Abstract:
This study aims to analyze the use of pediatric palliative sedation and understand how it is connected to medical training and the doctor-patient relationship in Brazil. This is a cross-sectional exploratory study using an online survey targeted at pediatricians working in Brazil to evaluate concepts of palliative sedation and aggressive symptom management. The lack of specific training, protocols, and institutionalized guidelines can create uncertainties in palliative care. This also contributes to the increased end-of-life suffering those children and their families face. Improving education in pediatric palliative care is an urgent and pressing need in Brazil.
Keywords: Critical care, Medical errors, Ethics, Pain, Palliative care.
Resumo:
Este artigo objetiva analisar o uso de sedação paliativa e entender como ela está ligada à formação médica e ao relacionamento médico-paciente no Brasil. Com base em pesquisa on-line focada em pediatras que trabalham no Brasil, este estudo transversal e exploratório buscou avaliar conceitos de sedação paliativa e tratamento de sintomas agressivos. A falta de treinamento específico, protocolos e diretrizes institucionalizadas pode gerar incertezas no cuidado paliativo. Isso também contribui para o aumento do sofrimento de fim da vida que essas crianças e suas famílias enfrentam. Melhorar a educação em cuidados paliativos pediátricos é uma necessidade urgente e imediata no Brasil.
Palavras-chave: Cuidados críticos, Erros médicos, Ética, Dor, Cuidados paliativos.
Resumen:
Este artículo tiene como objetivo analizar el uso de la sedación paliativa y comprender cómo esta se vincula con la formación médica y la relación médico-paciente en Brasil. Basándose en una encuesta en línea con pediatras que trabajan en Brasil, este estudio transversal y exploratorio pretendió evaluar los conceptos de sedación paliativa y tratamiento de síntomas agresivos. La falta de formación específica, de protocolos y guías institucionalizadas puede generar incertidumbres en los cuidados paliativos. Esto también contribuye al aumento del sufrimiento que enfrenta estos niños al final de la vida y sus familias. Es imprescindible y urgente mejorar la educación en cuidados paliativos pediátricos en Brasil.
Palabras clave: Cuidados críticos, Errores médicos, Ética, Dolor, Cuidados paliativos.
Carátula del artículo
Ethical dilemmas for pediatricians administering palliative sedation to children in Brazil
Dilemas éticos de pediatras ao administrar sedação paliativa em crianças no Brasil
Dilemas éticos de los pediatras al administrar sedación paliativa a niños en Brasil
 Daniele Rodrigues danieledemoura.rodrigues@gmail.com
Daniele Rodrigues danieledemoura.rodrigues@gmail.com
Universidade São Francisco, Brasil
Djalma Lessa djalma.lessa@usf.edu.br
Universidade São Francisco, Brasil
Denise Gonçalves Priolli denise.priolli@usf.edu.br
Universidade São Francisco, Brasil
Revista Bioética, vol. 30, no. 2, pp. 413-422, 2022
Conselho Federal de Medicina
Received: 11 September 2020
Revised document received: 17 May 2022
Accepted: 23 May 2022
The death of a child represents a subversion of the natural order of life. Moreover, the act of caring for a child facing death has always presented limitations 1 . However, medicine still has a long way to go in improving the palliative care (PC) of children with terminal illnesses 2 .
Palliative sedation (PS) is a form of aggressive symptomatic treatment during PC 3 , 4 . Authors define PS as a last resort treatment, initiated when all other methods of symptom control have failed 5 . PS is a highly specific therapy and thus it is crucial to identify both the continuous and persistent symptoms which are difficult to treat and bear by the patient 3 , 4 . It should be stressed, however, that it requires close monitoring and full cooperation between the family and hospital team 3 , 4 . PS, if carried out properly, is the intentional use of sedative medications to relieve intolerable suffering from refractory symptoms by reducing patients’ awareness and consciousness with their consent or their legal representatives’ and is incapable of accelerating death. Thus, it can also be defined as an aggressive form of symptomatic treatment 3 , 4 .
The advancement of medicine and technologies with more effective treatments for previously incurable diseases, accompanied by the advent of pediatric intensive care units, has directly impacted the perception of pediatrics and its conduct 6 . However, it is still necessary for the various health services in different localities to be structured to enable more humanized support for pediatric patients and their families 7 . In Brazil, medical training in PC is rare 8 , 9 .
If the use of PS in adults already faces complex ethical dilemmas and doubts, its use in children is even more complex. Its complexity lies not only in the difficult task of communicating with parents but also in the suffering caused by the potential death of the child. The prospect of violating ethical concerns with the deliberate decrease in patient consciousness is a big challenge for pediatricians 10 who, in general, feel uncomfortable practicing PS 11 .
Studies in European countries have shown that PS occurs in between 2.5% and 16.5% of all adult deaths and has become more widespread in recent years. As a result, the publication of guidelines and recommendations to guide and help doctors deal with the clinical and ethical challenges of this practice with adults has increased in recent years 12 . On the other hand, while several studies suggest that PS is often used in end-of-life practices in children’s guidelines 10 , 13 , 14 , data on such practices remain rare. In the United States, recent studies have shown that the lack of research in the use of PS with children fails to reflect the frequency of its practice (which it is not rare) and the same scenario is a potential reality in Brazil. Additional in-depth research in Brazil is necessary so the literature can better understand how decisions are made and how PS relates to the explicit intent of reducing suffering in children with terminal illnesses 11 , 12 , 15 , 16 .
Some studies in Latin America have explored different aspects of the practice of pediatric PS and the lack of knowledge in Brazilian pediatricians about PC options, as well as how ethical and legal care protocols can cause insecurity with parental decision making in the use of PS. As a result, guardians lack knowledge of the alternatives available to them and critically ill children may suffer unnecessary pain and discomfort 17 - 24 .
Because of the limited data and absence of guidelines around pediatric PS in Brazil, it is thus crucial to survey pediatricians so as to understand their motivations and dilemmas for the practice of PS or lack of it in Brazil.
Method
This cross-sectional exploratory study used an online survey, targeting pediatricians working in Brazil, and followed STROBE guidelines. Respondents were invited to complete an online questionnaire and agreed to participate by signing an informed consent form. All procedures are in accordance with the Declaration of Helsinki (Code of Ethics of the World Medical Association) 25 and the Ethical Standards and Guidelines of CNS Resolution 466/2012 of the Ministry of Health 26 . The pediatricians in the sample were divided into two groups according to whether they had or not practiced PS.
The survey, now closed, conducted in the Portuguese language, was hosted online via Google Forms. Respondents were surveyed about the concepts of PS and Aggressive Symptom Management (ASM). PS concept was presented as the intentional use of sedative medications to relieve intolerable suffering of refractory symptoms by a reduction in patient awareness3 , whereas ASM is a procedure that produces sedation proportional to the anguish of symptoms, accepting unconsciousness as provided for unintentional side effect of this management11 .
Then, two short vignettes were given to assess the kinds of decisions physicians might make regarding treatment and drug administration, as well as the individuals and factors which might influence those decisions when caring for pediatric patients at the end of their lives. The questionnaire was based and adapted from Henderson and collaborators, as they described it: the survey assessed agreement with a definition of palliative sedation, as well as thoughts about its alignment with ASM11 . Respondents answered a total of 31 questions, ranging from objective and open-ended questions. It was structured around the following topics: PS concepts, the actual practices of pediatricians in the use of PS, perceptions regarding the institutionalization of PS in services around the country, and their knowledge of PC and PS in schools they attended. Duplicate responses were excluded from the analysis.
The minimum sample size was determined using a sample calculator (n=198). For open-ended answers, qualitative analysis by saturation was adopted, whereas demographic data were descriptively analyzed . Rather than thinking of qualitative and quantitative strategies as incompatible, they should be seen as complementary. Although procedures for textual interpretation differ from those of statistical analysis, because of the different type of data used and questions to be answered, the underlying principles are much the same27 . In the search for correlations, inferential statistical analysis was performed. For the rejection of the null hypothesis, p <0.05 was adopted. SPSS 20.0 for Windows was used for analysis.
Results
The research sample included 202 participating pediatricians, of which 34% were general pediatricians; 30%, critical care physicians; 25%, neonatologists; 10%, palliative care physicians; 8%, hematologists or oncologists; and 35%, from other specialties. In total, 61% of our sample were aged between 25 and 44 years old, whereas 38% was aged above 45 years old.
The young women from Southeast Brazil ( p =0.04) represented most pediatricians. The data showed that 50% of respondents had practiced PS in the last 12 months and that 86% of these lacked professional qualification in PC. Of the 10% respondents with professional qualification in PC, 74% had practiced PS in the last 12 months. In our sample, 90% of pediatricians received no training in PS during medical school. This was correlated with professional qualification in PC ( p =0.04), with a higher error rate for those without any professional qualification in PC (rho=−0.729; p <0.00). The practice of PS was also related to the practice of a religion ( p =0.04) ( Table 1 ).
Table 1
Pediatricians’ demographic and professional characteristics data. Brazil, 2019-2020
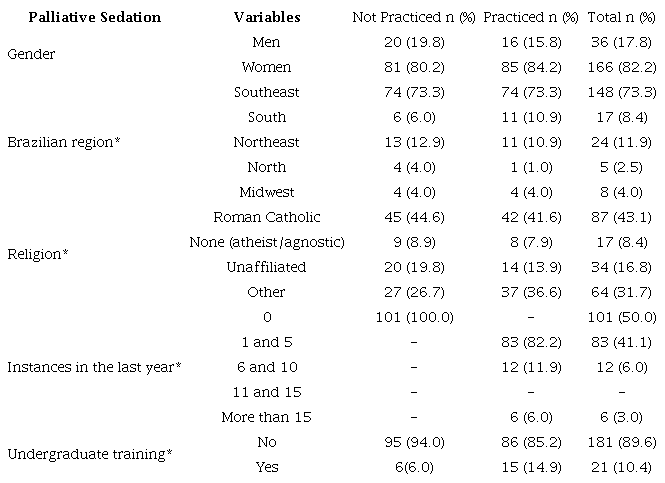 *p <0.05
*p <0.05
Respondents had doubts about reducing patients’ awareness and consciousness using PS. They were divided about their agreement with the adopted definition of PS (52% agreed versus 48% who disagreed), especially on the aspect of consciousness (36% pointed to an unnecessary reduction of consciousness). Otherwise, 52% of respondents believe that PS and ASM are equal and thus feel more comfortable with the term “ASM” than “PS,” highlighting the importance of keeping patients conscious.
The main indicators for the use of PS in the study were pain (85%), dyspnea (42%), and delirium (23%). Pediatricians who choose the indicators which constitute total pain correctly were more inclined to use PS (rho=0.872; p <0.00). Inversely, the wrong indications are related to absence of total pain identification (rho=-0.459; p =0.04).
In this study, 65% of the respondents also indicated they were afraid to opt for PS out of fear of creating conflicts with the family. Of those who were palliative specialists, 68% showed the same behavior.
Additionally, more than 55% of pediatricians surveyed stated that their institutions lack a standard protocol to implement PS and 89% said they were unaware of legal regulations in Brazil around the practice.
Discussion
The teaching of end-of-life care in medical schools in Brazil receives little attention 9 . Approximately 90% of all respondents in this study reported a lack of education on PS in their medical training. The scarcity of medical curricula focused on palliative medicine in undergraduate courses causes an empirical reduction in the use of PS in Brazil. Thus, its practice is not based on knowledge and qualification, increasing the risk of medical errors and creating danger for patients. On the other hand, since PS is also practiced by physicians without professional qualification in PC, current medical training should also contemplate adding courses around the provision of end-of-life care in their curriculum to provide guidance for future medical professionals. This training will provide generalists with an integrated, theoretical, and practical foundation in palliative skills 9 .
Among pediatricians with professional qualification in PC, 74% had practiced PS, suggesting that professionals with specific qualification are more likely to adopt appropriate measures to deal with end-of-life situations 11 . When analyzing the characteristics of the participants who practice SP, we found that several components may or may not influence it, such as religious practice. Non-Christian respondents practice it more than Christians, reflecting the multifactorial character of the practice.
Half of our respondents disagreed with the PS definition Wolf, Hinds and Sourkes adopted 3 , especially on consciousness maintenance. Some point to the lack of reduction of consciousness or even indicate the importance of keeping the patient conscious, suggesting a lack of knowledge of the definition of PS and pointing to the ambiguities surrounding the practice 11 .
In total, 52% of the respondents felt uncomfortable stating they are practicing PS but indicated that they are using aggressive symptom management (ASM), whereas half claimed that there was no difference between the two. It is extremely important to outline that there are no differences between PS and ASM. One reason that PS is not openly named, in addition to the question of the intention of maintaining consciousness (as discussed earlier), is that it might violate cultural beliefs of an ethical and/or religious character. The deliberate decrease in the patient’s consciousness is seen to be close to the practice of euthanasia 28 . The international literature also corroborates our data, in which U.S. pediatricians also question the maintenance of consciousness and differences between PS and ASM 11 . Specifically, the practice of euthanasia, in addition to being unethical, is also considered a crime in Brazil (Brazilian Penal Code, Art. 121. Paragraph 1) 29 . The lack of knowledge arising from lack of training creates an internalized concept of PS that is fueled by fears and fantasies not only in relation to the legitimacy of the practice but also regarding the legal support to limit the provision of curative therapy in patients with terminal illnesses 5 . The Code of Medical Ethics 30 currently in force in Brazil makes explicit the need and ethical duty of the physician to provide PC for patients with terminal illnesses.
Regardless of the circumstances, pediatricians should be prepared to address symptoms as they manifest themselves in the death process 11 . Although pediatricians’ motivations to use PS are influenced by the manifestation of pain and dyspnea, which are classic criteria for the use of PS, other symptoms – which are currently incompatible with the practice of PS, such as immobility, convulsion, sweating, pallor, tachycardia, nausea, fatigue, hypertension, crying, communication difficulties, epilepsy, bone disorders, headache, orthopedic deformities, cases of self-harm and suicide attempt – were also identified 31 - 34 . International studies advocate the need for guidelines clarifying what is considered acceptable practice and point to the role and importance of institutions in developing PS protocols which include criteria such as patient selection, choice of duration of therapy, as well as the necessary documentation for the protection of the doctor and the patient 16 . More than half (55%) of our respondents stated that their institutions lack a standard protocol to implement PS and 89% said they were unaware of legal regulations in Brazil about the practice 11 . The lack of guidelines in PS, the various barriers to the implementation of bioethics committees in Brazil, given their importance in advising decision-making and the dignity of the person 35 , the lack of specific training, and the difficulty of communication with the family could increase the possibility of professional exhaustion and errors in the conduct of clinical practice and ethical management, creating greater risk to the provision of end-of-life care. However, to the best of our knowledge, no studies consider the rate of error of physicians’ use of PS and its correlation to the absence of specific guidelines in PC. Most pediatricians feel they are helpless in decision-making and highlight the need for substantial materials explaining PS 4 , 9 , 11 .
Although they were first implemented in the United States in the 1960s, bioethics committees remain optional in Brazilian health institutions and hospitals 36 . Hospital bioethics committees are multi- and transdisciplinary, assisting in decision-making and in issues of moral health conflicts 37 , 38 and offering support and protection to patients, their families, caregivers, and other health professionals. They are spaces for dialogue in hospitals and health institutions, helping and reinforcing the quality of services and decisions in health, guaranteeing respect for fundamental individual freedoms 39 , and responsible for the educational and advisory challenge of fostering ethical awareness sustained in the autonomy and dignity of patients regarding decision-making 40 , 41 .
In the absence of guidelines and protocols, the following questions could be used to generate greater confidence in pediatricians who consider the use of PS. They are as follows: have all efforts been made to identify and treat the causes producing reversible suffering? Have all non-pharmacological approaches been applied, such as relaxation and distraction techniques? Is sedation consensual 8 ?
PS is a valuable option for children with terminal illnesses, although it presents additional complexities in pediatric practice, such as parental consent and understanding 11 . For fear of conflict with the family, 65% of respondents were afraid to use PS, and 68% of palliative specialists have the same fear. This suggests that the fear of conflict is not an exclusively key determinant of the use of PS 2 . Only after knowing the effective participation of the family in the end-of-life process can an appropriate strategy be defined to improve the quality of care for children hospitalized with terminal illnesses. In this context, it is essential to use preventive measures, using the ethical motivation of anticipatory virtue and the mitigation of conflicts, aiming to anticipate negative outcomes and enabling an individualized and studied planning for each patient, reconciling the desires of patients and family members and the performance of the health team 42 . Without the participation of the family in this decision, physicians may be engaging in practices that fail to meet the expectations, wishes, and values of patients with terminal illnesses and their parents 2 , which could lead to undesired consequences.
Due to the absence of protocols and guidelines, the difficulty of managing the care of children with terminal illnesses and the lack of education around PC and PS in medical schools, increased by physicians self-sufficiently practicing PS, it is necessary to reflect on their possible impact, raising the idiosyncrasies distinctly from non-pediatrician physicians 5 . The internalized concept about PS in the absence of clear protocols and guidelines is formed by personal morals and beliefs, which are based on subjective experiences. This subjectivity is not based on medical training and will cause professionals to make incorrect decisions. Pediatricians who use PS without clear guidelines on patient eligibility raise the possibility of errors in practice. Physicians will also be engaging in unethical and negligent practice. This can prolong end-of-life suffering for patients and their families, generating dysthanasia and acting against the ethical principle of non-maleficence. On the other hand, if PS is used in an ineligible patient, another unethical practice will have been practiced, mysthanasia, which may cause suffering and hurt to patients and their families. The term comes from the Greek ( mys =unhappy, thanathos =death, “unhappy death”); which means miserable, precocious, and avoidable death. Mysthanasia indicates that death is impinged by the maintenance of poverty, violence, drugs, and lack of infrastructure 8 , 29 . The systematic reduction of health financing; the indiscriminate opening of medical schools, the misuse of money available in the budget; the contempt and devaluation of physicians, eroded by corruption, incompetence, and inhumanity are facets of mysthanasia. It affects life and death, increasing the vulnerability of the patients in most need 2 and based on the concept of social responsibility and health — Article 14 of the Universal Declaration on Bioethics and Human Rights — health promotion is one of the central objectives of governments, which should cherish access to quality health care and eliminate marginalization without distinction or discrimination 39 , 43 . The concept of mysthanasia can also be applied to the education budget, an area which is directly interconnected with health since it offers the right conditions to medical training and practice and decrease idiosyncrasies. This is in fact, malpractice, in which such imprudent acts can lead to violation of the principle of dignity in death (Appendix).
The bioethical discussion thus arises to contribute to the search for balanced responses to current conflicts, essential in determining the forms of intervention to be scheduled and in prioritizing actions 46.
The generalizability of our results to the larger population of Brazilian pediatric physicians is threatened by the questionable accuracy of the list we used for our population. Some physicians within the population were likely excluded from the list and/or had incorrect e-mail addressed listed, and several other names on the list are probably now not a part of the population. Consequently, the likelihood of both under- and overcoverage must be considered as a study limitation.
Final considerations
In Brazil, the lack of guidelines on end-of-life care for the pediatric population is evident. Guidelines with this scope are of paramount importance as they enable the improvement of practice, deepen the discussion on indications, and guarantee the maintenance of ethics in decision-making. We need better training in pediatrics regarding end-of-life practices to increase patient safety, considering that pediatric palliative sedation is not only practiced by palliative care providers. Morally, the best practice will result in less suffering in the end-of-life process and guarantee the active participation of the family in the decision-making process. The improvement of education in pediatric palliative care is an urgent need in Brazil with the objective of making end-of-life care services increasingly refined and articulated in ethical principles.
Several spheres may be responsible for improving education in palliative care and developing professionals with the knowledge and ability to deal with end-of-life situations. From hospital managers improving the training aimed at palliative care in undergraduate and medical residencies with their teams, an growing number of hospital ethics committees promoting continuous training and assisting in decision-making and moral health conflicts, to professionals who must be aware that end-of-life processes are part of the practice of medicine and that the possession of this knowledge will impact the quality and offer good-quality medicine for their patients, actively seeking to develop this sphere of knowledge.
In conclusion, Brazilian pediatricians who practice PS are mostly young women who are not necessarily trained in PS and usually work in the developed areas of the country. Their main motivation to practice PS is to relieve patients’ pain and dyspnea. However, there is concern around the family’s role in the decision-making process of the use of PS. The lack of specific training, protocols, and institutionalized guidelines can create uncertainties over the conduct of PC with risks of misconduct in the practice of medicine, raising the possibility of increased end-of-life suffering of patients with terminal illnesses.
Acknowledgments
Palliative Care League USF.
References
Iglesias S, Zollner A, Constantino C. Cuidados paliativos pediátricos. Resid Pediatr [Internet]. 2016 [acesso 12 ago 2021];6(supl 1):46-54. DOI: 10.25060/residpediatr-2016.v6s1-10
Lago PM, Devictor D, Piva JP, Bergounioux J. End-of-life care in children: the Brazilian and the international perspectives. J Pediatr [Internet]. 2007 [acesso 12 ago 2021];83(2 supl):109-16. DOI: 10.2223/jped.1627
Wolfe J, Hinds PS, Sourkes BM. Preface. In: Wolfe J, Hinds PS, Sourkes BM, editores. Textbook of interdisciplinary pediatric palliative care [Internet]. Philadelphia: Elsevier Saunders; 2011 [acesso 12 ago 2021]. p. xvii. DOI: 10.1016/b978-1-4377-0262-0.00055-4
Korzeniewska-Eksterowicz A, Przysło Ł, Fendler W, Stolarska M, Młynarski W. Palliative sedation at home for terminally ill children with cancer. J Pain Symptom Manage [Internet]. 2014 [acesso 12 ago 2021];48(5):968-74. DOI: 10.1016/j.jpainsymman.2014.01.012
Piedade MAO, Cardoso Filho CA, Priolli DG. Prevalência de sedação paliativa no Estado de São Paulo: uma demanda médica emergente. Einstein (São Paulo) [Internet]. 2020 [acesso 12 ago 2021];18:eAO5395. DOI: 10.31744/einstein_journal/2020AO5395
Piva JP, Garcia PCR, Lago PM. Dilemas e dificuldades envolvendo decisões de final de vida e oferta de cuidados paliativos em pediatria. Rev Bras Ter Intensiva [Internet]. 2011 [acesso 12 ago 2021];23(1):78-86. DOI: 10.1590/S0103-507X2011000100013
Garros D. Uma “boa” morte em UTI pediátrica: é isso possível? J Pediatr [Internet]. 2003 [acesso 12 ago 2021];79(supl 2):S243-54. DOI: 10.1590/S0021-75572003000800014
Ferreira SP. Sedação paliativa. In: Oliveira, RA, coordenador. Cuidado paliativo [Internet]. São Paulo: Cremesp; 2008 [acesso 1 jun 2022]. p. 355-361. Disponível: https://bit.ly/3m4Qjkn
Toledo AP, Priolli DG. Cuidados no fim da vida: o ensino médico no Brasil. Rev Bras Educ Méd [Internet]. 2012 [acesso 12 ago 2021];36(1):109-17. DOI: 10.1590/s0100-55022012000100015
Drake R, Frost J, Collins JJ. The symptoms of dying children. J Pain Symptom Manage [Internet]. 2003 [acesso 1 jun 2022];26(1):594-603. DOI: 10.1016/s0885-3924(03)00202-1
Henderson CM, FitzGerald M, Hoehn KS, Weidner N. Pediatrician ambiguity in understanding palliative sedation at the end of life. Am J Hosp Palliat Care [Internet]. 2017 [acesso 12 ago 2021];34(1):5-19. DOI: 10.1177/1049909115609294
Pousset G, Bilsen J, Cohen J, Mortier F, Deliens L. Continuous deep sedation at the end of life of children in Flanders, Belgium. J Pain Symptom Manage [Internet]. 2011 [acesso 12 ago 2021];41(2):449-55. DOI: 10.1016/j.jpainsymman.2010.04.025
Postovsky S, Moaed B, Krivoy E, Ofir R, Ben Arush MW. Practice of palliative sedation in children with brain tumors and sarcomas at the end of life. Pediatr Hematol Oncol [Internet]. 2007 [acesso 12 ago 2021];24(6):409-15. DOI: 10.1080/08880010701451079
Mallinson J, Jones PD. A 7-year review of deaths on the general paediatric wards at John Hunter Children’s Hospital, 1991-97. J Paediatr Child Health [Internet]. 2000 [acesso 12 ago 2021];36(3):252-5. DOI: 10.1046/j.1440-1754.2000.00495.x
Kiman R, Wuiloud AC, Requena ML. End of life care sedation for children. Curr Opin Support Palliat Care [Internet]. 2011 [acesso 12 ago 2021];5(3):285-90. DOI: 10.1097/SPC.0b013e3283492aba
Gurschick L, Mayer DK, Hanson LC. Palliative sedation: an analysis of international guidelines and position statements. Am J Hosp Palliat Care [Internet]. 2015 [acesso 12 ago 2021];32(6):660-71. DOI: 10.1177/1049909114533002
Barbosa SMM, Lecussan P, Oliveira FFT. Particularidades em cuidado paliativo: pediatria. In: Oliveira, RA, coordenador. Cuidado Paliativo [Internet]. São Paulo: Cremesp; 2008 [acesso 1 jun 2022]. p. 128-38. Disponível: https://bit.ly/3m4Qjkn
González-Ronquillo MA, Velasco Pérez G, Garduño-Espinosa A. Sedación y analgesia en la fase terminal en pediatría. Informe de dos casos y revisión de la literatura. Acta Pediatr Méx [Internet]. 2013 [acesso 12 ago 2021];34(1):21-7. Disponível: https://bit.ly/3x9U3ri
Támara LM. Descriptive cohort trial of terminal patients in medical home care in Bogotá-2008-2012. Rev Colomb Anestesiol [Internet]. 2014 [acesso 12 ago 2021];42(2):100-6. DOI: 10.1016/j.rca.2014.01.002
Vallejo-Palma JF, Garduño-Espinosa A. Palliative care in paediatrics. Acta Pediátr Méx [Internet]. 2014 [acesso 12 ago 2021];35:428-35. DOI: https://bit.ly/3PUjYKC
Lazzuri OE. Sedación agónica en niños: ¿es moralmente ética? Rev Fac Cienc Méd (Córdoba) [Internet]. 2017 [acesso 12 ago 2021];74(2):85-7. Disponível: https://bit.ly/3PUmpgn
Fernández Urtubia B, Trevigno Bravo A, Rodríguez Zamora N, Palma Torres C, Cid Barria L. Uso de opiáceos en niños con cáncer avanzado en cuidados paliativos. Rev Chil Pediatr [Internet]. 2016 [acesso 12 ago 2021];87(2):96-101. DOI: 10.1016/j.rchipe.2015.10.006
Cacciavillano W. Soporte clínico oncológico y cuidados paliativos en el paciente pediátrico [Internet]. Buenos Aires: Instituto Nacional del Cáncer; 2013 [acesso 12 out 2021]. Disponível: https://bit.ly/3atiPcJ
Zuleta-Benjumea A, Muñoz SM, Vélez MC, Krikorian A. Level of knowledge, emotional impact and perception about the role of nursing professionals concerning palliative sedation. J Clin Nurs [Internet]. 2018 [acesso 12 out 2021];27(21-22):3968-78. DOI: 10.1111/jocn.14582
Associação Médica Mundial. Declaração de Helsinque [Internet]. Helsinki: Associação Médica Mundial; 1964 [acesso 24 maio 2022]. Disponível: www.ufrgs.br/bioetica/helsin1.htm
Conselho Nacional de Saúde. Resolução nº 466, de 12 de dezembro de 2012. Trata de pesquisas e testes em seres humanos. Diário Oficial da União [Internet]. Brasília, 13 jun 2013 [acesso 24 maio 2022]. Disponível: https://bit.ly/3mnoWSV
Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet [Internet]. 2001 [acesso 12 out 2021];358(9280):483-8. p. 483. DOI: 10.1016/S0140-6736(01)05627-6
Morrison W, Kang T. Judging the quality of mercy: drawing a line between palliation and euthanasia. Pediatrics [Internet]. 2014 [acesso 12 ago 2021];(133 supl 1):S31-6. DOI: 10.1542/peds.2013-3608f
Marcão RF. Eutanásia e ortotanásia no anteprojeto do Código Penal brasileiro [Internet]. 2005 [acesso 12 ago 2021]. Disponível: https://bit.ly/3aflQgC
Conselho Federal de Medicina. Código de Ética Médica: Resolução CFM nº 2.217, de 27 de setembro de 2018, modificada pelas Resoluções CFM nº 2.222/2018 e 2.226/2019 [Internet]. Brasília: Conselho Federal de Medicina; 2019 [20 maio 2022]. Disponível: https://bit.ly/2YX9oNm
Chater S, Viola R, Paterson J, Jarvis V. Sedation for intractable distress in the dying: a survey of experts. Palliat Med [Internet]. 1998 [acesso 12 ago 2021];12(4):255-69. DOI: 10.1191/026921698671831786
Fainsinger RL, Waller A, Bercovici M, Bengtson K, Landman W, Hosking M et al. A multicentre international study of sedation for uncontrolled symptoms in terminally ill patients. Palliat Med [Internet]. 2000 [acesso 12 ago 2021];14(4):257-65. DOI: 10.1191/026921600666097479
Del Fabbro E, Dalal S, Bruera E. Symptom control in palliative care: part III: dyspnea and delirium. J Palliat Med [Internet]. 2006 [acesso 12 ago 2021];9(2):422-36. DOI: 10.1089/jpm.2006.9.422
de Graeff A, Dean M. Palliative sedation therapy in the last weeks of life: a literature review and recommendations for standards. J Palliat Med [Internet]. 2007 [acesso 12 ago 2021];10(1):67-85. DOI: 10.1089/jpm.2006.0139
Sayago M, Amoretti R. Comitês de bioética hospitalar: importância, funcionamento e dificuldades de implementação. Rev. bioét. (Impr.) [Internet]. 2021 [acesso 12 ago 2021];29(4):832-4. DOI: 10.1590/1983-80422021294517
Goldim JR, Raymundo MM, Fernands MS, Lopes MH, Kipper DJ, Francisconi CF. Clinical bioethics committees: a Brazilian experience. J Int Bioethique [Internet]. 2008 [acesso 20 maio 2022];19(1-2):181-92. DOI: 10.3917/jib.191.0181
Marinho SL, Costa A, Palácios M, Rego S. Implementação de comitês de bioética em hospitais universitários brasileiros: dificuldades e viabilidades. Rev. bioét. (Impr.) [Internet]. 2014 [acesso 20 de maio de 2022];22(1):105-15. Disponível: https://bit.ly/3nmEJBk
Oliveira MCG, Oliveira RA, Martins MCFN. A experiência do comitê de bioética de um hospital público. Rev. bioét. (Impr.) [Internet]. 2017 [acesso 20 maio 2022];25(2):338-47. DOI: 10.1590/1983-80422017252194
Organização das Nações Unidas para a Educação, a Ciência e a Cultura. Declaração universal sobre bioética e direitos humanos [Internet]. Brasília: Universidade de Brasília; 2005 [acesso 20 maio 2022]. Disponível: https://bit.ly/3jCZjfQ
Rabadán AT, Tripodoro VA. ¿Cuándo acudir al comité de bioética institucional? El método deliberativo para resolver posibles dilemas. Medicina (B.Aires) [Internet]. 2017 [acesso 20 maio 2022];77(6):486-90. Disponível: https://bit.ly/3Gm9Jdd
Pitskhelauri N. Clinical ethics committees: overview of the european experience. Georgian Med News [Internet]. 2018 [acesso 20 maio 2022];(283):171-5. Disponível: https://bit.ly/3EgmAvP
Berlinguer G. Bioética da prevenção. Bioética [Internet]. 1994 [acesso 20 maio 2022];2(2). Disponível: https://bit.ly/3PXGUJa
Barbosa, S. A participação brasileira na construção da Declaração Universal sobre Bioética e Direitos Humanos da Unesco. Rev Bras Bioét [Internet]. 2006 [acesso 20 maio 2022];2(4):423-36. DOI: 10.26512/rbb.v2i4.8011
Garrafa V. Da bioética de princípios a uma bioética interventiva. Rev. bioét. (Impr.) [Internet]. 2005. [acesso 20 maio 2022]. Disponível: https://bit.ly/3ujI4W1
Notes
Notes
Approval CEP-USF 83309518.0.0000.5514
Conflict of interest declaration
The authors declare no conflict of interest.
Author notes
Daniele Rodrigues – Undergraduate – danieledemoura.rodrigues@gmail.com
Djalma Lessa – Graduate (specialist) – djalma.lessa@usf.edu.br
Denise Gonçalves Priolli – Master – denise.priolli@usf.edu.br
Participation of the authors
Daniele Rodrigues and Denise Gonçalves Priolli conceived the idea of the study; Daniele Rodrigues and Djalma Lessa performed the experiment and collected the data; Denise Gonçalves Priolli supervised and guided the research. All authors discuss the results of this research and contributed to this final draft.
Correspondence: Denise Gonçalves Priolli – Rua São Vicente, 614, Jardim Paulista CEP 12947-390. Atibaia/SP, Brasil.
