Odontologia
Accuracy of cone-beam CT in detecting vertical root fractures in teeth with post-endodontic restorations: an in vitro study
Accuracy of cone-beam CT in detecting vertical root fractures in teeth with post-endodontic restorations: an in vitro study
Acta Scientiarum. Health Sciences, vol. 43, e54332, 2021
Universidade Estadual de Maringá
Recepción: 15 Septiembre 2020
Aprobación: 18 Enero 2021
Abstract: The aim of this study was to evaluate the accuracy of cone-beam CT (CBCT) for the detection of artificially created vertical root fractures (VRF) in extracted teeth restored with metallic (MP) and fiberglass (FGP) posts. After root canal obturation, 60 extracted human premolars were scanned by using the highest-resolution settings of a CBCT unit. The prepared roots were randomly divided into three groups: group C (control group): non-restored and non- endodontically treated teeth (n = 20); group MP (n = 20); group FGP (n = 20). In all groups, 10 teeth were artificially fractured. Two external and independent observers blindly recorded the presence or absence of VRF. Sensitivity, specificity, accuracy, intra- and interobserver agreement were calculated. Kappa value for inter- and intraobserver agreement was 0.82 and 0.84 respectively, demonstrating good agreement. The highest values for sensitivity (0.80 - 0.90), specificity (1.00) and accuracy (0.90 - 0.95) were found in the control group. The teeth with FGP restoration presented the lowest sensitivity (0.30 - 0.50) and accuracy (0.60 - 0.65) values. Both examiners had a good performance in the diagnosis of fractures in teeth with MP, with accuracy ranging between 0.85 - 0.90. The presence of MP did not influence accuracy; however, the presence of FGP reduced the diagnostic capacity of CBCT.
Keywords: diagnosis, tooth fracture, in vitro, diagnostic imaging.
Introduction
The diagnosis of vertical root fractures (VRF) represent a major challenge in the clinic, with an overall prevalence of 3.69 to 31.7% (Morfis, 1990; Tamse, 2006; Yoshino, Ito, Kuroda, & Sugihara, 2015). They are more frequent in endodontically treated teeth and posts restoration represents its main etiological factor (Tamse, 2006). It is postulated that the fracture resistance of reconstructed teeth with metallic (MP) and fiberglass (FGP) posts is similar (Mitsui, Marchi, Pimenta, & Ferraresi, 2004). Nevertheless, because MP presents an elasticity module superior to FGP, it is associated with greater stress on dentin and, therefore, requires greater strength (Bacchi et al., 2013). On the other hand, prefabricated FGP has an elastic modulus similar to that of dentin and provides a homogeneous stress distribution (Barjau-Escribano et al., 2006) along the dentin/post interface. In addition, in the medium term, in cases of restoration of teeth treated endodontically with no more than two remaining coronal walls, the FGP had higher overall survival rates (3 to 7 years) than the MP (Wang et al., 2019).
A complete dental history with collection of signs and symptoms is essential in the diagnosis of VRF, followed by a careful radiographic examination, in which the fracture line can be observed. In addition, periodontal ligament thickening and localized periradicular and vertical bone loss are important radiographic characteristics (Tamse, 2006). For this purpose, periapical radiographs are often used. However, the fracture line is not visualized in many cases, especially in those with cracks and fractures without fragment separation (Tamse, 2006). The presence of radiopaque materials such as gutta-percha or artificial crowns can create artefacts, making diagnosis more difficult (Talwar et al., 2016).
Considering that conventional radiographs are not accurate to detect VRF (Bernardes et al., 2009), cone-beam CT (CBCT) has emerged as an alternative resource, especially in the diagnosis of buccal-lingual fractures. Therefore, the aim of this study was to evaluate the accuracy of CBCT for the detection of artificially created VRF in extracted endodontically treated teeth restored with MP and FGP. The null hypothesis was that the accuracy of CBCT does not vary depending on the postoperative system.
Material and methods
This in vitro study was approved by the Ethics Committee on Research Involving Human Beings (number: 2.058.912; CAAE: 67199717.0.0000.0104). The sample consisted of 60 human second mandibular premolars extracted due to periodontal disease or orthodontic treatment. Periapical radiographs were taken, so that teeth with only one root canal were included. Teeth that had endodontic treatment, intracanal calcifications and roots with caries, resorption, fracture, malformations and sharp dilacerations were excluded. Then, the teeth were stored in 0.1% thymol solution to prevent dehydration.
The teeth were then randomly distributed in three groups: group C (control group): teeth not treated endodontically and not restored with pins (n = 20); group MP: endodontically treated teeth restored with MP (n = 20); and group FGP: endodontically treated teeth restored with FGP (n = 20).
Endodontic treatment
All teeth (experimental groups) were prepared by a single operator using hand files. First, a #10 k-file was used for patency. Root canal instrumentation was performed with 1st and 2nd series nickel-titanium K files (Dentsply Maillefer, Ballaigues, Switzerland) using the crown-down technique, rinsing with 2.5% sodium hypochlorite. Later, the application of 2 mL of 17% ethylene diamine tetraacetic acid (EDTA) (Biodinâmica, Biodinâmica Química e Farmacêutica Ltda, Ibiporã, Paraná, BR) was performed for three minutes. Finally, each canal was irrigated with 2 mL of 2.5% sodium hypochlorite to neutralize the action of the EDTA. Then, root canals were filled with gutta-percha and Endofill sealer (Dentsply Ind. e Com., Petrópolis, RJ, Brazil) using the lateral condensation technique.
Post-endodontic restorations
After root canal obturation, the crowns were removed at 3 mm from cement-enamel junction using flexible diamond discs (KG Sorensen, Cotia, SP, Brazil). Then, the canals were prepared for post fixation. Gutta-percha was removed using a #2 Peeso reamer (Dentsply Maillefer, Ballaigues, Switzerland) up to 2 3-1 of the working length, to allow preparation for root posts.
FGP number 1 (Exacto, Angelus, Londrina, PR, Brazil) was used, and cast MP was obtained by direct modeling with a prefabricated acrylic post–core pattern (Pin-Jet, Angelus, Londrina, PR, Brazil) and acrylic resin (DuraLay/Reliance, IL, EUA). All posts were cemented with glass ionomer cement (Maxxion C, FGM, Joinville, SC, Brazil) following the manufacturer’s instructions. Before cementation, conditioning with polyacrylic acid (Maxxion C liquid, FGM, Joinville, SC, Brazil) was carried out for 20 seconds.
In a laboratory environment, 10 teeth for each group (C, MP, FGP), randomly selected, were inserted into a mold made of acrylic resin. Then, these specimens were submitted to the fracture strength test using a universal testing machine (EMIC - DL 1000, EMIC, São José dos Pinhais, PR, Brazil). A standard compressive load was applied in the vertical direction with a crosshead speed of 1 mm/min until the fracture occurred in the middle and apical thirds. Although the teeth were restored with different materials, the standardization of the method sought to produce similar fractures in the entire sample, always in the vertical direction.
CBCT imaging
For CBCT image acquisition, teeth were covered with a thin layer of utility wax (Tenatex Red; Kemdent, Swindon, UK). Then, they were fixed in prefabricated sockets in dry human mandibles, which were coated with three layers of wax buccally and lingually to provide soft-tissue simulation (Tolentino et al., 2020). The samples were scanned in the i-Cat Next Generation® equipment (Imaging Sciences International, Hatfield, Pennsylvania, USA) according to manufacturer’s protocol and using the highest-resolution settings (8 x 8 cm FOV, 0.125 mm voxel size, 120 Kv, 37.07 mA). The mandible was positioned with its occlusal plane parallel to the ground and its mid-sagittal plane perpendicular to the ground. Images were examined by using the scanners’ proprietary software (Xoran 3.1.62 version, Xoran Technologies, Ann Arbor, MI) in parasagittal, axial and coronal slices (Figure 1). Two external and independent radiologists (both with 10 years of experience with CBCT) performed a blind analysis of each exam, in which they were asked about the presence or absence of the fracture. Calibration was carried out with 20% of the sample, randomly selected, with an interval of 15 days. All analyzes were performed in a semi-dark and silent room and the examiner was instructed to perform intervals between analyzes to avoid eye fatigue.
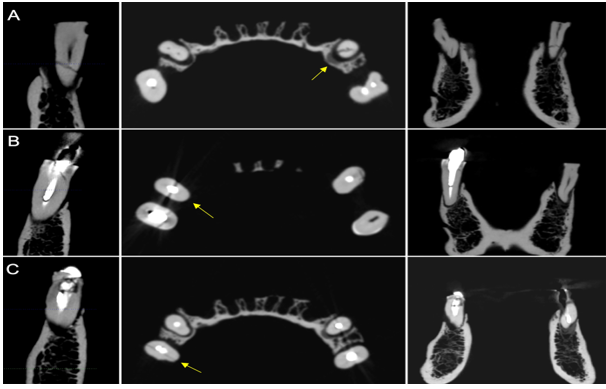
Figure 1. CBCT i-Cat® reconstructions. Parasagittal, axial (arrow) and coronal slices showing the VRF in (A) non-restored teeth, (B) in teeth with MP and (C) with FGP.
Statistical analysis
A diagnostic test was used to predict the presence or absence of a VRF, considering that the two basic measures of quantifying the diagnostic accuracy are sensitivity and specificity. Sensitivity, specificity and accuracy were calculated for CBCT. Kappa index was used to assess inter and intraobserver agreement. All statistical procedures were computed with R 3.2 for Windows (R Foundation for Statistical Computing, Vienna, Austria). The significance level was set at 5%.
Results
Kappa value for inter and intraobserver agreement was 0.82 and 0.84 respectively (almost perfect agreement). The highest values for sensitivity (0.80-0.90), specificity (1.00) and accuracy (0.90 - 0.95) were found in the control group.
Examiner 1 did not perform well in detecting fractures (sensitivity) in teeth with FGP (0.50); a better performance was observed in the diagnosis of absence of fracture (specificity) (0.80). The accuracy (0.65) was also not high, indicating low diagnostic power. Similarly, for examiner 2, sensitivity was low (0.30) and specificity was better, with 90% accuracy. Both examiners performed well in diagnosing fractures in teeth with MP, both in sensitivity (0.70 - 0.80) and in specificity (1.00) (Table 1), despite the presence of beam hardening artefacts.

Discussion
The aim of the study was to verify the performance of CBCT in identifying the presence of VRF, depending on each type of restorative treatment on the tooth. For this, metrics were used to assess the examiner's ability to find ‘true values’, through accuracy, sensitivity and specificity. The accuracy of statistical information is the degree to which the information correctly describes the phenomena/standard it was designed to measure, i.e., if the examiner is able to indicate a positive result when there is a fracture and a negative result when there is no fracture. The two basic measures of quantifying the diagnostic accuracy of a test are the sensitivity and specificity. Sensitivity (true positive rate) is the test's ability to detect true positives, i.e., when the examiner detects the fracture when it actually exists. Specificity (true negative rate) is the test's ability to detect true negatives, i.e., when the examiner does not detect the fracture when it actually does not exist. According to the results of the present study, VRFs were visualized in the CBCT images, and the accuracy varied according to the restorative treatment. Thus, the null hypothesis was rejected.
As stated previously (Bernardes et al., 2009; Hassan, Metska, Ozok, van der Stelt, & Wesselink, 2009; Talwar et al., 2016), our results indicated that CBCT imaging is reliable to detect VRF, especially in non-restored teeth. Using CBCT, Talwar et al. (2016) showed a diagnostic odds ratio of 5.53 and 94.26 for endodontically treated (unpinned) and non-treated teeth, respectively. Hassan et al. (2009) found that CBCT is more sensitive in the diagnosis of VRF when compared to periapical radiographs, although the specificity (true negative rate) values were similar. They found lower values for specificity in teeth with endodontic treatment, although this did not influence the overall accuracy (Hassan et al., 2009). Bernardes et al. (2009) also reported statistically significant differences between periapical radiographs and CBCT for the diagnosis of root fractures, with better results for CBCT. Although some authors suggest that root canal sealers can affect the resistance and the pattern of the fracture (Lertchirakarn, Timyam, & Messer, 2002), and that, especially glass ionomer cement can strengthen the root dentin (Trope & Ray, 1992), more recent investigations have concluded that sealers have no effect on fracture resistance (Yusufoglu, Akman, Akbulut, & Eldeniz, 2019).
It is known that high-density materials (gutta-percha and MP) can induce beam hardening artifacts, which present themselves as striations (Talwar et al., 2016) that can hide or mimic fracture lines and, consequently, deceive the clinician (Byakova, Novozhilova, Makeeva, Grachev, & Kasatkina, 2019a). These artefacts significantly degrade CBCT image (Neves, Freitas, Campos, Ekestubbe, & Lofthag-Hansen, 2014) and reduce the sensitivity and accuracy of the exam in detecting VRF (Hassan et al., 2010; Menezes et al., 2016; Byakova, Novozhilova, Makeeva, Grachev, & Kasatkina, 2019b). As expected, we found that sensitivity, specificity and accuracy were higher in non-restored teeth. However, despite the presence of beam hardening artifacts, MP did not negatively influence the specificity, corroborating Jakobson et al. (2014), but contradicting Byakova et al. (2019a), who found that VRF in teeth with MP cannot be accurately identified with CBCT. Contrary to the findings of Neves et al. (2014), we found the lowest values for teeth restored with FGP. Although this restorative material produces less hardening beam artifacts, gutta-percha does.
It is known that, FGP is able to create a homogeneous distribution of stress due to its elastic modulus similar to dentin (Barjau-Escribano et al., 2006), reducing the catastrophic fracture of the root, i.e., producing a more tenuous fracture line and, therefore, more difficult to be visualized. In addition, factors such as post type and diameter can modify the stress distribution (Barjau-Escribano et al., 2006; Zicari, Coutinho, Scotti, Van Meerbeek, & Naert, 2013). According to Vasconcelos et al. (2016) the FGP post masks the fracture line and reduces the sensitivity, increasing the specificity, i.e., the number of undetected fractures will be greater than those detected (Vasconcelos et al., 2016).
Despite the standardization of the method, restoration with different materials certainly produced different characteristics in fractures. This is a limitation of the study, but it also represents a clinical situation. According to our results, despite the lower amount of beam-hardening artifacts in teeth restored with FGP, apparently the fracture pattern in these cases is more difficult to be detected, justifying the lower accuracy in this group.
One way to minimize some types of artifacts is the design features incorporated into modern CT scanners and software programs. Previous investigations have applied image filters at different resolutions, with quite divergent results (Wenzel, Haiter-Neto, Frydenberg, Kirkevang, 2009; Ferreira et al., 2015). While some authors (Ferreira et al., 2015) have not shown significant discrepancies, others (Wenzel et al., 2009) have found significant differences in the accuracy of detecting transverse root fractures when using digital filters. In the present study, i-Cat equipment was used, as it offers several acquisition configurations that meet the demands of different specialties (Tolentino et al., 2020). The scanners’ proprietary software was also used, in an attempt to represent the real and common conditions for evaluating these images. Hassan et al. (2010), who compared the capacity of five different devices to detect VRF, found that the i-Cat system was the most accurate. The authors justified these results based on the design of the detector, since this equipment has a flat-panel detector, which is superior to other detectors in terms of contrast and spatial resolution, which would be reducing image artifacts and noise (Hassan et al., 2010).
Although this system is considered a large volume device with several available FOVs [10], the smallest volume (8 x 8 cm) and voxel size available (0.125 mm) were used. The amount of x-ray noise decreases as FOV decreases, improving the spatial resolution and image quality (Hassan, Payam, Juyanda, van der Stelt, & Wesselink, 2012). Likewise, the voxel size also influences the image resolution (Ferreira et al., 2015), with smaller voxels providing better images (Tolentino et al., 2020). Variations in voxel size are reported to directly influence the accuracy of CBCT in detecting VRF, with higher accuracy when small voxels are used (Bragatto et al., 2016). CBCT spatial resolution plays an important role in the image quality due to the high level of accuracy required to exam small structures (Scarfe, Aboelmaaty, Scott, & Farman, 2012), such as VRF. For this reason, for endodontic examinations, where high resolution images are often required, small FOV and voxels are preferred (Hassan et al., 2012; Tolentino et al., 2020). We agree with Byakova et al. (2019a), who also used a larger FOV to detect VRF, that the use of this equipment can be considered a limitation of the study, since the use of a smaller size of voxel and FOV would be more reasonable for the detection of VRFs. Fractures that could not be detected were probably thinner than the maximum resolution of the i-Cat scanner (0.125 mm). The phenomenon of partial volume averaging that limits the capacity of CBCT to detect thinner objects may explain this, when the voxel resolution of the scan is higher than the spatial resolution of the object (Brady, Mannocci, Brown, Wilson, Patel, 2014; Tolentino et al., 2020).
The accuracy of fracture detection between in vitro and in vivo studies varies widely. In vitro studies do not incorporate patient factors such as movement during CBCT scanning and greater volume of hard and soft tissues (Byakova et al., 2019b). Moreover, the artificially produced VRF may be greater than in an in vivo scenario (Hassan et al., 2009). Byakova et al. (2019a) (the detection) investigated the accuracy of CBCT in the detection of VRF in post-core restored teeth and found that, in the in vivo assay, observers were unable to identify the presence or absence of the fracture in 90% of cases due to poor image quality. For the authors (Byakova et al., 2019a), the detectability of VRFs in vitro depended on their width. Our in vitro results suggest that CBCT is reliable in diagnosing VRF in non-restored teeth and in teeth restored with MP. However, this data should be extrapolated to a clinical scenario with caution, since many other factors could not be considered, such as soft tissue attenuation, presence of restored crowns, movement and position of the patient. Extrapolating the present findings to clinical practice, the accuracy, sensitivity and specificity of the CBCT exams would probably be lower in scans of living patients. It is important to emphasize that the diagnosis of VRF would be based on a combination of clinical and imaging findings (Byakova et al., 2019a; 2019b).
Conclusion
The highest values for sensitivity, specificity and accuracy of CBCT to detect VRF in premolars were found in the non-restored teeth. The presence of MP did not influence accuracy; however, the presence of FGP reduced the diagnostic capacity of CBCT.
References
Bacchi, A., Dos Santos, M. B., Pimentel, M. J., Caetano, C. R., Sinhoreti, M. A. C., & Consani, R. L. X. (2013). Influence of post-thickness and material on the fracture strength of teeth with reduced coronal structure. Journal of Conservative Dentistry, 16(2),139-143. DOI: https://doi.org/10.4103/0972-0707.108196
Barjau-Escribano. A., Sancho-Bru, J. L., Forner-Navarro, L., Rodríguez-Cervantes, P. J., Pérez-González, A., & Sánchez-Marín, F. T. (2006). Influence of prefabricated post material on restored teeth: fracture strength and stress distribution. Operative Dentistry, 31(1), 47-54. DOI: https://doi.org/10.2341/04-169
Brady, E., Mannocci, F., Brown, J., Wilson, R., & Patel, S. (2014). A comparison of cone beam computed tomography and periapical radiography for the detection of vertical root fractures in nonendodontically treated teeth. International Endodontic Journal, 47(8), 735-746. DOI: https://doi.org/10.1111/iej.12209
Bernardes, R. A., de Moraes, I. G., Húngaro Duarte, M. A., Azevedo, B. C., de Azevedo, J. R., & Bramante, C. M. (2009). Use of cone-beam volumetric tomography in the diagnosis of root fractures. Oral Surgery, Oral Medicine, Oral Pathology, and Oral Radiology, 108(2), 270-277. DOI: https://doi.org/10.1016/j.tripleo. 2009.01.017
Bragatto, F. P., Iwaki Filho, L., Kasuya, A. V., Chicarelli, M., Queiroz, A. F., Takeshita, W. M., & Iwaki, L. C. V. (2016). Accuracy in the diagnosis of vertical root fractures, external root resorptions, and root perforations using cone-beam computed tomography with different voxel sizes of acquisition. Journal of Conservative Dentistry, 19(6), 573-577. DOI: https://doi.org/10.4103/0972-0707.194029
Byakova, S. F., Novozhilova, N. E., Makeeva, I. M., Grachev, V. I., & Kasatkina, I. V. (2019a). The detection of vertical root fractures in post-core restored teeth with cone-beam CT: in vivo and ex vivo. Dento Maxillo Facial Radiology, 48(6), 1-7. DOI: https://doi.org/10.1259/dmfr.20180327
Byakova, S. F., Novozhilova, N. E., Makeeva, I. M., Grachev, V. I., & Kasatkina, I. V. (2019b). The accuracy of CBCT for the detection and diagnosis of vertical root fractures in vivo. International Endodontic Journal, 52(9), 1255-1263. DOI: https://doi.org/10.1111/iej.13114
Ferreira, L. M., Visconti, M. A., Nascimento, H. A., Dallemolle, R. R., Ambrosano, G. M., & Freitas, D. Q. (2015). Influence of CBCT enhancement filters on diagnosis of vertical root fractures: a simulation study in endodontically treated teeth with and without intracanal posts. Dento Maxillo Facial Radiology, 44(5), 1-6. DOI: https://doi.org/10.1259/dmfr.20140352
Hassan, B., Metska, M. E., Ozok, A. R., van der Stelt, P., & Wesselink, P. R. (2009). Detection of vertical root fractures in endodontically treated teeth by a cone beam computed tomography scan. Journal of Endodontics, 35(5), 719-722. DOI: https://doi.org/10.1016/j.joen.2009.01.022
Hassan, B., Metska, M. E., Ozok, A. R., van der Stelt, P., & Wesselink, P. R. (2010). Comparison of five cone beam computed tomography systems for the detection of vertical root fractures. Journal of Endodontics, 36(1), 126-129. DOI: https://doi.org/10.1016/j.joen.2009.09.013
Hassan, B. A., Payam, J., Juyanda, B., van der Stelt, P., & Wesselink, P. R. (2012). Influence of scan setting selections on root canal visibility with cone beam CT. Dento Maxillo Facial Radiology, 41(8), 645-648. DOI: https://doi.org/10.1259/dmfr/27670911
Jakobson, S. J. M., Westphalen, V. P. D., Silva Neto, U. X., Fariniuk, L. F., Schroeder, A. G. D., & Carneiro, E. (2014). The influence of metallic posts in the detection of vertical root fractures using different imaging examinations. Dento Maxillo Facial Radiology, 43(1), 1-7. DOI: https://doi.org/10.1259/dmfr.20130287
Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33(1), 159-74.
Lertchirakarn, V., Timyam, A., & Messer, H. (2002). Effects of root canal sealers on vertical root fracture resistance of endodontically treated teeth. Journal of Endodontics, 28(3), 217-219. DOI: https://doi.org/10.1097/00004770-200203000-00018
Menezes, R. F., Araújo, N. C., Santa Rosa, J. M., Carneiro, V. S. M., Santos Neto, A. P., Costa, V., ... Gerbi, M. E. M. M. (2016). Detection of vertical root fractures in endodontically treated teeth in the absence and in the presence of metal post by cone-beam computed tomography. BMC Oral Health, 48(1), 1-6. DOI: https://doi.org/10.1186/s12903-016-0207-y
Mitsui, F. H., Marchi, G. M., Pimenta, L, A. F., & Ferraresi, P. M. (2004). In vitro study of fracture resistance of bovine roots using different intraradicular post systems. Quintessence International, 35(8), 612-616.
Morfis, A. S. (1990). Vertical root fractures. Oral Surgery, Oral Medicine, Oral Pathology, and oral radiology, 69(5), 631-635. DOI: https://doi.org/10.1016/0030-4220(90)90248-q.
Neves, F. S., Freitas, D. Q., Campos, P. S. F., Ekestubbe, A., & Lofthag-Hansen, S. (2014). Evaluation of cone-beam computed tomography in the diagnosis of vertical root fractures: the influence of imaging modes and root canal materials. Journal of Endodontics, 40(10),1530-1536. DOI: https://doi.org/10.1016/j.joen. 2014.06.012
Scarfe, W., Li, Z., Aboelmaaty, W., Scott, S. A., & Farman, A. G. (2012). Maxillofacial cone beam computed tomography: essence, elements and steps to interpretation. Australian Dental Journal, 57(1):46-60. DOI: https://doi.org/10.1111/j.1834-7819.2011.01657.x
Talwar, S., Utneja, S., Nawal, R. R., Kaushik, A., Srivastava. D., & Oberoy, S. S. (2016). Role of cone-beam computed tomography in diagnosis of vertical root fractures: a systematic review and meta-analysis. Journal of Endodontics, 42(1), 12-24. DOI: https://doi.org/10.1016/j.joen.2015.09.012
Tamse, A. (2006). Vertical root fractures in endodontically treated teeth: diagnostic signs and clinical management. Endodontic Topics, 13(1), 84-94. DOI: https://doi.org/10.1111/j.1601-1546.2006.00200.x
Tolentino, E. S., Amoroso-Silva, P. A, Alcalde, M. P., Honório, H. M., Iwaki, L. C. V., Rubira-Bullen, I. R. F., & Húngaro-Duarte, M. A. (2020). Limitation of diagnostic value of cone-beam CT in detecting apical root isthmuses. Journal of Applied Oral Science, 28(1), e20190168. DOI: https://doi.org/10.1590/1678-7757-2019-0168
Trope, M., & Ray, H. L. (1992). Resistance to fracture of endodontically treated roots. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, 73(1), 99-102. DOI: https://doi.org/10.1016/0030-4220(92)90163-K
Vasconcelos, T. V., Santaella, G. M., Nascimento, H. A. R., Rovaris, K., Ambrosano, G. M. B., & Freitas, D. Q. (2016). Digital radiographs displayed on different devices: effect on the detection of vertical root fractures. International Endodontic Journal, 49(4), 386-392. DOI: https://doi.org/10.1111/iej.12466
Wang, X., Shu, X., Zhang, Y., Yang, B., Jian, Y., & Zhao, K. (2019). Evaluation of fiber posts vs metal posts for restoring severely damaged endodontically treated teeth: a systematic review and meta-analysis. Quintessence International, 50(1), 8-20. DOI: https://doi.org/10.3290/j.qi.a41499
Wenzel, A., Haiter-Neto, F., Frydenberg, M., & Kirkevang, L-L. (2009). Variable-resolution cone-beam computerized tomography with enhancement filtration compared with intraoral photostimulable phosphor radiography in detection of transverse root fractures in an in vitro model. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, 108(6), 939-945. DOI: https://doi.org/10.1016/j.tripleo.2009.07.041
Yoshino, K., Ito, K., Kuroda, M., & Sugihara, N. (2015). Prevalence of vertical root fracture as the reason for tooth extraction in dental clinics. Clinical Oral Investigations, 19(6), 1405-1409. DOI: https://doi.org/10.1007/ s00784-014-1357-4
Yusufoglu, S. I., Akman, M., Akbulut, M. B., & Eldeniz, A. U. (2019). Fracture resistance of roots enlarged with various rotary systems and obturated with different sealers. Journal Of Dental Research, Dental Clinics, Dental Prospects, 13(3), 215-220. DOI: https://doi.org/10.15171/joddd.2019.033
Zicari, F., Coutinho, E., Scotti, R., Van Meerbeek, B., & Naert, I. (2013). Mechanical properties and micro-morphology of fiber posts. Dental Materials, 29(4), e45-e52. DOI: https://doi.org/10.1016/j.dental.2012.11.001
Notas de autor
nandayamashita@gmail.com