Articles

This work is licensed under Creative Commons Attribution-NonCommercial 4.0 International.
Received: 23 March 2019
Accepted: 03 July 2019
Abstract: Italy is one of the countries with the oldest population in the world. In spite of that fact and the alarming estimates about future demographic trends, long-term care (LTC) policy is still struggling to be acknowledged as a relevant issue in the public debate and political agenda. In sharp contrast with the policy inertia prevailing at the national level, in recent years, many territories have been experimenting with new solutions in the field of LTC, addressing the challenge of building more inclusive local care environments for frail (dependent) elderly people and their families. Building upon this, the current paper aims at dealing with the most recent academic literature on social innovation and the policy discourse elaborated by the European Union to i) develop a “working definition” of social innovation, with specific reference to LTC and elderly care; ii) provide a comparative analysis of a set of selected innovative solutions, which fall between full institutionalization and full family-based care, implemented in two Italian regions, namely, Lombardy and Piedmont; and iii) discuss the factors behind the adoption of socially innovative policy solutions at the local level, thereby shedding light on the key role played by new actors and multistakeholder networks.
Keywords: Aging, Long-term Care, social innovation, inclusive local care environments, Italy.
Resumen: Italia es uno de los Países más envejecidos del mundo. A pesar de eso y de las alarmantes estimaciones sobre las tendencias demográficas futuras, la política de cuidado de larga duración (Long Term Care - LTC, por sus siglas en inglés) está encontrando dificultades para ser reconocida como uno de los temas centrales del debate público y de la agenda política. Sin embargo, en contraste con la inercia que prevalece a nivel nacional, en los últimos años, muchos territorios han experimentado nuevas soluciones en el campo de la LTC, enfrentando el desafío de crear entornos de cuidado local más inclusivos para las personas mayores vulnerables (dependientes) y sus familias. El presente documento apunta a la literatura académica más reciente sobre innovación social y el discurso político elaborado por la Unión Europea. A lo largo del texto se desarrolla una “definición operacional” de innovación social, con referencia específica al LTC y al cuidado de las personas mayores. Por otro lado, proporciona un análisis comparado sobre las respuestas innovadoras que se han dado ante la institucionalización completa y la atención familiar en las dos regiones italianas de Lombardía y Piamonte. Por último, se discuten los factores que hay detrás de la adopción de soluciones políticas socialmente innovadoras a nivel local, arrojando luz sobre el papel clave que desempeñan los nuevos actores y las redes de múltiples stakeholders.
Palabras clave: Envejecimiento, cuidado de larga duración, innovación social, ambientes de cuidado local inclusivo, Italia.
1. Introduction1
According to the OECD’s most recent figures, Italy is one of the countries with the oldest population in the world. With an old-age dependency ratio equal to 36.3, the share of elderly people (65+) to working-age individuals (20-64) is second only to that of Japan. In spite of that fact and the alarming estimates about future demographic trends, long-term care (LTC) policy for frail, elderly people in Italy is still struggling to be acknowledged as a relevant issue both in the public debate and in the political agenda.
From a comparative perspective, Italian LTC public policies are generally assessed as being largely unfit to address the socioeconomic challenges coming from these major sociodemographic trends (see NNA, several years; Gori, 2010; Ranci and Pavolini, 2013). Although the overall figures on the Italian public expenditure on LTC appear roughly in line with the average values of other European countries, the Italian case stands out due to a number of key elements. Compared with other European countries, such as France, Germany and the UK, which have developed more coherent systems to respond to LTC needs, the peculiarity of the Italian case consists of a polarization in the supply of LTC between two poles: informal family-based home care solutions on one hand and full institutionalization on the other. We argue that this situation is directly linked with the shortcomings (in some cases, the full absence) of intermediate solutions that, in other countries, have been established to bridge the gap between pure informal home-care assistance provided by families and residential health-care driven assistance.
Despite high functional pressures and in contrast with what has developed in several European countries, during the last two decades, no major reform of LTC policy has been adopted in Italy, hence leaving unanswered the question of how to take care of the growing number of vulnerable elderly people who are largely dependent on the abilities of (shrinking) families. While institutionalization rates are comparatively low, and public home care services are poorly developed, since the 1980s, the main national measure to support elderly people in need of care consists of a flat-rate, unconditional cash-transfer, which has been shown to be highly ineffective in meeting the costs of care in the private market, thus making it a disproportionate burden for households (especially those that are medium-low income) (Albertini & Pavolini, 2015; Luppi, 2016; 2018)2. Most families, therefore, end up taking care of the elderly at home, often directly (through informal care, especially from female relatives), sometimes indirectly (by hiring a caregiver or a helper, who is often foreign and in the shadow economy), most of the time with mixed solutions.
These “informal welfare” tools present both virtues and vices. While families appreciate having relatives assisted in their home environments, closely supervised by flexible and cheap workers, on a one-to-one basis, research has also underlined this model’s pitfalls (cf. Ambrosini, 2012). Lack of qualification, exploitation and overwork, informality (often paired with migrants’ undocumented status) and difficulties in managing the employer-employee relationship in a domestic and highly emotional field represent major obstacles for the provision of adequate, sustainable and equitable care services to the elderly population.
Against this backdrop, despite the institutional inertia in the field of LTC at the national level, the intersection between the mounting unmet care needs and constrained public budgets has fostered the emergence over the last two decades, in some local contexts, of a number of socially innovative pilot projects and initiatives. In sharp contrast with the frozen national scenario, many territories – especially in the richest areas located in the northern part of the country – have in fact been experimenting with new solutions in the field of elderly care and LTC, addressing the challenge of building in novel and creative ways inclusive local care environments for frail (dependent) elderly people and their families. Some of those initiatives are the main focus of this article, which is approached from a threefold perspective.
First, drawing from existing comparative studies on social innovation, the paper asks how can “socially innovative” solutions in LTC be conceptualized. Second, the paper aims to provide a comparative overview of a set of selected programs implemented in two northern Italian regions, namely, Lombardy and Piedmont; we explore the social innovation potential of these solutions, which stand out for falling in between full institutionalization and full family-based care. Third, from a more explanatory standpoint, empirical evidence and field research allow us to advance some preliminary hypotheses about the factors that might be key to explaining the adoption of socially innovative policy solutions in those local contexts. In particular, the article develops three main hypotheses in relation to the mobilization of a series of private actors and stakeholders (nonprofit organizations, bank foundations, social partners, private companies), the creation of multistakeholder networks involving local public institutions, and the strategic valorization of the financial support made available through additional private funding.
The article proceeds as follows. Section 2 addresses the most recent academic literature on social innovation to develop a working definition of socially innovative LTC and elderly care policies and to conceptualize the notion of an “inclusive local care environment”. Section 3 presents a comparative overview, relying on a common analytical grid, of four selected cases of socially innovative LTC measures run at the local level in Lombardy and Piedmont. Section 4 finally turns to interpretation and concludes by advancing and discussing three explanatory hypotheses that help to shed some light on the factors that favored the setup of socially innovative solutions in the local contexts under review.
2. Social innovation and long-term care: towards a working definition
Over the last fifteen years, the concepts of innovation and social innovation have gained, especially on the impulse of the European Union, an increasing importance in the public discourse and in the reform agendas of the Union and its Member States. The interest in social innovation has become particularly intense in the decade since the Great Recession. The concept appeared able to satisfy the double need to make social protection systems not only more adequate in addressing new and old social risks (exacerbated by the recession) but also more sustainable in terms of costs; this appeared possible thanks to the mobilization of new resources, which were particularly valuable in the presence of increasingly stringent budgetary constraints, and to the positive stimulus of the economy potentially induced by innovation itself (cf. Hubert, 2010; Ferrera and Maino, 2014; Tepsie, 2014; Maino, 2017). Among the most frequently mentioned “challenges” to justify the need for stimulating social innovation processes – alongside long-term unemployment, social exclusion, poverty and migratory flows – are those linked to the rapid aging process occurring in Europe (cf. Caulier-Grice et al., 2010; CE, 2010; Hubert, 2010). Therefore, it appears crucial to clarify the contours of the concept of “social innovation” and, in particular, its meaning in the specific context of policies for the (frail) elderly. What does “social innovation” mean in the LTC and elderly care field? In which sense can a policy measure for elderly people who are frail or no longer self-sufficient be qualified as “innovative”? What are the current trends in the EU on this front?
From a general viewpoint, many authors note that social innovation is not a new concept; it could in fact be traced back to the works of the founding fathers of sociology – from Durkheim to Weber to Tarde – although with a meaning quite different from that commonly attributed to it today (Moulaert et al., 2017). However, the first explicit mention of social innovation in its current meaning goes back to the second half of the 2000s, within the EU agenda. Since then, two phases can be distinguished (Hubert, 2010; Sabato et al., 2015). In the first phase, started with the relaunch of the Lisbon Strategy through the Renewed Lisbon Strategy (2005-2010), the promotion of social innovation – although partly achieved through the Structural Funds, the Open Method of Coordination and the Seventh Framework Program – struggled to be identified in European documents as a separate and clearly defined policy objective, while the priority seemed still to lie in supporting innovation that was understood in a technical-industrial sense. Social innovation kept being “between the lines”, and its presence in the European agenda, although growing, remained sporadic and often implicit (Sabato et al., 2015). It was with the Renewed Social Agenda, launched in 2008 (EC 2008a), and some initiatives promoted by the Commission between 2009 and 2010 that social innovation became explicitly thematized by the Union and appeared systematically in some of its official documents, including in the Europe Strategy 2020 (EC, 2010), which considered it a key-area in pursuing the general objective of a smart, sustainable and inclusive growth (Sabato et al., 2015) and in the subsequent Social Investment Package (SIP) promoted by the Commission (EC, 2013a), as well as in the European Pillar of Social Rights (European Parliament et al., 2017).
It was in this second phase that emerged the definition of “social innovation” that has been more frequently used in the official documents produced by the European Union in recent years, namely, that proposed in 2010 by the Bureau of European Policy Advisers (BEPA) (Hubert, 2010). Although not officially adopted by the EU, there is no doubt that its influence has had a significant impact both in terms of policymaking and in the academic debate, as well as among experts. As highlighted by Sabato et al. (2015), the BEPA and its definition have in fact played a central role in the agenda-setting process that explicitly imposed the issue of social innovation on the attention of European policymakers, then merged into the Europe 2020 Strategy. According to BEPA – in line with what was proposed by the Young Foundation in a document previously commissioned by the Bureau itself (Caulier-Grice et al., 2010) – social innovations should be “social in both their ends and their means” and should consist of “new ideas (products, services and models) that simultaneously meet social needs (more effectively than alternatives) and create new social relationships or collaborations. They are innovations that are not only good for society but also enhance society's capacity to act” (Hubert, 2010, p. 33). Taken literally, this definition would imply that one could speak properly of social innovation only in the presence of interventions (not necessarily of policies), meeting at the same time the following four necessary conditions:
- 1. offering a new response to a social need (novelty and responsiveness);
- 2. doing it more effectively than existing solutions (greater effectiveness);
- 3. renewing or improving social skills and relationships (greater inclusiveness and empowerment); and
- 4. determining a better use of goods and resources (greater efficiency).
Such a definition, however, cannot be taken as unproblematic. In addition to its evident normative connotation, the BEPA conceptualization appears at the same time extremely broad in terms of the range of measures classifiable under its label (ideas, products, services and models) but undoubtedly highly restrictive in terms of empirically observable objects. To be such, social innovation should in fact be both product and process innovation. The former should also consist of a result (output), which – in addition to being more effective than the existing alternatives in satisfying the social needs present in society – should also be more efficient in the use of available resources; however, the latter should ensure that the output itself is achieved through a renewal of social interactions, in light of the principles of the involvement and empowerment of the beneficiaries, the inclusion of the various stakeholders called into question by the policy, the widespread participation in decision-making processes, the adoption of collaborative rather than competitive logics and that of a bottom-up rather than a top-down approach. Given this restrictiveness, in our view, it is more useful to consider the formulation proposed by the BEPA (Hubert, 2010) as the stylization of an ideal type, an ideal limit concept that, as such, tends to be lacking in definition of real empirical referents and is mainly useful as a coherent and unitary conceptual framework from which to measure the distance of the observed reality and its peculiarities.
Reviews of the main definitions produced by the literature and numerous European reports indeed show high variability in terms of characteristics identified, explicitly or implicitly, to define social innovation (Jensen and Harrison, 2013; Moulaert et al., 2013; Tepsie, 2014). From this point of view, recent attempts made to break down the general (and otherwise generic) concept of social innovation and detect different types or dimensions (tendentially complementary), more easily observable at the empirical level, are certainly valuable. Beyond the specificities of the single proposals (Evers & Ewert, 2014; Tepsie, 2014), what seems to emerge from empirical research is the opportunity to increase the denotative power of the concept of “social innovation” by adopting operational definitions at a lower ladder of abstraction, which, on the one hand, allows the capture of different degrees of innovation and, on the other hand, takes into account the specificities of the policy and the welfare context in which solutions that can be qualified as “innovative” are located.
In line with this operational approach, in order to investigate the specific connections between social innovation, elderly care and LTC, we suggest considering the policy guidelines promoted by the EU over the past decade to address the challenges posed by the aging of the population, as well as the research initiatives supported in this field by the Union itself (Razetti, 2018). Overall, and coherently with the paradigm of social investment, the policy discourse promoted by the European Union locates aging and LTC issues in the wider life cycle of the individual, thus emphasizing the importance of an approach aimed primarily at preventing or delaying the emergence of dependency (EC, 2008b; EC, 2008c; SPC, 2010; EC, 2013a; EC, 2013b; SPC-WG-AGE, 2014; Cibinel et al., 2017). A preventive and proactive rather than a reparative approach is considered essential to curb the demand for assistance, reduce costs (direct and indirect) for the whole system, and improve, at the same time, the quality of life of the elderly and their caregivers. In this sense, social innovation, favoring a discontinuity with respect to long-established policy practices, becomes a significant functional element in the development of new models of assistance inspired by social investment (Fransen, 2014). Although within the EU’s reports on aging, references to social innovation became more explicit only from 2013 onwards, there is no doubt that the attention given to some basic guidelines for renewing processes and products in the LTC field contributes to defining a common ground between social innovation, social investment and LTC, i.e., healthy and active aging; prevention and rehabilitation; coordination and integration between the different components of the system (formal and informal care, social and health care); the mobilization of a plurality of actors (public, private, for-profit and nonprofit) – above all at local level – in the functions of codesign and coproduction, financing, organization, governance, monitoring and evaluation; individual and collective empowerment; home care instead of residential care; and the transversal use of ICT. If applied, these guidelines should help contain the demands for assistance, qualify and increase their supply, reduce their costs, and increase the quality of life of older people, as well as that of their formal and informal assistants.
Moreover, a review of the research projects supported by the European Union over the last decade on social innovation in the field of LTC policies (through the Seventh Framework Program, Horizon 2020 and other specific initiatives promoted by the Commission) highlights the initial development of operational definitions of social innovation that are useful for empirical analysis policies under examination in this article (for an overview see Razetti, 2018). Beyond specificities, these definitions tend, first, to stress the context-sensibility of the concept (for instance, depending on the features of the more general care regime), i.e., in the Italian model, the areas in which it would be a priority to stimulate innovation processes would be those of integration, support for families in their search for caregivers, qualification of assistance, and recognition of informal skills (Schulman & Leichsenring, 2015). Second, research on social innovation and LTC generally adopts an extensive interpretation of what can be understood as “socially innovative” in long-term care policies. Consistent with the policy discourse outlined above, these definitions tend, on the one hand, to interpret social innovation as a “lever” to promote social investment, which explains the attention paid to wider concepts, such as those of active and healthy aging; on the other hand, and strictly connected with the first remark, the conceptualizations of innovative LTC policies tend to view as beneficiaries not only the elderly but also their formal and informal caregivers.
These development lines are outlined schematically in Figure 1, which stresses the multidimensional nature of innovation by distinguishing process and product innovations in LTC policies.
Considering the Italian system of policies for nonself-sufficiency, its overall distance from this design is clear. Some peculiarities of the Italian model evoked in the previous section – in particular the widespread use of cash benefits combined with a large use of informal care and the (often irregular) employment of foreign family assistants – seem to pose nonsecondary obstacles to these kinds of innovations (cf. Di Santo & Ceruzzi, 2010; Zilli, 2018). The greatest difficulties would be concerning integration (between migrant workers, families and professionals, health and social services), the qualification of caregivers, and the access to and use of information and communication technologies (ICTs). At the same time, the most recent literature has begun to gather evidence on the existence, at the local level, of multistakeholder network experiences that proved capable of introducing some form of innovation into these policies (Crescentini et al., 2018; Cibinel et al., 2017).
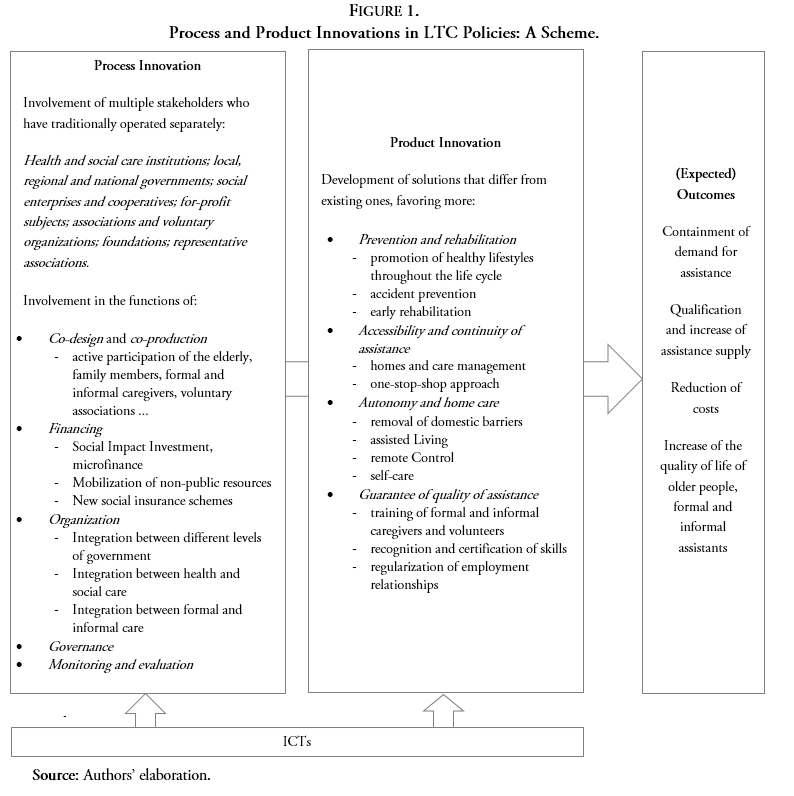
Figure 1.
Process and Product Innovations in LTC Policies: A Scheme
Source: Authors’ elaboration.
3. Towards more “inclusive local care environments”? A comparative overview of four cases
In this section, we describe four cases of “innovative” LTC measures from two Northern Italian regions. These cases have been selected as illustrative experiences of interventions aiming at filling the existing gap between informal family-based home care solutions on one hand and full institutionalization on the other hand, by means of the introduction of at least one kind of innovation among those listed in Figure 1 on both the process side and the product side. Regarding the process dimension, the four cases illustrated below are characterized by the involvement of a plurality of actors who have traditionally operated separately: Local administrations and Plan offices, Territorial areas, service consortia, third sector organizations, voluntary associations and volunteers, and families. The activation of these actors and the setup of multistakeholder networks, strongly rooted at the local level, allow them to qualify the cohesion effects they produce on their communities as “inclusive local care environments”, i.e., networks of integrated and territorially localized services, built-up to address the needs linked to aging and LTC, with particular attention to the most vulnerable members of the community. Regarding products, in all cases, projects have tried to implement solutions enhancing at least one dimension among prevention and rehabilitation, accessibility and continuity of care, elderly autonomy at home, and quality of provided care; many innovative projects crosscut these four dimensions. Both process and product innovation may be supported by the use of new ICTs. In all cases, the intent, by their promoters, is to positively impact, by means of the project itself, the final outcomes of the LTC policy, not only in terms of increasing the quality of life of older people and their formal and informal assistants but also – depending on single experiences – of containing the demand, and/or qualification and increase of assistance supply, and/or reduction of costs.
The illustration of the four cases ranges from those pertaining to “lighter” types of products (impacting mostly the guarantee of the quality of care through orientation measures) to the “harder” types, which are related to innovative forms of institutionalization for severe cases (see also Table 1 at the end of this section).
3.1. WeMi – La città per il welfare
Opened in 2016, “WeMi – La città per il welfare” (“WeMi – The City for Welfare”) is an innovative project led by the Municipality of Milan and supported by the Cariplo Foundation through its initiative “Welfare in Azione”3. WeMi is articulated into three different but coordinated “platforms”, conceived as a unique system aimed at increasing the access of users to existing (both public and private) home services for families and favoring their orientation among them. The three platforms are i) the WeMi physical spaces or “territorial platforms”, ii) the WeMi on-line portal, and iii) domestic help, babysitters and caregivers. The underlying logic of the whole initiative is inspired by the purpose of re-inventing the role of public administration to adapt its services to old and new risks that are not adequately matched by traditional forms of intervention and to address the needs of social targets often missed by public interventions.
In the WeMi territorial platforms (currently eleven), operators favor the provision of shared services, i.e., one or more babysitters shared among several children from the same neighborhood or school, family caregivers shared among the inhabitants of the same condominium, and welfare services shared among the workers of the same company. By the WeMi portal, the Municipality of Milan makes available to all citizens, individuals, families, and companies, a single point of access through which they can find information about Milan's welfare services, while providing to third sector organizations (TSOs – social enterprises and nonprofit cooperatives) the opportunity to present and offer their services. In fact, the platform makes available not only a “front end” to which citizens have access but also a “back end” to which both the Municipality and accredited providers have access. In particular, through a single portal, quality services (including all the domicile services of the city) are provided by 58 TSOs accredited by the Municipality of Milan. Citizens and families can benefit from accessible costs and orientation, as well as qualified staff and operators
Led by the Municipality, the project involves as partners the Polytechnic University of Milan (Department of Architecture and Urban Studies and Department of Design), the National Centre of Social Prevention and Defense (CNPDS), the Gruppo Territoriale Zona 8 and Gruppo Territoriale Zona 5 (two multistakeholder networks operating within two territorial areas of Milan: areas 8 and areas 5). As noted by Guidetti (2016), the role of the Municipality is fundamental because it can take the risk of innovation and make an investment that TSOs alone cannot do, forced as they are to face objective difficulties also linked to a long-lasting social and economic crisis. The awareness of the fact that the platform is a tool is important, but behind it, there is a vision of changing the welfare system, and keeping these two pieces together is very difficult, because the public administration does not normally work on such changes.
3.2. “La Cura è di Casa” project
“La Cura è di Casa” (“Care is at Home”), a three-year project started in May 2016, aims at helping elderly people to age well at home by improving their quality of life and offering support to families, as well as to the entire community. The objective is to favor vulnerable elderly people staying in their own homes by relieving families from the daily management of the person with a view to prevention and social caring.
This goal is pursued through a process of combining and integrating the various health, social and solidarity-based systems of services offered in the area. This outcome is made possible by the adoption of a new governance model that favors better coordination of existing resources and the activation of new energies present in the local social fabric, thanks to the development of both real and digital community networks. From this perspective, the development of a new service management model for vulnerable elderly people is also intended as the experimentation of a new and more sustainable model of welfare provision that is potentially reproducible even in relation to other population targets.
The area covered by the project is that of the local health enterprise (LHA) of the Verbano Cusio Ossola (VCO) area in the North-Eastern area of Piedmont, which includes3 intermunicipal social services consortia4. Beneficiaries of the interventions are the elderly (over 65) – vulnerable or close to the loss of autonomy – who live in the VCO and are not in charge of their social-health services5. The vulnerable elderly cared for thus far number approximately 5506. This number is expected to reach 700 (equal to 38,000 hours of intervention) at the end of the project (Cibinel et al., 2017).
With reference to the services provided, the elderly can benefit from a large set of measures, ranging from monitoring services, personal care and hygiene, physiotherapy and nursing assistance, domestic visits, and assistance for daily activities. Their integrated management involves the use of more traditional territorial social services and more specialized figures (physiotherapists, psychologists, specialist doctors, professional nurses), as well as volunteer activities. Moreover, thanks to the local network of NPOs, the beneficiaries can take advantage of socialization services and cultural and aggregative activities to contrast the loneliness and the tendency towards isolation that often characterize the elderly population.
Currently, the selection of vulnerable elderly people occurs through reports coming from traditional services (LHE, social services, Residential health structures – RHSs) or from “community antennas” such as voluntary associations. In the first phase of the project, an integrated information system between territorial social services and LHE was developed so that general practitioners (GPs) may report users who meet the characteristics of vulnerability and who could benefit from the services offered by the “Care is at Home” project.
The VCO has been divided into 8 functional territorial aggregations governed by a network manager who coordinates 3-4 care planners (usually local social workers) as well as the resources available, both in terms of project budgets for the aggregations and in terms of staff (nurses, other professional figures, volunteers). Once the report is received, a care planner is chosen; he/she contacts the family and goes to the elderly person’s home to carry out an assessment of his/her needs. If the elderly person is considered to be entitled to the services, the care planner and the network manager jointly define a specific “home care project” and the related necessary resources. Every three months, an evaluation of the elderly person is carried out by those in charge of the plan, which may lead to an adjustment of the type of services provided. The information system aims at connecting the four types of actors on which the development of the new service management and delivery model is based upon, including public administration and institutions, residential health structures, volunteers, and families. In this way, the project intends to provide new tools for fostering integration between operators belonging to different organizations, communication links between the services system and families, and simplified links between families, public and private accredited care systems, and private systems (family assistants) to facilitate access to services.
In addition, one innovative element of the project is the investment in “people-raising actions”, i.e., the recruitment of new volunteers. The purpose of this element is to introduce new operational support tools for professional services into the elderly integrated care system. The institutions, the NPOs, and the for-profit actors, as well as the voluntary services and private citizens, are expected to foster the boost of “virtuous circles” that, in addition to improving the quality of care to the elderly, are able to create new solidary bonds to the benefit of the whole community. The core of the project relies on the idea that the community is no longer conceived as a collector of problems but as a living and vital organism to be used to generate well-being. A second, specific innovative element is the VCO Social Fund, established in the summer of 2016 under the VCO Community Foundation (the project partner responsible for fundraising activities and governance). Many actions, already initiated, have allowed us to gather considerable resources, which often connect to local social events7. Some initiatives have also created connections with other social interventions, generating links of mutual support and developing a network of solidarity economy.
The estimated cost of the project is approximately 1.9 million euros. Fondazione Cariplo awarded the initiative with a contribution covering 46% of the total value; 36% of the project costs will be covered by the partners, while the remaining 18% of the costs are expected to be met through territorial fundraising (Cibinel et al., 2017). Since its establishment, the VCO Social Fund has collected approximately 425 thousand euros. The fund is run by a management committee that includes the three community foundations involved in the initiative8, a representative of the project leader and a representative of the partner associations.
3.3. “Veniamo a trovarvi” project
The very first round of “Veniamo a trovarvi” (“We Come to See You”) was launched in 2009 as an initiative of the local bank foundation (Fondazione CRC)9 in close collaboration with an association (La Bottega del Possibile) committed, since 1994, to promoting the “culture of home care”. The project aims to favor the permanence of elderly people at their own domicile by reinventing the role of residential structures existing in the area. For this first experimentation, the Municipality of Bernezzo was selected, which is a small village (3,500 inhabitants) located in a peripheral mountain area.
Two major lines of intervention characterize the project. The first consists of a survey of the care needs present in that mountain community through the activation of the so-called “Itinerant Home Visitor”, a person in charge of regularly visiting elderly people (those aged 70 or more), either alone or in pairs, to monitor their health status and needs. As highlighted in FCRC (2012), this type of service has relied on long-established pioneering experience accumulated since the early 1970s by the social services of the close Val Pellice Mountain Community10. To carry out this delicate function, an intermediate care technician (nurse) is chosen. Once the needs of the elderly have been mapped and a core of particularly fragile subjects has been singled out, the second line of intervention consisting of the activation of care services (made available at the local residential health structure and/or delivered at home), aimed at allowing fragile people to stay in their own home for as long as possible, becomes necessary. The usual relationship between the user and the structure is thus reversed, i.e., instead of waiting for the health of the elderly to deteriorate enough to enter the structure, the structure itself was tasked with looking for potential users and providing them with services useful for delaying as much as possible his/her institutionalization. The dialog among the operators of the residential structure and the itinerant home worker is the method adopted to define, on a regular basis, the mix of interventions most suited to individual cases.
From the financial point of view, for the first year, the costs of the project were fully covered by the CRC Foundation (with approximately 116,000 euros), which basically supported the expenses of the itinerant home visitor and allowed the selected elderly to access for free the services provided by the nursing home located in Bernezzo. In the second year, 50% of the costs were charged to the users, while the remaining part was still supported by the Foundation (with 50,000 Euros). From the third year onwards, the costs were entirely borne by the families using the service.
The evaluation of the project, which was carried out by the CIS (Centro Iniziative Sociali) on behalf of the foundation, showed that the hypothesis that the activation of these services leads to a reduction in health expenditure does not appear confirmed by facts (FCRC, 2012). However, it was noted that, in some cases, the project has led to net savings in healthcare spending, thus becoming an effective alternative to the more expensive nursing home; savings, it was emphasized, have been achieved not so much on the costs borne by the social-assistance services – whose contribution to the integration of the fee depends on the income status of the beneficiary, which is not predictable a priori – or on the costs of the share connected to the health component paid by the LHE (FCRC, 2012, p. 104). More generally, according to the analysis proposed in FCR (2012), the problems linked to the replication of this intervention model seem to be ascribable to the presence of clearly “visible” costs – additional to those of the previous situation – in the face of “invisible” savings, which are potential missed costs (in terms of missed hospitalization in the nursing home and/or at the hospital), due to the adoption of an approach aiming at preventing the deterioration of pathologies, which are measured over a longer time span than the experiment has been carried out.
In spite of these mixed results in terms of savings, the model carried out in Bernezzo has been subsequently replicated, thanks to the support provided again by Foundation CRC, in several municipalities of the province, including its capital, Cuneo, thus leading to the first experimentation of the model in an urban environment (56,000 inhabitants). While a new evaluation round is still to be implemented by the CRC Foundation, the person in charge of these measures stresses the relevance of these innovative ways of delivering services being carefully accompanied in terms of process management, to foster learning dynamics and defuse potential conflicts. For these reasons, in the attempt to ensure continuity to these measures and support their activation by new residential structures willing to follow Bernezzo’s path, the CRC Foundation has invested in operators’ specific training, has stimulated a structured dialog among the directors of the different residential structures involved, and has supported newcomers by putting them in “tandem” with structures already participating in the project.
Based on the experience accumulated by the CRC Foundation over the ten years since the beginning of the project, some remarks can be advanced. Involvement in training activities by not only the operator selected as the “itinerant home visitor” but also the entire staff of the structure has proved crucial to avoiding or defusing deleterious competition, if not full-blown envy dynamics, among operators who, often overworked, could view those colleagues selected to work outside the structure as being “privileged” (less controlled, with a slower pace of work, and so on). At the same time, making operators rotate in this function would be unfeasible, as the relationship between the itinerant home visitor and the elderly people he/she takes care of is deeply based on trust and often requires a long time to build. To increase trust, particularly in mountain and rural areas marked by high levels of diffidence towards strangers, consciousness-raising and communication activities are of major importance (for example, a letter from the mayor explaining the new services offered, having the information conveyed by a priest at Sunday mass, and so on). The financing scheme initially adopted and sketched as described above was revised, because in many cases, it ended up arousing unrealistic expectations in terms of never-ending free access to the services. Ultimately, the experiment has shown that, while probably reducing some costs thanks to prevention measures, the initiative tends to increase costs as it promotes higher take-up rates.
3.4. Il Paese Ritrovato
Opened in June 2018, the “Paese Ritrovato” (“Rediscovered Village”) is a small village in Monza that was expressly designed and built for hosting elderly people suffering from dementia or Alzheimer's syndrome and allows them to live as autonomously as possible. The initiative was taken by a local social cooperative (“La Meridiana”), founded in 1976 as a voluntary association, with the aim of guaranteeing the well-being of older citizens seen as an active part and an added value to the life of the whole community. To achieve this goal, over the years, the social cooperative has begun to manage numerous services, including day centers, multipurpose centers, residences and a hospice.
To address the needs of people with dementia or Alzheimer's syndrome and guarantee their well-being, the social cooperative has looked at the Netherlands, where dementia-friendly communities for the elderly are a long-established experience, i.e., special neighborhoods where elderly people with mental illness can live freely and safely in a protected but not totalizing environment. The first and most well-known example is the village of Hogewey, where “the focus is on what people can still do, rather than what they can’t” (Godwin, 2015, p. 29).
In Monza, the overall project was defined in the first half of 2015, then sponsors were looked for (July-December 2015); once all necessary authorizations were obtained, construction work began in October 2016, and in June 2018 the structure was officially open. The village is a small neighborhood close to the local Residential health structure (the San Pietro Multi-Functional Geriatric Center) and is made up of a square, a chapel, a large hall for events, a bar, a hairdresser, a minimarket and a garden, as well as some apartments for elderly residents. The flats (8 total to house 64 people maximum) are designed according to the latest innovations in home automation so that residents can carry out, by themselves, most daily domestic activities. Consistent with the logic of the Dutch villages used as a template, everything has been conceived to maximize the independence and autonomy of the elderly. Thanks to the wide availability of services, guests can move freely throughout the village and live their life in autonomy while maintaining, as long as possible, their previous habits. All operating personnel, including the gardener, the cashier and the hairdresser, are social-health workers specifically trained to adequately support the elderly. The “Rediscovered Village” currently hosts 47 people (31 women and 16 men), with an average age of 83; previously, mainly assisted in their own homes.
As a guarantee of the overall quality of the project, a monitoring system has been activated, based on a network composed of important private and public research institutions, i.e., the University of Milan Bicocca is in charge of evaluating the impact of the model on illness evolution, the Polytechnic University of Milan, whose students have contributed to the design of the furnishings and assistive technologies, will estimate the impact of these technologies on the elderly inhabitants’ well-being, the National Research Council has been tasked with the assessment of the effects of physical activities on disease evolution, and eventually, the LUIC University will evaluate the sustainability and replicability of the model. In this way, according to its promoters, the “Paese Ritrovato” aims to be a “valuable domain of research and innovation”. Preliminary observations made during the first six months highlight a slight increase of guests’ “active time” (measured through the Index of Social Engagement, raised from 4.19 to 4.65), as well as reductions in depression (from 7.52 to 6.58, according to the Cornell Scale), behavioral disorders (from 19.2 to 13.8 in the Neuropsychiatric Inventory), and caregiver stress (from 32.2 to 16.6 along the Caregiver Burden Inventory; La Meridiana Due, 2019).
Concerning the business model used to finance and run the structure, in contrast with the Dutch experience in which most of the resources for the village building came from the central government11, this initiative promoted by La Meridiana mostly relies on private resources. The global costs, equal to 10.4 million euros, were covered by means of consistent donations from some local businesses and entrepreneurial families, as well as from the Foundation of the Community of Monza and Brianza Onlus, where a collection fund is active to which anyone can contribute to support the project. For guests, monthly fees are equal to about three thousand euros. Since 2019, the Lombardy Region has contributed 29 euros per day, which results in a partial reduction of the fee charged to the guests. To further increase the number of local public actors involved in this initiative, the social cooperative collaborates with the Municipality of Monza and the LHE.
Inclusive Local Care Environments: The Four Cases under Review
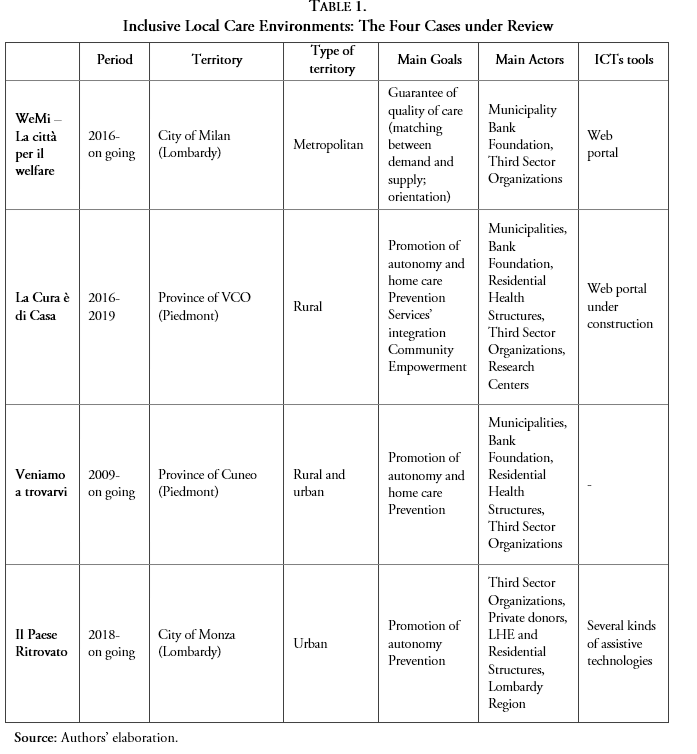
Source: Authors’ elaboration.
4. The factors behind: a discussion
Drawing from the empirical evidence collected in relation to the cases under review, this section aims to discuss some preliminary hypotheses about the factors that might help to explain the adoption of socially innovative policy solutions in the local contexts. Despite the flourishing strand of literature dealing with social innovation (cf. Section 2), only a few studies have thus far explicitly addressed innovation in the social field from an explanatory standpoint. The development of an inventory of causal factors and enabling conditions, as well as the empirical validation of hypotheses, is, therefore, still lacking.
Against this backdrop, building on an in-depth review of the main findings of existing comparative studies, Table 2 offers the first collection of those factors that have been acknowledged by the literature as possible “drivers” or “barriers” to social innovation. The list may be organized by looking at a multiplicity of dimensions, ranging from aspects concerning local governance settings to institutional features and legal constraints.
Drivers and Barriers to Social Innovation: A Review
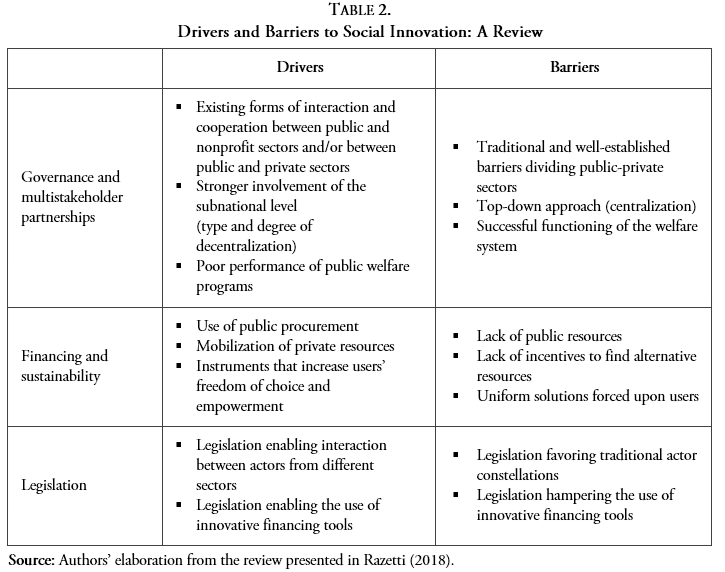
Source: Authors’ elaboration from the review presented in Razetti (2018).
Although all these factors are helpful for understanding the overall background in which social innovation is more likely to occur, we contend that the inventory falls short in shedding light on aspects properly related to the politics dimension of social innovation, that – quite the contrary and based on many empirical cases, including those presented in this article – may be expected to play a crucial role. In particular, in our view, readings purely based on policy and background elements are ill equipped to fully grasp the related factors because they are unable to capture the agential and/or conflictual dynamics that might emerge in the policy arena. More precisely, building on these latter considerations, we argue that, to make sense of the adoption of new programs that alter the allocation of resources in a local community (such as the provision of LTC), one cannot avoid paying specific attention to the presence and mobilization of actors and stakeholders in the local context, as well as to the preferences and instances that they convey in the policy arena. Accordingly, on the basis of our evidence, we expect that three sets of factors are key in shaping the emergence and implementation of socially innovative solutions at the local level, namely, the presence and mobilization of multiple actors and stakeholders in the LTC sector (such as nonprofit organizations, bank foundations, social partners, private companies), their ability to set up multistakeholder networks in which local public institutions act as steering partners, and the strategic valorization of the financial support made available through private additional funding.
Although the findings that emerged from the four cases under review do not lend themselves to be generalized, they can nonetheless feed into further research around the drivers of social innovation. When looking at the four programs analyzed herein, it becomes evident that the setup of multistakeholder networks, strongly rooted at the local level, allows them to qualify, together with the cohesion effects they produce on their communities, as “inclusive local care environments”, i.e., networks of integrated and territorially localized services built-up to address the needs linked to aging and LTC, with particular attention to the most vulnerable subjects of the community. Most notably, in all four cases, the emergence of these networks – characterized by the involvement of a plurality of actors who had traditionally operated separately, such as Local administrations and Plan offices, Territorial areas, service consortia, third sector organizations, voluntary associations, volunteers, and families, with public authorities often called to play a vital steering role – was at the same time a manifestation of innovation and a sort of precondition to foster it in terms of processes and products, as well as a way to channel external financial resources in LTC initiatives.
We want to conclude with a final remark that relates to the future research agenda. The investigation of the four initiatives under review has offered some promising insights into the factors that may trigger the adoption of socially innovative solutions at the local level. However, to effectively test our findings about the drivers and, possibly, to shed light on the barriers to social innovation, our analysis would need to be complemented by an in-depth study of some failed initiatives. In other words, the politics of social innovation deserves to have in the future more attention than has thus far been given to it in social research, in LTC policy and beyond.
References
Albertini, A., & Pavolini, E. (2015). Unequal Inequalities: The Stratification of the Use of Formal Care Among Older Europeans’, The Journals of Gerontology: Series B, 72 (3), 510–521.
Ambrosini, M. (2012). Surviving underground. Irregular migrants, Italian families, invisible welfare. International Journal of Social Welfare, 21 (4), 361-371.
Caulier-Grice, J., Kahn, L., Mulgan, G., Pulford, L., & Vasconcelos, D. (2010). Study on Social Innovation: A paper prepared by the Social Innovation eXchange (SIX) and the Young Foundation for the Bureau of European Policy Advisors, European Union/Young Foundation, March 2010.
Cibinel, E., Maino, F., Manfredda, F., & Porzio, G. (2017). Indagine propedeutica allo sviluppo di un intervento di sistema sul territorio regionale nell’ambito dell’assistenza familiare, Regione Piemonte, POR Piemonte FSE 2014/2020.
Crescentini, L., Maino, F., & Tafaro, T. (2018). Non autosufficienza: analisi e proposte per un nuovo modello di tutela, 2WEL Working Paper Series, 3/2018, Turin, Centro di Ricerca e Documentazione Luigi Einaudi.
Di Santo, P., & Ceruzzi, F. (2010). Migrant care workers in Italy. A case study, Interlinks Project.
European Commission – EC (2008a). Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions “Renewed social agenda: Opportunities, access and solidarity in 21st century Europe”, Brussels, 2.7.2008 SEC(2008) 2156.
European Commission – EC (2008b). Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions “A renewed commitment to social Europe: Reinforcing the Open Method of Coordination for Social Protection and Social Inclusion”, Brussels, 2.7.2008, COM(2008) 418 def.
European Commission – EC (2008c). Commission Staff Working Document “Long-term Care in the European Union” Accompanying the document “Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions, Towards Social Investment for Growth and Cohesion – including implementing the European Social Fund 2014-2020”, Luxembourg, Office for Official Publications of the European Communities.
European Commission – EC (2010). Communication from the Commission “Europe 2020. A strategy for smart, sustainable and inclusive growth”, Brussels, 3.3.2010, COM(2010) 2020.
European Commission – EC (2013a). Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions “Towards Social Investment for Growth and Cohesion – including implementing the European Social Fund 2014-2020”, Brussels, 20.2.2013, COM(2013) 83 final.
European Commission – EC (2013b). Long-term care in ageing societies - Challenges and policy options, Brussels.
European Parliament, European Council and European Commission (2017). European Pillar of Social Rights, Brussels.
Evers, A., & Ewert, B. (Eds.) (2014). Social Innovations for Social Cohesion: Transnational patterns and approaches from 20 European Cities, WILCO: Welfare Innovations at the Local Level in Favour of Cohesion, Liege, EMES European Research Network.
Ferrera, M., & Maino, F. (2014). Social Innovation Beyond the State. Italy's Secondo Welfare in a European Perspective, 2WEL Working Paper Series, n. 2/2014, Turin, Centro di Ricerca e Documentazione Luigi Einaudi.
Fondazione CRC (2012). Veniamo a trovarvi. Il contesto, l'esperienza, i risultati e le prospettive. Progetto sperimentale di assistenza alla domiciliarità degli anziani, Le ricerche socio-economiche della Fondazione CRC, Cuneo.
Fransen, L. (2014). The Policy Agenda – EU approach to long-term care, 5th Senior Government Officials Meeting Connecting the Dots: Formal and Informal Care, 10 June 2014, HICC Hyderabad India.
Godwin, B. (2015). Hogeway: a ‘homefrom home' in the Netherlands. Journal of Dementia Care, 23(3), 28-31.
Gori, C. (2010). L'assistenza agli anziani non autosufficienti in Italia. Secondo rapporto promosso dall'IRCCS, Bologna, Maggioli.
Guidetti, C. (2016). Welfare di tutti: innovare strumenti e misure per un sistema di welfare aperto alla città. Lombardia Sociale, 24 November 2016.
Hubert, A. (Ed.) (2010). Empowering people, driving change. Social Innovation in the European Union, Luxembourg, Publication Office of the European Union.
Jensen, J., & Harrison, D. (2013). Social innovation research in the European Union. Approaches, findings and future directions. Luxembourg, Publications Office of the European Union.
Jessoula, M., Pavolini, E., Raitano, M., & Natili, M. (2018). ESPN Thematic Report on Challenges in long-term care, Italy, 2018. European Social Policy Network (ESPN), Brussels, European Commission. https://ec.europa.eu/social/BlobServlet?docId=19853&langId=en
La Meridiana Due s.c.s (2019). Il Paese Ritrovato, Power Point Presentation, March 2019.
Luppi, M. (2016). Le riforme nel settore dell'assistenza agli anziani: l'Italia nel contesto europeo. Percorsi di secondo welfare, 21 September 2016. https://secondowelfare.it/innovazione-sociale/le-riforme-nel-settore-dellassistenza-agli-anziani-litalia-nel-contesto-europeo.html
Luppi, M. (2018). Long-Term Care Reforms in Time of Economic Crisis. How Elderly Care Affects Family and their Private Resource in Europe. Rome, Aracne Editore.
Magni, B. (2019). La forza dell’esempio: il Paese Ritrovato. Percorsi di secondo welfare, 23 April 2019. https://secondowelfare.it/innovacare/la-forza-dellesempio-il-paese-ritrovato.html
Maino, F. (2017). Secondo welfare e innovazione sociale in Europa: alla ricerca di un nesso. In F. Maino & M. Ferrera (Eds.), Terzo Rapporto sul secondo welfare in Italia 2017 (pp. 19-42). Turin, Centro di Ricerca e Documentazione Luigi Einaudi.
Moulaert, F., MacCallum, D., Mehmood, A., & Hamdouch, A. (Eds.) (2013). The International Handbook on Social Innovation: Collective Action, Social Learning and Transdisciplinary Research. Cheltenham/Northampton, Edward Elgar Publishing.
Moulaert, F., Mehmood, A., MacCallum, D., Leubolt, B. (Eds.) (2017). Social Innovation as a Trigger for Transformations - The Role of Research. Luxembourg, European Commission, Publications Office.
Ranci, C., & Pavolini, E. (Eds.) (2013). Reforms in Long-Term Care Policies in Europe. Springer.
Razetti, F. (2018). LTC e innovazione sociale: quali spunti dall’Europa?. Paper presented at the SISP (Società Italiana di Scienza Politica) Conference, Turin, 5-7 September 2018.
Sabato, S., Vanhercke, B., & Verschraegen, G. (2015). The EU framework for social innovation - Between entrepreneurship and policy experimentation. ImPRovE Working Paper No. 15/21, Anversa, Herman Deleeck Centre for Social Policy – University of Antwerp, Social Policy Committee.
Schulman, K., & Leichsenring, K. (2015). A qualitative inventory of the key drivers of social innovations in social support and long-term care. WP8 Deliverable 8.3, MoPAct Project.
Social Protection Committee – SPC (2010). A Voluntary European Quality Framework for Social Services. SPC/2010/10/8 final.
Social Protection Committee – Working Group on Ageing (SPC-WG-AGE) (2014). Adequate social protection for long-term care needs in an ageing society. Report jointly prepared by the Social Protection Committee and the European Commission, Luxembourg, Publications Office of the European Union.
Spasova, S., Baeten, R., Coster, S., Ghailani, D., Pena-Casaa, R., & Vanhercke, B. (2018). Challenges in long-term care in Europe. A study of national policies. European Social Policy Network (ESPN), Brussels, European Commission. https://ec.europa.eu/social/main.jsp?catId=738&langId=en&pubId=8128&furtherPubs=yes
Tepsie (2014). Social Innovation Theory and Research. A Guide for Researchers. TEPSIE Deliverable no. 1.4.
Zilli, C. (2019). Donne immigrate e lavoro di cura: un welfare invisibile ma bisognoso di innovazione sociale. InnovaCAre Working Paper, September 2018.
Notes
Additional information
JEL classification: I30; I38.
Corresponding author: ilaria.madama@unimi.it
