REPORTE DE CASO
Pulsatile tinnitus due to vein of Labbé diverticulum and transverse sinus stenosis: a case report
Tinnitus pulsátil por divertículo de la vena de Labbé y estenosis del seno transverso: reporte de caso
 Martiel Manrique-Zegarra
Carlos Toledano-Illán
Juan Brin
María Jesús García-Sánchez
Claudio Rodriguez-Fernández
Martiel Manrique-Zegarra
Carlos Toledano-Illán
Juan Brin
María Jesús García-Sánchez
Claudio Rodriguez-Fernández
Pulsatile tinnitus due to vein of Labbé diverticulum and transverse sinus stenosis: a case report
Revista de Neuro-Psiquiatría, vol. 88, núm. 3, pp. 311-316, 2025
Universidad Peruana Cayetano Heredia
Recepción: 02 Junio 2024
Aprobación: 09 Abril 2025
Abstract: Venous pulsatile tinnitus is an uncommon type of tinnitus caused by cerebral venous vascular etiology such as stenosis or venous thrombosis. We report the case of a 58-year-old male with pulsatile venous tinnitus with persistent symptoms despite symptomatic treatment and without defined etiology. The patient was referred to the interventional neuroradiology unit and underwent an angiography where stenosis in the left transverse sinus at the level of the vein of Labbé drainage was identified, along with a small diverticulum with slow flow. Based on the findings, endovascular stent placement was performed in the left transverse sinus. At the one-month follow-up the patient reported complete resolution of the tinnitus since the procedure was performed. Given that venous pulsatile tinnitus is associated with a decrease in quality of life and sometimes indicative of a serious vascular condition, an accurate diagnostic and therapeutic approach is crucial.
Keywords: tinnitus, interventional radiology, stents, case report.
Resumen: El tinnitus pulsátil venoso es un tipo infrecuente de tinnitus, ocasionado por etiología vascular cerebral venosa como estenosis o trombosis venosa. Se reporta el caso de un adulto varón de 58 años con tinnitus pulsátil venoso con persistencia de síntomas a pesar de tratamiento sintomático y sin etiología definida. Acudió a consulta de neurorradiología intervencionista, se realizó una angiografía donde se identificó una estenosis en el seno transverso izquierdo a nivel del drenaje de la vena de Labbé, en la cual se aprecia un pequeño divertículo con enlentecimiento de flujo. Dado los hallazgos se procedió a colocación endovascular de stent en el seno transverso izquierdo. En el control al mes del procedimiento, el paciente refirió que, desde el día posterior a la intervención, tuvo resolución completa de sintomatología del tinnitus. Es importante el correcto enfoque diagnóstico y terapéutico de estos pacientes, pues esta condición está asociada a una disminución en la calidad de vida y puede ser causada por condiciones vasculares serias.
Palabras clave: acúfeno, radiología intervencional, stents, reportes de casos.
INTRODUCTION
Pulsatile tinnitus represents less than 5% of all tinnitus cases, and manifests as an abnormal perception of a rhythmic sound, which is synchronous with the heartbeat (1).
According to the reviewed literature, the etiology of pulsatile tinnitus can be identified in up to 70 % of cases. Among the main conditions associated with pulsatile tinnitus are structural causes (neoplasms and temporal bone abnormalities), metabolic causes (medications and high cardiac output pathologies) and vascular causes (arterial and/or venous) (2).
The importance of a precise diagnostic and therapeutic approach lies in the fact that this condition is associated with a decrease in the quality of life and can be caused by potential serious vascular conditions (3).
Pulsatile venous tinnitus (PVT) can arise from venous cerebral vascular etiology such as stenosis or venous thrombosis, and unlike the other etiologies, venous causes are usually not recognized in a timely manner (4).
Here we describe an atypical case of an adult patient with a one-year history of PVT treated with endovascular management, accompanied with a review of the literature. This manuscript was prepared following the CARE guidelines for case reports (5) and the patient's authorization was obtained for the preparation of this report.
CASE REPORT
A 58-year-old male with a history of diabetes mellitus and dyslipidemia presented with a one-year history of left tinnitus, which he described as a "rhythmic" sensation that worsened with intense physical activity. He was examined by neurology and otorhinolaryngology units on several occasions, without identifying any apparent etiology and with persistence of symptoms despite symptomatic treatment.
On neurological examination the patient appeared alert, attentive and with adequate language. Muscle strength and sensibility were preserved. Muscle tone and trophism were adequate. Osteotendinous reflexes were normal. No ataxia or dysmetria were identified. Romberg was negative. Pupils were isochoric and normoreactive, confrontation campimetry was normal and there was no ophthalmoparesis nor nystagmus. No paresis or facial sensory alteration were present.
Magnetic resonance image (MRI) of the brain with contrast showed focal ectasia of the vein of Labbé in its retrograde trajectory to the Sylvian fissure with varicose dilatation at the confluence with the left transverse sinus and edema in the adjacent temporal gyri. No signs of acute thrombosis were present (Figure 1).
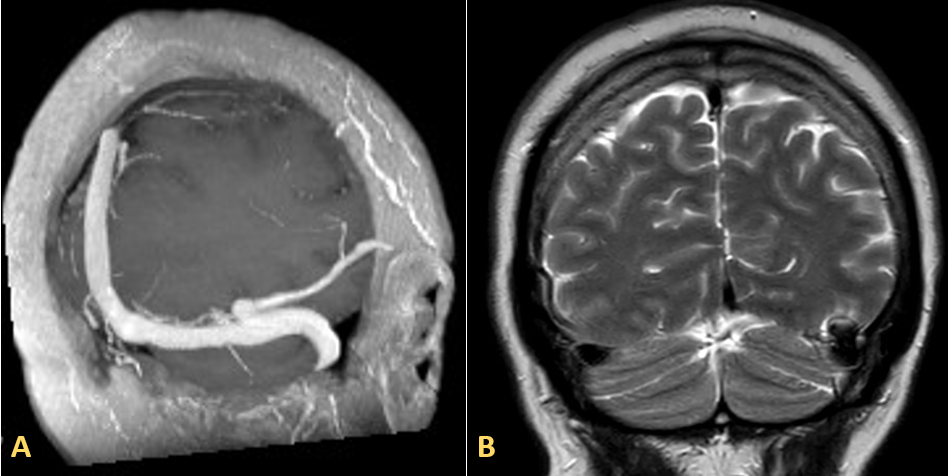
Figure 1.
Magnetic resonance venography. A) Sequence 3D T1: The MIP reconstruction reveals a diverticulum situated at the junction of the vein of Labbé and the left transverse sinus, demonstrating permeability. B) Coronal T2 sequence: Mild hyperintensity in the adjacent temporal gyri.
He was referred to the interventional neuroradiology unit and underwent a diagnostic arteriography that showed stenosis of the left transverse sinus at the level of the vein of Labbé drainage, in which a small diverticulum with slow flow was observed (Figure 2). No evidence of dural or pial arteriovenous fistula, arteriovenous malformation, aneurysms or signs of vasculitis were found. Given the clinical picture and radiological findings, endovascular treatment was scheduled.
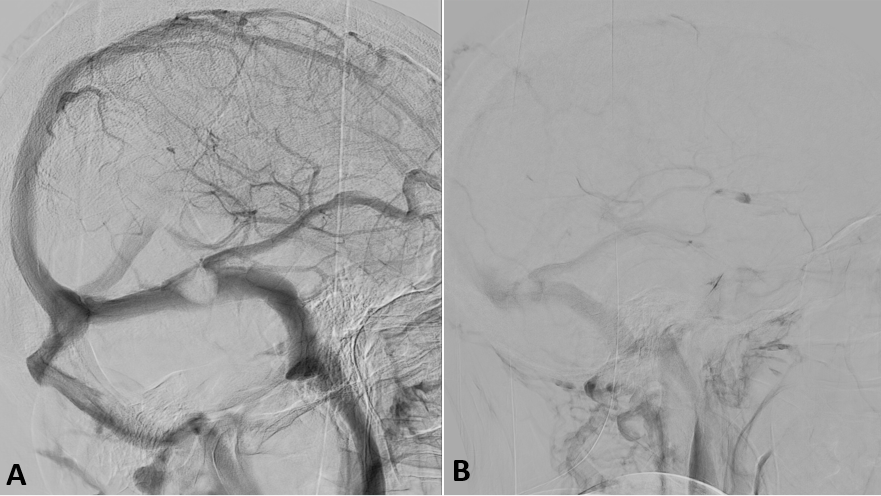
Figure 2.
Cerebral angiography. A) Venous phase where a rounded repletion defect is observed in the left transverse sinus, at the level of the confluence with the vein of Labbé, which causes a significant stenosis. B) Late venous phase showing delayed washout of the vein of Labbé.
A selective venous catheterization with stent placement in the left transverse sinus was planned. Systemic anticoagulation with sodium heparin and antiaggregation with acetylsalicylic acid was administered prior to the procedure, as well as 12 mg of endovenous dexamethasone. After obtaining venous access through the left jugular vein, a guide catheter was placed in the left transverse sinus. Angiographic series and pressure measurements were performed, documenting a gradient pressure greater than 8 mmHg and significant hemodynamic stenosis at the level of the middle third of the left transverse sinus in the region of the vein of Labbé drainage, visualizing a delay in angiographic times at the level of the lateral sinus, vein of Labbé, as well as tributaries and secondary moderate congestion of the deep venous system. A 9x40 mm Wallstent (Boston Scientific, USA) was placed in the left transverse sinus covering the area of stenosis. Improvement of venous drainage resulting in disappearance of contrast retention was observed in the initial series (Figure 3).
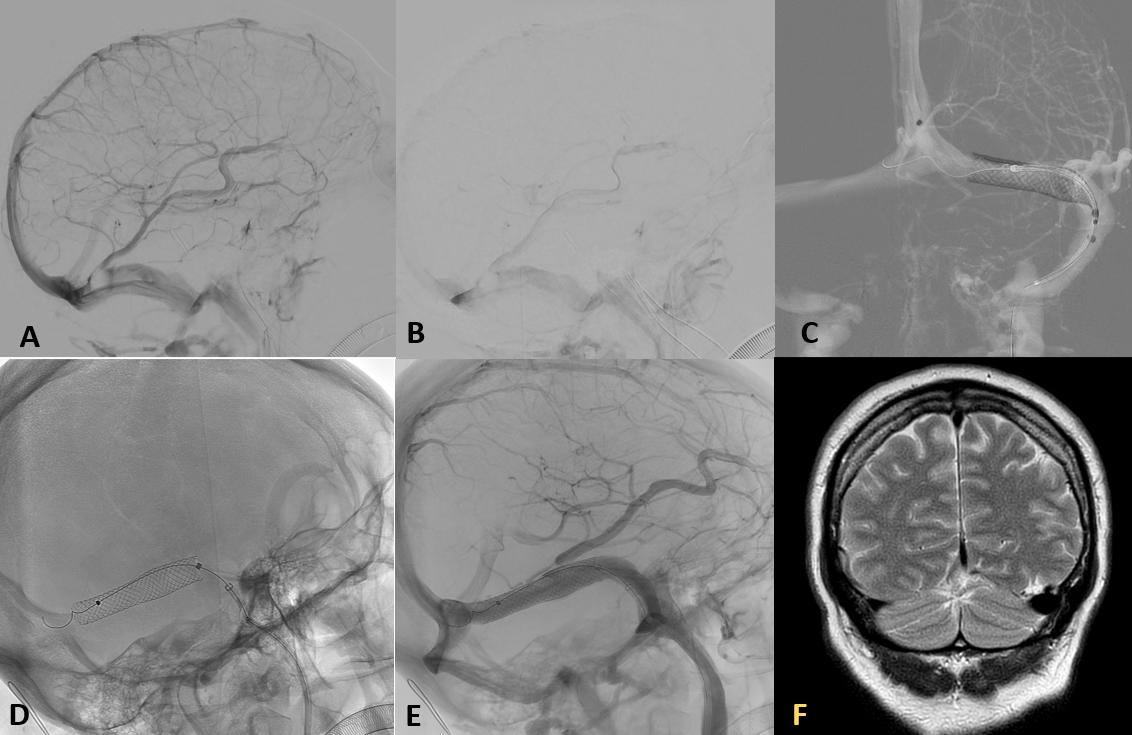
Figure 3.
Cerebral angiography. A, B) Pre-treatment venous phase: persistence of repletion defect in the left transverse sinus and a noticeable delay in contrast lavage with compared to the diagnostic study. C, D) Stent deployment in AP and oblique projections, respectively. E) Venous phase in control series demonstrates adequate stent apposition. F) Control of MRI, coronal T2 sequence, shows permeability of the stent and vein of Labbé, with practical resolution of the diverticulum, without complication signs.
The patient was started on double antiplatelet therapy (acetylsalicylic acid 100 mg and clopidogrel 75 mg) for 3 months and then switched to single antiplatelet therapy (acetylsalicylic acid 100 mg) indefinitely. In the one month follow-up the patient reported complete resolution of the tinnitus since the procedure.
DISCUSSION
High clinical suspicion for a venous cause of pulsatile tinnitus is needed. In most cases it is necessary to perform imaging with specific angiographic study in search of vascular causes. In our patient, PVT was suspected due to the semiological description of rhythmic character that the patient reported. Various clinical maneuvers have been described to guide the clinicians in this suspicion, such as assessing the patient’s pulse and asking him to replicate the sound they hear. Additionally, symptomatic relief upon performing Valsalva maneuver or with the compression of the ipsilateral jugular vein and the increase of tinnitus when compressing the jugular vein on the opposite side to the lesion can help to distinguish a tinnitus of venous cause from one of arterial cause or other non-vascular forms (4).
Tao et al. (3) identified venous stenosis with venous aneurysm or post-stenosis diverticulum as the most common cause of PVT in a cohort of patients evaluated with invasive and non-invasive brain imaging studies, a finding reported in our patient. These authors mention that the high percentage of venous etiology identified in their cohort is probably due to the increased use of contrast-enhanced MR venography (MRV), which is important to highlight, since early detection of venous stenosis can be treated with a stent in the venous sinus and this has already been shown to lead to resolution of symptoms (3, 6). In our case the MRI study evidenced transverse sinus stenosis and a diverticulum in the confluence of vein of Labbé with left transverse sinus, a finding that to our knowledge has not been previously reported in the literature.
Concerning the therapeutic options for PVT, they depend on the etiology involved, and although various surgical options have been described, such as Sinus Resurfacing Surgery, these may be associated with venous thrombosis and neurological complications with poor functional outcomes (7). Increasingly, satisfactory cases of endovascular management of PVT have been reported and it is nowadays considered the first option in cases of PVT associated with sinus wall abnormalities or venous stenosis (8, 9).
Endovascular management options include three main techniques that can be associated in the same procedure: coiling, ballon-assisted coiling and endovascular stenting of the stenosis. Selection of the technique depends on the findings involved. All of them have reported good results, with reports of disappearance of tinnitus or a decrease in its intensity in the long term (9-11).
In cases of diverticulum with a narrow neck, coiling is preferred, whereas if there is a wide neck and/or associated sinus stenosis, balloon-assisted coiling is preferred, leaving stent implantation to those cases where there is isolated sinus stenosis and idiopathic intracranial hypertension. Rare complications such as transient headache, pseudo-aneurysms or retroperitoneal hemorrhage have been reported (9).
In our case, we chose to perform stenting of the left transverse sinus because significant stenosis of the sinus was the most evident finding during the procedure and we theorized that with the hemodynamic correction of this stenosis the wall defect (diverticulum) would be corrected, which indeed occurred in the control series post stent implantation.
Controls after interventional procedures can be performed with noninvasive neuroimaging, leaving digital subtraction angiography (DSA) for cases where there is any suggestive sign of complication or when a second intervention is planned due to persistent symptomatology (12). Computational fluid dynamics has also been proposed as an innovative follow-up technique to detect flow changes after transverse sinus stenting with venous diverticulum. This is based on the known role of turbulent flow in the generation of PVT and the theory that stenosis is responsible for the formation of the associated venous diverticulum (8, 9).
CONCLUSION
We report an atypical case of PVT due to a vein of Labbé diverticulum and stenosis of the left transverse sinus successfully treated with stent implantation, resulting in complete symptom resolution. Given that venous pulsatile tinnitus is associated with a decrease in quality of life and sometimes indicative of a serious vascular condition, an accurate diagnostic and therapeutic approach is crucial.
REFERENCES
1. Hofmann E, Behr R, Neumann-Haefelin T, Schwager K. Pulsatile tinnitus: imaging and differential diagnosis. Dtsch Arztebl Int [Internet]. 2013; 110(26): 451-458. Available from: https://doi.org/10.3238/arztebl.2013.0451
2. Narsinh KH, Hui F, Saloner D, Tu-Chan A, Sharon J, Rauschecker AM, et al. Diagnostic approach to pulsatile tinnitus: a narrative review. JAMA Otolaryngol Head Neck Surg [Internet]. 2022; 148(5): 476-483. Available from: https://doi.org/10.1001/jamaoto.2021.4470
3. Tao AJ, Parikh NS, Patsalides A. The role of noninvasive imaging in the diagnostic workup for pulsatile tinnitus. Neuroradiol J [Internet]. 2022; 35(2): 220-225. Available from: https://doi.org/10.1177/19714009211036696
4. Essibayi MA, Oushy SH, Lanzino G, Brinjikji W. Venous causes of pulsatile tinnitus: Clinical presentation, clinical and radiographic evaluation, pathogenesis, and endovascular treatments: a literature review. Neurosurgery [Internet]. 2021; 89(5): 760-768. Available from: https://doi.org/10.1093/neuros/nyab299
5. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D, et al. The CARE Guidelines: Consensus-based clinical case reporting guideline development. Glob Adv Health Med [Internet]. 2013; 2(5): 38-43. Available from: https://doi.org/10.7453/gahmj.2013.008
6. Patsalides A, Santillan A, Sundararajan SH, Michael M, Suurna M, Alexiades G. Venous sinus stenting for the treatment of isolated pulsatile tinnitus: results of a prospective trial. Interv Neuroradiol [Internet]. 2021; 27(2): 266-274. Available from: https://doi.org/10.1177/1591019920974185
7. Yun J, Cheong TY, Jung K-W, Lee JM. Cerebral venous thrombosis and persistent pulsatile tinnitus after sigmoid sinus resurfacing surgery. Ear Nose Throat J [Internet]. 2024; 103(2): NP72-NP75. Available from: https://doi.org/10.1177/01455613211038269
8. Cuellar H, Maiti T, Patra DP, Savardekar A, Sun H, Nanda A. Endovascular treatment of pulsatile tinnitus by sigmoid sinus aneurysm: technical note and review of the literature. World Neurosurg [Internet]. 2018; 113: 238-243. Available from: https://doi.org/10.1016/j.wneu.2018.02.087
9. Abdalkader M, Nguyen TN, Norbash AM, Raz E, Shapiro M, Lenck S, et al. State of the art: venous causes of pulsatile tinnitus and diagnostic considerations guiding endovascular therapy. Radiology [Internet]. 2021; 300(1): 2-16. Available from: https://doi.org/10.1148/radiol.2021202584
10. Abdalkader M, Ma A, Cohen M, Aliphas A, Sakai O, Nguyen TN. Endovascular coiling of large mastoid emissary vein causing pulsatile tinnitus. Interv Neuroradiol [Internet]. 2020; 26(6): 821-825. Available from: https://doi.org/10.1177/1591019920926333
11. Quintas-Neves M, Freitas E, Amorim JM, Rocha J, Pinho J. Venous sinus stenosis causing isolated pulsatile tinnitus. Can J Neurol Sci [Internet]. 2019; 46(5): 591-592. Available from: https://doi.org/10.1017/cjn.2019.73
12. Fiani B, Kondilis A, Doan T, Runnels J, Fiani NJ, Sarno E. Venous sinus stenting for intractable pulsatile tinnitus: a review of indications and outcomes. Surg Neurol Int [Internet]. 2021; 12: 81. Available from: https://doi.org/10.25259/sni_1_2021
Notes
MMZ, CTI, JB, MJGS, CRF: conceptualization, visualization, writing – original draft preparation, writing – review & editing.
Notas de autor
Corresponding author: Miguel A. Vences, e-mail: miguel.vences@upch.pe
Información adicional
redalyc-journal-id: 3720
Enlace alternativo
https://revistas.upch.edu.pe/index.php/RNP/article/view/5484/6674 (pdf)