Papers
Received: 28 May 2024
Accepted: 11 August 2024
Published: 18 October 2024
DOI: https://doi.org/10.14393/SN-v36-2024-73720
Abstract: Considering that COVID-19 has had a major impact on public health around the world, we aimed to elucidate the clinical and sociodemographic characteristics of non-hospitalized patients in Quirinópolis, southwest Goiás, from 2020 to 2022. We performed a cross-sectional study, using secondary data on all suspected COVID-19 visits in Basic Health Units, bivariate data analysis and logistic regression. 18,036 suspected cases were registered with 56.1% laboratory confirmed. COVID-19 was concentrated in the central regions of the city and was more associated with the vaccinated group, which may be a reflection of the vaccine's protective effect on the worsening of symptoms. The final logistic regression model showed a higher risk of COVID-19 among mixed race (1.30; CI1:20-1.42) and young people as a protective factor (0.88; CI:0.78-0.98). Gustatory (2.78; IC:2.19-3.53) and olfactory (2.83; IC: 2.18-3.66) disorders, headache (1.11; IC: 1.02-1.11), fever (1.77; CI: 1.62-1.92) and cough (1.48; CI: 1.36-1.61) were also associated with a positive diagnosis of COVID-19. Only respiratory disease was found to be a risk factor, probably due to underreporting of other factors. COVID-19 is ubiquitous among non-hospitalized patients, with easy transmission in clusters and with striking demographic and clinical characteristics: Brown population, taste and olfactory disorders, headache, fever, cough and respiratory disease as risk factors; young people apparently as a protective factor and vaccinated more related to COVID-19 may be a reflection of the profile of the sampled group (outpatients). The ubiquity of SARS-CoV-2 in the municipality may be related to public policies promoting ineffective medicines and population behavior that contribute to the spread of the virus. In contrast, vaccines have proven effective in containing the severe disease. In the future, approaches to hospitalized patients are necessary to better understand the impacts of COVID-19.
Keywords: Cross-sectional studies Public health, Respiratory tract infections, SARS-CoV-2.
INTRODUCTION
The World Health Organization (WHO) declared the end of the Public Health Emergency of International Concern for COVID-19 in May 2023. However, the disease is still considered a pandemic. This means that the virus continues to pose a serious threat to public health globally. It spreads quickly and efficiently, with new variants emerging regularly and prolonged periods of high number of cases (Focosi et al., 2023; Morawska; Cao, 2020). A significant decrease in vaccination coverage (Altman et al., 2023) has contributed to the emergence of new strains, leading to outbreaks with undefined clinical characteristics (Focosi et al., 2023; Tallei et al., 2023). Therefore, the clinical presentation of the disease varies and depends on a variety of factors.
It is important to note that most people infected with COVID-19 develop mild clinical symptoms. These symptoms are mostly related to fever, cough, sore throat, vomiting, diarrhea, loss of smell, and loss of taste (Yan et al., 2020; Zhu et al., 2020). Additionally, a significant number of patients experience prolonged symptoms, lasting anywhere from four months for those who were not hospitalized to nine months for those who were previously hospitalized (Hanson et al., 2022).
In relation to the severity of COVID-19, it is widely reported that several risk factors can exacerbate the disease (Atkins et al., 2020; Wang et al., 2020). It is important to note that Black populations and ethnic minorities are disproportionately affected due to social inequities (Hopman et al., 2020). Therefore, it is crucial to consider the geographical and epidemiological diversity of a region to establish ongoing clinical and laboratory surveillance of COVID-19 (Hallal et al., 2020).
Primary health care plays a vital role in addressing this pandemic, despite the inherent challenges in both dealing with the disease and the healthcare system itself (Patiño-Escarciña; Medina, 2022). Valuable information has been continually gathered to assist public authorities in decision-making, even within small municipalities, with the significant involvement of community health agents (Costa et al., 2021). Although Sistema Único de Saúde (SUS -Unified Health System) information systems may have issues leading to possible data inaccuracies (Farranha et al., 2022), this data remains an accessible and highly relevant tool for investigative approaches.
This study aims to definitively determine the clinical and sociodemographic factors associated with COVID-19 in non-hospitalized patients in southwest Goiás, Brazil from 2020 to 2022. Understanding these determinants and establishing a clinical-demographic profile is crucial for identifying high-risk groups for COVID-19 and establishing mechanisms to address this vulnerability.
MATERIALS AND METHODS
The study is a cross-sectional analysis based on data from the Quirinópolis City Hall database for the years 2020 - 2022. It includes clinical, demographic and laboratory information obtained from ESUS notifies. The study was approved by the Ethics and Research Council of Universidade Estadual de Goiás under protocol 4,737,576/2021.
The data excluded variables with inconsistent information, such as an unusually low number of occurrences, for analysis. The collected data was exported to an Excel® spreadsheet, and then analyzed using the Epi Info 7.2.2 computer program. Measures of frequency, significance and association were also calculated using this program.
Spatial analyses were conducted using spatial autocorrelation techniques, specifically the Global and Local Moran's I indexes (Anselin, 1995). The Global Moran's I offers a broad measurement of spatial association for the dataset, which can range from -1 to +1, indicating spatial independence (when the variable’s value is zero and the null hypothesis of no spatial dependence is confirmed), positive spatial dependence (when the value is positive), or negative spatial dependence (when the value is negative) (Câmara et al., 2004). However, the single value provided by this index’s autocorrelation function may obscure local (or regional) patterns that are encompassed with this single global value. So, we decided to use a method called Local Indicators of Spatial Association (LISA) or Local Moran's I, which was first suggested by Anselin (1995). The aim was to identify specific areas where the indicator shows strong spatial relationships and tends to form clusters. Using LISA helped us identify spatial patterns that we could then compare later on. We analyzed the Global and Local Moran's I indices along with a pseudo significance test, which is crucial for determining whether the data is random (stationary) or has spatial dependence. In this study, we rejected the null hypothesis of data randomness with a 99% confidence level in the mentioned test.
The data was analyzed using the Moran scatter plot. This diagram consists of four quadrants: Q1 (High-High) and Q2 (Low-Low) represent positive spatial autocorrelation between the values of a variable and the mean of the neighbors. This means that the values of a given indicator in a location are similar to the values of neighboring locations, forming clusters. Quadrants Q3 (High-Low) and Q4 (Low-High) indicate negative spatial autocorrelation, meaning that the values of a variable in a given location are not related to the values of the neighbors. These cases are commonly evaluated as situations of spatial stationarity, as they indicate locations whose value of a given indicator is opposite to that presented by the nearby locations. These atypical spatial situations are represented as outliers (Câmara et al., 2004).
The GeoDa 1.22 program was used to perform statistical operations and spatial representation of the data. The cartographic base, on a scale of 1:25,000,000, was taken from IBGE. Census sectors of the municipality of Quirinopólis-GO were considered to calculate the incidence rate of COVID-19 by sector, based on the IBGE Demographic Census of the year 2022. The data analysis involved the following steps:
-
Checking data consistency;
-
Frequency distribution of all researched variables, characterizing the studied population according to demographic aspects, comorbidities, symptoms and clinical signs;
-
Bivariate analysis: for comparisons of two proportions, the Chi-square test (α= 5%) was used. For continuous variables, the non-parametric Wilcoxon-Mann-Whitney test (abnormal variables) or Student's t-test (normal variables) (α= 5%) was used. The association between possible associated factors was qualified using the Odds Ratio (OR) with a 95% confidence interval.
The process included using logistic regression to create dummy variables for categories with more than two variables. Multivariate analysis was then conducted using the logistic regression in the following steps:
- 1. Initially, variables with p < 0.20 were selected for bivariate analysis;
- 2. Intermediate logistic models were constructed using two subgroups -demographic variables and clinical variables. Variables with p < 0.15 were retained in these models;
- 3. A final model was created, which only included variables with p < 0.05.
RESULTS
Our study looked into all suspected cases of COVID-19 in patients treated at the Basic Health Units of Quirinópolis, GO, over three consecutive years: 2020, 2021 and 2022. During this period, there were 18,036 suspected cases of COVID-19, out of which 56.1% (10,124 patients) were confirmed through laboratory tests. There was a progressive increase in cases over the three years: 17.6% in 2020, 34.4% in 2021 and 48.0% in 2022. Concurrently, the number of confirmed negative cases decreased annually: 49.8% in 2020, 36.4% in 2021, and 13.8% in 2022.
The findings from the global Moran's I Index indicate that the spread of COVID-19 in the municipality of Quirinopólis is spatially correlated. The positive spatial autocorrelation values for the years 2020, 2021 and 2022 were I = 0.266, I = 0.348, and I = 0.210, respectively. Additionally, the results of the Global Moran's Index led to the calculation of local autocorrelation indicators (LISA) were calculated (see Figure 1). Over the three years studied, a significant concentration of high COVID-19 cases was observed in the central region of the municipality, while low case clusters were found in the surrounding areas (see Figure 1).
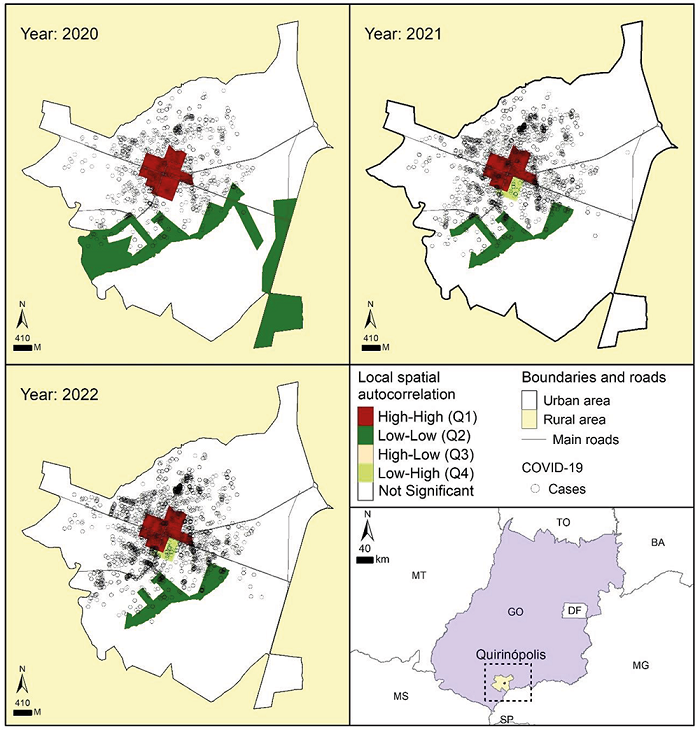
Figure 1
Spatial distribution of confirmed COVID-19 cases in the municipality of Qurinópolis, southeast of Goiás, from 2020 to 2022.
OR: odds ratio; IC95%: Confidence interval 95%. Source: The authors (2024).
We found that vaccinated individuals were five times more likely to test positive for COVID-19 compared to those who were not vaccinated (OR 5.27, CI 4.88-5.70).
In our analysis of sociodemographic data, we found no difference in the occurrence of COVID-19 based on gender (table 1). However, we observed that brown individuals were twice as likely to have the disease compared to white individuals, and black individuals were almost 1.5 times more likely.
Association between demographic variables and positivity FOR COVID-19, Quirinópolis, Goiás, 2020-2022.
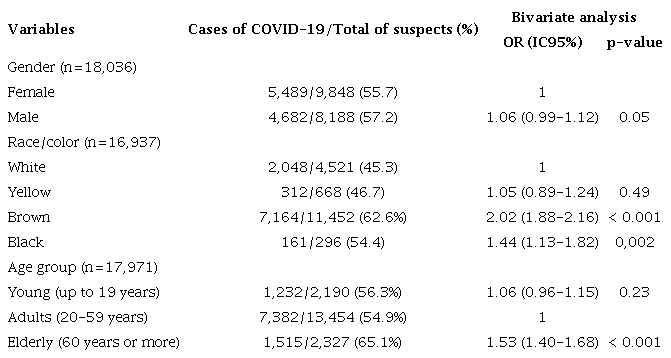
OR: odds ratio; IC95%: Confidence interval 95%. Source: The authors (2024).
The risk of contracting the disease was higher among elderly people, with 65.1% of cases occurring in this age group. They were 1.5 times more likely to have COVID-19 compared to adults.
Certain symptoms such as taste and smell disorders, headache, sore throat, fever and cough were significantly linked to a positive COVID-19 diagnosis (see table 2). Patients experiencing these symptoms were 1.76 to 2.52 times more likely to have had COVID-19.
Association between the presence of symptoms and positivity for COVID-19, Quirinópolis, Goiás, 2020-2022.
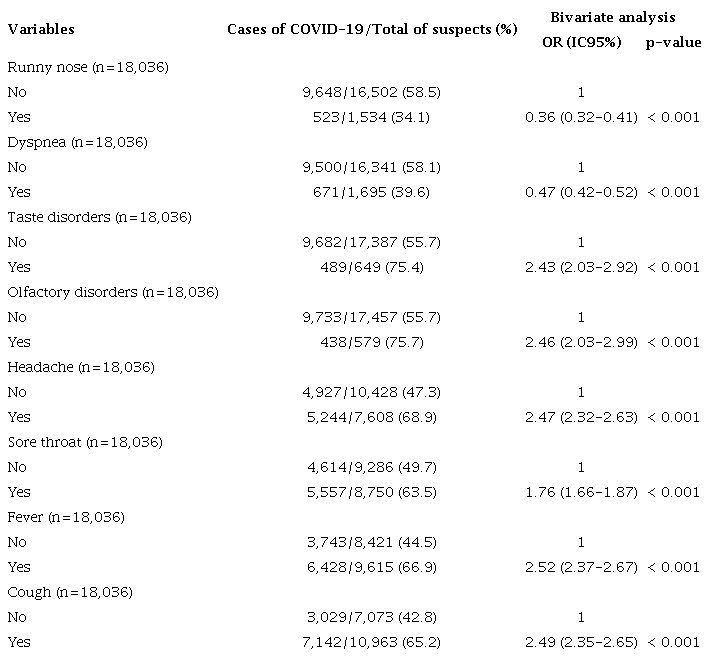
OR: odds ratio; IC95%; Confidence interval 95%; n: number of cases. Source: The authors (2024).
In our analysis, we found that previous respiratory diseases had a strong relationship with positive cases of COVID-19. Specifically, 98.2% of positive cases had this comorbidity (OR 76.13; 95% CI 61.04-94.98; p<0.001).
We also observed other comorbidities, but they were less common: 163 cases of heart disease, 112 cases of diabetes, 60 cases of kidney disease, 37 cases of immunosuppression, and 29 cases of obesity. Due to uncertainties about the accuracy and completeness of the data on these variables, we did not conduct inferential statistical analysis on them.
Furthermore, we used logistic regression to examine the relevance of clinical and sociodemographic variables for COVID-19, as shown in table 3.
Intermediate logistic regression models performed separately for each set of previously analyzed factors (variables that remained statistically significant), Quirinópolis, Goiás, 2020-2022.
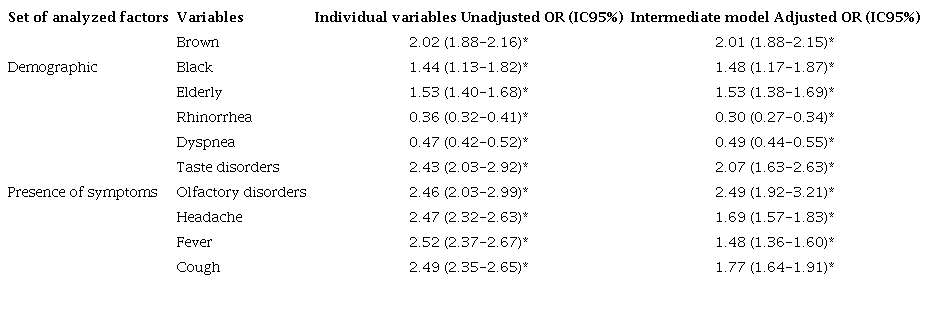
*p<0.001; OR: odds ratio; IC95%: Confidence interval 95%. Source: The authors (2024)
The demographic data showed that individuals of brown and black ethnicities, as well as elderly people, remained risk factors for COVID-19 (OR 2.01, CI 1.88-2.15; OR 1.48, CI 1.17-1.87; OR 1.53, CI 1.38-1.69, respectively). These results were consistent with the bivariate analysis. In terms of symptoms, taste and olfactory disorders, along with headache, cough and fever continued to be associated with COVID-19 in cases that did not require hospitalization (services in Basic Health Units). However, the statistical significance of most symptoms decreased in the intermediate logistic regression model. The final logistic regression model confirmed that individuals of brown ethnicity were 30% more likely to have COVID-19 within the scope of care at Basic Health Units (see table 4). Additionally, the age group corresponding to younger people was found to be a protective factor against COVID-19 (OR 0.88, CI 0.78-0.98).
Final logistic regression model performed with the variables that remained statistically significant in the intermediate regression models, Quirinópolis, Goiás, 2020-2022.
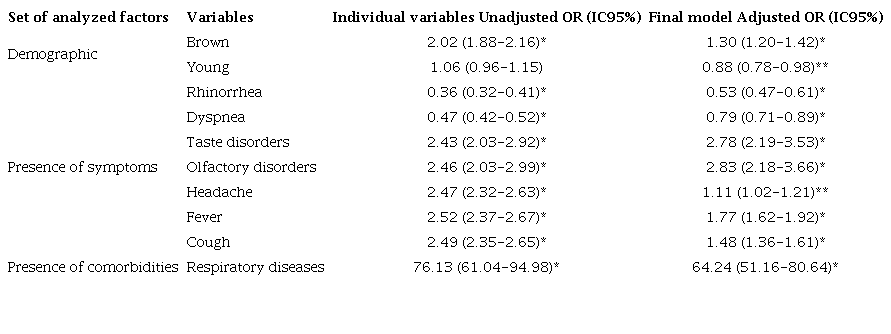
*p<0.001; **p<0.05; OR: odds ratio; IC95%: Confidence interval 95%. Source: The authors (2024).
The final regression model showed that symptoms such as taste and smell disturbances, headache, fever and cough were found to be associated with COVID-19 in cases of mild to moderate disease. The odds ratio (OR) ranged from 1.11 to 2.87 for headache and smell disturbances, respectively. However, runny nose and dyspnea were not associated with COVID-19.
Furthermore, previous respiratory diseases were identified as a significant risk factor for COVID-19, with the highest association found in this study (OR: 64.24). This variable was not included in an intermediate regression model, as data referring to other comorbidities were not analyzed due to concerns about their reliability, particularly underreporting.
DISCUSSION
Our study looked at all suspected and confirmed cases of COVID-19 reported by ESUS from 2020 to 2022 in a small Brazilian municipality. Our data provides a snapshot of how the pandemic has evolved from the beginning to the present day, including the period when vaccines became available. This gives us strong indicators about the clinical profile of COVID-19 overall. However, some of the information about certain factors may not be complete or reliable, and we believe that some issues, like diabetes, heart disease, and obesity, may have been underreported. Nonetheless, the results clearly show the clinical profile and some demographic aspects of the disease in mild and moderate cases of care in Basic Health Units.
According to our study, the vast majority of patients treated in Basic Health Units showed clinical symptoms, which was to be expected because COVID-19 primarily causes symptoms (Wang et al., 2020). Additionally, more than half of the recorded cases were confirmed through laboratory tests, indicating the widespread presence of the virus in the population and the high frequency of the disease in mild and moderate cases. Seroprevalence and laboratory surveillance studies have also revealed the high frequency of viral circulation in the general population, both regionally or locally (Baethgen et al., 2023; Costa et al., 2021). Furthermore, the high number of cases seen in Basic Health Units (Struyf et al., 2022) emphasizes the pervasive nature of COVID-19.
During the 2020-2022 period, there was a gradual increase in COVID-19 cases, while cases resulting from other unidentified pathogens but confirmed as negative for COVID-19 decreased. This change may be linked to the introduction of social distancing, which reduced the transmission of other viruses, subsequently altering the epidemiological landscape of these other agents later on (den Hartog et al., 2023; Stein; Zar, 2023). Despite social distancing measures, SARS-CoV-2 continued to spread and became the predominant virus, likely due to its high contagiousness (Morawska; Cao, 2020). Additionally, although vaccination platforms were available from 2021 onwards, there may not have been sufficient vaccination adherence to significantly reduce viral circulation (Gomes et al., 2022).
This factor is related to challenges to the COVID-19 vaccine, arising from anti-vaccine movements and as a result of harmful public policies, mainly affecting children and adolescents (Bivar et al., 2021; de Lima et al., 2024; Nehab et al., 2023). Our georeferencing data shows an increase in cases over the years. We believe that the inadequate implementation of social distancing rules, combined with a portion of the population not getting vaccinated, failure to use masks, and the highly infectious nature of the virus, may have contributed to the ongoing spread. Furthermore, the local public authorities recommended distributing a “covid kit” (containing chloroquine and ivermectin) for preventive treatment throughout the pandemic. In this context, a sense of well-being was found to be associated with an increased risk of disease (Cipolletta et al., 2022). This feeling arises from the false perception that early treatment was effective against the virus. In addition, the concentration of cases in the central regions of the municipality reflects the epidemiological nature of viral spread in a densely populated area with high virus exposure.
The data shows that vaccinated individuals were more likely to test positive for COVID-19 compared to those who were not vaccinated (OR 5.27, CI 4.88-5.70). This could be due to the fact that vaccines do not completely prevent SARS-CoV-2. However, it is possible that the vaccinated individuals experienced milder symptoms as our study focused on non-hospitalized patients. We cannot rule out the possibility that unvaccinated individuals may have experienced more severe disease, although this was not confirmed in our study. Vaccines are known to reduce the severity of symptoms and the likelihood of transmission within the community (Mohammed et al., 2022; Stokel-Walker, 2022). Additionally, it is important to note that long COVID appears to be more severe and persistent in unvaccinated people compared to vaccinated people (Hanson et al., 2021). Finally, we believe that the vaccine may have affected the results of laboratory tests, leading to false-positive results, especially for those who were tested only by serological tests (Mouliou; Konstantinos, 2021).
In order to assess the factors contributing to a higher risk of developing the disease, we employed logistic regression. Our findings indicate that black and brown individuals are more strongly linked to the risk of COVID-19 compared to white individuals, reflecting the greater social vulnerability of these groups and their increased likelihood of contracting the disease (Gariboti et al., 2022; Gaynor; Wilson, 2020; Kemei et al., 2023; Pan et al., 2020; Poteat et al., 2020; Rendon et al., 2021). However, no significant association was observed for black individuals with COVID-19 in the final regression analysis. This discrepancy might be related to the subjective self-identification of individuals as black or brown, considering that both groups are equally vulnerable across various social indicators.
In our analysis, we found that elderly people were 1.5 times more likely to have COVID-19 compared to adults. This was evident in both our initial analysis and in intermediate logistic regression, which focused only on demographic data. Various studies (Atkins et al., 2020; Daoust, 2020; Wang et al., 2020) also point to this age group as an important risk factor for COVID-19. However, our final regression model did not show a direct relationship between the elderly and the disease. The absence of a relationship may be due to the fact that older patients are more associated with more severe clinical cases of the disease. On the other hand, the final regression model indicated that young people seemed to have some level of protection against the disease, especially in cases of non-hospitalized patients. It is important to note, though, that long COVID can still have a significant impact on young people in terms of morbidity (Hanson et al., 2022).
In terms of clinical signs and symptoms, various studies have found that taste and olfactory disorders, along with headache, fever and cough are the most common symptoms of COVID-19 in non-hospitalized patients. These symptoms have been widely observed among non-severe patients (Struyf et al., 2022; Wang et al., 2020). Taste and olfactory disorders have been particularly strongly associated with the disease, as reported by various sources (Costa et al., 2021; Yan et al., 2020).
Respiratory diseases are the only comorbidity strongly linked to COVID-19 in non-hospitalized patients and are considered an important predictor of vulnerability to the disease (Atkins et al., 2020; Wang et al., 2020). However, while other comorbidities are also considered significant risk factors, this study was unable to gather complete and consistent data on the majority of comorbidities such as diabetes, hypertension, and obesity from the SUS system. These non-communicable diseases are known to affect populations worldwide, and it is believed that many comorbidities were underreported: 163 cases of heart disease, 112 of diabetes, 60 kidney diseases, 37 immunosuppression, and 29 cases of obesity.
This perception of underreporting stems from the analysis of a sample of over 18,000 records. Additionally, concerns about the accuracy of COVID-19 diagnosis and the reliability of the data collection system (Farranha et al., 2022; Struyf et al., 2022) could indicate issues with recording and capturing COVID-19 data.
Despite these concerns, our study provided a robust understanding of the clinical and demographic characteristics of non-hospitalized COVID-19 patients. This information is crucial for informing public health decision-making. The reliability of our findings is supported by the large sample size (over 18,000 cases) and the rigorous statistical analyses used. As a result, we were able to establish a clinical and epidemiological profile of COVID-19 in primary care settings, which can guide more accurate and timely medical interventions. Additionally, it can inform public authorities about preventive measures and vaccination campaigns as part of ongoing virus surveillance.
It is worth noting that COVID-19 remains a pandemic, with the emergence of new variants (Focosi et al., 2023) whose clinical and epidemiological developments are still unclear.
CONCLUSIONS
The evidence shows that SARS-CoV-2 is a highly prevalent pathogen that easily spreads within human clusters, despite the existence of safe vaccination platforms. This could suggest that there is low adherence to vaccination among the population (Altman et al., 2023; Bivar et al., 2021; Gomes et al., 2022; Nehab et al., 2023). People with a darker skin tone seemed to have some protection against mild to moderate disease. Conversely, young people seem to have some protection against mild to moderate disease. The common clinical characteristics were cough, fever, headache, as well as olfactory and taste disorders. It was observed that COVID-19 cases among outpatients were more prevalent in the vaccinated group compared to the unvaccinated group, probably due to the specific selection of patients - those not requiring hospitalization, as well as the protective effect of vaccines against severe symptoms. For future investigations, it is important to assess the clinical and sociodemographic profiles of critically ill patients who necessitate hospitalization. Despite the data capture failures of the public health system in a developing country, it is important to emphasize the significance of this investigative approach in the context of socially excluded populations and the impact of the pandemic on these social groups. The care provided by the SUS, combined with low-cost scientific investigations and in regions with limited financial support, can help mitigate the impacts of COVID-19 on vulnerable populations and in economically disadvantaged regions within a country with significant social inequality.
ACKNOWLEDGEMENTS
The authors of this study would like to thank the Municipality of Quirinópolis, Department of Health, for the support, assistance and various directions in accessing and obtaining DATASUS data from patients treated in the municipality and region.
REFERENCES
ALTMAN, J. D.; MINER, D. S.; LEE, A. A.; ASAY, A. E.; NIELSON, B. U.; ROSE, A. M.; HINTON, K.; POOLE, B. D. Factors affecting vaccine attitudes influenced by the COVID-19 pandemic. Vaccines, v. 11, n. 3, p. 516, 2023. Doi: 10.3390/vaccines11030516
ANSELIN, L. Local indicators of spatial association − LISA. Geographical analysis, v. 27, n. 2, p. 93-115, 1995. Doi: 10.1111/j.1538-4632.1995.tb00338.x
ATKINS, J. L.; MASOLI, J. A. H.; DELGADO, J.; PILLING, L. C.; KUO, C. L.; KUCHEL, G. A.; MELZER, D. Preexisting Comorbidities Predicting COVID-19 and Mortality in the UK Biobank Community Cohort. The Journals of Gerontology: Series A, v. 75, n. 11, p. 2224-2230, 2020. Doi: 10.1093/gerona/glaa183
BAETHGEN, L. F.; et al. SARS-CoV-2 laboratory surveillance during the first year of the COVID-19 pandemic in southern Brazil. Revista da Sociedade Brasileira de Medicina Tropical, v. 56, p. e0146-2022, 2023. Doi: 10.1590/0037-8682-0146-2022
BIVAR, G. C. C.; DE AGUIAR, M. E. S. C.; SANTOS, R. V. C.; CARDOSO, P. R. G. COVID-19, the anti-vaccine movement and immunization challenges in Brazil: a review. Scientia Medica, v. 31, n. 1, p. 33, 2021. 10.15448/1980-6108.2021.1.39425
CÂMARA, G.; CARVALHO, M. S.; CRUZ, O. G.; CORREA, V. Análise espacial de áreas. In: DRUCK, S; CARVALHO, MS; CÂMARA, G; MONTEIRO, AVM, et al (eds). Análise espacial de dados geográficos. Brasília: EMBRAPA; 2004. p. 155- 205.
CIPOLLETTA, S.; ANDREGHETTI, G. R.; MIONI, G. Risk perception towards COVID-19: A systematic review and qualitative synthesis. International Journal of Environmental Research and Public Health, v. 19, n. 8, p. 4649, 2022. Doi: 10.3390/ijerph19084649
COSTA, L. F.; SOUZA, R. B.; DE OLIVEIRA, A. M. M.; EZEQUIEL, J. Seroprevalence of SARS-CoV-2 in southwest Goiás, Brazil, 2020: a population-based cross-sectional serological study. One Health & Implementation Research, v. 1, p. 31-42, 2021. Doi: 10.20517/ohir.2021.05
DAOUST, J. F. Elderly people and responses to COVID-19 in 27 Countries. PloS one, v. 15, n. 7, p. e0235590, 2020. Doi: 10.1371/journal.pone.0235590
FARRANHA, A. C.; RODRIGUES, L. C.; BATAGLIA, M. B. O direito à informação em saúde diante da base de dados do DATASUS: desafios jurídicos e políticos em tempos de COVID-19. Cadernos Ibero-Americanos de Direito Sanitário, Brasília, v. 11, n. 1, p. 32-47, 2022. Doi: 10.17566/ciads.v11i1.873
FOCOSI, D; QUIROGA, R.; MCCONNELL, S.; JOHNSON, M. C.; CASADEVALL, A. Convergent evolution in SARS-CoV-2 spike creates a variant soup from which new COVID-19 waves emerge. International journal of molecular sciences, v. 24, n. 3, p. 2264, 2023. Doi: 10.3390/ijms24032264
GARIBOTI, D. F.; SILVA JÚNIOR, F. M. R. Ethnic-racial disparity and mortality due to Covid-19: Case study of two medium-sized cities. Sociedade & Natureza, v. 34, p. e64009, 2022. Doi: 10.14393/SN-v34-2022-64009
GAYNOR, T. S.; WILSON, M. E. Social vulnerability and equity: The disproportionate impact of COVID‐19. Public administration review, v. 80, n. 5, p. 832-838, 2020. Doi: 10.1111/puar.13264
GOMES, I. A.; SOARES, P.; ROCHA, J. V.; GAMA, A.; LAIRES, P. A.; MONIZ, M.; PEDRO, A. R.; DIAS, S.; GOES, A. R.; LEITE, A.; NUNES, C. Factors associated with COVID-19 vaccine hesitancy after implementation of a mass vaccination campaign. Vaccines, v. 10, n. 2, p. 281, 2022. Doi: 10.3390/vaccines10020281
HALLAL, P. C., et al. SARS-CoV-2 antibody prevalence in Brazil: results from two successive nationwide serological household surveys. The Lancet Global Health, v. 8, n. 11, p. e1390-e1398, 2020. Doi: 10.1016/S2214-109X(20)30387-9
HANSON, S. W., et al. Global Burden of Disease Long COVID Collaborators. Estimated global proportions of individuals with persistent fatigue, cognitive, and respiratory symptom clusters following symptomatic COVID-19 in 2020 and 2021. Jama, v. 328, n. 16, p. 1604-1615, 2022. Doi: 10.1001/jama.2022.18931
DEN HARTO, G. G.; VAN KASTEREN, P. B.; SCHEPP, R. M.; TEIRLINCK, A. C.; VAN DER KLIS, F. R.; VAN BINNENDIJK, R. S. Decline of RSV-specific antibodies during the COVID-19 pandemic. The Lancet Infectious Diseases, v. 23, n. 1, p. 23-25, 2023. Doi: 10.1016/S1473-3099(22)00763-0
HOPMAN, J.; ALLEGRANZI, B.; MEHTAR, S. Managing COVID-19 in Low- and Middle-Income Countries. Jama , v. 323, n. 16, p. 1549-1550, 2020. Doi: 10.1001/jama.2020.4169
KEMEI, J.; TULLI, M.; OLANLESI-ALIU, A.; TUNDE-BYASS, M.; SALAMI, B. Impact of the COVID-19 Pandemic on Black Communities in Canada. International Journal of Environmental Research and Public Health , v. 20, n. 2, p. 1580, 2023. Doi: 10.3390/ijerph20021580
DE LIMA, E. E. C.; DA COSTA, L. C. C.; SOUZA, R. F.; ROCHA, C. O. D. E.; ICHIHARA, M. Y. T. Presidential election results in 2018-2022 and its association with excess mortality during the 2020-2021 COVID-19 pandemic in Brazilian municipalities. Cadernos de Saúde Pública, v. 40, n. 5, 2024. Doi: 10.1590/0102-311XEN194723
MOHAMMED, I., et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: a systematic review. Human vaccines & immunotherapeutics, v. 18, n. 1, p. 2027160, 2022. Doi: 10.1080/21645515.2022.2027160
MORAWSKA, L.; CAO, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environment international, v. 139, p. 105730, 2020. Doi: 10.1016/j.envint.2020.105730
MOULIOU, D. S.; KONSTANTINOS, I. G. False-positive and false-negative COVID-19 cases: respiratory prevention and management strategies, vaccination, and further perspectives. Expert review of respiratory medicine, v. 15, n. 8, p. 993-1002, 2021. Doi: 10.1080/17476348.2021.1917389
NEHAB, M. F., et al. Willingness of Brazilian caregivers in having their children and adolescents vaccinated against Covid-19. Vaccine, v. 41, n. 3, p. 735-743, 2023. Doi: 10.1016/j.vaccine.2022.11.077
PAN, D., et al. The impact of ethnicity on clinical outcomes in COVID-19: A systematic review. EClinical Medicine, v. 23, 2020. Doi: 10.1016/j.eclinm.2020.100404
PATIÑO-ESCARCINA, J. E.; MEDINA, M. G. Vigilância em Saúde no âmbito da atenção primária para enfrentamento da pandemia da Covid-19: revisão documental. Saúde em Debate, v. 46, p. 119-130, 2022. Doi: 10.1590/0103-11042022E108
POTEAT, T.; MILLETT, G. A.; NELSON, L. E.; BEYRER, C. Understanding COVID-19 risks and vulnerabilities among Black communities in America: the lethal force of syndemics. Annals of epidemiology, v. 47, p. 1-3, 2020. Doi: 10.1016/j.annepidem.2020.05.004
RENDON, A. F. V., et al. Marginalization, vulnerability and economic dynamics in COVID-19. International Journal of Cardiovascular Sciences, v. 34, p. 319-323, 2021. Doi: 10.36660/ijcs.20210029
STEIN, R.; ZAR, H. J. RSV through the COVID‐19 pandemic: Burden, shifting epidemiology, and implications for the future. Pediatric Pulmonology, v. 58, n. 6, p. 1631-1639, 2023. Doi: 10.1002/ppul.26370
STOKEL-WALKER, C. What do we know about covid vaccines and preventing transmission? BMJ, v. 376, 2022. Doi: 10.1136/bmj.o298
STRUYF, T., et al. Cochrane COVID-19 Diagnostic Test Accuracy Group. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID‐19. Cochrane database of systematic reviews, n. 5, 2022. Doi: 10.1002/14651858.CD013665.pub3
TALLEI, T. E., et al. Update on the omicron sub‐variants BA. 4 and BA. 5. Reviews in medical virology, v. 33, n. 1, p. e2391, 2023. Doi: 10.1002/rmv.2391
WANG, B.; LI, R.; LU, Z.; HUANG, Y. Does comorbidity increase the risk of patients with COVID-19: evidence from meta-analysis. Aging (Albany NY), v. 12, n. 7, p. 6049, 2020. Doi: 10.18632/aging.103000
YAN, C. H.; FARAJI, F.; PRAJAPATI, D. P.; OSTRANDER, B. T.; DECONDE, A. S. Self-reported olfactory loss associates with outpatient clinical course in COVID-19. In: International forum of allergy & rhinology, v. 10, n. 7, p. 821-831. 2020. Doi: 10.1002/alr.22592
ZHU, J.; JI, P.; PANG, J.; ZHONG, Z.; LI, H.; HE, C.; ZHANG, J.; ZHAO, C. Clinical characteristics of 3062 COVID‐19 patients: a meta‐analysis. Journal of medical virology, v. 92, n. 10, p. 1902-1914, 2020. Doi: 10.1002/jmv.25884
