Otras temáticas
Georeferencing at a Health Service, an Experience from Community Assets1
La georreferenciación al servicio de la salud, una experiencia desde los activos comunitarios
Georreferenciamento a serviço da saúde, u,a experiêcia dos bens da comumidade
 Diana Paola Betancurth Loaiza diana.betancurth@ucaldas.edu.co
Consuelo Vélez Álvarez consuelo.velez@ucaldas.edu.co
Natalia Sánchez Palacio natalia.sanchez@ucaldas.edu.co
Diana Paola Betancurth Loaiza diana.betancurth@ucaldas.edu.co
Consuelo Vélez Álvarez consuelo.velez@ucaldas.edu.co
Natalia Sánchez Palacio natalia.sanchez@ucaldas.edu.co
Georeferencing at a Health Service, an Experience from Community Assets1
Ánfora, vol. 30, núm. 54, pp. 236-253, 2023
Universidad Autónoma de Manizales

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-CompartirIgual 4.0 Internacional.
Recepción: 03 Marzo 2022
Aprobación: 09 Mayo 2022
Abstract: Objective: to analyze the use of physical and digital georeferencing techniques in the service of health from a community asset experience. Methodology: in the framework of an exploratory study with a mixed method, with a recurrent transformative design, a social cartography was carried out that included the analysis of physical and digital georeferencing. Results: the community territorial experience is part of the concrete experience, digital mappings as a result of technological tools and ICT development were used, with social mappings that directly linked the communities. On the one hand, it is an input that allowed to know the general context to streamline processes and on the other hand, other elements were highlighted in the practices, such as socio-cultural, economic and political elements. Conclusions: in the globalized world, the use of physical and digital maps enrich the processes of assessment and community participation, they are configured as a means, but not an end, which provides decision-makers with a tool to dynamize interaction and community empowerment processes.
Keywords: Community, Community health, Sense of Coherence, Geographical locations, Geographic mapping (MeSH, NCBI).
Resumen: Objetivo: analizar el uso de técnicas de georreferenciación física y digital al servicio de la salud desde una experiencia de activos comunitarios. Metodología: en el marco de un estudio exploratorio con método mixto, de diseño transformativo recurrente, se realizó una cartografía social que incluyó el análisis de la georreferenciación física y digital. Resultados: la experiencia territorial comunitaria hace parte de la vivencia concreta, se utilizaron mapeos digitales producto de herramientas tecnológicas y desarrollo en TICS, con los mapeos sociales que vincularon las comunidades directamente. Por un lado, es un insumo que permitió conocer el contexto general para agilizar procesos y de otro lado, se destacaron otros elementos en las prácticas, como las socio-culturales, económicas y políticas. Conclusiones: en el mundo globalizado la utilización de los mapas físicos y digitales enriquecen los procesos de valoración y participación comunitaria, se configuran como un medio, más no un fin, que sin lugar a dudas aporta a los tomadores de decisiones como herramienta para dinamizar procesos de interacción y empoderamiento comunitario.
Palabras clave: comunidad, salud comunitaria, sentido de coherencia, ubicaciones geográficas, mapeo geográfico (DeCS, BIREME).
Resumo: Objetivo: analisar o uso de técnicas de georreferenciamento físico e digital a serviço da saúde a partir de uma experiência de bens comunitários. Metodologia: no âmbito de um estudo exploratório de método misto com um desenho transformador recorrente, foi realizado um mapeamento social que incluiu a análise de georreferenciamento físico e digital. Resultados: a experiência territorial comunitária é parte da experiência concreta, os mapeamentos digitais foram utilizados como produto de ferramentas tecnológicas e de desenvolvimento de TIC, com mapeamentos sociais que ligavam diretamente as comunidades. Por um lado, é um input que permitiu conhecer o contexto geral para agilizar os processos e, por outro, outros elementos foram destacados nas práticas, tais como socioculturais, econômicas e políticas.Conclusões: no mundo globalizado, o uso de mapas físicos e digitais enriquece os processos de avaliação e participação comunitária e se configura como um meio e não como um fim, o que sem dúvida contribui para os tomadores de decisão como uma ferramenta para dinamizar os processos de interação e empoeiramento comunitário.
Palavras-chave: comunidade, saúde comunitária, Senso de coerência, localizações geográficas, mapeamento geográfico (DeCS, BIREME).
Cómo citar:
Betancurth, D. P., Vélez, C. &Sánchez, N. (2023). Georeferencing at the health service, an experience from community assets. Ánfora, 30(54), 236-253. https://doi.org/10.30854/anf.v30.n54.2023.912
Universidad Autónoma de Manizales. L-ISSN 0121-6538. E-ISSN 2248-6941. CC BY-NC-SA 4.0
Introduction
Georeferencing is considered the basic way to introduce plans and maps into an information system (Solanas Jiménez, 2018). The combination of physical and digital georeferencing as a result of technological development and the demands for studying social phenomena in recent years has developed information analysis tools that enable decision-makers to identify groups of greater vulnerability and thus the targeting of actions and the management of intersectoral strategies based on existing resources to improve living conditions (Yumisaca et al., 2018).
The use of georeferencing systems has allowed citizens to participate and agree on recognizing and locating information that has been stored and that can become a valuable resource to strengthen community interactions (Cascón Katchadourian & Ruiz Rodríguez, 2016).
In the health context, Geographic Information Systems (GIS) have been highlighted by the World Health Organization (WHO) for their contribution to public health, insofar as they allow the spatio-temporal location of events (Carvalho & OPAS., 2006). Geoprocessing generates more than technical benefits. It creates the possibilities of visualizing the response capacity of the health sector to the needs of the population and the resources that communities can contribute to devise solutions (Angélica et al., 2018).
Traditionally, georeferencing systems have been used to identify risks in communities and thus prioritize vulnerable populations, analyzed from variables such as housing, working conditions, environmental problems, and access to the health system, among others (Aguirre, 2016; Ramasco-Gutiérrez et al., 2017). At present and under the salutogenic perspective, the importance of its use is highlighted for the identification of community assets in health. The concept focuses on those material and human resources that can improve communities’ capacities to maintain health and well-being, which when located in the territorial space add value and facilitate lifestyle (Cubillo-Llanes et al., 2018).
Social cartography as a method of physical georeferencing and a methodological approach to the recognition and analysis of the territory allows understanding it and representing it through maps. Therefore, it is possible to affirm that this is a social and political tool at the service of communities and policyholders, as well as a tool for decision making (Barragán-León, 2019).
The processes of physical or digital georeferencing of community assets make sense, insofar as they allow placing those assets in the perspective of health promotion, and incorporating positive health by seeking to promote participatory actions with transformative capacity and intersectoral vision (Cofiño et al., 2016).
Based on the previous approaches, the objective of this work is to analyze the use of physical and digital georeferencing techniques at the service of health from an experience of community assets.
Methods
Within the framework of an exploratory study with a mixed method, with a recurrent transformative design, a social mapping was carried out that included, the analysis of physical and digital georeferencing for the identification of community assets.
Cartography is a methodological route, which can nest different techniques. It is woven from the relationships that emerge in the space/territory context in health (Silva et al., 2020). On the one hand, it is understood that the construction of the social map of community assets is a process that allows “the approach to a conception of a certain territory in permanent change, while allowing consolidating a sense of belonging from graphic representations of the community existing reality in the community” (Betancurth et al., 2020). On the other hand, it is worth reflecting that georeferencing tools are fundamental for the public agency. As a whole, their analysis allows proposing reducing the gaps, attacking inequality and tending toward better levels of well-being (Longhi, 2020). The tools per se are a dead letter if they do not derive focused and effective actions.
- 1. Selection criteria used. The immersion in the territory by the researchers-subject was carried out between May 2018 and May 2019, in four neighborhoods of the department of Caldas (Colombia). Within the selection criteria used, was the identification of risk by Family record. For this case it was an accumulated risk with ratings between 3.29 and 3.89 indicting a medium-low risk. This study was carried out within the framework of the implementation of the Primary Health Care strategy.
- 2. Analysis unit. The unit of analysis focused on the community. The key actors were community leaders, with whom the logistics of the mapping activities were structured, planned, and executed.
- 3. Techniques used. Cartographic techniques were used through seven workshops and interviews with 40 community leaders and the community in general, in addition to the analysis of electronic georeferencing in the four neighborhoods where it was decided to carry out the research. In the first instance, four physical neighborhood maps were prepared based on the tours with the community. Later they were contrasted with the georeferencing of the Caldas Social Observatory (APS) and with Google Maps tools. The field diaries kept during each visit were taken into account as analytical devices for the apprehension (Silva et al., 2020).
- 4. Analysis. For the analysis, the geocoding and georeferencing process was taken into account, with which the content analysis was performed.
- 5. Ethical aspects. By virtue of compliance with the parameters expressed in the Declaration of Helsinki and in Resolution 08430 of 1993 for the Colombian territory, the study was approved by the ethics committee of the University of Caldas with the code CBCS-065 where it realized the required parameters and principles for working with the community.
Results
The community territorial experience is part of the specific experience. It is a necessary complement that was evidenced in this research. the digital mapping product of technological tools and ICT development was put into dialogue, with the social mapping that linked the communities directly. Both were of interest as methodological devices that were incorporated and complemented within the social cartography framework whose purpose in a critical aspect sought to provide the best alternatives for decision-making and targeting of the institutional offer.
In the study for the identification of community assets, the research team started from the knowledge of a geo-positioning and geo-referencing system of the Social Observatory of Caldas (see figure 1), Google Maps tools and the geographic referrer of the ATLAS.ti software, to access digitally to the properties to visit (four neighborhoods) in terms of space-time location – in the sense of place – which simultaneously could be contrasted with the characterization in terms of number of families. This characterization was obtained from the observatory and permited knowing the families and their main public health problems in each of the neighborhoods. It is noteworthy that this is a procedure that the Territorial Directorate of Health of Caldas carries out in the Municipalities.
This input allowed previously ascertaining, and as a general approximation, the social situation of the subject population. Outlining the points where people with a similar condition were located (for example, health conditions, disability conditions, minors, older adults, population of special vulnerability) with this system through filters was possible.
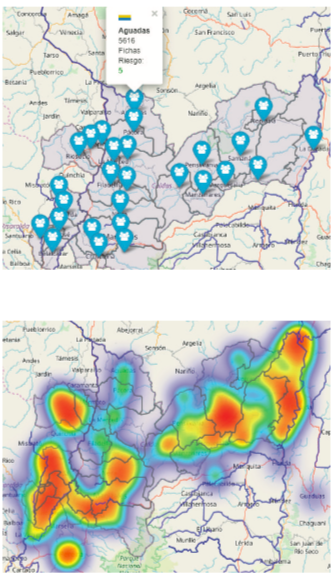
Figure 1
Digital Mapping
Source: Social Observatory of Caldas.
The physical map was built directly with the people of the neighborhood (collective mapping). To create it, the researchers motivated the participants to highlight other aspects to take into account in the practices in the field, such as social, cultural, temporal, and circumstantial elements, which are invisible in digital mapping (traditionally analyzed to identify risks) (see figure 2).
This methodology beyond the traditional, allows communities to recognize and build knowledge about their territory, by valuing their heritage, wealth, and resources (community garden, parks, courts, educational centers, representative people, etc.), so that they can motivate themselves and trend toward healthier lifestyles. In other words, this type of work with the communities makes gradually developing love for the territory possible, as a way of establishing emotional relationships among the residents, the neighborhoods, and the cities they inhabit. The mappings carried out went beyond the micro-territory. They were socialized with community leaders and representatives in workshops and meetings, which allowed recognizing, highlighting, prioritizing, agreeing and focusing on specific processes, with the aim of strengthening them or purposefully setting needs, whose solutions integrate the participation of the inhabitants and decision makers of each territory.

Figure 2
Map of Assets La Floresta Villamaría (Neighborhood 2)
The preceding implied the rapprochement, as well as the articulation with the municipal offices (including all their secretariats), the municipal hospitals and local health directorates, both municipalities and the Departmental Health Directorate. This intersectorality enabled negotiating/building together, formulating actions to follow, achieving that with the identification of the offer, articulation has to be required. The interconnection of all the actors led to more structured processes, such as the formulation of specific proposals based on exposure factors, as well as on community assets that would make dynamizing and strengthening protective factors possible (define both at the bottom of the page).
For example, there is the progress in the second phase of community gardens within the framework of the Good Living project. In the mapping it was identified as the greatest asset along with their homes. Alternatively, it allowed showing the strengthening of assets related to the local economy as a greater need (this is considered an intermediary social determinant) and associative group assets, that would allow greater political participation of the communities.
The end of the process was complemented with metaplans on future situations to continue working. The results of community work remained in the neighborhoods, since they are by and for the community. with them they are expected to become the input and starting point for both the public and private institutions and estates to streamline their actions, for the benefit of the quality and living conditions of the people of these prioritized neighborhoods.
| Visual schemes that allowed community interpretations. | Visual diagrams that allowed decision-makers to interpret and locate specific situations by locality. |
| Dialogues were established with the community as a producer of knowledge; it is the community that is in charge of contributing and validating the maps, since no one knows its environment better than it does and can value its relevance for a better quality of life. | There was evidence of empirical progress in the use of geoprocessing (benefits of the use of technology) in the management of Primary Health Care (PHC) services, given that it was previously done only manually, which leaves a precedent of the importance of articulating digital georeferencing in the area to improve and make more timely decision. |
| The mapping allowed the community to become visible and have recognition, which contributed to the creation of a neighborhood identity. There was participation in the construction and validation of the maps, as well as giving the community a voice by listening to their perceptions of how they see their neighborhood and what it means to them. | It provided a rich set of tools (location, filtering by events, identification of points of deepening or focalization) and virtual procedures for the treatment and analysis of health data, under a territorial analytical approach, which enables its implementation and dynamization as part of social epidemiology, in which the georeferencing of events related to the Social Determinants of health is a current challenge. |
| Values such as solidarity, dialogue and trust, which are consolidated and built into community work, were promoted. | The time performance is efficient (given that the research was carried out in four neighborhoods in different municipalities), this allowed for a great advance prior to the visits, since the information is available in real time and digitally geo-referenced. |
| The social fabric was strengthened through neighborhood networks (they know each other and interact). They also recognize each other's potential so that in the future they can complement each other to solve problems and activate protective factors. | When entering, the platforms are equipped. The satellite data can be seen in real time (global positioning system or GPS). So the most accurate and updated information is being received, and thus can guide the health manager ensuring that their actions are direct and specific to the needs and vulnerable populations and thus more effective. |
| Symbolically, the community values its territory and its perception complements what in digital georeferencing is systematized in the software. | It is dynamic, agile, and easy to access, available at all times. |
| It accounts for settlements or invasions, which the digital maps did not detect (in one of the neighborhoods this situation was detected). | The dynamism is related to the platforms and the possibility of manipulating the information; it must also be continually updated so that the information is real. |
| The maps made permit representing potentialities and/or principal needs of the community, which in the future become inputs for those actors working with these prioritized communities. | The access was digital, under the assumption that it corresponds to updated information. |
Both mappings allowed knowing, recognizing, and valuing the territories inhabited by the people in the neighborhoods. The resources and needs were integrally identified (Table 1), which made adjusting community processes possible which in the beginning were weakened and became stronger through autonomy and commitment. Those processes improve residents’ living space, allow them to feel more identified and united with the territory they inhabit.
These types of processes can be interrelated with the aim of expediting the identification of needs and vulnerabilities in populations through digital mapping, which can be complemented with the community vision expressed in the work developed with them through physical georeferencing and thus make a more effective intervention of the different actors and sectors that wish to act on their benefit possible.
Discussion
The use of physical and digital georeferencing in health has experienced rapid growth in recent decades. It has become an additional tool for decision makers to apply the required measures of the events being analyzed and epidemiological studies that allow for the inclusion of spatial variability by identifying disease clusters or the distribution of the population by age groups for subsequent interventions (Valbuena & Rodriguez, 2018). In this regard, authors such as Angélica, Chiaravalloti, and Luiz presented a project in PHC in which the use of geolocation as a powerful technical tool to improve health response capacity is evidenced (Angélica et al., 2018).
The approximation to the social conditions of greater vulnerability and their location on the maps as georeferencing techniques of location and spatialization, are opportunities that should be taken into account by the public agency to reduce gaps between groups of equal conditions, as confirmed by Longhi in his study about living conditions in Argentina (Longhi, 2020). As such, Delgado, Agudelo, Vargas, and Moreno show that the social, cultural, and anthropological relationships that the population creates as a source of solutions to personal and collective health needs can be understood (Jaramillo Delgado et al., 2022).
Participation processes constitute a challenge for states to the extent that they allow the strengthening of the social fabric. In this sense, under the gaze of the communities, the construction of physical maps in which the community assets are located through participatory methods, are another important source of participation and information. They are configured as a possibility of valuing their heritage, wealth, and expressing their relationship with the immediate environment, which is their neighborhood or city. In this sense, social cartography can be affirmed as contributing to the development of life routes at the community level (Betancurth et al., 2020). In addition, they can be used as a strategy that stimulates the processes of promoting lifestyles in the territory (María et al., 2019; Valencia González et al., 2019). The starting point of these processes is the recognition and participation of the social actors. The territorial study invites one to rethink health, even more so when it is framed through community ownership (Betancurth et al., 2020; Spinelli, 2016).
The preceding is evidenced in the study carried out by Ospina concerning the reconfiguration of spatial practices. In this study, mapping implies the reconstruction of the meanings, actions, and discourses that integrate people and their way of living. Additionally, it broadens the vision of the subject as an instrumental being that appropriates and represents its environment and its socio-territorial relations. This allows conceding value and a sense of belonging to the territory and the community that inhabits it, while at the same time fostering the construction of images, stories, memories, and knowledge that arise from collective spaces where the members of the community are ready to intervene and promote those links that articulate the social-personal plane with the spatial-geographical plane.
Another important aspect within the framework of using mapping is the possibility of identifying the sectors that are configured as a contribution to the development of the daily life of the communities supported under the guise of how each of them makes significant contributions to the communities’ quality of life and therefore better health indicators (Ramos Herrera et al., 2019). In relation to the previous, studies such as the one carried out by Delgado et al. show how the territory, which is graphically represented, is a space with relationships and forms of connection on a personal level, as well as on environmental and physical levels that promote the daily activities of the people who occupy it, by redefining their values, beliefs, knowledge, and popular practices that allow generating cultural responses and appropriation of their territories (Jaramillo Delgado et al., 2022).
This is how, in the words of Feo-Ardila and Espinel-Rubio, the territory is configured as a space of discoveries where behaviors, actions and thoughts converge and sprout, as well as individual and collective practices, which allows the territory to be associated as a physical and symbolic area, in which they can establish an interpersonal and family daily life, as well as the creation of community fabric and ties that start from social and community dynamics, which are consolidated through cultural practices and the relationship with the inhabited space. In this sense, through mapping, the communities and their actors determine their social, political, and cultural identity, which allows the territory to be identified as an emblematic and strong space, where meeting points are established either from oppression/vulnerability or empowerment/appropriation of common interest. This is confirmed by the results of the study carried out by Barragán which states that cartography is a social product with political intentions.
As can be evidenced in the results of the studies contrasted with the research experience, the characteristics of the individuals predominate. In effect, there is a gap in the recognition of the territory when understanding that the place is decisive for the community analysis in the framework of public health. In this sense georeferencing is a strategy of great contribution.
Both physical community mappings and digital ones according to the research experience, have allowed understanding that they are configured as a means and not the end. They are not static techniques that reflect the inhabited place or spatial information as a source of information. On the contrary, they go far beyond those limits that define it; it is a joint analysis of living spaces and social relationships that need to be known in order to manage their resources in a positive way (Arenas-Monreal et al., 2019; Esteban Peña et al., 2020; Molina-Betancur et al., 2020). In this sense, one of the contributions of the developed work confirms that stated by Radicelli et al. who affirm that the cartographic processes allow the different disciplines of the social sciences to interrelate and recognize their potentialities to analyze and understand the social dynamics that allow for improving their quality of life. Other authors expose the importance of knowing the dynamics of the public and private health sectors through mechanisms of networks and physical and digital georeferences for the success of any public health initiative, as they allow the identification of relationships, variations in the phenomena, as well as helping to focus the actions aimed at impacting them.
For Buzai (2019), the quantitative spatial analysis through the Geographic Information System (GIS) through the use of cartographic modeling, turns out to be very useful in the identification of central elements and the definition of critical work areas for their strengthening. In addition, it allows integrating social, cultural, and psychological elements into the geographic context (Domínguez et al., 2018). In this sense, digital advances at the service of community health pose new challenges, allowing those who use the tools and devices the freedom for a holistic analysis and the flexibility to take advantage of this type of resources, in a way that generates constructive and collaborative learning. What stands out is the importance of geographic data to arrive at concrete analyzes of phenomena, the establishment of alliances with government institutions, and with this, adequately influence community intervention policies (Shah et al., 2020).
The authors recognize as a possible limitation of the work developed, the non-use of maps of time (past, present, and future) as a connection that may allow carrying out in-depth understandings or interpretations of the reality lived by the communities in future investigations.
Conclusions
In the globalized world, the use of physical and digital maps enrich valuation and community participation processes. The location and recognition of assets favors synergy with their environment, however, georeferencing is a means and not an end, which contributes to decision-makers and becomes a tool to stimulate processes of interaction and community empowerment.
In community mapping, it is evident that it is the populations know their territory best, therefore, proposals that are generated have a greater possibility of being accepted and providing continuity if those populations are included.
In the context of innovation in health, digital georeferencing becomes an opportunity for the elaboration of thematic maps and generates new challenges in community participation processes when it comes to the analysis of health conditions and situations. In this sense they interact in an ideal way for the work with the communities through physical georeferencing.
Referencias
Aguirre, J. (2016). La aplicación de las tecnologías de información y comunicación en la prevención comunitaria del delito: los casos de georreferenciación en Monterrey, México. Rev.Relac.Int.Estrateg.Segur, 11(2), 239–270. https://www.redalyc.org/articulo.oa?id=92746462011
Angélica, E., Rebolledo, S., Neto, F. C., & Giatti, L. L. (2018). Experiencias, beneficios y desafíos del uso de geoprocesamiento para el desarrollo de la atención primaria de salud. Rev Panam Salud Publica, 42, 1–13. https://doi.org/10.26633/RPSP.2018.153
Arenas-Monreal, L., Pacheco-Magaña, L., Parada-Toro, I., Rueda-Neria, C., & Cortez-Lugo, M. (2019). Mapeo Comunitario para impulsar la participación comunitaria dentro del diagnóstico de salud poblacional. Enfermería Universitaria, 16(2), 120–127. https://doi.org/10.22201/eneo.23958421e.2019.2.636
Barragán-León, A. N. (2019). Cartografía social: lenguaje creativo para la investigación cualitativa. Sociedad y Economía, 36, 139–159. https://doi.org/10.25100/sye.v0i36.7457
Betancurth, D. P., Vélez Álvarez, C., & Palacio, N. (2020). Cartografía social: construyendo territorio a partir de los activos comunitarios en salud. Entramado, 16(1), 138–151. https://doi.org/10.18041/1900-3803/entramado.1.6081
Buzai, G. D. (2019). Condicionantes socioespaciales de la salud. Definición de áreas críticas en la cuenca del río luján, argentina. Geofocus: Revista Internacional de Ciencia y Tecnología de La Información Geográfica, 24, 99-16. https://doi.org/10.21138/GF.650
Carvalho, M. S. org. P. M. de F. de, org. S. S. M. dos, org., & OPAS., B. M. da S.-M. O. P. da S.-. (2006). Conceitos básicos de sistemas de informação geográfica e cartografia aplicados à saúde, 2000. http://www.opas.org.br/informacao/temas_produtos_detalhe.cfm?id=58&idprod=8
Cascón Katchadourian, J. D., & Ruiz Rodríguez, A. Á. (2016). Descripción y valoración del software MapTiler del mapa escaneado a la capa interactiva publicada en la Web. El Profesional de La Información, 25–26. https://dialnet.unirioja.es/servlet/articulo?codigo=5730199
Cofiño, R., Aviñó, D., Benedé, C. B., Botello, B., Cubillo, J., Morgan, A., Paredes-Carbonell, J. J., & Hernán, M. (2016). Promoción de la salud basada en activos: ¿cómo trabajar con esta perspectiva en intervenciones locales? Gaceta Sanitaria, 30(s1), 93–98. https://doi.org/10.1016/j.gaceta.2016.06.004
Cubillo-Llanes, J., Botello-Díaz, B., Gea-Caballero, V., March, S., Segura-Benedicto, A., & Hernán-García, M. (2018). Assets: from maps to territory. SESPAS Report 2018. Gaceta Sanitaria, 32, 98-102. https://doi.org/10.1016/j.gaceta.2018.06.006
Domínguez, D. L., Hermosillo, A., Méndez, C., Sahagún, M., & Palacios, P. (2018). Mapa Digital de México para el análisis de riesgo suicida. Investigación Y Práctica En Psicología Del Desarrollo, 2, 90–102. https://revistas.uaa.mx/index.php/ippd/article/view/690/667
Esteban Peña, M., Fernandez Velasco, E., Jiménez García, R., Hernández Barrera, V., & Fernandez del Pozo, I. (2020). Salud e incidencia y diferencias en vulnerabilidad territorial de la ciudad de Madrid. Rev Esp Salud Pública., 94(7), 1–14. https://www.mscbs.gob.es/biblioPublic/publicaciones/recursos_propios/resp/revista_cdrom/VOL94/ORIGINALES/RS94C_202004020.pdf
Jaramillo Delgado, G., Agudelo Arias, M., Jaramillo Vargas, J., & Moreno Villa, F. (2022). Reconocimiento de agentes reproductores de saberes y prácticas populares en salud. Hacia Promoc. Salud, 27(1), 159–175.
Longhi, F. (2020). Condiciones de vida y contextos de salud. Un análisis territorial aplicado a la población argentina (2001-2010). Huellas, 24(1), 133–156. https://dialnet.unirioja.es/servlet/articulo?codigo=7499252
María, A., Pastas, C., Andrés, G., Bolaños, S., Álvarez Bravo, M., Alexander, C., Guerrero, Z., De Lourdes Hernández Narváez, E., Maritza, S., & Tulcan, M. (2019). Promoción de estilos de vida saludables: estrategias y escenarios. Hacia. Promoc. Salud., 24(2), 139–155. https://doi.org/10.17151/hpsal.2019.24.2.11
Molina-Betancur, J. C., Agudelo-Suárez, A. A., & Martínez-Herrera, E. (2020). Community health assets mapping in a slum in Medellin (Colombia). Gaceta Sanitaria, 35(4), 333-338. https://doi.org/10.1016/j.gaceta.2020.04.012
Ramasco-Gutiérrez, M., Heras-Mosteiro, J., Garabato-González, S., Aránguez-Ruiz, E., & Aguirre Martín-Gil, R. (2017). Implementación del mapa de la vulnerabilidad en salud en la Comunidad de Madrid. Gaceta Sanitaria, 31(5), 432–435. https://doi.org/10.1016/j.gaceta.2016.07.026
Ramos Herrera, I., Portugal Zegarra, F., González Castañeda, M., & Robles Pastrana, J. (2019). Distribución geoespacial de la salud en Jalisco: análisis sobre los Objetivos de Desarrollo del Milenio. Salud Jalisco, 6(3), 147–156. https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=92038
Shah, D., Vijayan, S., Chopra, R., Salve, J., Gandhi, R. K., Jondhale, V., Kandasamy, P., Mahapatra, S., & Kumta, S. (2020). Map, know dynamics and act; a better way to engage private health sector in TB management. A report from Mumbai, India. Indian Journal of Tuberculosis, 67(1), 65–72. https://doi.org/10.1016/j.ijtb.2019.07.001
Silva, V. M., Lopes, J. M. R., Dantas, R. T., Abreu, S. M. B. de, & Pinto, N. V. (2020). Cartografia do programa de atividade física desenvolvido no Núcleo Ampliado de Saúde da Família e Atenção Básica de Canindé, Ceará. Research, Society and Development, 9(7), 1-12. https://doi.org/10.33448/rsd-v9i7.5076
Solanas Jiménez, J. (2018). Tratamiento de cartografía histórica para el análisis de la forma urbana en sistemas de información geográfica. Biblio3W, 23(1), 742–798.
Spinelli, H. (2016). Volver a pensar en salud: Programas y territorios. Salud Colectiva, 12(2), 149–171. https://doi.org/10.18294/sc.2016.976
Valbuena, A. M., & Rodriguez, L. A. (2018). Análisis espacial en epidemiología: revisión de métodos. Rev. Univ. Ind. Santander. Salud, 50(4), 358–365.
Valencia González, A., Hincapié Zapata, M., Gómez Builes, G., & Molano Builes PE. (2019). Tendencias de evaluación en promoción de la salud. Actualización del debate en la década 2005-2015. Hacia Promoc. Salud., 24(1), 123–137. https://doi.org/10.17151/hpsal.2019.24.1.11
Yumisaca, J., Ruiz, F., & Orrala, O. (2018). Propuesta metodológica basada en herramientas gis para el inventario de recursos turísticos en la Provincia de Santa Elena Methodological proposal based on gis tools for the inventory of tourist resources in the Province of Santa Elena. Revista de Estrategias Del Desarrollo Empresarial, 4(11), 1–11. www.ecorfan.org/spain
Notes