Abstract: Adoption of an Intervention to Promote Physical Activity and Healthy Eating in Brazilian Health Care Settings. We analyzed the adoption of the VAMOS Program in Primary Health Care settings (PHC). We carried out a community-based study using mixed-methods in Primary Care Units in Florianópolis, Santa Catarina, Brazil. We assessed adoption through the RE-AIM framework. The Primary Care Unit adoption rate was 25%, and the adoption rate among professionals was 80%. We identified three themes related to adoption and, we found that organizational factors are among the challenges that health professionals face when they implement collective actions in PHC units. Still, they were not inherent factors in adopting VAMOS. Therefore, the VAMOS Program can be offered as a new health promotion methodology in PHC settings.
Keywords: community-based programs, programs evaluation, health promotion, professional.
Resumen: Analizamos la adopción del Programa VAMOS en el contexto de la Atención Primaria de Salud (APS). Realizamos un estudio de base comunitaria con métodos mixtos en Unidades Básicas de Salud en Florianópolis, Santa Catarina, Brasil. Evaluamos la adopción mediante la herramienta RE-AIM. La tasa de adopción de las Unidades de Atención Primaria fue del 25% y la tasa de adopción entre los profesionales fue del 80%. Identificamos tres temas relacionados con la adopción y encontramos que los factores organizacionales están entre los desafíos que enfrentan los profesionales de la salud cuando implementan acciones colectivas en las unidades de APS. Aún así, no fueron factores inherentes a la adopción de VAMOS. Por lo tanto, el Programa VAMOS puede ofrecerse como una nueva metodología de promoción de la salud en el contexto de la APS.
Palabras clave: programas basados en la comunidad, programa de evaluación, promoción de la salud, profesional.
Adoption of an intervention to Promote Physical Activity and Healthing Eating in Brazilian Health Care Settings
Universidad Nacional de Córdoba
Recepción: 18 Febrero 2018
Aprobación: 18 Julio 2021
Fuente: Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina (FAPESC)
Nº de contrato: 2014TR2263 -3513/2013
Financiamiento
Fuente: Coordenação deAperfeiçoamento de Pessoal de Nível Superior
Nº de contrato: 001
Prevention of chronic non-communicable diseases (NCDs) and promoting healthy lifestyles are essential components of the public health sector mission (World Health Organization [WHO], 2018). Accordingly, in many countries, public policies have focused on changing lifestyles throughout the population (WHO). In the Brazilian context, most of these actions have been integrated into a set of educational activities and programs implemented by the National Health System (known in Brazil as SUS) (Ministério da Saúde, 2017) to promote physical activity and healthy eating (Ramos et al., 2014).
The SUS guidelines (Ministério da Saúde, 2017) instruct its professionals to develop actions to primary prevention of NCDs and health promotion, especially in Primary Health Care settings (PHC). Since 2006, SUS has facilitated the implementation of some new community-based health programs such as “Academia da Cidade” in Recife (Hallal et al., 2010) and Aracaju (Mendonça et al., 2010) (Northeast region); “Curitiba Ativa” in Curitiba (Reis et al., 2010), and “Floripa Ativa” in Florianópolis (Benedetti & Lopes, 2009) (Southern region). The nature of these programs is similar, involving structured exercise classes, usually taught by instructors who are graduates of physical education degree programs. A wide variety of exercise modes are offered, such as aerobics, water aquatics, swimming, volleyball, yoga, weight training, dance, and others (Benedetti, Schwingel, Gomez, & Chodzko-Zajko, 2012). Despite these efforts, the adoption of effective health promotion strategies in PHC settings has shown varied performances (Manta et al., 2020; Ramos et al., 2014).
The management and implementation of health promotion initiatives vary substantially in Brazil from region to region (Manta et al., 2020). Studying the adoption of interventions allows researchers to understand what factors facilitate and/or hinder this process. It is also necessary to investigate how well proposed interventions align with organizational priorities and resources (Glasgow & Estabrooks, 2018). Thus, our study analyzed factors influencing the adoption of the “Vida Ativa Melhorando a Saúde” (VAMOS Program) version 2.0, in PHC settings in Florianópolis, Santa Catarina, Brazil.
VAMOS is a behavior change program that uses the "health education" methodology to motivate people to adopt an active and healthy lifestyle through physical activity and food (Benedetti, Manta, Gomez, & Rech, 2017). In addition, the program uses RE-AIM as a planning and evaluation tool (Almeida, Brito, & Estabrooks, 2013; Brito et al., 2018). However, this type of program in PHC units, with behavioral, educational, and multidisciplinary approaches aimed at integral health, is still incipient (Benedetti, Tomicki, & Konrad, 2019). Thus, it is relevant to analyze the adoption of the VAMOS in real Brazilian public health settings. Often, unknown organizational issues hamper the adoption of health promotion interventions potentially beneficial to the population.
The adoption of the VAMOS was analyzed using the RE-AIM framework (Almeida et al, 2013; Brito et al., 2018). Adoption is one of the framework’s dimensions, which is a measure of participation at the organizational level. It refers to the percentage and characteristics of the locations and/or professionals willing to offer a program or intervention (Almeida et al., 2013). Adoption is fundamental to understanding quantitative aspects of a program and addressing characteristics of the settings invited to implement the intervention (Glasgow & Estabrooks, 2018). Evaluating adoption and its intervening aspects permits us to fill gaps in the process of reach, implementation, effectiveness, and maintenance of an intervention. These dimensions are also considered in the RE-AIM framework, enabling a global analysis of different aspects during evaluating an intervention (Almeida et al., 2013; Brito et al., 2018). However, adoption has been poorly reported in studies, and data on this topic are scarce, as evidenced in systematic reviews using the RE-AIM framework (Holtrop et al., 2021; Konrad, Tomicki, Silva, Almeida, & Benedetti, 2017; Squarcini, Rocha, Munaro, Benedetti, & Almeida, 2015).
We conducted a mixed methods study based on the RE-AIM framework. A cross-sectional study design was adopted, combining quantitative and qualitative approaches.
Our study targeted two levels of participation: locals and professionals. 1) Primary Care Units (known in Brazil as UBS) in the Florianópolis with physical education professionals certified by the VAMOS Program's online training (n = 20) and 2) The physical education professionals working in UBS within the Florianópolis’ municipal network certified by the VAMOS Program's online training (n = 5). We point out that all physical education professionals in the Florianópolis municipal network were invited (n = 12) via electronic mail to participate in the 20-hour online training for VAMOS Program leaders and, subsequently, to offer the intervention at the UBS where they worked. However, only 5 conducted the training and received certification. Twenty UBS were eligible to adopt the VAMOS since each professional worked not only in a single UBS but between three and five units.
Physical education professionals working in public health in Florianópolis were identified through electronic contact with the Municipal Health Secretariat. In this way, an invitation was sent to participate in the training of the intervention. The trained professionals were invited to adopt and offer the VAMOS to users at the UBS where they worked. The professionals who adopted the program defined where (in which UBS) they would implement the VAMOS. They made the necessary adjustments with the management to implement the program. The research team offered all the support to the professionals who offered the program and those who worked at UBS to explain about the VAMOS and to solve possible implementation doubts.
We used the RE-AIM framework as an instrument to evaluate adoption (Almeida et al., 2013; Brito et al., 2018). The adoption dimension was assessed by the number of UBS that agreed to host the intervention and the number of professionals who chose to become program leaders and implement the VAMOS. Thus, we calculated two adoption rates. The first was the adoption rate of locations: dividing the number of UBS that offered the intervention by the number of eligible UBS in the city, multiplied by 100; and the second was the adoption rate of professionals: dividing the number of health professionals who offered the intervention by the number of eligible health professionals, multiplied by 100.
Furthermore, we collected qualitative data to identify factors that may have influenced the adoption of the intervention. We conducted 33 interviews (semi-structured) with UBS health professionals, including: physical education professionals – leaders of the VAMOS (PEF; n = 4), UBS managers (GE; n = 4), and professionals from other areas who were part of the health teams and who were, directly or indirectly, involved in the intervention (n = 25), including: community health workers (ACS; n = 11), nursing technicians (TE; n = 4), administrative technicians (TA; n = 3), physicians (ME; n = 2), nurses (EN; n = 2), oral health assistants (ASB; n = 2) and nursing residents (RE; n = 1).
The professionals who participated in the interviews were chosen at random. That is, they were approached at the workplace and invited to participate in the study. To verify the impact of adopting the VAMOS in the UBS, we considered both professionals who were directly involved with the intervention and professionals that did not participate in the intervention. In addition, we conducted a focus group with the program leaders to obtain additional information about the VAMOS and investigate adoption-related perceptions.
The interviews and the focus group addressed the following topics: opinion about the intervention adoption by the UBS, facts that motivated the adoption of the intervention, the importance of the intervention training (offered via distance education) for its adoption (specific question to the program leaders), among others. We also asked how the UBS’ routine changed with the adoption of the intervention, opinions about the inclusion of the intervention in the health service offered by the UBS, the UBS professionals’ qualifications and available time to offer the intervention, the most interesting and least interesting aspects of the intervention. We also asked the UBS managers for a cost-benefit analysis of the intervention.
Although the adoption dimension proposed by the RE-AIM framework considers only the organizational level of participation, we conducted focus groups (n = 5) with PHC users who participated in the intervention (P; n = 26). We asked about the reason that they chose to adopt the VAMOS, as well as why their UBS unit adopted the intervention.
The interviews were conducted individually by a research team member, with an average duration of 30 minutes each. The focus groups were conducted by three research team members, with an average duration of 50 minutes each. The interviews and focus groups were recorded and transcribed. All participants agreed to participate in the research by signing a consent form. After analyzing the data, the names of all participants were coded (example: PEF1; ME2...). The data were confidential, and only three members of the research team had access to the recordings, transcriptions, and data analysis.
We geo-referenced the eligible UBS units (n = 20) through their addresses using the Google Earth Pro platform. We established three network buffer sizes to verify the UBS surrounding characteristics based on the accessibility of walking routes near each UBS (Lopes, Hino, Moura, & Reis, 2018). The UBS socio-demographic characteristics were calculated based on the 2010 census (Instituto Brasileiro de Geografia e Estatística, 2011). We analyzed the number of households, number of residents, average household income per capita, racial and ethnic distributions, the proportion of men, proportion of women, proportion of adults, and proportion of older adults. Geospatial analyses were performed using the ArcGIS 10.5 software.
We performed absolute and relative frequency measures for categorical variables and mean and standard deviation measures for numerical variables. We used Student t-tests for independent samples and the Mann-Whitney U test to determine the significance of differences in characteristics between the UBS adopted and did not adopt the intervention with p < .05. We analyzed the data using SPSS 22.0 software.
Furthermore, we used the NVivo 12 software to assist us in analyzing the qualitative collected data. To analyze the information, we adopted the content analysis technique (Bardin, 1977). Three researchers categorized the information, performed the content analysis, and selected the reports, when necessary, a third researcher resolved disagreements.
Our study was approved by the Human Research Ethics Committee of the Federal University of Santa Catarina (No. 1.394.492) and is registered at ClinicalTrials.gov (NCT02823301).
We implemented the VAMOS in 2016-2019 in UBS settings in Florianópolis. The program is designed for people aged 18 or over and offers educational and motivational experiences in 12 weekly face-to-face meetings for three months. The maintenance phase is evaluated 12 months after the end of the intervention. The program addresses topics that develop strategies to change behaviors. The meetings last 90 to 120 minutes and are conducted by previously trained health professionals. In addition, 20-hour online training for VAMOS leaders is offered free of charge via distance education (José, Konrad, Ribeiro, & Benedetti, 2019).Details about the VAMOS can be found in previous studies (Benedetti et al., 2017; Tomicki et al., 2021).
There are 49 UBS in Florianópolis, 20 (40.8%) were considered eligible to participate in the study, and five offered the intervention. The UBS adoption rate was 25%. The intervention cost was covered for units that chose to implement it, and program leaders duties were adjusted to allow them to deliver the program without an overload of responsibilities. Overall, there were few significant differences between UBS that offered the program and those that did not (see Table 1). However, considering the coverage area of the eligible UBS, UBS that adopted the intervention had a lower proportion of white users when compared to UBS that did not adopt it (p < .05).
All physical education professionals were invited to participate in the training for the VAMOS Program (n = 12; 91.6% women). Five completed the training, and four adopted the intervention (one health professional implemented the program in two UBS locations). The adoption rate for health professionals was 80%. The professionals were not authorized to attend the training during working hours. They attended when they were not working, according to interest level and motivation. The lack of interest in the VAMOS, the reduction of working hours, and increased demands in some UBS was pointed out as reasons for not adopting the intervention. The program leaders’ reasons for choosing locations to implement the intervention were related to the support of health teams, knowledge of the UBS and surrounding areas, and having a bond with the community that uses the UBS and knowledge of their needs. Table 2 shows the characteristics of the eligible professionals who adopted and did not adopt the intervention.
From the interviews and focus groups, we identified three themes related to adoption. The first theme speaks to the vital role that program leaders/health professionals play in adopting of the program by the UBS. Their attitude towards starting a new program, opinions about the curriculum, new duties and responsibilities, and opportunities for self-care improvements were key adoption factors. The second theme raises implementation challenges and how they influence adoption. Shortage of professionals, high workload, and the UBS organizational structure adversely affected adoption. Lack of infrastructure and limited financial resources are also among the implementation challenges. The third theme highlights the importance of partnerships for adoption. The support obtained from researcher partners, including thoughtful training modules, was an essential part of adoption.
Comparison of the sociodemographic characteristics of the population covered by the eligible Primary Care Units
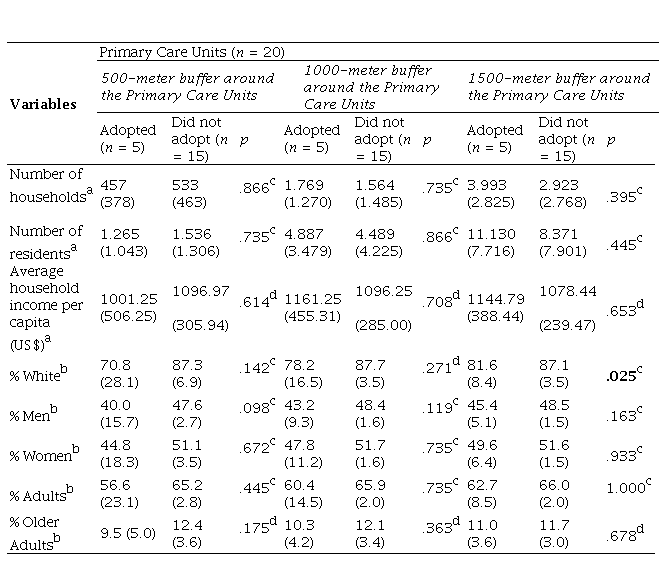
p = significance level at 5%. n = number. % = percentage. a = Data presented as mean and standard
Theme 1:Adoption centered on health professionals’ perceptions. A positive perception of professionals towards a new health initiative was the most salient finding from the qualitative part of this study. This theme reflects a consensus among all interviews. The following quote illustrates their overall welcoming attitude: "[...] having people around, mobilizing the population and proposing new activities and other things for them to do is always good" (TA3).
In the search for ways to meet the population's needs, health professionals see the nature of new health promotion programs and interventions essential to adoption in public health contexts. The focus of the VAMOS on health education, physical activity, and healthy eating positively influenced its perception by health professionals. The following quote supports this: “[...] we perceive a need for programs like this, aimed at improving lifestyle; so, working with this in primary care makes perfect sense [...] it is a program that is in accordance with public health” (PEF3).
The innovative intervention curriculum and related materials also motivated the adoption of VAMOS by health professionals. The material was perceived as inclusive and following high pedagogic standards, as shown in this quote: “A complete behavior change program [...] that offers a complete training, basic material, didactic material” (PEF3).
The intervention provided a novel approach to work and new duties and responsibilities for program leaders. The example in the following fragment: “[...] we will be able to care for those who have problems, but especially for those who do not have them yet; the program covers well what the Family Health Strategy recommends, which is not our daily routine” (TE2).
The “behavioral change” component of the intervention presented an opportunity for the health professionals to reflect on their health, as we can see in the fragment: "I think it is an incentive to the population and also to us, professionals [...] to reflect on the health issue" (TE4).
In addition, individual factors appear to influence the adoption of interventions by the UBS units and their professionals. UBS users decided to participate in the VAMOS Program because they needed an incentive to change their lifestyle and take better care of their health. For example, the following fragments: “[...] I had a health problem, and I needed something to encourage me to change my lifestyle” (P1).
Characteristics of eligible health professionals who adopted and did not adopt the VAMOS Program
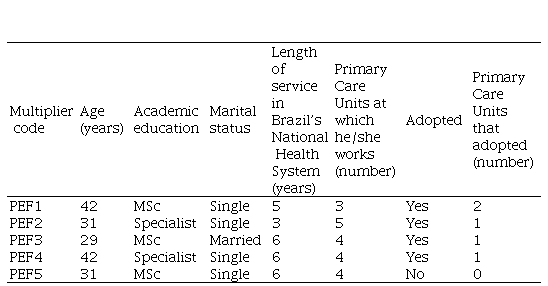
PEF = Pysical Education Professional. MSc = Master's Degree.
Theme 2: Adoption influenced by implementation challenges.Shortage of professionals and the high workload at UBS impacted the adoption of interventions, as shown in these quotes: "Most of the employees here at the UBS, due to the flow of the movement, get medical certificates, sick leaves, because they are stressed out" (ACS11). "[...] we have a population that is always larger than we can handle" (GE4).
Organizational structure and policies at each UBS were also considered to be essential factors in program adoption. The example in the following fragment: "Maybe the teams should be required to participate [...] here we only do what we are obliged to do" (GE4). "It depends on the professional [...] from technician to doctor it is much more difficult" (ACS3). Despite this, many UBS professionals are willing to adopt new health promotion strategies, as we can see in the fragment: "[...] we are always open to these activities that promote health" (GE4).
Interventions were perceived as beneficial to compensate for the lack of care at UBS settings, as we can see in this quote: “I think it comes to add more [...] to help us when we cannot meet the demand, we have to choose either preventive or curative measures, promotion is still maintained only because we have these aids [...] because if we do not, it is unfeasible, no way” (GE4).However, the profile of assistance and services offered by UBS units is gradually changing, impacting the collective service that is provided, for example: “I analyze what SUS was like [...] almost six years ago and today [...] before, we had many more groups, our meetings were much more productive, now the management tends to break this [...] spaces for groups are very reduced. Multidisciplinary work is increasingly difficult” (PEF2).
The UBS professionals supported the adoption of the program. However, the degree to which professionals were able to become engaged varied. The example in the following fragment: "We have an internal routine, and we were unable to participate as much as we would like to" (TE4). “The involvement of the professionals was positive” (GE3).The UBS's choice to adopt the intervention dependent on the support of the professionals who worked in them. The following fragment is an example: "I knew it would work there and that in other UBS this support is precarious" (PEF2). However, due to restrictions on time available for new programming, VAMOS adoption was not always a priority in the UBS service. The example in the following fragment: “[...] the professionals that we have [...] with the demand that we have, they are already involved in other programs, in other services, and there is little time left” (ME1).
When the program was implemented, there was no adverse impact on the routine of UBS and its professionals. For example: "[...] we have a lot of activities, meetings, groups and this was one more, so this is all part of our work routine, it is just another one that was included in our routine" (ACS6).Furthermore, there is a shortage of adequate space in the UBS to offer group interventions. The following fragments illustrate these concerns: “[...] there is no suitable place to receive a large weekly demand, the difficulty would lie in structure” (ME1) "The auditorium is always reserved for other UBS activities" (ASB1).
The method by which the municipal government administers transfers of funds from the federal government was viewed as problematic: "This question of funds, I do not know what amount we have available" (GE4). "[...] the municipal government acquires some things [...] which sometimes are not used, so we should be consulted about it because there is not much need, the demand is low" (GE1).Despite this, investing in new forms of work aimed at promoting the population's health was seen as positive, as we can see in the fragments: "I think any money that comes to encourage a healthy lifestyle is welcome" (GE2). "[...] this reflects a public benefit, a benefit for public health [...] I think it would be worth investing" (GE3).
Theme 3: Partnerships promote adoption.It was viewed as essential to subsidize and support health professionals regarding the adoption of public health interventions, as shown in the following fragments: “[...] training to be able to participate is very interesting” (GE2). “[...] the more training we have, the more ideas we’ll have for the job, they always have something to contribute” (PEF1).
The VAMOS Program training was well accepted and met its primary objective of training health professionals to act as program leaders of the intervention and to promote its adoption: "It [the training] delivered the basic tools of the work to us" (PEF1). “With the training, it is likely to become a program that is part of the UBS strategies. Brought it to my practice, many strategies to approach behavior change in the most diverse spheres within my service [...] I realized that the [blinded for review] language ended up pervading other activities that I develop" (PEF3).
In addition, to the VAMOS Program training, some professionals understood that the researchers’ participation was fundamental. For example: “[...] the link with the University, I find it very interesting [...] the issue of evaluating an activity within the UBS, we have many difficulties and do not have time to see what we are achieving in each activity, so I thought that being monitored by the University was a very good proposal” (PEF1).
Our study analyzed the adoption of the VAMOS by health professionals working in UBS settings within the Brazilian PHC system. We used the RE-AIM framework to assess adoption. It is through adoption that a program starts. Thus, it is necessary to have professionals interested in offering the program so that the evaluation of other dimensions of RE-AIM is possible. Our results show that one-quarter of the eligible UBS adopted the intervention and, of the certified professionals invited to be program leaders, only one did not.
We found few differences when the UBS that adopted the program and those that declined to adopt the intervention were compared. Adopters and non-adopters had similar numbers of health care teams working at each unit. Sociodemographic characteristics of individuals living close to units that adopted the intervention were similar to those living near units that did not. However, UBS units that chose to adopt the VAMOS were in communities that were more ethnically diverse than those that did not. This finding is encouraging, as public health interventions are most needed in vulnerable populations (Baba et al., 2017) and for low-income groups living in areas with high population densities (Hallal, Matsudo, & Farias Júnior, 2012).
The health professionals who adopted the intervention and the professionals who did not adopt it were broadly similar in profile. All the program leaders had considerable experience in the public health service. Our interviews suggest that motivation to adopt public health interventions is related to an individual’s understanding and appreciation of behavioral change methodology and strategy (Benedetti et al., 2017). The support that the UBS professionals received from the University, either through training or through contact with the research team, was essential. Strengthening the relationship between researchers and professionals working in the public health service is a way to optimize program delivery and outcomes. Our study suggests that strong collaborations between researchers and front-line public health workers can enhance the efficacy of an intervention. This finding is consistent with the conclusions of a prior study which found that joint action between researchers, managers, and professionals can be an efficient strategy in the formulation, application, evaluation, and control of public health interventions (Florindo & Guerra, 2017).
The availability of resources can impact the adoption of a public health intervention. In our study, the scarcity of health professionals was a significant impacting adoption. Prior research (Borges et al., 2019; Maissiat, Lautert, Pai, & Tavares, 2015) has suggested that turnover of professionals in health teams and exhaustion, overwork, and the high number of work responsibilities are among the reasons UBS professionals fail to adopt interventions. A multi-professional approach that emphasizes collaborative teams is essential for success in the SUS system in Brazil (Santos, Guerra, Andrade, & Florindo, 2015).
Many factors related to UBS infrastructure also influenced the adoption of the VAMOS. The absence of adequate spaces to offer group activities has been previously reported (Borges et al., 2019). Similarly, inadequate physical space has been identified by others as a factor that hinders the adoption of interventions (Figueira et al., 2018). The inadequacies of UBS facilities adversely impact the delivery of quality health care, which leads to dissatisfaction among professionals and users and limits the overall quality of service delivery (Moreira, Lima, Vieira, & Costa, 2017).
The UBS managers who adopted the intervention saw the VAMOS as a useful investment in cost and population impact. Despite this, we found that they seldom participated in decisions regarding the use of federal resources allocated to a UBS unit with the PHC system. The Ministry of Health recently reformulated the PHC financing model, prioritizing equity criteria, health team performance indicators, and incentives to implement priority programs (Harzheim et al., 2020). When deciding to use resources in specific health promotion actions such as the VAMOS, UBS teams should be consulted in the decision-making process, taking the population’s health care needs into account.
One of the main reasons influencing the VAMOS Program's adoption by UBS users was emphasizing preventive health care through an active and healthy lifestyle. The VAMOS was developed given the lack of UBS sponsored interventions with a preventive focus. It was developed with the population’s needs in mind (Ferreira et al., 2019). We believe that VAMOS motivates users to participate because of its differentiated approach based on two essential elements to healthy living: physical activity and healthy eating.
Our study has some limitations. One of them is that we conducted interviews and focus groups during the VAMOS Program's implementation at the UBS. They may have influenced the professionals' perceptions of the adoption process. Furthermore, we did not interview the health professional who chose not to adopt the intervention, which would have added insights related to the program's acceptability. However, it is also important to stress the strengths of our study. First, our data are pioneering in Latin America. Second, the intervention was adopted in realistic public health settings and conducted by health professionals who work in the UBS units. Third, we used the RE-AIM framework, which is used internationally to evaluate programs but is little used in Latin America. Moreover, we identified the sociodemographic characteristics of the catchment area of eligible UBS through geospatial analyses. Finally, we addressed essential elements related to adopting public health interventions and collected information from everyone, directly and indirectly, involved in the intervention.
The design and method of the VAMOS, the presence of support from researchers, and users’ perceptions of need positively influenced the adoption. Organizational factors such as human resources, infrastructure, and financial support are frequent challenges that health professionals face when implementing any type of collective action in PHC settings. However, our study found that UBS can successfully overcome these challenges. In addition, understanding and addressing the existing challenges to the adoption process at the institutional level will enable understanding of the impact and sustainability of public health interventions. Thus, we recommend that the adoption of interventions in PHC should be assessed along with intervening factors, especially those related to the management and organization of the system.
https://revistas.unc.edu.ar/index.php/racc/article/view/32202/41163 (pdf)
[Artículo corregido , vol. 15, 35] https://revistas.unc.edu.ar/index.php/racc/article/view/32202/41163
To the Municipal Health Secretariat of Florianópolis for their collaboration in implementing the VAMOS Program at the Primary Care Units, as well to the managers, professionals of the health teams, and users of Primary Health Care involved in the study.
This work was supported by the Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina (FAPESC) - Programa Pesquisa para o SUS (PPSUS) [No. 2014TR2263 - 3513/2013] and; Coordenação de Aperfeiçoamento de Pessoal de Nível Superior [Finance Code 001] studentship
camitomicki@gmail.com
Comparison of the sociodemographic characteristics of the population covered by the eligible Primary Care Units
p = significance level at 5%. n = number. % = percentage. a = Data presented as mean and standard
Characteristics of eligible health professionals who adopted and did not adopt the VAMOS Program
PEF = Pysical Education Professional. MSc = Master's Degree.
