Original Article
Relevance of indicators of clinical supervision strategies in nursing
Relevance of indicators of clinical supervision strategies in nursing
Revista da Rede de Enfermagem do Nordeste, vol. 18, no. 1, pp. 19-25, 2017
Universidade Federal do Ceará
Received: 11 October 2016
Accepted: 21 November 2016
Objective: to identifying the indicators of strategies of clinical supervision in nursing that nurses consider more relevant.
Methods: it is a descriptive and exploratory research with a quantitative approach. A questionnaire was constructed to collect data, applied to a sample of 316 nurses who performed functions in a hospital context and primary health care.
Results: the relevance attributed by the nurses to the indicators of clinical supervision strategies, especially the reflexive processes, as well as to methods directed to action and demonstration, are highlighted.
Conclusion: the indicators identified in the study constitute an important step in the structuring and evaluation of supervision processes, contributing to the improvement of quality and safety of care.
Keywords: Nursing, Supervisory+ Quality Indicators, Health Care+ Quality Assurance, Health Care.
Introduction
Considered the priority of any health organization(1), the quality of care is one of the essential aspects of caring excellence and, at the same time, a goal that requires investment and motivation by the professionals and the institution. Research carried out in the clinical nursing supervision area has shown a decisive influence on the quality and safety of care provided to patients(2). In Portugal, an effort is made to explore the benefits of this process(3-5). The Order of Nurses considers clinical supervision as a “... the formal process of monitoring professional practice, which aims to promote autonomous decision making, valuing the protection of the person and the safety of care, through reflection processes and analysis of clinical practice”(6:5).
Clinical supervision may lead to a reduction in stress levels, to the prevention of Burnout Syndrome, and to an increase in satisfaction and professional efficiency(7), being considered as a key resource for achieving health gains. Its implementation in the clinical contexts can respond to some requirements evidenced in the literature, such as the implementation of programs of continuous improvement of the practice; The personal and professional development of nurses; The encouragement of innovation and creativity, as well as The needs and expectations of professionals and patients(8). It is necessary for the actors (supervisor and supervisor) to establish a learning environment conducive to well-being, self-esteem and motivation for the process of clinical supervision to be effective. For this, it is necessary to use strategies focused on the development of knowledge and skills, and on the appropriate support to the supervisee. In this sense, the design of indicators of clinical supervision strategies in nursing becomes a fundamental step.
The use of indicators in the Nursing subject has proved to be a preponderant factor to evaluate professional performance, since it allows planning, evaluating and reorganizing the care process, translating into the promotion of a quality of care policy(9). Currently, the indicators are used as guidelines for the monitoring, evaluation, and promotion of quality of care, revealing a health situation. Not being the only components in this problem, they represent an essential tool for the operationalization of any health strategy or program(10). Clinical supervision in nursing be a method that enhances the quality of nurses’ professional practice, so strategies should be used supported by a set of indicators that operationalize their implementation. In this way, each indicator will result from the deconstruction of the strategy in the most elementary concepts and characteristics, enabling to acquire information about the character and objectives of the professional development process.
Taking into account the already demonstrated benefits of the use of indicators in the health area and considering the scarcity of existing literature on indicators of clinical supervision strategies in nursing, it was admitted that this would be a relevant problem, and this research aimed to identify the indicators of clinical nursing supervision strategies most relevant to nurses.
Methods
Considering the specific nature of the problem under analysis, it was decided to carry out a quantitative research, of a descriptive and exploratory nature, since it was intended to obtain more information about the phenomenon under study, given that this is still little studied, particularly in Portugal.
The target population of this research was the nurses who worked in Portugal. The non-probabilistic sample consisted of 316 nurses from the hospital context and primary health care in the Porto district, being defined as inclusion criteria to be nurses and to perform nursing duties in Portugal.
The data collection was performed through a questionnaire built for this purpose, since no instrument was found that could achieve the proposed objective, and its elaboration was based on the following steps: determining what information to collect; Constituting a bank of questions; Formulating the issues; Sorting out the issues; Directing introduction and guidelines; Submitting the sketch of the questionnaire to the review and then submitting it to a pre-test(11).
There were 14 strategies for clinical supervision in nursing selected (observation, demonstration, case analysis with the supervisee, feedback, support, critical-reflexive analysis of practices, reflexive report, group supervision sessions, nursing care documentation analysis, continuous training, Individual supervision sessions, self-supervision, group case analysis and distance supervision) identified in the literature and considered as relevant(4), emerging the indicators for the basis for its construction from this exercise of analysis and exploration of each strategy and its defining characteristics. The questionnaire was analyzed by a group of 14 experts with experience and training in the clinical supervision area and Education Sciences to investigate the content validity. The experience and creativity of this group of experts were essential to establishing collective judgment about it. The questionnaire was reconstructed based on the suggestions given by the experts regarding the organization, clarity, and relevance of some indicators. Subsequently, the questionnaire was pre-tested to nine nurses from the hospital context and primary health care, with and without training in clinical nursing supervision to identify gaps and make corrections that would improve their understanding.
The final version of the questionnaire was obtained after these steps, and it was called as “Questionnaire for Assessment of the Relevance of Indicators of Strategies for Clinical Supervision in Nursing.” This questionnaire consists of two parts: the first part is composed of 20 questions and aims to obtain characterization data of the sample. The second part contemplates 63 closed questions, which refer to the indicators of the 14 strategies of clinical supervision. Their completion is done using multiple choice answers, using the following semantic differentials: 1 - nothing relevant; 2 - not relevant; 3 - relevant; 4 - very relevant and 5 - totally relevant. The instrument was applied to nurses between June and September 2012.
For the descriptive and inferential analysis of the data, the version 20.0 of the Statistical Package for Social Sciences was used. Since it was an investigation involving the assessment of consensus, it was essential to define its levels. While there is no pre-determined rule to do so, it is found that the level considered in other investigations ranges from 50 to 80.0%(10). In this case, it was considered that there was consensus when each of the questions was simultaneously present, the following conditions: Median ≥ to four and cumulative frequency in scores four and five ≥75.0%.
The study complied with the formal requirements contained in the national and international regulatory standards for research involving human beings.
Results
The nurses who participated in the research were aged between 23 and 57 years old (mean=33.33; Standard deviation=6.72), with 78.0% female. The professional practice time ranged from one to 37 years (mean=10.44; standard deviation=6.59), 69.0% worked in a hospital context and 31.0% in primary health care. Most nurses (74.0%, n=234) reported not having training in clinical supervision in nursing. From 82 nurses with training in clinical nursing supervision, 54.0% (n=43) reported that they had a course on this subject during the academic year, 31.0% (n=25) attended a short course and only 15.0% (n=12) are qualified with a postgraduate course.
Regarding relevance data, a new variable of the quantitative type was computed through the calculation of the mean, ignoring the nulls, of the group of indicators that could be associated with each strategy from a theoretical point of view., The average of the group of indicators obtained in each strategy to establish a ranking of relevance of indicators of clinical supervision strategies. Regarding the indicators, these were analyzed individually, considering the consensus criteria previously described.
Through the analysis of Table 1, the highest means obtained in the groups of indicators referring to each strategy of clinical supervision in nursing are about the “observation” strategy (Mean=4.358), followed by the “demonstration” (Mean=4.344) and “case analysis with the supervisee” (Mean=4.247). The indicators of clinical supervision strategies in nursing with less relevance are those of “distance supervision” (Mean=3.503), “group case analysis” (Mean=4,138) and “self-supervision” (Mean=4.135).
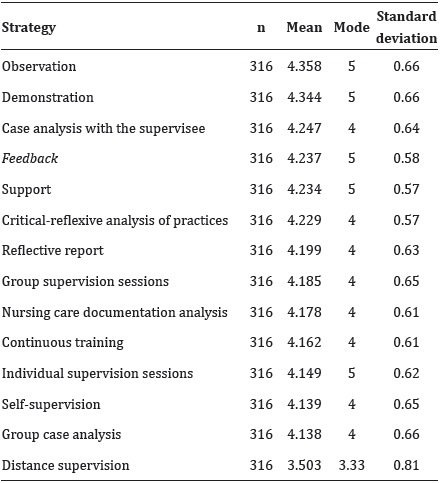
Figure 1 shows the indicators that obtained a cumulative frequency in scores 4 and 5 higher than 86.0%. It was decided to present only the indicators with these levels of consensus because they are the most relevant.
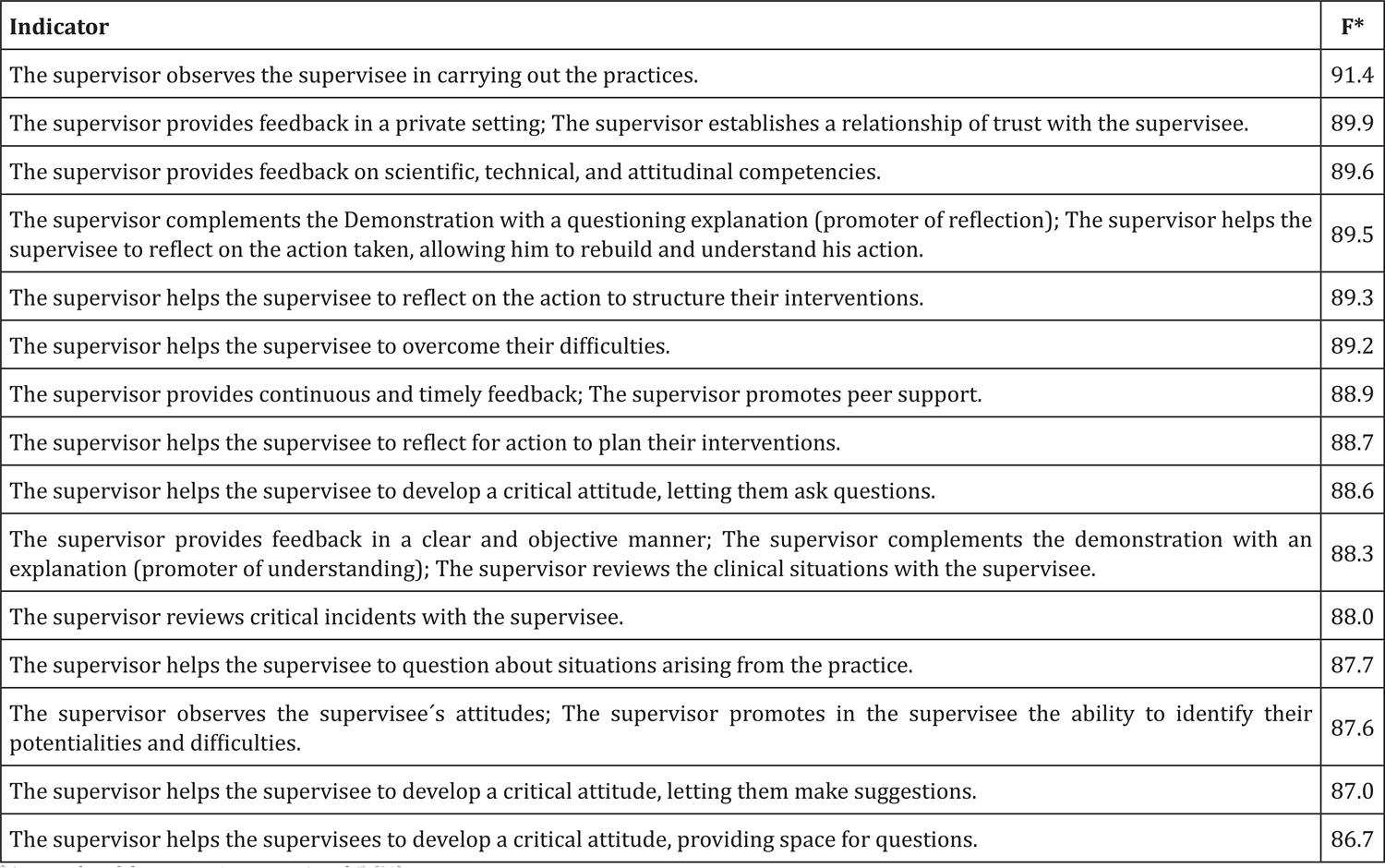
Figure 1
Indicators of clinical supervision strategies in nursing with accumulated frequencies scores 4 and 5 higher than 86.0%
* Accumulated frequency in scores 4 and 5 (%)
The indicators that did not obtain consensus among the nurses are: the supervisor is available via skype® to contact the supervisee at the agreed time (32.6%); The supervisor is available to communicate via telephone with the supervisee (52.6%); The supervisor provides positive feedback (57.3%); The supervisor indicates research sources (67.4%); The supervisor negotiates supervisory strategies (68.3%); The supervisor responds to the supervisee´s e-mails in the agreed time (71.2%); The supervisor takes into account the previous experiences of the supervisee (74.4%).
Discussion
Analyzing the relevance attributed by nurses to the set of indicators of each strategy of clinical supervision in nursing, it is highlighted the concern of the supervisors, to collect data by the “observation” of the supervisees, to use the “demonstration” as a vehicle to fill potential gaps in their performance, and encourage behavior change through “case analysis with the supervisee”. The data found corroborate other studies, which reveal the importance of case analysis in the process of thought development(5); the demonstration of a given intervention, accompanied by reflection(12) and observation as the starting point for sustained and anchored growth(13).
By analyzing the indicators that have obtained a greater consensus, it is observed that the processes of clinical supervision in nursing for nurses should be based on observation methods, demonstration of practices and reflection on the care provided, and the supervisor is responsible for supporting difficulties and providing adequate feedback to the supervisee, through a trust-based and peer-supported supervisory relationship. Besides the benefits of observing practices and demonstration, the use of feedback should be continuous and on the competencies of the supervisee(14) to foster their development and effective follow-up. In existing scientific evidence, support is highlighted as one of the key points of clinical nursing supervision, enabling the creation of a trustful atmosphere conducive to learning and promoting a peer support relationship(15), essential to the adequacy of behaviors, especially when unpredictable in the clinical context.
It can be concluded that there is a high level of consensus in the indicators directed to reflexive processes, which is corroborated by some researchers who consider reflexive practice as an integral part of clinical supervision(3-4), making it essential to have specific training in this area(16) that includes in its plan strategies for developing the critical-reflexive capacity of the supervisee(17). Nurses increasingly need to think critically and reflect on their actions to promoting and delivering quality health care so that they can be properly prepared and able to adapt to the constant changes in health contexts. Based on this assumption, it is perceived that the supervisor plays an important role in the training of nurses, and their contribution is based on a reflexive dialogue with them, making them able to think critically to provide quality and significant care to patients. In the clinical nursing supervision area, it is essential that the supervisor develops activities that enhance an improvement in the critical-reflexive abilities of the supervisee(17).
There is also a clear preference of nurses for the indicators of clinical supervision strategies in face-to-face nursing, to the detriment of those at a distance (telephone, email or Skype®), which can be understandable due to the limited evidence(3) and its influence on the supervisory relationship and the improvement of the care provided to the patient(18). A study developed in this area concluded that the implementation of strategies that enhance the visual contact, especially the supervision by video conference, involves the trainees in the learning(19). The advantages of the use of new technologies in training are recognized at different levels and contexts(3,18-19). Although there is still little research in this area, it is perceived that the use of these strategies applied to clinical supervision in nursing can approach the agents involved in this process, promoting support, interaction and communication. In this context, research shows that nurses, especially those who work in primary health care, want distance supervision strategies to be implemented in their contexts, even considering that they should be carried out more frequently than they do it currently(3). Given the increasing dissemination and use of this type of methodologies, there seems to be a motivation of professionals towards distance supervision strategies, which can be an important and necessary starting point for their implementation in health contexts.
Although some of the indicators do not reach consensus, they are considered relevant not only by some authors, who point out the benefits of using positive feedback(14), distance supervision(3,18-19) and negotiating strategies(13), as well as the group of experts who validated the content of the questionnaire. We believe that this result will be related to the fact that the sample of the study consists mainly of nurses with no training in clinical nursing supervision, who are probably not so much aware of the importance of these indicators during supervised practices.
Conclusion
It was concluded that all the indicators were considered relevant, with the idea that clinical nursing supervision should be based on observation, demonstration, feedback and support methodologies, favoring reflection for the growth and development of knowledge and skills of the supervisee. The use of these indicators enables the supervisor to objectively plan, organize and evaluate their performance and the objectives of the supervisee, while supporting their performance, contributing to the success of supervisory practices.
Considering the high levels of consensus that emerged from this study, it is assumed that these can be used not only in the development of instruments or guidelines for clinical supervision in nursing but also in the definition of models of supervision that promote quality and safety of care.
References
1. Moore A, Waters A. All eyes on the patient. Nurs Stand. 2012; 26(27):20-2.
2. Hyrkäs K, Lethi K. Continuous quality improvement through team supervision supported by continuous self-monitoring of work and systematic patient feedback. J Nurs Manag. 2013; (11):177- 88.
3. Rocha IARS, Santos MR, Pires RMF. Supervisão à distância em enfermagem: uma realidade desejada pelos enfermeiros. Rev Referenc. 2016; IV(10):95-102.
4. Pires R, Santos MR, Pereira F, Rocha I. Most relevant clinical supervision strategies in nursing practice. In: 2nd International Conference on Health and Health Psychology Most Porto: The European; 2016; p. 351-61.
5. Teixeira SMM, Carvalho ALRF, Cruz SSSMS. Self-care assessement as na indicator for clinical supervision in nursing. Rev Rene. 2016; 17(3):356-62.
6. Ordem dos Enfermeiros (PT). Caderno temático: modelo de desenvolvimento profissional – fundamentos, processos e instrumentos para a operacionalização do sistema de certificação de competências. Lisboa: Ordem dos Enfermeiros; 2010.
7. Wallbank S. Maintaining professional resilience through group restorative supervision. Comm Pract. 2013; 86(8):26-8.
8. Freitas JS, Silva AEBC, Minamisava R, Bezerra ALQ, Sousa MRG. Quality of nursing care and satisfaction of patients attended at a teaching hospital. Rev Latino-Am Enfermagem. 2014; 22(3):454-60.
9. Gabriel CS, Melo MRAC, Rocha FLR, Bernardes A, Miguelaci T, Silva MLP. Use of performance indicators in the nursing service of a public hospital. Rev Latino-Am Enfermagem. 2011; 19(5):1247-54.
10. Pereira F. Informação e qualidade do exercício profissional dos enfermeiros. Porto: Formasau; 2009.
11. Fortin F. Fundamentos e etapas do processo de investigação. Loures: Lusodidacta; 2009.
12. Rua M. De aluno a enfermeiro: desenvolvimento de competências em contexto de ensino clínico. Loures: Lusociência - Edições Técnicas e Científicas, Ltda; 2011.
13. Alarcão I, Tavares J. Supervisão da prática pedagógica: uma perspectiva de desenvolvimento e aprendizagem. Coimbra: Almedina; 2010.
14. Clynes M, Raftery S. Feedback: an essential element of student learning in clinical practice. Nurse Educ Pract. 2008; 8:405-11.
15. Vlachou E, Plagisou L. Clinical supervision as a tool for nurses. Nosileftiki. 2011; 50(3):279-87.
16. Fowler J. Supporting self and others: from staff nurse to nurse consultant. Part 6: giving and receiving feedback. Brit J Nurs [Internet]. 2011 [cited 2016 Sept 13]; 20(14):885. Available from:http://www.magonlinelibrary.com/doi/abs/10.12968/bjon.2011.20.14.885
17. Winstanley J, White E. The MCSS-26: Revision of the Manchester Clinical Supervision Scale using the rasch measurement model. J Nurs Manag. 2011; 19(3):160-78.
18. Wright J, Griffiths F. Reflective practice at a distance: using technology in counseling supervision. Refl Pract. 2010; 11(5):693-703.
19. Bolle SR, Johnsen E, Gilbert M. Video calls for dispatcher-assisted cardiopulmonary resuscitation can improve the confidence of lay rescuers – surveys after simulated cardiac arrest. J Telemed Telecare. 2011; 17(2):88-92.
Author notes
Pinto DJE contributed in the conception, data collection, analysis and discussion of the results, and writing of the article. Santos MR and Pires RM contributed to the critical review of the content of the article and final approval of the version to be published.
Corresponding author: Duarte José Esteves Pinto. Rua Álvaro Castelões, 463, 1º Frente N, Bloco B. 4450-042. Matosinhos, Portugal. E-mail: djestevespinto@gmail.com