Investigación
Efficacy of a resin-modified glass ionomer varnish in the prevention of tooth enamel demineralization around orthodontic brackets: an in vitro study
Eficacia del barniz a base de ionómero de vidrio modificado con resina en la prevención de la desmineralización del esmalte dental alrededor de brackets ortodónticos: un estudio in vitro
Efficacy of a resin-modified glass ionomer varnish in the prevention of tooth enamel demineralization around orthodontic brackets: an in vitro study
Investigación Clínica, vol. 58, no. 4, pp. 365-375, 2017
Universidad del Zulia
Received: 08 August 2016
Accepted: 08 June 2017
Abstract.: The purpose of this work was to evaluate the efficacy, in vitro, of a resin-modified glass ionomer varnish in the prevention of tooth enamel demineralization, around orthodontic metallic brackets. Thirty healthy premolars extracted for orthodontic reasons were selected and they were divided into two groups. In group A, a resin-modified glass ionomer varnish (Clinpro XTTM varnish) was applied on the premolar enamel surface around the metallic brackets; group B was used as a control. Both groups were subjected to 500 cycles in thermal baths, they were submerged under a lactic acid solution; then, methylene blue was applied to identify and observe the demineralization zones under a stereoscopic microscope. A lesser degree of demineralization was observed in group A in comparison to group B. A greater demineralization was observed in the cervical third of both groups, showing a significant difference (p≤0.0001). The use of a resin-modified glass ionomer cement varnish was shown to be effective in preventing demineralization on the enamel surfaces around the metallic brackets, decreasing the penetration of acid substances in vitro on the enamel of the tooth.
Keywords: Demineralization, glass ionomer, fluoride varnish, ClinproTM XT varnish, bracket.
Resumen.: Se evaluó la eficacia in vitro de un barniz a base de un ionómero de vidrio modificado con resina en la prevención de la desmineralización del esmalte dental adyacente al bracket ortodóncico metálico. Se seleccionaron 30 premolares sanos, extraídos por razones ortodónticas y se dividieron en 2 grupos. En el grupo A se aplicó el barniz ionomérico Clinpro™ XT alrededor del bracket metálico y el grupo B se utilizó como control. Ambos grupos se sometieron a 500 ciclos de termociclado, se sumergieron en una solución de ácido láctico y después se aplicó azul de metileno para identificar y observar las zonas de desmineralización al microscopio estereoscópico. Se determinó menor desmineralización en el grupo A en comparación con el grupo B. Fue más evidente la desmineralización en el tercio cervical de ambos grupos, mostrando una diferencia significativa (p≤0.0001). La aplicación de barniz a base de ionómero de vidrio modificado con resina mostró ser efectiva en la prevención de la desmineralización de las zonas adyacentes al bracket metálico disminuyendo la penetración de substancias ácidas in vitro a la superficie del esmalte dental.
Palabras clave: Desmineralización, ionómero de vidrio, barniz fluorado, Clinpro XT, brackets.
INTRODUCTION
The prolonged use of brackets during fixed orthodontic treatment causes retention and accumulation of dental biofilm when the patient’s hygiene is deficient. If the biofilm is not removed properly, it can create demineralization zones on the surface around the cemented brackets; these zones are called white spots (1-5). White spots are defined as the porosity of the tooth enamel’s subsurface demineralized by caries with a white opacity on the smooth surfaces of the tooth. The changes in the dispersion of light by the demineralized enamel make the white spots visible, which rarely become cavities around the brackets and generally do not needrestorative treatment. These lesions become evident around the brackets about a month after their placement, even though the formation of caries usually takes around six months (1,4-6). Carious lesions adjacent to the brackets can be reduced, or even eliminated, with fluoride compounds; however, the use of such compounds depends on the control of each patient, which usually is not the most appropriate (5,6).
Glass ionomer cements have a dental caries-preventive effect because these materials release fluorides, although they have low mechanical resistance. Composites with glass ionomer have been developed with better mechanical properties and still retain the benefit of the fluoride release (6,7). Bishara et al. demonstrated that glass ionomer cements that release fluorides diminish tooth enamel demineralization in fixed orthodontic treatment (8). Other investigations show that the use of modified resins with a glass ionomer can reduce tooth enamel demineralization significantly compared to conventional resins, along with fluorides and calcium phosphate application (9-13). Also, it has been proved that amorphous calcium phosphate inhibits the demineralization in vivo in areas next to the brackets (14,15).
An important highlight is the fact that there is no better treatment against demineralization than the own prevention. Preventive measures that do not depend on an individuals’ compliance have been developed in order to solve the tooth enamel demineralization problem. One of these measures is the combination of dental materials with fluorides releasing properties as an additional source of fluorides near to the brackets (4-6). Such is the case of the ClinproTMXT varnish (3M ESPE) which is a light-cured, durable, fluoride-releasing coating varnish for specific sites of the enamel and dentine, presented in an innovative formulation of a resin-modified glass ionomer. This new technology also contains and releases fluoride, calcium and phosphate. It provides immediate dentinal hypersensitivity relief (16-18) and has a proven remineralization effect (19). The “XT” in the product name is intended to reflect the product’s properties as an “extended varnish”; smooth, soft and virtually invisible, having long-term durability with fluoride release (remains on the tooth for six months or longer according to the manufacturer). It’s virtually invisible making it ideal for protecting tooth surfaces around orthodontic brackets and non-cavitated caries lesions (5,6,16-19).The purpose of this study was to evaluate the efficacy in vitro of the ClinproTM XT varnish as a tooth enamel demineralization preventive agent around the metallic brackets.
MATERIALS AND METHODS
This in vitro study was approved by the Ethics Committee of the Faculty of Dentistry, University of San Luis Potosi, Mexico (approved protocol number: CEI-FE-032-014). Thirty healthy human premolars were used. Teeth were extracted for orthodontic indications and were inspected clinically by transillumination, and microscopically to ensure that they were free of defects on all surfaces. In addition, the teeth were analyzed carefully by laser fluorescence (DIAGNOdent pen 2190, Biberach, Germany) on the buccal dry surface with the tip of the DIAGNOdent held in contact with the tooth surface and tilted around the measuring site so that fluorescence would be collected from all directions. The measurements of the teeth included in this study were in a score from one to five, which indicates “no demineralization” according to the manufacturer (20). Teeth were disinfected in 0.5% chloramine-T for a week and stored in distilled water at 4°C. They were randomly divided into two different groups, Group A (15 premolars) had a metallic bracket placed and the ClinproTMXT varnish (3M ESPE) was applied around it on the adjacent tooth enamel. Group B (15 premolars) was used as a control group, just a metallic bracket was placed and nothing was applied around this group.
First, a prophylaxis was performed to clean the buccal surface with non-fluoride oil-free pumice paste (Prophy Tech by Zeico, Jalisco, Mexico) using a nylon brush attached to a low-speed hand piece for 10 s. The surface was rinsed with water and dried with an oil-free air spray; brackets (3G SCAPE by Ah-Kim-Pech, D.F., Mexico) were bonded to the teeth with the direct technique using TransbondTM XT light cure adhesive system (3M Unitek, CA, USA). Etching with 37% phosphoric acid gel for 20 s over the entire buccal surface was done. A layer or TransbondTM XT primer was applied to the tooth and bracket mesh and the bracket was bonded according to the manufacturers’ instructions. Careful removal of excess material was performed and light curing was applied for 60 s (15 s from cervical, incisal, mesial and distal directions). Only in Group A specimens, a thin layer (0.5 mm or less) of Clinpro™ XT varnish was applied (previously mixed the liquid and the paste on the mixing pad).varnish was placed whit a micro-brush on the entire buccal surface around the metallic bracket and light cured for 20 s according to the manufacturer (Fig.1). After this process, the teeth were stored for 24 hours in artificial saliva (Salivart by Fineman, Cleveland OH, USA) at 37 °C. Later, all specimens were submitted to a thermal cycling process, which consisted in submerging the dental organs in thermal baths filled with distilled water at three different temperatures for five hundred cycles. The temperatures were 55°C, 5°C and 37°C, the duration of each bath was 30 seconds plus 10 seconds for transporting. Then, all of the samples were submerged in a demineralizing solution (20% lactic acid solution in a deionized water, pH= 2.74) for 72 uninterrupted hours in the same solution. They were drawn out of the solution and they were rinsed with distilled water. Every sample was coated with two layers of nail polish (ORLY™, California., USA) on all tooth surfaces, except on the buccal surface where the bracket was placed. After that, the brackets were removed from both groups by using a bracket removing plier and the apical part of the root was sealed with wax to prevent the colorant to penetrate through the apex. The samples were then submerged into amber colored glass containers with 10% methylene blue (MerckTM, Damstadt, Germany) for 24 hours and they were rinsed with distilled water, letting them dry for 12 hours. A longitudinal cut was performed in every sample using a cutter (Isomet Low Speed Saw™ by Buehler, Illinois, USA) with a diamond disc. The samples were rinsed in distilled water to eliminate residues, allowing them to dry for 12 hours in order to be observed under a stereoscopic microscope (Leica EZ4HD, Singapore, Singapore). The obtained images were analyzed with the software LAS EZ 3.0.0 (Switzerland); the standard zoom for every picture was 8.5x.
Every sample was measured three times for each of three different observers at an interval of two weeks. The observer was previously calibrated with 10 samples and a kappa concordance index was established (95%). The measurements were made based on the images obtained from the stereoscopic microscope, restricting the measurements to three zones regarding the bracket’s placement on the tooth: a) 2 mm of the occlusal third, b) on the medial third (where the bracket was placed) and c) 2 mm of the cervical third. The scale used to measure the depth of penetration (demineralization) is explained as follows: 0. - Represents no penetration of methylene blue. 1. - Represents a penetration of methylene blue of 1/3 of the enamel’s width (from the enamel surface to the dentin). 2. - Represents a penetration of methylene blue of 2/3 of the enamel’s width (from the enamel surface to the dentin).3. - Represents a penetration of methylene blue of 3/3 of the enamel’s width (the entire thickness of the enamel) (Fig. 2). The data was submitted to the data collection form, it was then analyzed using the software Minitab version 17(Pennsylvania, USA).
Fig.1.
Procedure a) Cemented bracket with the direct technique. b) Application of glass ionomer varnish.
Fig.2.
Zones assessed on the buccal aspect of the dental organ: a. occlusal third, b. medial third and c. cervical third. The depth of penetration was evaluated by thirds of the enamel thickness (1/3, 2/3 and 3/3).
RESULTS
By analyzing all the samples (30 premolars) under the stereoscopic microscope, the penetration of methylene blue was obtained (demineralization) for every third of the buccal surface of the studied teeth. The score of penetration of every sample can be observed in Table I.
A score of penetration of 0 and 1 prevailed among the 15 premolars from Group A (penetrations 2 and 3 were less frequent), which means they presented a tooth enamel demineralization of 1/3 maximum (from the enamel surface to the dentin). By comparing Groups A and B, it can be seen that the group that had the greater protection against the demineralization was group A, with 69%; unlike group B who presented a protection of 26.6% (Table II).
A higher penetration of methylene blue (therefore, a greater demineralization) was observed in the dental organs untreated with the ClinproTM XT varnish compared to the group where it was applied (Fig. 3). By comparing the thirds in every zone of the buccal surface, a greater percentage of demineralization was found in the cervical third of the crown. A Student’s t test was performed to find the mean and standard deviation of the measurements performed in the occlusal third, the middle third and the cervical third in each tooth. A higher significance was observed in the cervical third p≤0.0001 compared to the middle third p≤0.05 and the occlusal third p≤0.03(Table III, Fig. 4 and 5).
DISCUSSION
The prevention of tooth enamel demineralization during fixed orthodontic treatment is one of the biggest challenges that professionals have to face despite all the existing technological advances to inhibit the development of dental caries. In the last few years numerous investigations about this subject have been conducted and demonstrate that glass ionomer cements diminish tooth enamel demineralization in orthodontic treatments (8). Other investigations showed that the use of resins modified with a glass ionomer could reduce tooth enamel demineralization significantly compared to conventional resins. If these resins are used along with a frequent application of fluorides and calcium phosphates, the reduction of the tooth enamel demineralization can become even greater (9.10).
| Group A | Group B | ||||||
| Third | |||||||
| SAMPLE | Occlusal | Medial | Cervical | SAMPLE | Occlusal | Medial | Cervical |
| 1 | 1 | 0 | 1 | 16 | 1 | 0 | 0 |
| 2 | 1 | 3 | 0 | 17 | 1 | 0 | 3 |
| 3 | 0 | 0 | 1 | 18 | 3 | 3 | 3 |
| 4 | 0 | 0 | 0 | 19 | 1 | 0 | 3 |
| 5 | 3 | 0 | 1 | 20 | 1 | 0 | 3 |
| 6 | 0 | 0 | 0 | 21 | 1 | 0 | 3 |
| 7 | 0 | 0 | 0 | 22 | 2 | 3 | 3 |
| 8 | 1 | 0 | 0 | 23 | 2 | 0 | 3 |
| 9 | 1 | 0 | 1 | 24 | 1 | 1 | 1 |
| 10 | 1 | 0 | 0 | 25 | 1 | 1 | 3 |
| 11 | 1 | 0 | 0 | 26 | 2 | 0 | 3 |
| 12 | 0 | 0 | 0 | 27 | 2 | 0 | 0 |
| 13 | 1 | 0 | 0 | 28 | 1 | 3 | 3 |
| 14 | 0 | 0 | 0 | 29 | 1 | 0 | 2 |
| 15 | 0 | 0 | 3 | 30 | 1 | 0 | 0 |
| Scale | 0 | 1 | 2 | 3 |
| Group A | 69.00% | 24.40% | 0.00% | 6.60% |
| Group B | 26.60% | 31.10% | 8.88% | 33.33% |
In this in vitro study, it was proven that aresin-modified glass ionomer cement varnish (ClinproTM XT varnish) is effective as a demineralization-preventive agent on the tooth enamel’s surface adjacent to the metallic brackets. The group of premolars in which the varnish was applied presented a better protection against the penetration of methylene blue (demineralization) obtaining a score of zero penetration (no impact on the enamel’s superficial structure) in 69% of the samples. That was not the case in the control group, where only 26.6% of the cases presented a score of 0. It was observed that in both groups, the portion of the surface that suffered the highest penetration was in the cervical third (Group A with 6.6% and Group B with 66.6%). This can be due to the fact of the dental organs studied, were previously in the oral cavity, where the cervical segment is more likely to suffer demineralization because of the accumulation of dental biofilm in this specific zone. Furthermore, this section has the thinnest enamel of the analyzed thirds; this can contribute to the fact that a score of three (the whole width of the enamel) were observed in the cervical third. Tooth enamel sealants have proven to be effective in reducing the depth of demineralization injuries, suppressing them in up to 97% (21), probably because it acts as a physical barrier that doesn’t allow the accumulation of food remains and microorganisms applied. In like manner, we presume that the ClinproTM XT varnish acted mainly as a physical barrier that prevented the direct contact of the acid substance used on the samples. Consequently, a lesser demineralization was observed on the surfaces adjacent to the metallic bracket where the varnish was applied.
Fig.3.
a) Penetration of methylene blue in occlusal third in a representative sample of Group A. b) Penetration of methylene blue in occlusal third in a representative sample of Group B. c) Penetration of methylene blue in medial third in a representative sample of Group A. d) Penetration of methylene blue in medial third in a representative sample of Group B. e) Penetration of methylene blue in cervical third in a representative sample of Group A.f) Penetration of methylene blue in cervical third in a representative sample of Group B. All samples were randomly selected.
Glass ionomer materials should be capable of releasing, absorbing and re-releasing fluor over a long period in order to be effective in caries inhibition and this allows too for a continuous contribution of this element to the demineralized surfaces; remineralizing the surfaces with calcium and phosphate (18). In the presence of fermentable carbohydrates, tooth enamel demineralization around the brackets can appear in approximately in four weeks (6,22). By contrast, tooth enamel remineralization can be quantified within the first three-six weeks, it then progresses slowly and constantly after 12 weeks (23). This is why we think that the fluorides release from the varnish did not play an important role in the demineralization process in this study; consequently, it could not have affected the results. As it was mentioned, fluorides are liberated in a slow and continuous motion on a period of six months (according to the manufacturer); this, along with the fact that the study was conducted for a short period of time, and there was no bioavailability of calcium and phosphate (as in an oral cavity), did not allow the remineralization process to be carried out. We propose to make subsequent studies, where we can measure the time of fluoride release as well as the quantity of fluorides released by the ClinproTMXT varnish.
| Group A | Group B | ||
| Occlusal third | Mean SD p value | 0.66 ±0.8 ≤0.03 | 1.26 ±0.7 |
| Medial third | Mean SD p value | 0.20 ±0.77 ≤0.05 | 0.46 ±0.83 |
| Cervical third | Mean SD p value | 0.93 ±1.33 ≤0.0001 | 2.26 ±1.16 |
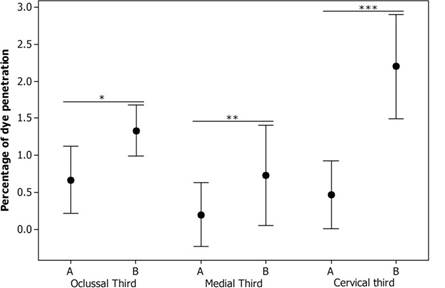
Fig.4.
Percentage of methylene blue dye penetration into the enamel by thirds in Group A (A) and Group B (B).
*p≤0.03, **p≤0.05, ***p≤0.0001
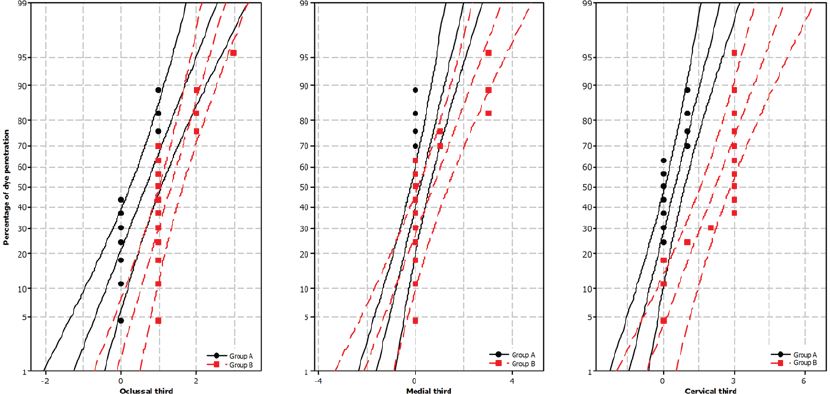
Fig.5.
Probability of methylene blue dye penetration into the enamel by thirds in Group A and Group B. It shows the distribution of the data by thirds in Group A and Group B.
Kumar Jena et al. (6) performed a split mouth study to evaluate the efficacy of resin-modified glass ionomer cement varnish in the prevention of white spot lesions during early orthodontic treatment with fixed appliances. White spot lesions were evaluated by DIAGNOdent and direct visual inspection after six months of varnish application. They concluded that the use of ClinproTM XT varnish had a modest beneficial effect in the prevention of white spot lesions. We agree with the authors because we also demonstrated that ClinproTM XT varnish showed to be an effective fluoride product to diminish the demineralization in vitro.
Even though nowadays there are a wide variety of fluoride products with an advanced technology, it is important to emphasize that there is no better treatment than prevention. For this purpose, preventive measures that do not depend on patient cooperation are the best choice; therefore, we recommend that the professional perform an application of the resin-modified glass ionomer varnish in those patients who can be classified as high risk for caries because they do not carry out regular oral hygiene. This varnish is effective in preventing and reducing demineralization, as well as remineralizing existing lesions.
Within the limitations of this in vitro study, the use of a resin-modified glass ionomer varnish was shown to be effective in preventing demineralization on the enamel surfaces around the metallic brackets, decreasing the penetration of acid substances in vitro on the surface of the tooth. ClinproTM XT varnish could be an effective alternative as a demineralization preventive agent on the tooth enamel during orthodontic fixed appliances treatments because it avoids, in a high percentage, demineralization around the brackets.
ACKNOWLEDGEMENT
To the clinic of Orthodontics and Dentomaxilofacial Orthopedics of the Autonomous University of San Luis Potosi for the equipment and installations to perform this research.
REFERENCES
1. Tufekci E, Dixon JS, Gunsolley JC, Lindauer SJ. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod 2011; 81:206-210.
2. Attin R, Stawarczyk B, Keçik D, Knösel M, Wiechmann D, Attin T. Shear bond strength of brackets to demineralize enamel after different pretreatment methods. Angle Orthod 2012; 82(1):56-61.
3. Naidua E, Stawarczykb B, Tawakolic PN, Attind R, Attine T, Wiegandf A. Shear bond strength of orthodontic resins after caries infiltrant reconditioning. Angle Orthod 2013;83:306-312.
4. Maxfield BJ, Hamdan AM, Tufekc¸i E, Shroff B, Best AM, Lindauer SJ. Development of white spot lesions during orthodontic treatment: perceptions of patients, parents, orthodontists, and general dentists. Am J Orthod Dentofacial Orthop 2012;141:337-344.
5. Montasser MA, Taha M. Effect of enamel protective agents on shear bond strength of orthodontic brackets. Prog Orthod 2014;18;15:34.
6. Kumar Jena A, Pal Singh S, Kumar Utreja A. Efficacy of resin-modified glass ionomer cement varnish in the prevention of white spot lesions during comprehensive orthodontic treatment: a split-mouth study. J Orthod 2015;42(3):200-207.
7. Da Silva Fidalgo TK, Pithon MM, do Santos RL, de Alencar NA, Abrahão AC, Maia LC. Influence of topical fluorides application on mechanical properties of orthodontic bonding materials under ph cycling. Angle Orthod 2012;82:1071-1077.
8. Bisharaa SE, Solimanb M, Laffoonc JF, Warrend J. Shear bond strength of a new high fluorides release glass ionomer adhesive. Angle Orthod 2008;78:125-128.
9. Sudjalim TR, Woods MG, Manton DJ, Reynolds Victoria EC. Prevention of demineralization around orthodontic brackets in vitro. Am J Orthod Dentofacial Orthop 2007;131:705.
10. Manfreda L, Covellb DA, Crowec JJ, Tufekcid E, Mitchelle JC. A novel biomimetic orthodontic bonding agent helps prevent white spot lesions adjacent to brackets. Angle Orthod 2013;83: 97-103.
11. Brown ML, Davis HB, Tufekci E, Crowe JJ, Covell DA, Mitchell JC. Ion release from a novel orthodontic resin bonding agent for the reduction and/or prevention of white spot lesions. An in vitro study. Angle Orthod 2011;81: 1014-1020.
12. Derks A, Katsaros C, Frencken JE, van’t Hof MA, KuipersJagtman AM. Caries-inhibiting effect of preventive measures during orthodontic treatment with fixed appliances. A systematic review. Caries Res 2004; 38:413-420.
13. Robertson MA, Kau CH, English JD, Lee RP, Powers J, Nguyen JT. MI Paste Plus to prevent demineralization in orthodontic patients: a prospective randomized controlled trial. Am J Orthod Dentofacial Orthop 2011;140:660-668.
14. Tuysal, Amasyali M, Ozcan S, Koyuturk AE, Akyol M, Sagdic D. In vivo effects of amorphous calcium phosphate-containing orthodontic composite on enamel demineralization around orthodontic brackets. Aust Dent J 2010;55:285-291.
15. Shimazu K, Ogata K, Karibe H. Evaluation of the caries-preventive effect of three orthodontic band cements in terms of fluorides release, retentiveness, and microleakage. Dent Mater J 2013;32:376-380.
16. Lee SH, Lee NY, Lee IH. Clinical evaluation of the efficacy of fluoride adhesive tape (F-PVA) in reducing dentin hypersensitivity. Am J Dent 2013;26(3):143-148.
17. Ding YJ, Yao H, Wang GH, Song H. A randomized double-blind placebo-controlled study of the efficacy of Clinpro XT varnish and Gluma dentin desensitizer on dentin hypersensitivity. Am J Dent 2014;27(2):79-83.
18. Sohn S, Yi K, Son HH, Chang J. Caries-preventive activity of fluoride-containing resin-based desensitizers. Oper Dent 2012;37(3):306-315.
19. Zhou SL, Zhou J, Watanabe S, Watanabe K, Wen LY, Xuan K. In vitro study of the effects of fluoride-releasing dental materials on remineralization in an enamel erosion model. J Dent 2012;40(3):255-263.
20. Castilho LS, Cotta FV, Bueno AC, Moreira AN, Ferreira EF, Magalhães CS. Validation of DIAGNOdent laser fluorescence and the International Caries Detection and Assessment System (ICDAS) in diagnosis of occlusal caries in permanent teeth: an in vivo study. Eur J Oral Sci 2016;124(2):188-194.
21. Loucks Buren J, Staley RN, Wefel J, Qiand F. Inhibition of enamel demineralization by an enamel sealant, pro seal: an in-vitro study. Am J Orthod Dentofacial Orthop 2008;133:88-94.
22. Benhama AW, Campbell PM, Buschang PH. Effectiveness of pit and fissure sealants in reducing white spot lesions during orthodontic treatment. Angle Orthod 2009;79:337-344.
23. Wua G, Liub X, Houc Y. Analysis of the effect of CPP-ACP tooth mousse on enamel remineralization by circularly polarized images. Angle Orthod 2010;80:933-938.
Author notes
Corresponding author: Jairo Mariel Cárdenas. Orthodontics Postgraduate Program, Faculty of Dentistry, University of San Luis Potosi, Mexico. Av. Dr. Manuel Nava 2, Zona Universitaria, Zip Code 78290; San Luis Potosí, S.L.P., México. Phone: 52 (444) 826 23 57 ext.5122. Fax: 52 (444) 826 23 57. Email: llairo@hotmail.com.