RESEARCH ARTICLE
Assessment in Schizotypy: A Systematic Review Towards Clinical and Personality Models
Evaluación en esquizotipia: una revisión sistemática hacia los modelos clínicos y de personalidad
Assessment in Schizotypy: A Systematic Review Towards Clinical and Personality Models
International Journal of Psychological Research, vol. 15, no. 1, pp. 84-97, 2022
Facultad de Psicología. Universidad de San Buenaventura, Medellín
Received: 26 February 2022
Revised document received: 18 June 2021
Accepted: 23 August 2021
Abstract
Introduction: research carried out regarding the psychological concept of schizotypy responds to a field of extensive development since its conceptualization decades ago, which includes schizophrenia spectrum disorders (SSD) and schizotypal personality disorder (SPD). However, controversies still persist marked by the difficulty of establishing definitive consensus.
Objective: the research purpose aimed to synthesize the empirical evidence involved in the use of various methodologies and tools for understanding schizotypy.
Methodology: A systematic review was carried out in the following databases: Web of Science, Scopus, PubMed, Taylor and Francis, Wiley, Science Direct, Google Scholar, and PsycNet. By using the PRISMA guidelines, 65 studies published in the last decade (2010-2020) were discriminated.
Results: The synthesis of cumulative knowledge made it possible to define schizotypy as an integrating multidimensional construct and to identify valid assessment tools in use, in its psychometric, clinical, and personality characterizations.
Discussion/Conclusions: Clinical implications found in these reports are addressed, as well as notions of the continuum of psychoses, taxonomic, and multidimensional models.
Keywords: Schizotypy+ Personality+ Schizophrenia spectrum+ Psychometrics+ Psychological assessment.
Resumen: La investigación alrededor del constructo esquizotipia responde a un campo de extenso desarrollo desde su denominación décadas atrás, que incluye los trastornos del espectro de la esquizofrenia (TEE) y al trastorno de personalidad esquizotípica (TPE), aunque persisten controversias marcadas por la dificultad de establecer consensos definitivos. La necesidad de consolidar los avances en la evaluación de este campo volvió operativa la ejecución de una revisión sistemática de la literatura internacional en las bases de datos Web of Science, Scopus, PubMed, Taylor y Francis, Wiley, Science Direct, Google Schoolar y PsycNet, donde, valiéndose de los lineamientos PRISMA, se seleccionaron 65 investigaciones publicadas en la última década (2010-2020). Tras una síntesis del conocimiento acumulativo, los resultados permitieron definir a la esquizotipia como un constructo multidimensional integrador e identificar herramientas de evaluación válidas y en uso, en sus caracterizaciones psicométricas, clínicas y de personalidad, además de las implicaciones clínicas encontradas en sus resultados. También se discuten nociones del continuum de la psicosis, taxonómicas y de modelos multidimensionales.
Palabras Clave: Esquizotipia, Personalidad, Espectro de la esquizofrenia, Psicometría.
1. Introduction
The relationship betweenmental health and psychopathology has been deemed essential in the deepening of psychological mechanisms and processes related to psychopathological expressions and the evolutionary trajectories of such manifestations (Tortella et al., 2016). At this point, schizotypy stands out as one of the constructs on which there is still no definitive consensus (Suzuki et al., 2015).
In a framework of commonassociationbetweenschizotypal personality, schizotypal personality disorder (SPD), and schizophrenia spectrum disorders (SSD; Cheli et al., 2019), the possession of associated traits is considered at risk of developing SSD (Fonseca & Inchausti, 2018). This highlights the relevance of understanding all its dimensions, when it has been found overlapping of its features with others of a psychiatric and subclinical type (Zhang et al., 2019).
In the research carried out on the schizotypy construct, two marked lines can be seen: those of personality and clinical (Álvarez, 2005). From the analysis of personality, it is characterized in the types that fit within cluster A (APA, 2013), which present traits that are distinguished by strange behaviors, eccentricity, social withdrawal, and suspicion (Belloch and Fernández, 2010). In parallel, in the clinical approach, schizotypy comprises the correlational and probability terms towards the understanding of schizophrenia (Cabrera et al., 2017). The DSM5 classificatory model (APA, 2013) presents schizotypy as a personality type with its relative pathological expression. DeYoung et al. (2012) highlight the complexity of the construct, composed of multiple subfactors that probably come from different sources, and that sometimes present contradictory models. Thus, a global definition denotes schizotypy as a unifying construct, representing the underlying vulnerability of SSD psychopathology, and is expressed through a wide range of personality phenomenology and clinical parameters (Kwapil & Barrantes, 2014). However, there are still notable gaps, referring both to its correct definition and to the diagnostic and pathological implications (Fumero et al., 2017), which are able to recognize three characteristic domains used by various approaches, these are the negative/interpersonal, positive/cognitive, and disorganization.
Based on the above, the purpose of this study aims to synthesize the recent and high-quality empirical evidence, through the analysis and synthesis of the research works developed for the assessment of schizotypy, in order to respond to the difficulties in the replication and consolidation of empirical research results within psychology (Shrout & Rodgers, 2018).
2. Method
The following systematic review is consolidated on the quality of reporting based on the guidelinesof the PRISMA Systematic Review Reporting and Meta-Analysis Referred Submission (Liberati et al., 2009) and with an AMSTAR checklist (Shea et al., 2007) for the review articles used.
PRISMA method proposes an organization system in 4 stages: identification, screening, eligibility, and inclusion, which are reported through a flow chart, to guarantee transparency in the search and selection. In addition, it provides a list of criteria to structure the report (Liberati et al., 2009), complementing the AMSTAR checklist given the diversity of methodologies found. The lists also allowed us to examine the articles reviewed, as well as their methodology and quality.
Consequently, to maximize the breadth of the research, studies of both psychometric validation and other types of design were considered for review. Therefore, there were no specifiers of control/comparison conditions and studies were selected independently of this process. From the same intention, investigations were included without considering the temporal moments.
Criteria for the inclusion of studies imply: a) articles in English in an indexed journal reviewed by external peers published until September 2020; b) articles that identify with the keywords “schizotypy”, “assessment”, “clinical”, “psychometric”; c) articles with a sample defined by clinical, subclinical, and non-pathological participants; d) those that take into consideration at least one validated tool; e) articles that use healthy controls; f) those that reported an outcome measure designed to verify the schizotypy construct.
The exclusion criteria mainly comprised a) research papers that do not report their methodology, b) studies that exclusively comprised the child or adolescent population, c) undergraduate or undergraduate thesis, and d) single case studies or interviews with professionals.
The process of identification and selection of studies began with a search in the Web of Science databases, Scopus, PubMed, Taylor and Francis, Wiley, Science Direct, Google Schoolar, and PsycNet. As a result, an initial total of 9030 records was obtained through the keywords and using search commands. Similarly, after applying the first ten-year time filter (2010-2020), they were reduced to 5797. To those, a first screening was carried out, which resulted in 369 selected texts.
Later, a detailed individual review delimited 156 texts to the base articles. Through the selection criteria, as well as the review protocols and counting repeated records, 91 articles were discarded, concluding with a total of 65
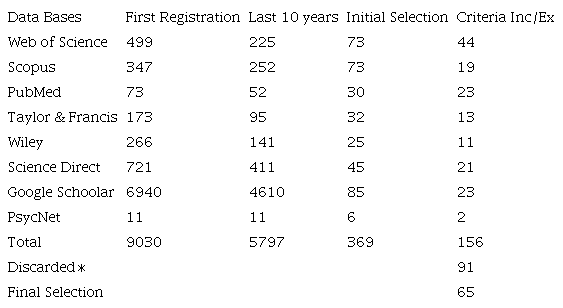
Note. Own elaboration. ∗After the last selection phase.

Figure 1
PRISMA flow chart for file identification and selection
Note. Graphic model from Moher et al. (2009) in Preferred Reporting Items for Systematic Reviews and MetaAnalyses
articles selected for the final review and information synthesis. The selection by databases is detailed in Table 1.
Finally, a list of selected studies was compiled, from which, after an in-depth individual review, the relevant information was extracted using a data extraction protocol (reading sheet). The information synthesis was carried out according to thematic axes on which the results section is organized. The PRISMA flow chart is illustrated in Figure 1.
3. Results
Given the plurality of research methodologies found, it is necessary to establish generalities about the group of articles reviewed. The methods chosen to evaluate the construct show a variety of designs: proposal of new tools, validation of pre-existing models, and correlational proposals to cement a multidimensional model. This disintegration of methodologies could be representative of the lack of consensus when defining this issue (Kwapil & Barrantes, 2014).
Another remarkable characteristic is the predominance of the use of large university populations or young adults. In contrast, those with small samples used clinical, psychometrically delimited or extreme group populations, using control groups (Mason, 2015). The university characterization implies limitations when generalizing the results and on their ecological validity (Ragsdale & Bedwel, 2013).
Those designs with university groups respond to what could be called large-scale epidemiological research (Mason, 2015); from the same groups more delimited secondary investigations appear, ranging from subclinical samples to designs with extreme groups (Kocsis et al., 2017). In this sense, the publications reflect segments in the research projects, evidencing research teams in specific regions (Debbané & Mohr, 2015; Giakoumaki, 2016). A generalized naming of the articles reviewed is summarized in Table 2.
Basic theories vary between the clinical and personality approaches (Mason, 2015); they also highlight attempts to unify both current (Debbané & Mohr, 2015) and multidimensional procedures (Gross et al., 2018; Kemp et al., 2019; Kwapil et al., 2018). In addition to the motivation to reach a definition (Mason, 2015), there are works that study the relationships of the construct with other phenomena (Haslam et al., 2019; Siddi et al., 2017), mainly towards the role it manifests in the risk to SSD (Bora et al., 2014).
The latter highlights that the approach from schizotypy opens the doors to low-cost, high-benefit research (Kline & Schiffman, 2014), since the use of subclinical and non-pathological populations has cemented advances for research on clinical, factorial fronts, risk, cognitive, brain structure, and even genetic factors of schizophrenia (Lawrie et al., 2011).
Using terminology found in Kwapil and Barrantes (2014), the results will be classified as psychometric tools, which define schizotypy in three main dimensions; personality tools, which integrate normal and pathological personality models; and clinical tools, focused on the expression of symptoms or clinical correlates. This classification is not representative of the basic theories, since certain protocols follow from the same theoretical frameworks.
3.1 Psychometric Definition Tools
The psychometric proposal in the reviewed research sample is made up of evaluations with a factorial structure, characterized by three dimensions: positive, negative, and disorganized (Oezgen & Grant, (2018). These tools represent the backbone in terms of construct assessment (Mason, 2015). Mainly highlighting the Schizotypal Personality Questionnaire (SPQ; Raine, 1991), the Wisconsin Schizotypy Scales (WSS; Winterstein et al., 2011) and the Oxford-Liverpool Inventory of Feelings and Experiences (O-LIFE; Mason et al., 1995).
Specifically, predominance of the SPQ stands out, as it is used in more than half of the researches reviewed, and it has a wide acceptance in clinical, subclinical, and general populations (Torbet et al., 2015) that extends to its short versions SPQ-B, SPQ-BR (Callaway et al., 2014; Mitchell and Cohen, 2017), demonstrating capacity of adaptation to the advances of current models, such as the DC-SPQ structure developed for DSM 5 (Xi, et al., 2019).
From a factor analysis between these instruments, it is possible to establish a common framework and make accurate comparisons of the positive and negative dimensions (Gross et al., 2014), with reported ecological validity (Kwapil et al., 2012). In contrast, ambiguity is found when dealing with disorganization, as there is no consensus on its constituent features. This implies that there is no complete unit in the construct and the results may vary by tool (Oezgen & Grant, 2018).
A need for these dimensions to be differentiated when evaluated is emphasized (Barrantes et al., 2013), being disorganization the weak point when using these tools, mainly internationally and in various languages (Kocsis et al., 2016). The differential functioning of the items may lose validity when comparing multiethnic samples, as some even cancel each other out (Cicero et al., 2017).
In contrast, the SPQ-B, in a transnational internal structure validation process, integrated results from 14 countries, corroborating the three-factor structure on a large scale; it showed levels of invariance in the configurable measurement, although its quality varied between samples (Fonseca-Pedrero et al., 2018).
Although the development of these psychometric tools found a kind of zenith decades ago, their status has been relegated by more precise and reliable biological and neurological tests (Cicero et al., 2019), especially when evaluating the risk of psychosis (Moritz et al., 2019). Therefore, additional measures and protocols have been designed and validated in an attempt to establish a more complete framework (Kemp et al., 2020), since their results can be contrasted with other measures referred to here as clinical and personality measures (Ragsdale & Bedwel., 2013).
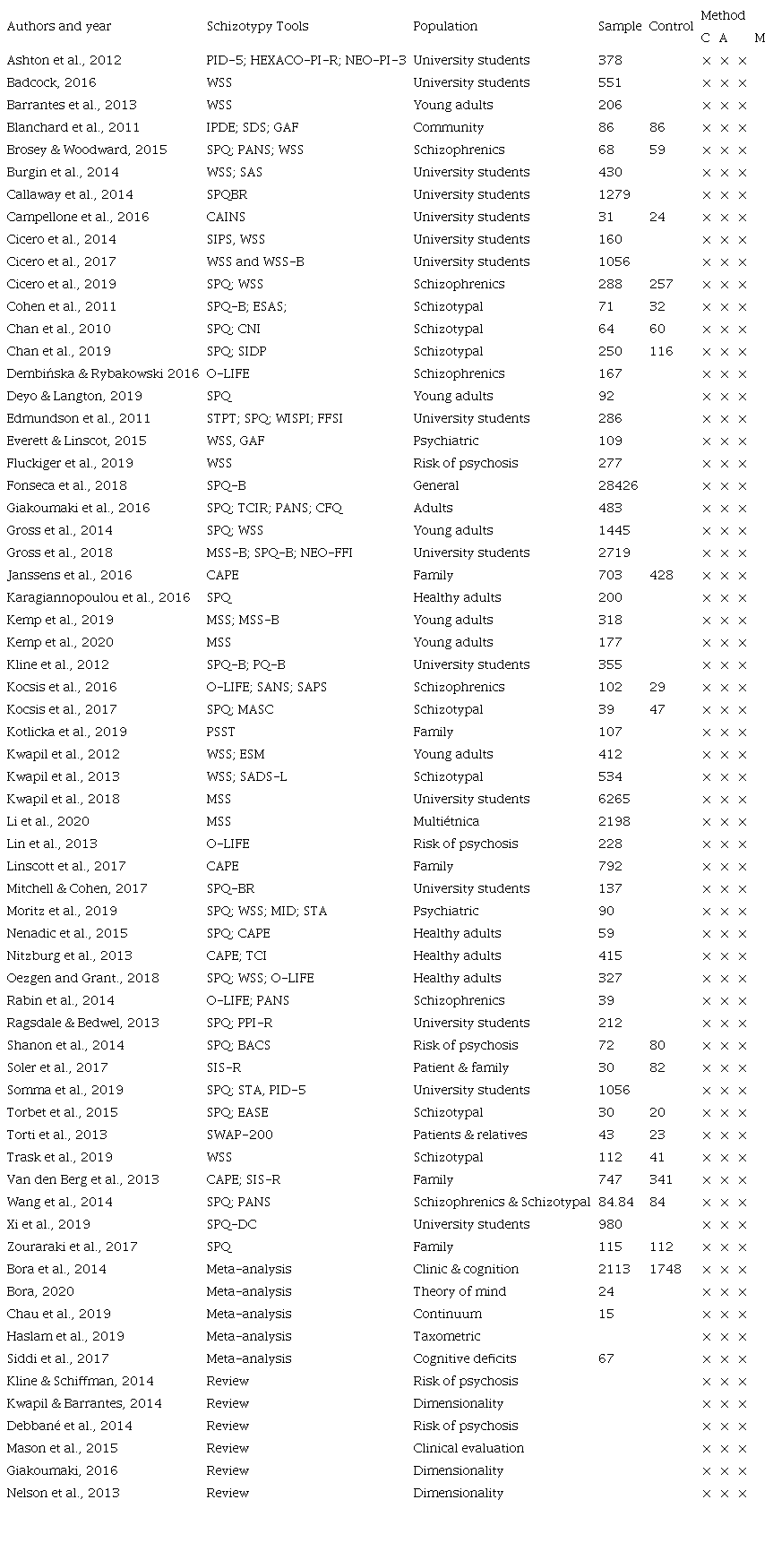
Note. Wisconsin Schizotypy Scales (WSS, WSS-B), Schizotypal Personality Questionnaire (SPQ; SPQ-B; SPQBR; SPQ-DC), Oxford-Liverpool Inventory of Feelings and Experiences (O-LIFE; O-LIFE-B), Assessment of Negative Symptoms (SANS), and Positive Symptoms (SAPS) Multidimensional Schizotypal Scale (MSS). Personality Inventory DSM5 (PID5) HEXACO-Revised Personality Inventory (HEXACO-PI-R,) Personality Inventory (NEO-PI), International Examination of Personality Disorders (IPDE), Global Evaluation of Functioning Scale (GAF), Interview Clinical Evaluation of Symptoms Negative (CAINS), Five Factor Schizotypal Inventory (FFSI), Wisconsin Personality Disorders Inventory (WISPI), Explicit Social Attitudes Scale (ESAS), Marlowe-Crowne Social Desirability Scale (SDSM-C), Structured Interview for DSM-IV Personality Disorders (SIDP), Community Assessment of Psychic Experiences (CAPE), Program for Affective Disorders and Schizophrenia (SADS-L), Premorbid Schizotypal Traits Assessment Scale (PSST), Anomalous Self-Experience Test (EASE), Shedler-Westen Personality Assessment (SWAP-200), Structured Interview for Schizotypy revised (SIS-R), Psychopathic Personality Inventory-Revised (PPI-R), Brief Prodromal Questionnaire (PQ B), and Structured Interview for Prodromal Syndromes (SIPS); Method: C=quantitative approach; A=reports a statistical analysis; M=evidence of some measure of Validity. Own elaboration.
3.2 Personality tools
Personality approaches respond to the study of temperament and character patterns associated with schizotypal traits in healthy populations. Furthermore, they address how these patterns interact with other variables (Nitzburg et al., 2013), defining a personality structure independent of pathologies (Deyo & Langton, 2019), in addition to the own specification of TPE (Chan et al., 2019).
Some relevant approaches respond to the five-factor model (FFM; Edmundson et al., 2011) and the six dimensions of HEXACO (Ashton et al., 2012); the model of personality disorders presented in the DSM5 is also considered (Somma et al., 2019) or previous derivatives, such as the structured interview of the DSM-IV (SIDP, Chan et al., 2019). Usually, other tools are used due to the incomplete measurement capacity compared to current theoretical models (Ashton et al., 2012).
Consequently, as a personality structure, schizotypy presents various features depending on the model taken, given its heterogeneity and overlap with other phenomena. Therefore, the study of personality by trait becomes fundamental (Cicero et al., 2019). Only with a specific definition of trait, the evaluation criteria for the TPE obtain internal consistency and discriminant validity, and can establish a bridge between normal and pathological (Edmundson et al., 2011).
To define personality disorders, the gold standard seems to be the clinical qualification through structured interviews. However, when trying to correlate them to cognitive or biological factors, the results vary depending on the tool used (Deyo & Langton, 2019). Therefore, the evaluation of schizotypal traits should include selfreport measures, as a complement to interviews rated by clinical criteria (Chan et al., 2019; Torti et al., 2013).
Finally, the dynamic nature of personality traits should be noted, including the decline in TPE symptoms during development in young adulthood (Blanchard et al., 2011). The alternative model for personality disorders is effectively articulated with the complementary use of psychometric and personality tools (Somma et al., 2019).
3.3 Clinical Definition Tools
These scales can be defined as symptomatological, which provide complementary accesses and allow the elaboration of correlates with cognitive and affective parameters (Siddi et al., 2017), which are relevant aspects within the constitution of the schizotypal experience (Bora et al., 2014) and associated neuropsychological functions (Siddi et al., 2017).
From these functions, cognitive deficits that characterize the different schizotypal dimensions are identified. For example, impairment of the shift in attention and working memory in paranoid negative and positive schizotypy, in addition to reduced performance in tasks that require frontotemporal connectivity (Karagiannopoulou et al., 2016; Kocsis et al., 2017; Rabin et al., 2014).
From the perception of cognitive functionality, clear relationships can be established between cognitive experience and clinical states. Individuals with schizotypy as a trait presented cognitive abnormalities in certain domains, which are markedly intensified in individuals at high risk for SSD (Shanon et al., 2014; Fluckiger et al., 2019).
Specifically, deficiencies in planning, problem solving, strategy formation, and working memory are central to the entire spectrum of schizophrenia. Greater difficulties in executive working memory and verbal fluency are associated with paranoid and negative schizotypy (Mitchell & Cohen, 2017; Zouraraki et al., 2017). Additionally, high-trait individuals show greater decreases in performance as the information processing load increases (Shanon et al., 2014).
In extreme groups, it is highlighted that high levels of psychometric schizotypy are equated with high clinical levels. Although, these tests imply a specific sensitivity to cognitive deficiencies that can translate nonsignificant results for the clinic (Shanon et al., 2014). Thus, this high-risk clinical approach is obstructed by a notable presence of false positives that would hinder an effective approach.
Understanding that schizotypy responds mainly to a construct in research, the development of a comprehensive framework could correct these shortcomings at the time of establishing specifically in the clinic (Cícero et al., 2014). Another viable alternative can be the analysis of the content of the discourse, mainly in a population with experiences close to schizophrenia (Trask et al., 2019).
Cognitive depressive symptoms can explain motivations and impairment of pleasure in a population at risk of SSD. Individuals with a high degree of schizotypy report being less emotionally expressive, although their behavior appears to be as expressive as that of subjects with a low degree (Campellone et al., 2016). Given the discrepancies between self-report and behavior, affective deficits in schizotypy may reflect deliberative processes rather than implicit/automatic (Cohen et al., 2011).
Other variables of an emotional nature have been identified as conceptually independent. For example, loneliness represents a variable related but not completely inherent to schizotypy (Badcock et al., 2016). Before this, the independent aspects of each correlate must be considered, since its implications can modulate the way in which we access these clinical notions.
3.4 The Continuum of Psychosis
A notion of origin for the creation of the schizotypy construct is its remarkable relationship with psychosis, currently SSD (APA, 2013). Formulating itself as a previous step to psychosis implies a continuous composition (Debbané et al., 2014). In longitudinal data, the dimensions of schizotypy and its enduring traits significantly predicted the development of SSD, psychotic symptoms, and poor adaptation (Kwapil et al., 2013; Kotlicka et al., 2019). Psychometric tools can be used to carry out an effective screening on the risk and development of pathology (Kline & Schiffman, 2014; Rabin et al., 2014).
Several biological and neurological tools have shown great precision in identifying relationships between brain structure, schizotypy, and the development of SSD (Nenadic et al., 2015). Genetic (Janssens et al. 2016), biological (Cicero et al., 2019) and environmental/familial (Soler et al., 2017) risk factor effects are more likely to be combined with high schizotypy in various cumulative and nonlinear knowledge to determine such a result (Kline & Schiffman, 2014).
Specifically, the bridge between schizotypy and schizophrenia can be explained from the Propensity-PersistenceImpairment (PPD) model that establishes how the psychotic and pseudo-psychotic experiences of schizotypy are more likely to lead to impairment when its expression becomes persistent, which indicates a higher risk of SSD (Janssens et al., 2016; Chau et al., 2019). Schizotype as a range within this continuum finds its value insofar as it contemplates the “normal” human experience, and the midpoints between health and dysfunction (Kline & Schiffman, 2014).
3.5 Taxonomy and Dimensionality
One of the main debates regarding the definition of the construct has been the question of dimensionality vs. categorization. Meehl’s (1992) taxonomic model sought to establish categorical principles in the distinction between the pathological and the normal (Haslam et al., 2020). However, taxonomic findings are scarcely reported in psychopathology and are practically nonexistent in personality (Haslam, 2019).
Since taxonomic findings represent complex processes and much of the taxometric research does not support the presence of a taxon, dimensional results are almost five times more likely (Haslam et al., 2020). Consequently, meta-analytic results have not found evidence that supports latent structures; on the contrary, taxonomic reports seem to blur the idea of a structure that supports categorical distinctions (Rosenström et al., 2019).
In any case, the developments in taxometric identification cannot be ignored, as the field still requires refinement and maintains options for its development (Everett & Linscot, 2015). It is also not ruled out that taxonomy can be integrated into a dimensional and continuous psychosis phenotype (Linscott et al., 2017). Ultimately, the evidence seems to favor schizotypy as a dimensional construct (Haslam et al., 2020).
3.6 Multidimensional Model
Multidimensional profiles have been used to understand the influence of schizotypy on affect, cognition, and schizophrenia (Giakoumaki et al., 2016). Scale scores are incomplete when traits are not compared, since a measure of schizotypy is represented by a generalized disposition (Van den Berg et al., 2013). Single-factor models of the scale versions may fail to fit their data based on fit statistics (Cícero et al., 2017).
The term multidimensionality does not represent a new advance. It can be evidenced through the Multidimensional Questionnaire of Schizotypal Traits (MSTQ; Rawlings & Macfarlane, 1994) or in tools such as OLIFE, which are defined as multidimensional and found operability when establishing cognitive correlates (Álvarez, 2005), but lack a complete and up-to-date rationale (Janssens et al., 2016).
This way, the development of the Multidimensional Schizotypy Scale (MSS; Kwapil et al., 2018) and its short version (MSS-B; Gross et al., 2018) are collected, which is based on current conceptual models that take advantage of the positive, negative, and disorganized dimensions; therefore, combining consolidated factors of the SPQ, WSS, and O-LIFE scales, and integrating new characteristics such as experiences of suspicion, passivity, lack of volition, allegiance, and flattened affect (Kwapil et al., 2018; Gross et al., 2018; Kemp et al., 2019; Li et al., 2020).
In conclusion, although the reports show good reliability for MSS and MSS-B (Kemp et al., 2019), even in different ethnic groups (Li et al., 2020), these results are initial, and have pending to reach levels of validation at the time of correlating their results, expanding to crosscultural samples and that their use becomes generalized as that of the tools on which they are based.
3.7 Clinical Implications
The research results highlight how the findings in this field imply important parameters for the clinic. These relationships include cognitive, functional, affective, family, and social parameters (Barrantes et al., 2013; Brosey & Woodward, 2015; Kwapil et al., 2013; Shanon et al., 2014; Wang et al., 2014). Also, some data suggest comorbidity with other mental pathologies (Dembin´ska & Rybakowski, 2016; Kline et al., 2012).
For example, the quality of interpersonal relationships appears to be protective against the risk of experiencing symptoms, it can act as a buffer against the development of SSD (Barrantes et al., 2013), and it is usually an indicator of the need for care (Lin et al., 2013). Decreasing pleasure experiences in the social environment can help in early identification in at-risk populations (Wang et al., 2014).
The use of preventive assessment tools in clinical settings can predict the possibility of psychotic transition (Kotlicka et al., 2019) and establish parameters of adaptation and functionality (Kwapil et al., 2013). Because of the way in which schizotypy and cognition are related, their evaluation can help establish differential diagnoses between different SSDs (Brosey & Woodward, 2015).
Those deficiencies related to schizotypal traits require individualized interventions, understanding that the three dimensions of schizotypy are related differently. Trait-specific intervention appears to improve outcomes in early intervention and functionality programs in individuals with SSD (Dembin´ska & Rybakowski, 2016; Zouraraki et al., 2017).
Each schizotypal dimension is differentially immersed in the expression and pathological experience; therefore, identifying its presence is not enough to establish clinical criteria. For example, as proposed by Kline et al. (2012), the anhedonia parameters that can modulate the type of interventions include the quantity, frequency, intensity, and persistence of these experiences. All this highlights the importance of a comprehensive evaluation in the multidimensional context and over time (Janssens et al., 2016).
4. Discussion
The development of the evaluation of the schizotypy construct during the last decade has implied the use of various methodologies and tools in order to achieve a greater understanding of the phenomenon. This research rescues how effective and valid measurement models were found, cementing consistent findings in the area, and also highlighting the need to adapt them to new theoretical and application advances.
In response to the research purpose, an updated definition of schizotypy can be formulated, specifying it as a multidimensional construct of personality and embedded within the continuum of psychosis. This complex character, although it brings controversies, allows the construct to be an extensive field for the development of research from psychometry, epidemiology, genetic studies, brain structure, and function.
The contribution of this review is to provide an updated and integrative overview of schizotypy from the psychometric tools that have studied it in recent years, and it has found in its results important advances in the study and definition of the construct from the psychometric, the personality, and the clinical, trying to provide a wellfounded and transparent image of the scope of the current literature, which serves as a platform for future advances.
Furthermore, the advances found in psychometry are expressed in terms of its capacity for the assessment and establishment of a behavioral phenotype, which is an essential component for neuroscience, biological psychology, and psychiatry. Schizotype questionnaires offer promising tools for identifying traits and the risk of developing SSD, as well as expanding phenotypic identification beyond the limits of diagnostic categorization.
Although it has been possible to draw some guidelines for the clinic, the research reports express them with due caution. This implies a challenge in the generation of data that can be translated to the clinic. Additionally, the use of large university samples and small high-risk groups, as well as the fact that quality research is limited to certain geographic spaces, imply local challenges for the development of the construct, not only in terms of converting the results to own, but also because of the wealth of information that diversity can imply for the field in general. One of the limitations of this review is the exclusion of research with adolescents, which represents a wide body of work that is undoubtedly key to understanding the construct from its origin and development. By focusing on the definition of the construct, adolescents were outside the scope of this article, but they represent an important resource that could be integrated into future research.
Accordingly, future lines of research can be established: in the first place, the importance of choosing the right tools, understanding the complexity and multidimensionality of the construct, and taking advantage of the complementary capacity between them; secondly, even with the considerable amount of research already produced, there are still gaps, contradictions, and undefined margins, which require the expansion of the capacity to conceptualize and measure this phenomenon.
Additionally, it is necessary to generate new research that manages to connect the contributions previously formulated, giving them relevance when evaluating, approaching, and intervening in individuals in the clinical, subclinical, and non-pathological ranges. This can occur in the formulation of protocols for prevention and intervention, or when complementing existing resources with the new discoveries achieved.
Finally, it is worth highlighting the usefulness of psychometry for schizotypy in other fields related to mental health such as psychiatry, neurology, and even those related to the well-being of the individual and their relationship with the world. The approach to such complex and intricate phenomena requires interdisciplinary articulations to achieve scientific production that fully understands them.
References
Álvarez, E. (2005). Personalidad esquizotípica y marcadores cognitivos: correlatos cognitivos en la esquizotipia psicométrica [Tesis doctoral. Universidad de Barcelona]. http://diposit.ub.edu/ dspace/bitstream/2445/42551/1/EAL_TESIS. pdf
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5a ed.). American Psychiatric Association.
Ashton, M., Lee, K., Vries, E., Hendrickse, J., & Born, M. (2012). The Maladaptive Personality Traits of the Personality Inventory forDSM-5(PID-5) in Relation to the HEXACO Personality Factors and Schizotypy/Dissociation. Journalof Personality Disorders, 26 (5), 641-659. https://doi.org/10.1521/pedi.2012.26.5.641
Badcock, J., Barkus, E., Cohen, A. S., Bucks, R., & Badcock, D. (2016). Loneliness and Schizotypy Are Distinct Constructs, Separate from General Psychopathology. Frontiers in Psychology, 7. https://doi.org/10.3389/fpsyg.2016.01018
Barrantes-Vidal, N., Chun, C., Myin-Germeys, I., & Kwapil, T. (2013). Psychometric schizotypy predicts psychotic-like, paranoid, and negative symptoms in daily life. Journal of Abnormal Psychology,122 (4), 1077-1087. https: //doi.org/10.1037/a0034793
Belloch, A., & Fernández, H. (2010). Tratado de los trastornos de la personalidad. Editorial Síntesis.
Blanchard, J., Collins, L., Aghevli, M., Leung, W., & Cohen, A. (2011). Social Anhedonia and Schizotypy in a Community Sample: The Maryland Longitudinal Study of Schizotypy. Schizophrenia Bulletin, 37 (3), 587-602. https://doi.org/10.1093/schbul/sbp107
Bora, E. (2020). Theory of mind and schizotypy: A metaanalysis. Schizophrenia Research, 222, 97-103. https://doi.org/10.1016/j.schres.2020.04.024
Bora, E., Lin, A., Wood, S., Yung, A., McGorry, P., & Pantelis, C. (2014). Cognitive deficits in youth with familial and clinical high risk to psychosis: A systematic review and meta-analysis. Acta Psychiatrica Scandinavica, 130 (1), 1-15. https://doi.org/10.1111/acps.12261
Brosey, E., & Woodward, N. (2015). Schizotypy and clinical symptoms, cognitive function, and quality of life in individuals with a psychotic disorder. Schizophrenia Research, 166 (1-3), 92-97. https://doi.org/10.1016/j.schres.2015.04.038
Burgin, C., Chun, C., Horton, L., Barrantes, N., & Kwapil, T. (2014). Splitting of Associative Threads: The Expression of Schizotypal Ambivalence in Daily Life. Journal of Psychopathology and Behavioral Assessment, 37 (2), 349-357. https://doi.org/10.1007/s10862-014-9457-7
Cabrera, S., Michel, C., & Cruzado, L. (2017). Estados clínicos de alto riesgo para esquizofrenia y otras formas de psicosis: Una breve revisión. Revista de neuro-psiquiatría, 80 (1), 42-59.
Callaway, D., Cohen, A., Matthews, R., & Dinzeo, T. (2014). Schizotypal Personality QuestionnaireBrief Revised: Psychometric replication and extension. Personality Disorders, 5 (1), 32-38. https://doi.org/10.1037/per0000041
Campellone, T., Elis, O., Mote, J., Sanchez, A., & Kring, A. (2016). Negative symptoms in psychometrically defined schizotypy: The role of depressive symptoms. Psychiatry Research, 240, 181-186. https://doi.org/10.1016/j.psychres.2016.04.020
Chan, C., Bulbena-Cabre, A., Rutter, S., Benavides, C., McClure, M., Calabrese, W., & Perez-Rodriguez, M. (2019). Comparisonofself-reportandclinicianrated schizotypal traits in schizotypal personality disorder and community controls. Schizophrenia Research, 209, 263-268. https://doi.org/10.1016/j.schres.2018.12.050
Chan, R., Wang, Y., Zhao, Q., Yan, C., Xu, T., Gong, Q., & Manschreck, T. (2010). Neurological Soft Signs in Individuals with Schizotypal Personality Features. Australian & New Zealand Journal of Psychiatry, 44 (9), 800-804. https://doi.org/10.3109/00048674.2010.482920
Chau, A., Zhu, C., & So, S. (2019). Loneliness and the psychosis continuum: A meta-analysis on positive psychotic experiences and a meta-analysis on negative psychotic experiences. International Review of Psychiatry, 31, 1-20. https://doi.org/10.1080/09540261.2019.1636005
Cheli, S., Lysaker, P., & Dimaggio, G. (2019). Metacognitively oriented psychotherapy for schizotypal personality disorder: A twocase series. Personality and Mental Health, 13 (3), 155-167. https://doi.org/10.1002/pmh.1447
Cícero, D., Jonas, K., Li, K., Perlman, G., & Kotov, R. (2019). Common Taxonomy of Traits and Symptoms: Linking Schizophrenia Symptoms, Schizotypy, and Normal Personality. Schizophrenia Bulletin, 45 (6), 1336-1348. https://doi.org/10.1093/schbul/sbz005
Cícero, D., Martin, E., Becker, T., Docherty, A., & Kerns, J. (2014). Correspondence between psychometric and clinical high risk for psychosis in an undergraduate population. Psychological Assessment, 26 (3), 901-915. https://doi.org/10.1037/a0036432
Cícero, D., Neis, A., Klaunig, M., & Trask, C. (2017). The Inventory of Psychotic-Like Anomalous SelfExperiences (IPASE): Development and validation. Psychological Assessment, 29 (1), 13-25. https://doi.org/10.1037/pas0000304
Cohen, A., Beck, M., Najolia, G., & Brown, L. (2011). Affective disturbances in psychometrically defined schizotypy across direct, but not indirect assessment modes. Schizophrenia Research, 128 (1-3), 136-142. https://doi.org/10.1016/j.schres.2011.02.004
Debbane, M., Eliez, S., Badoud, D., Conus, P., Fluckiger, R., & Schultze-Lutter, F. (2014). Developing Psychosis and Its Risk States Through the Lens of Schizotypy. Schizophrenia Bulletin,41 (2), 396-407. https://doi.org/10.1093/schbul/sbu176
Debbané, M., & Mohr, C. (2015). Integration and Development in Schizotypy Research: An Introduction to the Special Supplement. Schizophrenia Bulletin, 41 (2), 363-365. https://doi.org/10.1093/schbul/sbv003
Dembin´ska, D., & Rybakowski, J. (2016). The assessment of schizotypy by the O-LIFE in patients with schizophrenia and affective disorders. Psychiatr. Pol, 50 (6), 1147-1156. https://doi.org/10.12740/PP/62335
Deyo, C., & Langdon, R. (2019). “Formal Thought Disorder” in a General-Community Sample with Elevated Schizotypal Traits. The Journal of Nervous and Mental Disease, 207 (5), 410-416. https://doi.org/10.1097/nmd.0000000000000991
DeYoung, C., Grazioplene, R., & Peterson, J. (2012). From madness to genius: The Openness/Intellect trait domain as a paradoxical simplex. Journal of Research in Personality, 46 (1), 63-78. https://doi.org/10.1016/j.jrp.2011.12.003
Edmundson, M., Lynam, D., Miller, J., Gore, W., & Widiger, T. (2011). A Five-Factor Measure of Schizotypal Personality Traits. Assessment, 18 (3),321-334.https://doi.org/10.1177/1073191111408228
Everett, K., & Linscott, R. (2015). Dimensionality vs Taxonicity of Schizotypy: Some New Data and Challenges Ahead. Schizophrenia Bulletin, 41 (2), 465-474. https://doi.org/10.1093/schbul/sbu221
Flückiger, R., Michel, C., Grant, P., Ruhrmann, S., Vogeley, K., Hubl, D., & Schultze-Lutter, F. (2019). The interrelationship between schizotypy, clinical high risk for psychosis and related symptoms: Cognitive disturbances matter. Schizophrenia Research, 210, 188-196. https://doi.org/10.1016/j.schres.2018.12.039
Fonseca, E., & Inchausti, F. (2018). Actualización en la prevención de los trastornos del espectro psicótico. Papeles del Psicólogo, 39 (2), 127-139.
Fonseca-Pedrero, E., Ortuño-Sierra, J., Lucas-Molina, B., Debbané, M., Chan, R., Cicero, D., & Voracek, M. (2018). Brief assessment of schizoty-pal traits: A multinational study. Schizophrenia Research, 197, 182-191. https://doi.org/10.1016/j.schres.2017.10.043
Fumero, A., Rodríguez, M., Roa, A., & Peñate, W. (2017). Importancia diferencial de los componentes fundamentales de la esquizotipia: Un metaanálisis. Revista Latinoamericana de Psicología, 49 (1),5-18. https://doi.org/10.1016/j.rlp.2016.09.001
Giakoumaki, S. (2016). Emotion processing deficits in the different dimensions of psychometric schizo-typy. Scandinavian Journal of Psychology, 57 (3), 256-270. https://doi.org/10.1111/sjop.12287
Giakoumaki, S., Karagiannopoulou, L., Rózsa, S., Zouraraki, C., Karamaouna, P., & Cloninger, C. (2016). Psychometric properties of the Greek TCI-R and its clinical correlates: schizotypy and the self-regulation of affective and cognitive functioning. PeerJ, 4, e1830. https://doi.org/10.7717/peerj.1830
Gross, G., Kwapil, T., Burgin, C., Raulin, M., Silvia, P., Kemp, K., & Barrantes-Vidal, N. (2018). Validation of the Multidimensional Schizotypy ScaleBrief in Two Large Samples. Journalof Psychopathology and Behavioral Assessment, 40, 669-677. https://doi.org/10.1007/s10862-018-9668-4
Gross, G., Mellin, J., Silvia, P., Barrantes-Vidal, N., & Kwapil, T. (2014). Comparing the factor structure of the Wisconsin Schizotypy Scales and the Schizotypal Personality Questionnaire. Person-ality Disorders: Theory, Research, and Treatment, 5 (4), 397-405. https://doi.org/10.1037/per0000090
Haslam, N. (2019). Unicorns, snarks, and personality types: A review of the first 102 taxometric studies of personality. Australian Journal of Psychology, 71, 39-49.
Haslam, N., McGrath, M., Viechtbauer, W., & Kuppens, P. (2020). Dimensions over categories: A meta-analysis of taxometric research. Psychological Medicine, 1-15. https://doi:10.1017/s003329172000183x
Janssens, M., Boyette, L., Heering, H., Bartels-Velthuis, A., Lataster, T., Kahn, R., & Myin-Germeys,I. (2016). Developmental course of subclinical positive and negative psychotic symptoms and their associations with genetic risk status and impairment. Schizophrenia Research, 174 (1-3), 177-182. https://doi.org/10.1016/j.schres.2016. 03.028
Karagiannopoulou, L., Karamaouna, P., Zouraraki, C., Roussos, P., Bitsios, P., & Giakoumaki, S. (2016). Cognitive profiles of schizotypal dimensions in a community cohort: Common properties of differential manifestations. Journal of Clinical and Experimental Neuropsychology, 38 (9), 1050-1063. https://doi.org/10.1080/13803395.2016.1188890
Kemp, K., Bathery, A., Barrantes-Vidal, N., & Kwapil, T. (2020). Positive, Negative, and Disorganized Schizotypy Predict Differential Patterns of Interview-Rated Schizophrenia-Spectrum Symptoms and Impairment. Assessment, 28 (1), 141-152. https://doi.org/10.1177/1073191119900008
Kemp, K., Gross, G., & Kwapil, T. (2019). Psychometric Properties of the Multidimensional Schizotypy Scale and Multidimensional Schizotypy ScaleBrief: Item and Scale TestRetest Reliability and Concordance of Original and Brief Forms. Journal of Personality Assessment, 102 (4), 1-8. https://doi.org/10.1080/00223891.2019.1591425
Kline, E., & Schiffman, J. (2014). Psychosis risk screening: Asystematic review. Schizophrenia Research, 158 (1-3), 11-18. https://doi.org/10.1016/j.schres.2014.06.036
Kline, E., Wilson, C., Ereshefsky, S., Nugent, K., Pitts, S., Reeves, G., & Schiffman, J. (2012). Schizotypy, psychotic-like experiences and distress: An interaction model. Psychiatry Res, 200 (0), 647- 651. https://doi.org/10.1016/j.psychres.2012.07.047
Kocsis, K., Kotulla, S., Maier, S., Voracek, M., & HennigFast, K. (2017). Cognitive Correlates of Different Mentalizing Abilities in Individualswith High and Low Trait Schizotypy: Findings from an Extreme-Group Design. Frontiers in Psychology, 8. https://doi.org/10.3389/fpsyg .2017.00922
Kocsis, K., Nemes, Z., & Perczel-Forintos, D. (2016). Factorial structure of the Hungarian version of Oxford-Liverpool Inventory of Feelings and Experiences and its applicability on the schizophrenia-schizotypy continuum. Personality and Individual Differences, 90, 130-136. https://doi. org/10.1016/j.paid.2015.10.039
Kotlicka, M., Karbownik, M., Paweczyk, A., urner, N., Paweczyk, T., Strzelecki, D., & Urban-Kowalczyk, M. (2019). A developmentally-stable pattern of premorbid schizoid-schizotypal features predicts psychotic transition from the clinical high-risk for psychosis state. Comprehensive Psychiatry, 90, 95-101. https://doi.org/10.1016/j.comppsych.2019.02.003
Kwapil, T., & Barrantes-Vidal, N. (2014). Schizotypy: Looking Back and Moving Forward. Schizophrenia Bulletin, 41 (2), 366-373. https://doi.org/10.1093/schbul/sbu186
Kwapil, T., Brown, L., Silvia, P., Myin-Germeys, I., & Barrantes-Vidal, N. (2012). The expression of positive and negative schizotypy in daily life: An experience sampling study. Psychological Medicine, 42 (12), 2555-2566. https://doi.org/10.1017/s0033291712000827
Kwapil, T., Gross, G., Silvia, P., & Barrantes-Vidal, N. (2013). Prediction of psychopathology and functional impairment by positive and negative schizotypy in the Chapmans’ ten-year longitudinal study. Journal of Abnormal Psychology, 122 (3), 807-815. https://doi.org/10.1037/a0033759
Kwapil, T., Gross, G., Silvia, P., Raulin, M., & BarrantesVidal, N. (2018). Development and psychometric properties of the Multidimensional Schizotypy Scale: A new measure for assessing positive, negative, and disorganized schizotypy. Schizophrenia Research, 193, 209-217. https://doi.org/10.1016/j.schres.2017.07.001
Lawrie, S., Olabi, B., Hall, J., & Mcintosh, A. (2011). Do we have any solid evidence of clinical utility about the pathophysiology of schizophrenia? World Psychiatry, 10 (1), 19-31. https://doi:10.1002/j.2051-5545.2011.tb00004.x
Li, L., Meyer, M., Martin, E., Gross, G., Kwapil, T., & Cicero, D. (2020). Differential item functioning of the Multidimensional Schizotypy Scale and Multidimensional Scale-Brief across ethnicity. Psychological Assessment, 32 (4), 383-393. https://doi.org/10.1037/pas0000798
Liberati, A., Altman, D., Tetzlaff, J., Mulrow, C., Gotzsche, P., Loannidis, J. P., Clarke, M., & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and metaanalyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Medicine, 6 (7). https://doi.org/10.1371/journal.pmed.1000100
Lin, A., Wigman, J., Nelson, B., Wood, S., Vollebergh, W., van Os, J., & Yung, A. (2013). Follow-up factor structure of schizotypy and its clinical associations in a help-seeking sample meeting ultra-high risk for psychosis criteria at baseline. Comprehensive Psychiatry, 54 (2), 173-180. https://doi.org/10.1016/j.comppsych.2012.06.011
Linscott, R., Morton, S., Alizadeh, B., Bartels-Velthuis, A., van Beveren, N., & Bruggeman, R. (2017). The Latent Taxonicity of Schizotypy in Biological Siblings of Probands with Schizophrenia. Schizophrenia Bulletin, 44 (4), 922-932. https://doi.org/10.1093/schbul/sbx143
Mason, O. (2015). The Assessment of Schizotypy and Its Clinical Relevance. Schizophrenia Bulletin, 41 (2), 374-385. https://doi.org/10.1093/schbul/sbu194
Mason, O., Claridge, G., & Jackson, M. (1995). New scales for the assessment of schizotypy. Personality and Individual Differences, 18 (1), 7-13.
Meehl, P. (1992). Factors and taxa, traits and types, difference of degree and differences in kind. Journal of Personality, 60, 117-174.
Mitchell, K., & Cohen, A. (2017). Cognitive functioning in schizotypy through the lens of the accessibility model. Cognitive Neuropsychiatry, 22 (5), 422-435. https://doi.org/10.1080/13546805.2017.1371585
Moritz, S., Andresen, B., & Sengutta, M. (2019). The specificity of schizotypal scales and some implications for clinical high-risk research. Personality and Individual Differences, 151. https://doi.org/10.1016/j.paid.2019.05.056
Nelson, M., Seal, M., Pantelis, C., & Phillips, L. (2013). Evidence of a dimensional relationship between schizotypy and schizophrenia: A systematic review. Neuroscience & Biobehavioral Reviews, 37 (3), 317-327. https://doi.org/10.1016/j.neubiorev.2013.01.004
Nenadic, I., Lorenz, C., Langbein, K., Dietzek, M., Smesny, S., Schönfeld, N., & Gaser, C. (2015). Brain structural correlates of schizotypy and psychosis proneness in a non-clinical healthy volunteer sample. Schizophrenia Research, 168 (1-2), 37-43. https://doi.org/10.1016/j.schres.2015.06.017
Nitzburg, G. C., Malhotra, A. K., & DeRosse, P. (2013). The relationship between temperament and character and subclinical psychotic-like experiences in healthy adults. European Psychiatry, 29 (6), 352-357. https://doi.org/10.1016/j.eurpsy.2013.11.006
Oezgen, M., & Grant, P. (2018). Odd and DisorganizedComparing the factor structure of the three major schizotypy inventories. Psychiatry Research, 267, 289-295. https://doi.org/10.1016/j.psychres.2018.06.009
Rabin, S., Hasson, I., Avidan, M., Rozencwaig, S., Shalev, H., & Kravetz, S. (2014). Metacognition in schizophrenia and schizotypy: relation to symptoms of schizophrenia, traits of schizotypy and Social Quality of Life. The Israel journal of psychiatry and related sciences, 51 (1), 44-53. https://pubmed.ncbi.nlm.nih.gov/24858634/
Ragsdale, K., & Bedwell, J. (2013). Relationships between dimensional factors of psychopathy and schizotypy. Frontiers in Psychology, 4. https://doi:10.3389/fpsyg.2013.00482
Raine, A. (1991). The SPQ: A scale for the assessment of schizotypal personality based on DSM-III-R criteria. Schizophrenia Bulletin, 17 (4), 555-564.
Rawlings, D., & MacFarlane, C. (1994). A multidimensional schizotypal traits questionnaire for young adolescents. Personality and Individual Differences, 17 (4), 489-496. https://doi.org/10.1016/0191-8869(94)90086-8
Rosenström, T., Gjerde, L., Krueger, R., Aggen, S., Czajkowski, N., Gillespie, N., & Ystrom, E. (2019). Joint factorial structure of psychopathology and personality. Psychological Medicine, 49, 2158-2167.
Shanon, X., Best, M., Schorr, E., & Bowie, C. R. (2014). Neurocognition, functional competence and selfreported functional impairment in psychometrically defined schizotypy. Cognitive Neuropsychiatry, 20 (1), 53-63. https://doi:10.1080/13546805.2014.969419
Shea, B., Grimshaw, J., Wells, G., Boers, M., Andersson, N., Hamel, C., & Bouter, L. (2007). Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Medical Research Methodology, 7 (1), Article 10. https://doi.org/10.1186/1471-2288-7-10
Shrout, P., & Rodgers, J. (2018). Psychology, Science, and Knowledge Construction: Broadening Perspectives from the Replication Crisis. Annual Review of Psychology, 69 (1), 487-510. https://doi.org/10.1146/annurev-psych-122216-011845
Siddi, S., Petretto, D., & Preti, A. (2017). Neuropsychological correlates of schizotypy: A systematic review and meta-analysis of cross-sectional studies. Cognitive Neuropsychiatry, 22 (3), 186- 212. https://doi.org/10.1080/13546805.2017.1299702
Soler, J., Ferentinos, P., Prats, C., Miret, S., Giralt, M., Peralta, V., & Fatjó-Vilas, M. (2017). Familial aggregation of schizotypy in schizophreniaspectrum disorders and its relation to clinical and neurodevelopmental characteristics. Journal of Psychiatric Research, 84, 214-220. https://doi.org/10.1016/j.jpsychires.2016.09.026
Somma, A., Krueger, R., Markon, K., Borroni, S., & Fos-sati, A. (2019). Schizotypy from the Perspective of the DSM-5 Alternative Model of Personality Traits: A Study on a Sample of 1056 Italian Adult University Students. J Psychopathol Be-hav Assess, 41, 560-573. https://doi.org/10.1007/s10862-019-09718-1
Suzuki, T., Samuel, D., Pahlen, S., & Krueger, R. (2015). DSM-5 alternative personality disorder model traits as maladaptive extreme variants of the five-factor model: An item-response theory analysis. Journal of Abnormal Psychology, 124 (2), 343-354. https://doi.org/10.1037/abn0000035
Torbet, G., Schulze, D., Fiedler, A., & Reuter, B. (2015). Assessment of self-disorders in a non-clinical population: Reliability and association with schizotypy. Psychiatry Research, 228 (3), 857-865. https://doi.org/10.1016/j.psychres.2015.05.011
Tortella, M., Baños, R., Barrantes, N., Botella, C., Fernández, F., García, J., & Vázquez, C. (2016). Retos de la investigación psicológica en salud mental. Clínica y Salud, 27 (1), 37-43. https://doi.org/10.1016/j.clysa.2016.02.001
Torti, M., Buzzanca, A., Squarcione, C., Salerno, C., Mirigliani, A., Di Fabio, F., & Biondi, M. (2013). Schizotypy and personality profiles of Cluster A in a group of schizophrenic patients and their siblings. BMC Psychiatry, 13 (1). https://doi.org/10.1186/1471-244x-13-245
Trask, C., Cohn, J., Paxson, A., Hansen, G., & Cicero,D. (2019). Form and content of attenuated psychotic symptoms in psychometrically assessed positive and negative schizotypy. Early Intervention in Psychiatry, 14 (3), 321-329. https://doi.org/10.1111/eip.12856
Van den Berg, S., Paap, M., & Derks, E. (2013). Using multidimensional modeling to combine selfreport symptoms with clinical judgment of schizotypy. Psychiatry Research, 206 (1), 75-80. https://doi.org/10.1016/j.psychres.2012.09.015
Wang, Y., Lui, S., Zou, L., Zhang, Q., Zhao, Q., Yan, C.,& Chan, R. (2014). Individuals with psychometric schizotypy show similar social but not physical anhedonia to patients with schizophrenia. Psychiatry Research, 216 (2), 161-167. https://doi.org/10.1016/j.psychres.2014.02.017
Winterstein, B., Ackerman, T., Silvia, P., & Kwapil, T. (2011). Psychometric Properties of the Wisconsin Schizotypy Scales in an Undergraduate Sample: Classical Test Theory, Item Response Theory, and Differential Item Functioning. Journal of Psychopathology and Behavioral Assessment, 33 (4), 480-490. https://doi.org/10.1007/s10862-011-9242-9
Xi, C., Cai, Y., Peng, S., Lian, J., & Tu, D. (2019). A diagnostic classification version of Schizotypal Personality Questionnaire using diagnostic classification models. International Journal of Methods in Psychiatric Research, 29 (1), e1807. https://doi.org/10.1002/mpr.1807
Zhang, R., Zhou, H., Wang, Y., Yang, Z., Wang, Y., So, S., & Cheungf, E. (2019). Network analysis of schizotypal personality traits and their association with other subclinical psychiatric features. Asian Journal of Psychiatry, 44, 209-216. https://doi.org/10.1016/j.ajp.2019.08.005
Zouraraki, C., Karamaouna, P., Karagiannopoulou, L., & Giakoumaki, S. (2017). Schizotypy-Independent and Schizotypy-Modulated Cognitive Impairments in Unaffected First-Degree Relativesof Schizophrenia-spectrum Patients. Archives of Clinical Neuropsychology, 32 (8), 1010-1025. https://doi.org/10.1093/arclin/acx029
Notes
Author notes
⋆Corresponding author: Cristhian Javier Rivera Tapia. Email: c.riveratapia@hotmail.com
Conflict of interest declaration