Artículos
Art-based Assessment of Disease Experiences in Children and Adolescents with Cancer: Cognitive and Emotional Dimensions
Evaluación basada en arte de las experiencias de la enfermedad en niños y adolescentes con cáncer: Dimensiones cognitiva y emocional
Art-based Assessment of Disease Experiences in Children and Adolescents with Cancer: Cognitive and Emotional Dimensions
Revista Interamericana de Psicología/Interamerican Journal of Psychology, vol. 56, núm. 3, pp. 1-22, 2022
Sociedad Interamericana de Psicología

Esta obra está bajo una Licencia Creative Commons Atribución 4.0 Internacional.
Recepción: 01/04/2022
Aprobación: 02/09/2022
Abstract: This study assessed the disease experiences in children and adolescents with cancer through an art-based assessment. It used a longitudinal qualitative research design with inductive content analysis. The study included twenty children (6-17 years old) diagnosed with cancer from the Hospital de Especialidades Pediatricas, Maracaibo, Venezuela. The art-based assessment program consisted of 7 individual sessions in which self-image, family relationships, disease perception, child's experiences at the hospital, concerns about the disease and treatment, and positive feelings were evaluated through art exercises. Two main categories emerged from the analysis: (1) Cognitive Dimension, related to awareness and concerns regarding the disease and treatment, as well as patients' ability to take responsibility for their health, and (2) Emotional Dimension, which covers the positive emotional states, such as fighting spirit, affection towards others, happiness, and hope, along with the negative emotional states which include sadness, anxiety-fear, and anger. The results of this research support previous findings indicating that art-based assessment is a valid and effective tool to evaluate thoughts and emotions in children and adolescents with cancer.
Keywords: children, adolescents, art-based assessment, cancer, experiences.
Resumen: Este estudio evaluó las experiencias de la enfermedad en niños y adolescentes con cáncer a través de una evaluación basada en el arte. Utilizó un diseño de investigación cualitativa longitudinal con análisis de contenido inductivo. El estudio incluyó a veinte niños (6-17 años) diagnosticados con cáncer del Hospital de Especialidades Pediátricas, Maracaibo, Venezuela. El programa de evaluación basado en arte consistió en 7 sesiones individuales en las que se evaluaron la autoimagen, las relaciones familiares, la percepción de la enfermedad, las experiencias del niño en el hospital, las preocupaciones sobre la enfermedad y el tratamiento, así como, los sentimientos de bienestar. Dos categorías principales surgieron del análisis: (1) Dimensión cognitiva, relacionada con la conciencia de la enfermedad y las preocupaciones con respecto a esta y al tratamiento, así como la capacidad de los pacientes para asumir la responsabilidad de su salud, y (2) Dimensión emocional, que abarca los estados emocionales positivos, como el espíritu de lucha, el afecto hacia los demás, la felicidad y la esperanza, junto con los estados emocionales negativos que incluyen tristeza, ansiedad-miedo e ira. Los resultados de esta investigación respaldan hallazgos previos que indican que la evaluación basada en el arte es una herramienta válida y efectiva para evaluar los pensamientos y las emociones en niños y adolescentes con cáncer.
Palabras clave: niños, adolescentes, arte, cáncer, experiencias.
Introduction
Pediatric cancers are complex diseases that impact multiple aspects of a child's life. Therefore, these diseases require a systematic approach that takes into account the patient's physical, psychological, and social well-being. A multidisciplinary team should ideally conduct such an approach to provide optimal attention and care, improving the patient's quality of life (Marcus, 2012). In 2018, cancer affected 200,166 children under 14 years of age globally, with 74,956 deaths reported in this age range (Ferlay et al., 2018). It was estimated that 1,323 children and adolescents were diagnosed with cancer in Venezuela, and 421 cancer-related deaths occurred among children under 15 years of age (Ferlay et al., 2018). Current data suggest that children's survival rate is much lower in low-income and middle-income countries than in high-income ones (Allemani et al., 2018). This situation applies to Venezuela, where appropriate and timely diagnosis and integral treatment of cancer patients are often sub-optimal. This situation requires planning and executing programs that address the physical and psychological symptoms of the disease, as well as treatments side effects.
The most common physical symptoms reported in children and adolescents with cancer are pain, fatigue, vomiting, nausea, and diarrhea, which force patients to rest or lay down, preventing them from going to school and engaging in the activities they used to do before the diagnosis (Enskar et al., 2014). Furthermore, these children face psychological symptoms such as sadness, caused by thoughts and experiences associated with the condition and its treatment (isolated hospitalization, death of other kids at the hospital); anxiety related to painful medical procedures; and anger, as a consequence of the physical changes caused by the treatment. (Enskar et al., 2014). All of this involves profound life changes as the disease plays a dominant role in which now the time is increasingly spent at the hospital, and leisure and learning activities cannot be pursued as before, adding to the child's stress. Accessing the inner world of children and adolescents with cancer and assessing their experiences and needs is often difficult, especially in the youngest patients, who have limited ability to communicate thoughts and emotions due to their early cognitive development and reduced vocabulary (Aguilar, 2017). Moreover, young patients may not freely express their emotions because they feel guilty about being sick or do not want to increase parental anxiety (Gibson et al., 2010).
Within the mental health field, art therapy is one of the tools that allows evaluation of the disease experience in a more pleasant, less threatening way. It permits exploring a person's inner world through artistic expressions without the need of words (Malchiodi, 2005). Research has shown that the use of art as an evaluation/intervention tool in pediatric oncology settings can effectively assess children's self‑perception and their relationships with others (Sadruddin & Hameed Ur Rehman, 2013). It can also improve emotional expression and communication about the disease, contribute to develop patient's coping skills, reduce symptoms, enhance well-being (Aguilar, 2017), decrease depression (Tahmasebi et al., 2017), and reduce anxiety levels (Altay et al., 2017). However, despite advances that reflect its numerous benefits, art therapy is still a tool that needs to be more widely promoted and used to accurately meet the needs of the young cancer population. Currently, available studies on art-based assessment and its benefits in pediatric oncology patients are scarce. This kind of evaluation is based on the formal art therapy assessment that uses art processes such as drawing, sculpting, painting, and collage to evaluate the psychosocial aspects of children (Gantt, 2011). New research is needed to demonstrate the applicability and usefulness of art-based assessments in exploring the experiences of children and adolescents with cancer. Therefore, the present study aimed to assess disease experiences in children and adolescents with cancer through an art-based program and to provide an account of the cognitive and emotional dimensions unmasked by this approach.
Method
Participants
The study was carried out at the Pediatric Specialties Hospital in Maracaibo, Venezuela. It included 20 patients (6-17 years old) diagnosed with cancer and at any stage of their cancer journey (i.e., diagnostic phase, treatment phase, relapse, and up to 6th months after completing successful treatment). The inclusion criteria were a) cancer diagnosis; b) age between 6 and 17 years. The wide age range was selected to ascertain the disease experiences of both children (6-12 years) and adolescents (13-17 years), and c) sufficient knowledge of the Spanish language to participate in the study; Patients were invited to participate. All patients who expressed their willingness to participate in the study met the set criteria. Parents or legal guardians provided written consent, and assent was obtained from participating children. Patients' mean age was 12 ± 3.5 years (mean ± SD), most of them were girls (75%), and most of the participants (95%) had a low socioeconomic level. Most patients (70%) had been diagnosed with acute lymphoblastic leukemia and were receiving chemotherapy (95%) when the study was performed. Sociodemographic and clinical characteristics of the patients included in the study are shown in Table 1 and Table 2, respectively.
Design
This study was a longitudinal qualitative research design with inductive content analysis.
Procedures
Art-based Assessment Program
The art-based assessment program explored the children's experiences regarding cancer through art processes such as drawing, sculpting, painting, and mask making. It consisted of 7 sessions over six months where a series of artworks were collected to ensure the value of artwork variability and obtain a more thorough insight into patients' experiences. As it has been stated, the timing of works' collection in art-based assessments is critical because if the collection is limited to only one art product, this may show just a specific response facing a particular moment (Gantt, 2011). Having a higher quantity of artworks from each patient allows a more systemic and complete assessment of the patient's experiences.
The art-assessment was conducted by a clinical psychologist with training in psycho-oncology. She is an art therapy specialist with more than eight years of experience in the psychosocial oncology setting.
In most cases, sessions were conducted on the same day as the patient's medical appointment (one per month) since attendance frequency was restrained due to the families' financial limitations and deficiencies in the public transportation system.
One-hour sessions were carried out individually, usually at the pediatric psycho-oncology office, or in the case of hospitalized children, in the patient's room. Child-centered techniques were used to establish rapport between the child and the researcher (Donalek, 2005). All sessions were audio-recorded and later transcribed. In the first session, parents were asked to fill out the questionnaire on demographic data.
The Human Figure Drawing Test and Family Test were applied as part of the first two sessions.
Human Figure Drawing Test
This test assesses the patient's self-image and emotional reactions (Machover, 1953). The self-image expressed through the drawing reflects the patient's own perception and their relationship with the environment (Escribano, 1977). The instruction provided was Draw a whole person.
Family Test
This test evaluates how relationships between family members are perceived and how the child is included in the family system (Corman, 1961). The instruction for this activity was, Draw a family that you imagine. To better preserve the drawings' meaning and better capture their experiences' reflection, the children were invited to give verbal descriptions about their drawings (Altay et al., 2017; Angell & Alexander, 2015; Malchiodi, 1998).
In the following five program sessions, a subject related to body image, disease perception, experience at the hospital, feelings towards the disease and treatment, and positive feelings were addressed through art exercises. Field notes (Phillippi & Lauderdale, 2017) were made during all sessions, which included describing the patients' behavior, body language, and gestures during the artistic activity carried out by the child. Notes were taken in the most detailed, concrete, and objective way possible. Subsequently, these notes were transcribed into a narrative text to be later codified. In each session, after finishing an artwork, resulting in a visual, tangible product that reflects the patient's subjective experience, patients were invited to share the meaning of their artistic production, allowing the researcher to gain a better understanding of the underlying experiences.
Data analysis
Each session was transcribed and analyzed using content analysis. A detailed reading was made of each session's transcription, reflecting on what might be relevant concerning the experience described so that a general idea of the meaning was obtained. At the same time, notes and memos were produced as tentative ideas for future categorization. The words, phrases, or paragraphs that contained significant aspects of the experiences of the disease were underlined and identified as "units of meaning" (Graneheim & Lundman, 2004). Likewise, units of meaning, represented by characteristics specified in the projective tests (Corman, 1961; Escribano, 1977; Machover, 1953), were identified and assigned a code. Finally, the rest of the artworks were analyzed following Malchiodi's (1998) precepts, which suggest that children's drawings must be analyzed holistically, allowing the evaluation of several topics of interest rather than isolated characteristics within a specific test.
Ninety artworks were analyzed using Atlas.ti 8 software. Each artwork was photographed and using the mentioned software, specific characteristics (units of meaning) relevant to the study were selected. A total of 465 units of meanings were identified from the analysis of 190 documents (sessions' transcriptions, projective tests, and artworks). Subsequently, codes were assigned to units of meaning, and 178 codes were initially identified. Some of these codes were revised, and those that were inclusive (i.e., expressed the same meaning) were grouped into a single code. From the resulting 130 codes, the categories on which this study is based on were established. Different codes were assigned to different categories, considering: (1) Cognitive dimension: related to awareness, knowledge, and concerns regarding the disease and treatment, as well as patients' ability to take responsibility for their health; (2) Emotional dimension: positive emotional states and negative emotional states; (3) Physical dimension: issues related to the patient's physical symptoms, and side effects of treatment; (4) Family dimension: associated with the patient's family needs and family relationships; and (5) Social dimension: related to the patient's interrelations and social needs. Due to the extent of this research project, only the cognitive and emotional dimensions are discussed herein.
Ethical considerations
We followed the Universal Declaration of Ethical Principles for Psychologists (IAAP & IUPsyS, 2008) and the International Ethical Guidelines for Biomedical Research Involving Human Subjects (CIOMS, WHO & PAHO, 2016). The study was approved by the Bioethics Committee of the Pediatric Specialties Hospital.
Results
Our research results are presented considering the categories (dimensions) and main themes that emerged from our analysis. For each dimension, the characteristics found in the artworks and/or exemplifying quotations assigned to each theme are presented.
Cognitive Dimension
Disease and treatment awareness
Patients' awareness of their disease was expressed by the basic knowledge they had about their condition. This allowed them to understand better the disease and the process they face. Likewise, treatment awareness implied handling of basic aspects of the medical or surgical procedures they endured. This was expressed through graphic representations of cancer and drawings of scenes associated with medical procedures and medical appointments. Adolescents' explanations were more elaborated, including information about their diagnosis, medical test results, and treatment regimes. In turn, their artworks showed more realistic graphic compositions and more detailed descriptions of the parts of the body affected by cancer (see Figure 1).
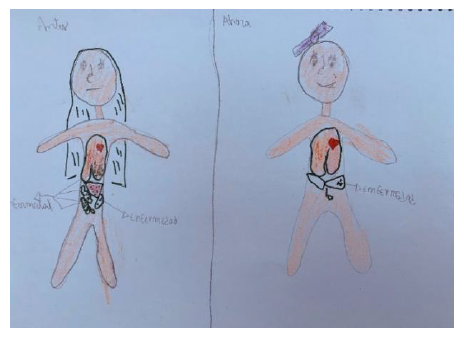
Figure 1
Disease representation (Girl, 16-year-old)
As expected, younger children's verbal descriptions were more concrete and allowed them to share why they were at the hospital and the type of treatment they were receiving.
Here (pointing to the drawing) they give me a lumbar puncture (Boy, 11-year-old).
They give me a blood transfusion here (pointing to the drawing) (Girl, 6-year-old).
Young children's art representations were more rudimentary, using lines and geometric figures, and lacked, in most cases, space perspectives or details about cancer body locations.
Predictably, how children and adolescents expressed awareness about disease and treatment was associated with the cognitive development stage for each group of age.
Of note, we found that open communication between the health professional and the patient (e.g., explaining the reasons for a medical procedure) played a facilitatory role in treatment acceptance and adherence.
I am calmer, I didn't want to be hospitalized, but now that the doctor explained it to me, I understand that it is necessary (Girl, 13-year-old).
Self-image Concerns
This section covers concerns about self-image in adolescent patients. The need to look physically attractive was an important aspect expressed by teenagers while they were drawing themselves. They also reported concerns about treatment side-effects, such as hair and weight loss, which affected their image of themselves and generated concerns about how they were seen by their peers. That was represented through drawings of bald and very thin patients.
I'm lanky; I look ugly in this drawing (Girl, 16-year-old).
I am completely bald here (pointing to the drawing) (Girl, 15-year-old).
One of the coping strategies used by the adolescents in the study was concealment, as they expressed the need to use wigs as a way to socially hide the disease or its effects, and thus avoid attracting attention or being bothered or questioned for looking different.
I want a wig for the school picture (Girl, 15-year-old).
Ability to take responsibility
This theme covers indicators of patients' ability to take responsibility from an early age. Artworks showed completion of basic activities that the patient must carry out, such as preparing food, taking care of their health when caregivers are not present, being vigilant about treatment adherence, and attending medical consultations. Exercising responsibility by following medical indications could suggest patients' personal growth due to the experience of the disease and a sense of control that helps to decrease anxiety.
I have to prepare breakfast because my mother is going to work (Girl, 8-year-old).
I need a watch (showing her clay artwork) to know at what time I have to take medicine, …I have to prepare my food (Girl, 14-year-old).
I told my mother that we must not miss the medical appointment (Girl, 13-year-old).
Emotional Dimension
Positive Emotional States
These include positive feelings associated with the patient's well-being, such as fighting spirit, affection towards others, happiness, and hope.
Fighting Spirit
This theme relates to the patient's will to face the disease and recover their health. A fighting spirit seemed to help patients to maintain positive feelings and to better cope with sadness and hopelessness.
…but do not get depressed, many of us do it and you can't, you have to continue (Girl,16-year-old).
I am delivering bread (showing his clay artwork) to the bakeries, and I am happy.
If I am happy, I can fight the bad cells (Boy, 11-year-old).
In the same way, artworks carried out by patients who had completed treatment reflected the desire to fight and resume life. This can be seen as a won battle that leads to joy and personal satisfaction (see Figure 2).
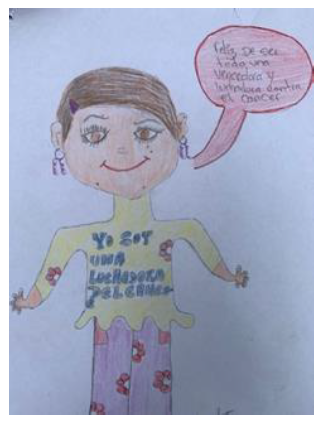
Figure 2
Fighting spirit representation: I am a cancer fighter (Girl,16-year-old)
Affection towards others
Affection towards family members, peers, friends from school, and those going through a similar disease experience at the hospital constitutes a positive emotion that promotes patient well-being. This was expressed through representations of family members and friends in drawing scenes. When the affection is focused on patients facing a similar situation, it may seem that feelings of empathy and compassion towards the other are present to channel the patient's own concerns about the disease. On the other hand, when this affection is directed toward people outside the hospital environment, this positive emotion would be a motivating factor that enforces the desire to resume the life they had before they were ill.
Feelings of happiness
Patients' feelings of happiness were mainly represented through artworks depicting recreational and sporting activities. Despite the difficult circumstances faced by children with cancer during treatment or hospital stays, they expressed the need to play and enjoy making art projects. In this study, happiness was also predictably associated with recovery from the disease.
I am happy; I will be discharged (Girl, 8-year-old).
I am healthy here(showing her clay artwork), happy and cheerful, my blood test values are good (Girl, 14-year-old).
Feelings of hope
These were related to the desire to recover from the disease. Patients expressed hope about being cured through colorful artworks, smiling faces, and written phrases associated with hope, faith, and optimism.
Never lose your faith, believe only in God (Girl, 16-year old)
There are many people who are cured of cancer; I will be one of them" (Boy, 12-year old).
The verbalizations also expressed that hope was an essential factor in facing the disease since it gave meaning to continue fighting and envisioning a future that offers the possibility of positive changes.
The heart is love (pointing to the drawing), and it wants me to be healthy (Girl, 14-year-old).
I am getting better, I will recover, and I will be back home (Boy, 11-year-old).
Negative Emotional States
This category considers those emotions that generate distress in the patient. It includes sadness, anxiety-fear, and anger.
Sadness
In the present study, sadness was found to be related to three main aspects: 1) a sense of loss, 2) suffering, and 3) consequence of treatment.
The perception of loss was expressed through sadness. Cancer entails the loss of basic pillars of a patient's life, such as health, daily routine, activities, and friends, which are further eroded by the awareness of peers who died from the disease. This was often expressed through drawing characteristics such as the absence of arms, small figures, drawing at the lower area of the page, sad and crying faces (Corman, 1961; Escribano, 1977; Machover, 1953).
I can't be with my little brother because I am sick, that makes me sad, I cry about it (Boy, 7-year-old).
Here (pointing to the drawing) is when I had cancer in the guts, lungs, liver; I felt sad (Girl, 16-year-old).
The second aspect associated with sadness was suffering, resulting from cancer's physical symptoms, including pain, weakness, and tiredness, which limit autonomy and independence.
"It is not easy" (Girl, 16-year-old); this patient refers to feeling weak because she had low platelets and will get a blood transfusion.
Yesterday I didn't want to come to the hospital because I don't want to get stung anymore; I felt sad and discouraged (Girl, 14-year-old).
The third aspect was that patients perceived the treatment as an element that made them sad and changed their behavior. Some medical indications aimed at protecting patients from infections tended to trigger sadness because they involved isolation and hence lack of social contact. That was shown through drawings expressing sad faces during a medical procedure and images depicting the patient's isolation in a hospital room. This aspect of sadness was also expressed verbally.
When I get the chemotherapy, I feel sad, and I don't want chemo, and I want to get out of here (Girl,13-year-old).
I am sad, hospitalized with chickenpox, when I have to stay in the hospital, I get very sad (Boy, 11-year-old) (Fig. 3).
Figure 3
Story at the hospital (Boy, 11-year-old)
Anxiety-Fear
To better address these emotions, the anxiety-fear dyad will be considered. Anxiety was expressed in artworks through specific features, such as unstable figures, omission of feet, cloud drawings, arms being close to the body, drawing of the joints, and imprecise lines (Corman, 1961; Escribano, 1977; Machover, 1953). We identified these elements, as well as others directly associated with body anxiety. Reflecting the physical vulnerability felt by the patients, several drawings depicted medical procedures (lumbar puncture, chemotherapy) and amputated body parts. Likewise, anxiety was expressed through verbalizations regarding health status and test results. Meanwhile, fear was related to sleeping alone, treatment side effects, and painful medical procedures.
I feel nervous about the medical appointment and what they (physicians) are going to tell me (Girl, 14-year-old).
...since I have cancer, I am afraid to sleep alone, …I want to be close to my mom if something bad happens to me (Boy, 11-year-old).
Anger
Indicators associated with anger, such as separate arms, visible teeth, and heavy strokes, were also found in patients' drawings (Corman, 1961; Escribano, 1977; Machover, 1953). These can be explained by the perception that patients have about the environment that surrounds them, seen as hostile due to the unpleasantness of medical procedures and the need to abide by the numerous medical restrictions. On the other hand, children reported mood swings associated with annoyance and discomfort, which could also be a consequence of medical treatment with steroids.
Discussion
Our art-based assessment of disease experiences in children and adolescents with cancer illustrated emerging themes within the cognitive and emotional dimensions. Through drawing features, clay figures, painted images, and stories, the artworks produced symbolized patients' cancer experiences and served them to express thoughts and feelings depicting what they were not able to express verbally (Malchiodi, 1999; Rollins et al., 2012; Sadruddin & Hameed-ur-Rehman, 2013). In addition, this kind of assessment promoted spontaneous verbal communication from patients regarding the artworks and facilitated the communication with the researcher.
The cognitive dimension considers several aspects of the disease experiences. We found that patients' disease and treatment awareness was expressed by their knowledge about their condition, allowing children to understand better their disease and the process they face. Understanding disease mechanisms is important for the patient (Filová & Sikorová, 2015; Soanes et al., 2009), as this influences the perception of the cancer experience, contributes to adaptation to the disease process (Husson & Zebrack, 2017; Ruhe et al., 2016), and increases treatment adherence (Stegenga & Ward-Smith, 2009). Accordingly, gaining knowledge about the disease was shown to reduce concerns and to generate feelings of safety and control in children with cancer (Darcy et al., 2019). A second aspect considered within the cognitive dimension is the concern about self-image, characteristic of adolescent patients and commonly related to treatment side-effects, such as hair loss (Dua & Heiland, 2017) and weight loss, which affect their image and generate concerns about how their friends perceive them (Sadruddin & Hameed-ur-Rehman, 2013). Alopecia is one of the most traumatic side effects of cancer (Im-Ryung et al., 2012; Torres et al., 2019) since it affects a person's identity and appearance in front of others (Dua & Heiland, 2017). In line with previous research (Williamson et al., 2010), adolescents' need to hide the disease and its effects was also detected in our study. A third aspect, namely patients' ability to take responsibility, was the execution of behaviors aimed at improving well-being and promoting treatment adherence, which may reflect children's and adolescents' maturity (Tilton-Weaver et al., 2001). On the other hand, the need to take responsibility for their treatment aids in generating a sense of control (Gibson et al., 2010), which decreases anxiety and helps children to adapt to the situation (Bjork et al., 2009).
The emotional dimension includes several positive emotional states. The fighting spirit represents the patients' willpower to keep up with the treatment plan and recover their health. A previous study reported that having a purpose in life contributes to maintaining the desire to recover health (Husson & Zebrack, 2017). The fighting spirit is also associated with fewer mood problems (Cordova et al., 2003), and correlates negatively with depression, anxiety, hopelessness, and helplessness (Cayrou et al., 2003). A second topic within the emotional dimension refers to affection towards family members and friends, which was detected as a positive emotion that can motivate patients to resume the life they had before being diagnosed with cancer (Bjork et al., 2009; Einberg et al., 2015; Swartzman et al., 2017). A third aspect includes feelings of happiness; as stated in previous studies, children expressed a need to play, feel joy, have fun, explore the world, and engage in social interactions, in spite of the difficult reality they face (Bjork et al., 2009;Enskar et al., 2014). Fourth, we found that patients' feelings of hope were associated with disease recovery. Bjork (2008) points out that children with cancer are hopeful about being cured after finishing treatment. In turn, hope is considered a positive factor in children and adolescents with cancer since it is associated with better psychological adjustment (Yuen et al., 2014).
The emotional dimension also considers negative emotions such as sadness, which we found to be related to three main aspects: 1) a sense of loss in reaction to a reality that has changed. Previous research reported that the disease involves the loss of key anchors of a child's life (Darcy et al., 2019; Soanes et al., 2009). Woodgate et al., (2003) showed that one of the meanings associated with the symptoms of cancer is I am hurting ... my heart is sad, denoting the psychological distress associated with falling ill and being unable to take part in activities that were important or enjoyable for patients; 2) suffering, resulting from physical symptoms of cancer (Best, Aldridge, Butow, Olver, & Webster, 2015); and 3) treatment-related sadness. Woodgate et al. (2003) found that treatment is perceived by patients as an element that changes their mood and behaviors. Also, medical indications regarding patient isolation can trigger sadness as they imply withdrawal from social contact (Bjork et al., 2009). Another negative emotion included in this dimension is the anxiety-fear dyad, which we found to be associated with the patient's body, test results, treatment side-effects, fear of sleeping alone, and painful medical procedures. Previous research indicated that surgical procedures and interventions involving needles caused the greatest rejection and discomfort in the young population (Leibring & Anderzén-Carlsson, 2019). Likewise, past research addressed children's fears about sleeping alone (Anderzén-Carlsson et al., 2010) and fear about treatment side-effects and painful medical procedures (Darcy et al., 2019; Leibring et al., 2019). Both anxiety and fear have been reported as high-frequency emotions in children with cancer (Enskar et al., 2014), commonly derived from feelings of threat (Darcy et al., 2019). A cancer diagnosis entails a strong feeling of threat against life, accompanied by constant confrontation with the person's reality, due to internal (cognitions) and external (symptoms, consultations, and medical procedures) reminders about cancer (Curran et al., 2017). In turn, feelings of anger can be explained by the patient's perception of a hostile environment due to medical interventions, restrictions, and treatment with steroids (Gibson et al., 2010; Pinheiro, 2015). One of the emotional states pointed out by Woodgate et al. (2003) on children and adolescents with cancer is I am cranky ... I am not myself, described by patients as feeling different in association with adverse mood changes. These mood expressions cannot be controlled and generate frustration because they affect social interactions at home and outside. In turn, these emotions reinforce the idea of how much cancer has changed their lives and the little control they have over it (Darcy et al., 2019).
The study's limitations include the small sample size and the lack of a standardized scale or quantifiable tools to assess artworks in the pediatric setting, which prevent our results from being generalized to other populations. Also, since we worked with children at different stages of the cancer journey and with different cancer diagnoses, the art assessment responses varied from one child to another, which could affect the results. Future studies might benefit from including a control group, which allows measuring the effect of an art therapy intervention on the cognitive-emotional variables highlighted in this research.
In summary, art-based assessments foster a bridge of connection between the pediatric patient and the healthcare provider, allowing the patient's needs to be accessed in a more pleasant and enjoyable way. Through the expression of thoughts, emotions, and needs through artwork, this type of evaluation can facilitate insight into the patient's inner experience to improve their coping skills and their ability to adapt to the disease burden. On the other hand, using art as a non-threatening evaluation-intervention tool can serve as a distraction technique from both disease and treatment to encourage the patient to be more willing to collaborate with the health team. It could also serve as a relaxation strategy to conduct a more focused and accurate assessment, thus improving the patient's care plan. Training health teams on basic aspects of how to use art as an evaluation and intervention tool, as well as establishing multidisciplinary teams that include art therapists, would contribute to meeting the needs of pediatric cancer patients. For children who might find it challenging to convey themselves verbally about their disease experience, art-based approaches can be a valid and helpful alternative to assess patients' psychosocial needs in pediatric oncology settings. Furthermore, the use of art could also facilitate verbal communication between the healthcare team and the patient, acting as a generator of spontaneous conversation that serves as a gateway to start interviews, evaluations, or interventions to improve the patient's treatment adherence and quality of life.
Conflicts of Interest:
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Aguilar, B. (2017). The Efficacy of Art Therapy in Pediatric Oncology Patients: An Integrative Literature Review. Journal of Pediatric Nursing, 36, 173-178. https://doi.org/10.1016/j.pedn.2017.06.015
Allemani, C., Matsuda, T., Di Carlo, V., Harewood, R., Matz, M., Nikšić, M.,…CONCORD Working Group. (2018). Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet, 391 (10125), 1023–75. https://doi.org/10.1016/S0140-6736
Angell, C., & Alexander, J. (2015). ¨Draw, write, and tell¨. A literature review and methodological development on the "draw and write" research method. Journal of Early Childhood Research, 13 (1), 17-28
Altay, N., Kilicarslan-Toruner, E., & Sari, Ç. (2017). The effect of drawing and writing technique on the anxiety level of children undergoing cancer treatment. European Journal of Oncology Nursing, 28, 1-6. https://doi.org/10.1016/j.ejon.2017.02.007
Anderzén-Carlsson, A., Kihlgren, M., Svantesson, M., & Sorlie, V. (2010). Parental handling of fear in children with cancer; caring in the best interests of the child. Journal of Pediatric Nursing, 25(5), 317-326. https://doi.org/10.1016/j.pedn.2008.10.004
Best, M., Aldridge, L., Butow, P., Olver, I., & Webster, F. (2015). Conceptual analysis of suffering in cancer: a systematic review. Psycho-Oncology, 24, 977-986.
Björk, M. (2008). Living with childhood cancer - Family members' experiences and needs. [Doctoral dissertation]. Lund: Department of Health Sciences, Faculty of Medicine. Lund University, Sweden. Retrieved from https://portal.research.lu.se/ws/files/4069139/1148900.pdf
Björk, M., Wiebe, T., & Hallstrom, I. (2009). An everyday struggle-Swedish families'lived experiences during a child's cancer treatment. Pediatric Nursing, 24(5), 423-432. https://doi.org/10.1016/j.pedn.2008.01.082
Cayrou, S., Dickes, P., Gauvain-Piquard, A., & Roge, B. (2003). The mental adjustment to cancer (MAC) Scale: French replication and assessment of positive and negative adjustment dimensions. Psycho-Oncology, 12, 8-23. https://doi.org/10.1002/pon.634
CIOMS, OMS & OPS (2016). Pautas éticas internacionales para la investigación relacionada con la salud con seres humanos. Retrieved from https://cioms.ch/wp-content/uploads/2017/12/CIOMS-EthicalGuideline_SP_INTERIOR-FINAL.pdf
Cordova, M., Giese-Davis, J., Kronnenwetter, C., Chang, V., McFarlin, S., & Spiege, D. (2003). Mood disturbance in community cancer support groups. The role of emotional suppression and fighting spirit. Psychosomatic Research, 55(5), 461-467. https://doi.org/10.1016/S0022-3999(03)00510-5
Corman, L. (1961). Le Test du Dessin de Famille. Paris: Presses Universitaires de France.
Curran, L., Sharpe, L., & Bulow, P. (2017). Anxiety in the context of cancer: A systematic review and development of an integrated model. Clinical Psychology Review, 56, 40-54. https://doi.org/10.1016/j.cpr.2017.06.003
Darcy, L., Enskar, K., & Bjork, M. (2019). Young children's experiences of living an everyday life with cancer - A three year interview study. European Journal of Oncology Nursing, 1-9. https://doi.org/10.1016/j.ejon.2018.12.007
Donalek, J. (2005). The interview in qualitative research. Urologic Nursing, 124-125.
Dua, P., & Heiland, M. (2017). Cancer-related hair loss: a selective review of the alopecia research literature. Psycho-Oncology, 26, 438–443. https://doi.org/10.1002/pon.4039.
Einberg, E., Nygren, J., Svedberg, P., & Enskark, K. (2015). "Through my eyes": health-promoting factors described by photographs taken by children with experience of cancer treatment. Child: care, health and development, 42(1), 76-86. https://doi.org/10.1111/cch.12285
Enskar, K., Knutsson, S., Huus, K., Granlund, M., Darcy, L., & Bjork, M. (2014). A literature review of the results from nursing and psychological research within Swedish pediatric oncology. Nursing and Care, 3(6), 1-11. https://doi.org/10.4172/2167-1168.1000217
Escribano, J. (1977). Test de la Figura Humana (Psicodiagnostico a priori de normalidad y patologia). Graficas Uguina.
Ferlay, J., Ervik, M., Lam, F., Colombet, M., Mery, L., Piñeros, M.,… Bray, F. (2018). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Retrieved from https://gco.iarc.fr/today, accessed 30 March 2020.
Filová, A., & Sikorová, L. (2015). Evaluating the needs of children with cancer. Central European Journal of Nursing and Midwifery, 6 (1), 224-230. https://doi.org/10.15452/CEJNM.2015.06.0007
Gantt, L. (2011). The Case for Formal Art Therapy Assessments. Art Therapy Journal, 21(1), 18-29. https://doi.org/10.1080/07421656.2004.10129322
Gibson, F., Aldiss, S., Horstman, M., Kumpunen, S., & Richardson, A. (2010). Children and young people's experience of cancer care: A quality research study using participatory methods. International Journal of Nursing Studies, 47(11), 1397-1407. https://doi.org/10.1016/j.ijnurstu.2010.03.019
Graneheim, U., & Lundman, B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105-112. https://doi.org/10.1016/j.nedt.2003.10.001
Husson, O., & Zebrack, B. (2017). Perceived impact of cancer among adolescents and young adults: Relationship with health‐related quality of life and distress. Psycho‐Oncology, 26, 1307–1315. https://doi.org/10.1002/pon.4300
IAAP & IUPsyS (2008). Universal Declaration of Ethical Principles for Psychologists. Available from the International Union of Psychological Science Web site: https://www.iupsys.net/about/governance/universal-declaration-of-ethical-principles-for-psychologists.html
Im-Ryung, K., Juhee, C., Eun-Kyung, C., In, G. K., Young, H., Sung, . . . Jung-Hyun, Y. (2012). Perception, attitudes, preparedness and experience of chemotherapy-induced alopecia among breast cancer patients: a qualitative study. Asian Pacific Journal of Cancer Prevention, 13(4), 1383–1388. https://doi.org/10.7314/apjcp.2012.13.4.1383
Leibring, I., & Anderzén-Carlsson, A. (2019). Fear and coping in children 5–9 years old treated for Acute Lymphoblastic Leukemia - A longitudinal interview study. Journal of Pediatric Nursing, 46, e29–e36. https://doi.org/10.1016/j.pedn.2019.02.007
Machover, K. (1953). The Human Figure Drawings of children. Journal of Projective Techniques, 17, 85-91. https://doi.org/10.1080/08853126.1953.10380466
Malchiodi, C. (1998). Understanding children's drawings. The Guilford Press.
Malchiodi, C. (1999). Medical art therapy with children. Jessica Kingsley Publishers.
Malchiodi, C. (2005). Expressive Therapies. Guilford.
Marcus, J. (2012). Psychosocial issues in pediatric oncology. The Ochsner Journal, 12, 211–215.
Phillippi, J., & Lauderdale, J. (2017). A guide to field notes for qualitative research: context and conversation. Qualitative Health Research. 28(3), 381-388. https://doi.org/10.1177/1049732317697
Pinheiro, I. (2015). Hospital psychological assessment with the drawing of the human figure: A contribution to the care to oncologic children and teenagers. Scientific Research Publishing Inc, 6(4), 484-500. http://dx.doi.org/10.4236/psych.2015.64046
Rollins, J., Drescher, J., & Kelleher, M. (2012). Exploring the ability of a drawing by proxy intervention to improve quality of life for hospitalized children. Arts & Health, 4(1), 55-69. https://doi.org/10.1080/17533015.2011.564194
Ruhe, K., Badarau, D., Brazzola, P., Hengartner, H., Elger, B., & Wangmo, T. (2016). Participation in pediatric oncology: views of child and adolescent patients. Psycho-Oncology, 25, 1036–1042. https://doi.org/10.1002/pon.4053
Sadruddin, M., & Hameed Ur Rehman, M. (2013). Understanding the perceptions of children battling cancer about self and others through drawing. South Asian Journal of Cancer, 2(3), 113-118. https://doi.org/10.4103/2278-330x.114100
Soanes, L., Hargrave, D., Smith, L., & Gibson, F. (2009). What are the experiences of the child with a brain tumor and their parents? European Journal of Oncology Nursing, 13(4), 255-261. https://doi.org/10.1016/j.ejon.2009.03.009
Stegenga, K., & Ward-Smith, P. (2009). On Receiving the diagnosis of cancer: The adolescent perspective. Journal of Pediatric Oncology Nursing, 26(2), 75-80. https://doi.org/10.1177/1043454208328767
Swartzman, S., Sani, F., & Munro, A. (2017). The role of social support, family identification, and family contraints in predicting posttraumatic stress after cancer. Psycho-Oncology, 26, 1330-1335. https://doi.org/10.1002/pon.4304
Tahmasebi, Z., Maghsoudi, J., & Talakoub, S. (2017). The effect of painting on depression in children with cancer undergoing chemotherapy. Iranian Journal of Nursing and Midwifery Research, 22(2), 102-105. https://doi.org/10.4103/ijnmr.ijnmr_242_15
Tilton-Weaver, L., Vitunski, E., & Galambos, N. (2001). Five images of maturity in adolescence: what does "grown up" mean?. Journal of Adolescence, 24(2), 143-158. https://doi.org/10.1006/jado.2000.0381
Torres, V., Darezzo, M., Machado, F., Bravo, L., Adlard, K., Secola, R., & Fernandes, A. (2019). Frequency, severity, and distress associated with physical and psychosocial symptoms at home in children and adolescents with cancer. Journal of Pediatric Health Care, 33(4), 404-414. https://doi.org/10.1016/j.pedhc.2018.11.007
Williamson, H., Harcourt, D., Halliwell, E., Frith, H., & Wallace, M. (2010). Adolescents' and parents' experiences of managing the psychosocial impact of appearance change during cancer treatment. Journal Pediatric Oncology Nurse, 27(3), 168-175. https://doi.org/10.1177/1043454209357923
Woodgate, R., Degner, L., & Yanofsky, R. (2003). A different perspective to approaching cancer symptoms in children. Journal of Pain and Symptom Management, 26(3), 800-817. https://doi.org/10.1016/s0885-3924(03)00285-9
Yuen, A., Ho, S., & Chan, C. (2014). The mediating roles of cancer-related rumination in the relationship between dispositional hope and psychological outcomes among childhood cancer survivors. Psycho-Oncology, 23, 412–419. https://doi.org/10.1002/pon.3433
Notas de autor
Correspondence about this article should be addressed Olimpia Petzold: olipr@hotmail.com