): 283-291. doi:10.1177/070674370905400502
Futterman A, Koenig H. Measuring religiosity in later life: What can gerontology learn from the sociology and psychology of religion?. Conference on Methodological Approaches of the study of religion, aging, and health. Bethesda, Maryland. NIA and Fetzer Institute; 1995.
Koenig H. Spirituality, wellness, and quality of life. Sexuality Reproduc Menopause. 2004;2(2):76-82. doi:10.1016/j.sram.2004.04.004.
Li S, Stampfer M, Williams D, VanderWeele T. Association of religious service attendance with mortality among women. JAMA Intern Med. 2016;176(6):777-785. doi:10.1001/jamainternmed.2016.1615
Cohen A, Koenig H. Religion, religiosity and spirituality in the biopsychosocial model of health and ageing. Ageing International. 2003;28(3): 215-241. doi:10.1007/s12126-002-1005-1
Hill T, Burdette A, Ellison C, Musick M. Religious attendance and the health behaviors of Texas adults. Prev Med. 2006;42: 309-312. Doi:10.1016/j.ypmed.2005.12.005
Chida Y, Steptoe A, Powell LH. Religiosity/spirituality and mortality. A systematic quantitative review. Psychother Psychosom. 2009;78(2):81-90. doi:10.1159/000190791
McCullough M, Hoyt W, Larson D, Koenig H, Thoresen C. Religious involvement and mortality: a meta-analytic review. Health Psychol. 2000;19(3):211-22. doi:10.1037/0278-6133.19.3.211
Reyes-Ortiz C, Payan C, Altamar G, Gómez F, Koenig H. Religiosity and self-rated health among older adults in Colombia. Colomb Med (Cali). 2019;50(2):67-76. doi:10.25100/cm.v50i2.4012
Amorim D, da Silveira C, Alves V, Faeiro V, Coelho K. Association between religiosity and functional capacity in older adults: a systematic review. Rev Bras. Geriatr Gerontol. 2017;20(5):722-730. doi:10.1590/1981-22562017020.170088
Ahrenfeld L, Möller S, Hvidt N, Lindahl-Jacobsen R. Religiousness and lifestyle among Europeans in SHARE. Public Health. 2018;165:74-81. doi:10.1016/j.puhe.2018.09.009
Deaton A. Aging, religion, and health. Working Paper 15271. National Bureau of Economic Research. 2016. doi:10.3386/w15271
Idler E, Kasl S. Religion among disabled and nondisabled persons: Cross-sectional patterns in health practices, social activities, and well-being. J Gerontol B Psychol Sci Soc Sci. 1997;52(6): S294-S305. doi:10.1093/geronb/52B.6.S294
Svensson N, Hvidt N, Nissen S, Storsveen M, Hvidt A, Sondergaard J, Thilsing T. Religiosity and health-related risk behaviours in a secular culture-is there a correlation? J Relig Health. 2020;59: 2381-2396. doi:10.1007/s10943-019-00919-2
Fernández MB, Valenzuela E. Religiosity and subjective wellbeing of the elderly in Chile: A mediation analysis. J Religion Spirituality Aging. 2020; 34(1): 17-38. doi:10.1080/15528030.2020.1839624
Katz S, Ford A, Moskowitz R, Jackson B, Jaffe M. Studies of Illness in the Aged. The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA. 1963; 21(185): 914-919. doi:10.1001/jama.1963.03060120024016
Lawton M, Brody E. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969; 9(3):179-186. doi: 10.1093/geront/9.3_Part_1.179
Koenig H, Parkerson G, Meador K. Religion index for psychiatric research. Am J Psychiatry. 1997;154(6): 885-886. doi:10.1176/ajp.154.6.885b
Moser A, Stuck AE, Silliman RA, Ganz PA, Clough-Gorr KM. The eight-item modified Medical Outcomes Study Social Support Survey: psychometric evaluation showed excellent performance. J Clin Epidemiol. 2012;65(10):1107-16. doi: 10.1016/j.jclinepi.2012.04.00
Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. 1978; 6(6): 1231-9.
Koenig H, Büssing A. The Duke University Religion Index (DUREL): A five-item measure for use in epidemiological studies. Religions. 2010;1: 78-85. doi: 10.3390/rel1010078
Koenig H, King D, Carson V. Handbook of religion and health. 2nd ed: Oxford University Press; 2012.
Haley K, Koenig H, Bruchett B. Relationship between private religious activity and physical functioning in older adults. J Religion Health. 2001;40: 305-312. doi:10.1023/A:1012561909054
Hybels C, Blazer D, George L, Koenig H. The complex association between religious activities and functional limitations in older adults. Gerontologist. 2012;52(5):676-85. doi: 10.1093/geront/gnr156
Park N, Klemmack D, Roff L, Parker M, Koenig H, Sawyer P, Allman R. Religiousness and longitudinal trajectories in elders' functional status. Res Aging. 2008;30(3):279-298. doi: 10.1177/0164027507313001
Koenig H. Religion, spirituality, and medicine: research findings and implications for clinical practice. South Med J. 2004;97(12):1194-200. doi: 10.1097/01.SMJ.0000146489.21837.CE
Zimmer Z, Chiu C, Saito Y, Jagger C, Ofstedal M, Lin Y. Religiosity dimensions and disability-free life expectancy in Taiwan. J Aging Health. 2020;32(7-8):627-641. Doi:10.1177/0898264319843445
Wang K, Kercher K, Huang JY, Kosloski K. Aging and religious participation in late life. J Relig Health. 2014;53(5):1514-28. doi: 10.1007/s10943-013-9741-y.
Valenzuela E. Importancia de la religión en el envejecimiento. En Larraín F, Marín PP, Valenzuela,. Cómo vivir bien 100 años. Santiago: Ediciones UC; 2016. p. 315-327.
Sowa A, Golinowska S, Deeg D, Principi A, Casanova G, Schulmann K, Ilinca S, Rodrigues R, Moreira A, Gelenkamp H. Predictors of religious participation of older Europeans in good and poor health. Eur J Ageing. 2016;13(2):145-157. doi: 10.1007/s10433-016-0367-2
Hornby-Turner Y, Peel N, Hubbard R. Health assets in older age: a systematic review. BMJ Open 2017;7:e013226. doi:10.1136/bmjopen-2016-013226
Susanti I, Latuperissa G, Soulissa F, Fauziah A, Sukartini T, Indarwati R, Aris A. The factors associated with successful aging in elderly: a systematic review. Journal Ners, 2020: 230-237. doi: 10.20473/jn.v15i2.19019
Hornby-Turner Y, Peel N, Hubbard R. Health assets in older age: a systematic review. BMJ Open. 2017;7:e013226. doi:10.1136/bmjopen-2016-013226
Susanti I, Latuperissa G, Soulissa F, Fauziah A, Sukartini T, Indarwati R, Aris A. The Factors Associated with Successful Aging in Elderly: A Systematic Review. Journal Ners, 2020: 230-237. doi: 10.20473/jn.v15i2.19019
Notes:
Author notes
Corresponding author: M Beatriz Fernández Lorca. E-mail: mrfernan@uc.cl
Conflict of interest declaration