Abstract: Evidence shows that migratory processes alter the dynamics of infectious diseases, thus representing a challenge to public health in both a do mestic and international scale. After the arrival of a group of 122 African medi cal asymptomatic students to Venezuela for an educational exchange program, screening for eight parasitic diseases was done. The aim was to determine the presence of these diseases using standard parasitological tests, ELISA, immu nochromatographic rapid test and MABA (Multiple Antigen Blot Assay). Six patients were found to have been carrying an active schistosomiasis and one was infected with Plasmodium falciparum. When using ELISA as the standard reference test, a total of 13 individuals were seropositive for toxoplasmosis, seven for amoebiasis, three for hydatidosis and two for cysticercosis. No pa tients exhibited seropositivity for trypanosomiasis and fascioliasis according to ELISA. The introduction of infected individuals to the country might represent a threat to public health, which raises the need to establish screening protocols for asymptomatic people who intend to stay in Venezuela. In the frame of these results, recommendations regarding an appropriate evaluation for immigrants are discussed.
Keywords: migrationmigration,parasitesparasites,screeningscreening.
Resumen: Hay evidencia que demuestra que los procesos migratorios alte ran la dinámica de las enfermedades infecciosas, representando un reto para la salud pública en una escala local e internacional. Tras la llegada de un grupo de 122 estudiantes africanos asintomáticos a Venezuela para un programa de in tercambio académico, se realizó un tamizaje de 8 enfermedades parasitarias. Se planteó determinar la presencia de estas enfermedades, a través del uso de mé todos parasitológicos, ELISA, pruebas rápidas inmunocromatográficas y MABA (Multiple Antigen Blot Assay). Seis estudiantes resultaron positivos para una es quistosomiasis activa y 1 se encontraba infectado con Plasmodium falciparum. Usando ELISA como la prueba de referencia estándar, un total de 13 individuos fueron seropositivos para toxoplasmosis, 7 para amebiasis, 3 para hidatidosis y 2 para cisticercosis. Ninguno presentó seropositividad para tripanosomiasis y fas cioliasis, según ELISA. La introducción de individuos infectados al país pudiera representar una amenaza para la salud pública, por lo que surge la necesidad de realizar protocolos de tamizaje para poblaciones asintomáticas con planes de permanecer en Venezuela. En el marco de estos resultados, se realizan recomen daciones con respecto a la evaluación integral para inmigrantes.
Palabras clave: migración, parásitos, pesquisa.
Original articles
Parasitic diseases in African students: how international exchange programs could affect public health
Enfermedades parasitarias en estudiantes africanos:cómo programas de intercambio internacional podrían afectar la salud pública
Universidad del Zulia
Received: 27 October 2017
Accepted: 05 April 2018
According to the United Nations (UN), in 2015 the number of international mi grants across the world reached an estimated number of 244 million. The movement of people from one place to another pursuing lifestyle changes due to poverty, political conflicts, natural disasters, among other reasons, represents a challenge to public health (1). However, tourism is the most numerous migration process, as the Inter national World Tourism Organization has estimated that in 2006, 842 million tourists traveled worldwide (2). Unlike migratory processes for other reasons, this human flow is usually shortlived and is mostly done by middle and highincome people from developed countries, usually with good health and low risk of transmitting diseases except those transmissible from person to person (sexually transmitted diseases, influenza, etc). Evidence suggests that the movement of people alters the epidemiology of Infectious Diseases (IDs), thus, infectious agents may be introduced into places with optimal conditions for a determined illness to be spread (3).
Mobile population travel either alone or in groups, as migrants, refugees, missionaries, international students, temporary work ers, airline personnel, etc. (4). A greater challenge is presented when migrants travel as asymptomatic carriers, meaning they have a silent infection, yet are capable of trans mitting the disease, thus, being a threat to public health (e.g. tuberculosis and HIV). Moreover, certain features of the migrant and host population may shape the dynamic of how IDs are transmitted, including socio economic, cultural, genetic, biological and behavioral conditions (5). All of these fac tors need to be taken into account when ef fective migration health policies are to be implemented.
The reduction of the globalization of IDs implies legislative and pragmatic efforts. Venezuela’s current legislation prohibits in fected migrants that could threaten public health to enter the country (6), yet current screening systems are not sufficiently strong and require more work. Screening protocols aimed at early detection in migrants who come from or arrive at endemic regions are highly encouraged, not only for those diseas es that can be transmitted at their arrival, but also for those that can be acquired dur ing their stay.
The present study was performed on a group of African medical students who came to Venezuela in a sixyear education exchange program. It attempts to highlight the importance of an infected mobile population as a relevant risk factor for parasite dissemination, and to recommend the improvement of migration health policies through screening protocols.
The study group was composed of 122 African medical students between the ages of 19 to 27, 83 males and 37 females. Gen der was not specified in the clinical history for two of the students. All individuals at tended the basic courses at the “Escuela Latinoamericana de Medicina: Salvador Allende” near Caracas, Venezuela. Later on, this group of students was distributed throughout different health centers across the country, making it difficult to follow up. The distribution of students according to their country of origin is represented in Fig. 1.
This is an observational, descriptive, crosssectional study, approved by the Ethical Committee of the Tropical Medicine Institute of the Faculty of Medicine of the Central University of Venezuela. An informed consent and a questionnaire containing epidemiological background inquiries was applied to the studied population to determine their past medical history, housing conditions and epidemiologic data, including re cent visits to caves and contact with waters of rivers and lakes in their countries.
The study population was screened for eight parasitic diseases (malaria, amoebiasis, trypanosomiasis, cysticercosis, fascioliasis, hydatidosis, schistosomiasis and toxoplasmosis) using multiple techniques depending on the disease to be studied, which will be described below.
Capillary and peripheral venous blood samples were collected from the total population to perform diagnostic tests in November 2012. The former were used for the thick and thin blood smears (TTS) to screen for hemoparasites and a rapid diagnostic test to screen for malaria. Venous blood samples were collected to use the sera for the immunological tests.
All diseases were screened using Multiple Antigen Blot Assay (MABA) except for malaria. Subjects that resulted positive for amoebiasis, trypanosomiasis, cysticercosis, fascioliasis, hydatidosis, and/ or toxoplasmosis, were tested with Enzymelinked Im munoabsorbent Assay (ELISA) as a confirmatory test. Recognizing the importance of schistosomiasis as the second most common parasitic disease in African countries (7), all subjects were screened for this disease with SMPELISA. Those who resulted positive were tested with Circumoval Precipitin Test (COPT) for confirmation.
Malaria was the only disease that was not evaluated by serology. Since malaria is endemic in almost all African countries, most populations maintain high levels of antibodies without diagnostic value for current infections. Therefore, this group was only evaluated by the thick and thin blood smear (TTS) stained with Giemsa and by a rapid diagnostic test that detects Pf/Pv antigens (OptiMALIT®).
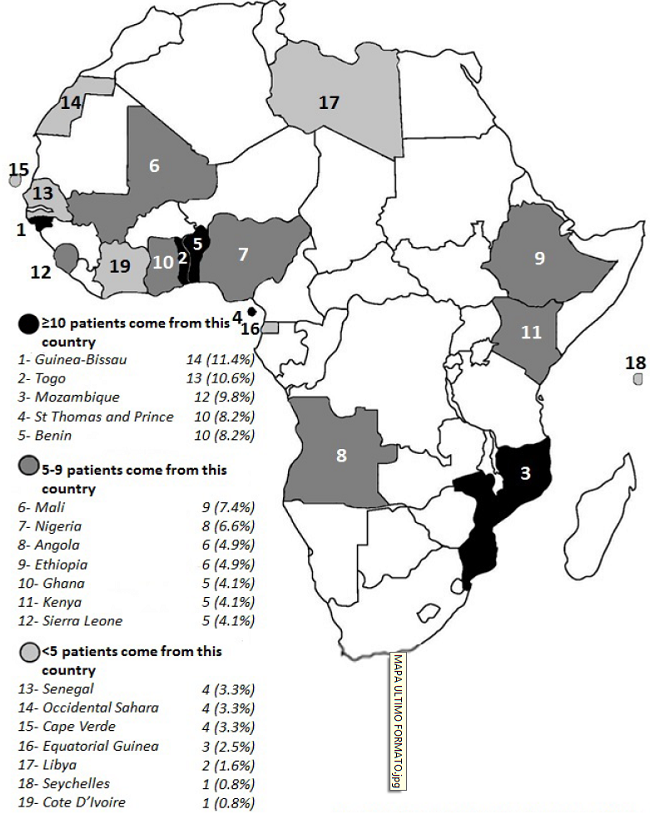
Fig. 1
Number of individuals according to their country of origin in Africa.
MABA is a versatile and inexpensive method that permits the simultaneous detection of antibodies to multiple antigens in a single assay. This technique was accomplished according to Noya & Alarcón de Noya, with an adjustment called “CrossMABA”, where multiple antigens are immobilized in a nitrocellulose sheet using a Miniblotter® acrylic device with parallel channels. After blocking, the nitrocellulose sheet is rotated in a way that makes the channels of the Mini blotter® perpendicular to the previously antigen sensitized rows, instead of cutting the paper in strips (8).
All serum samples were tested against the available crude antigens from different local parasite agents. Those were: Entamoeba histolytica (15 µg/mL), Trypanosoma cruzi (20 µg/mL), Cysticercus cellulosae (15 µg/mL), Fasciola hepatica (8 µg/mL), Echi nococcus granulosus (20 µg/mL) and Toxo plasma gondii (30 µg/mL). For Schistosoma mansoni three antigens were used: adult worm soluble antigen (20 µg/mL), soluble egg antigen (15 µg/mL) and the synthetic peptide IMT180/1086 (9) derived from Sm31 cathepsin B protein from S. mansoni (30 µg/mL). A positive response appears as a black spot, after using a peroxidase con jugate and chemiluminescent substrate. An example can be seen in Fig. 2.
All samples that tested positive for am oebiasis, Chagas’ disease, cysticercosis, fas cioliasis and hydatidosis using MABA, were confirmed with ELISA as the standard refer ence test (10). ELISA was made in the IMT using antigens manufactured by laboratories of the Institute. Furthermore, all patients who tested positive for toxoplasmosis us ing MABA were confirmed by Avidity ELISA (11). In the case of schistosomiasis, all se rum samples were tested, regardless of their MABA result, using the ELISA variant proto col known as sodium metaperiodate ELISA (SMPELISA) (12).
Those subjects with positive SMPELISA were tested by COPT to determine if they had an active S. mansoni infection. Fresh S. mansoni eggs incubated with serum of each patient were used as antigens, showing an tibody reactions as refractive bubbles and chains in more than 10% of the eggs in those positive and active cases (13).
All blood samples were examined through optical microscopy by TTS stained with Giemsa to look for any hemoparasites, particularly malaria and circulating trypano somes. For malaria, the parasite load was calculated as follows (14):
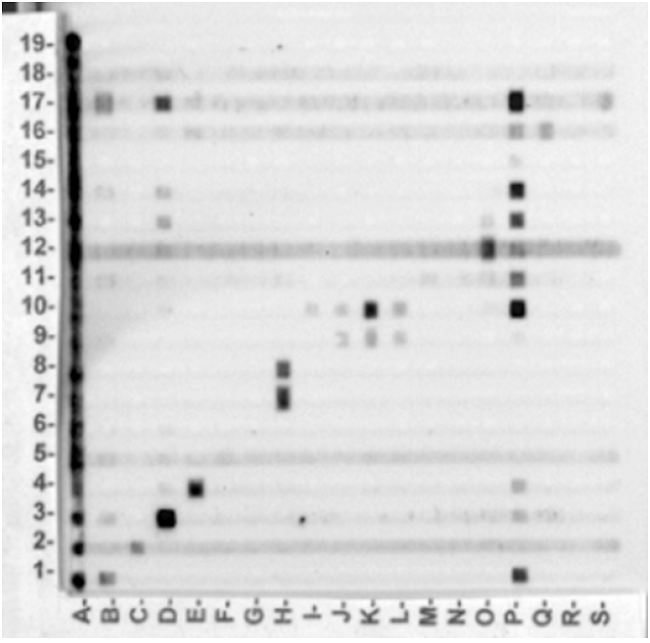
Fig. 2
Representative “CrossMABA” of this stu dy. Numbers from 1 to 19 correspond each to specific antigens for different diseases. Letters from A to S correspond to patients sera.
OptiMALIT® of P. falciparum and non P. falciparum infection (Diamed AG, 1785 Cressier S/Morat, Switzerland) test (Flow, Inc, Portland, OR, USA)(15) was carried out to detect Pf/Pv malaria antigens.
Statistical analysis was performed using the platform R version 3.4.3. The statistical package “exact 2×2” by Fay MP (16) was used to compute McNemar’s exact test estimates and its significance values. Hypothesis tests were performed using a predetermined alpha level of 0.05 and 95% confidence intervals were constructed where appropriate. In order to compare the results be tween MABA and SMPELISA, the proportion of positive results was calculated for each as say. McNemar’s test was used to evaluate the association between a positive SMPELISA and a positive MABA. The exact modification of the original McNemar’s test was used to calculate the odds of a positive MABA given a positive SMPELISA. Results are reported as odds ratio (OR).
The laboratory results of the 122 asymp tomatic African medical students evaluated by six different techniques against eight dif ferent parasitic diseases are summarized in Table I. The number of positive individuals corroborated by the confirmatory tests ac cording to their country of origin are shown in Fig.3. Different levels of sensitivity were ob served with three immunoenzymatic assays.
Schistosomiasis: 9.84% of the studied population had seropositivity for schistosomiasis by MABA, whereas 63.93% resulted positive by SMPELISA. Positive SMPELISA samples were confirmed using the COPT, in which 7.69% were proven to carry an active schistosomiasis infection. This number rep resents 4.92% of the total population (five were male and one female) all with ages be tween 20 and 26 years old. These individuals came from Nigeria (2), Sierra Leone (2), Mozambique (1) and Angola (1). These patients had mediumtohigh optical density in SMPELISA. In the epidemiological questionnaire, patients were asked about contact with water in rivers or lakes. Twentyeight patients (22.95%) out of the 78 (63.93%) that were positive using SMPELISA claimed to have had contact. When comparing MABA to SMPELISA, the McNemar’s test reported a p value <0.001 and OR: 23.0 (CI95 7.54114.25).
LABORATORY RESULTS OF 122 AFRICAN MEDICAL STUDENTS EVALUATED FOR EIGHT DIFFERENT PARASITIC DISEASES
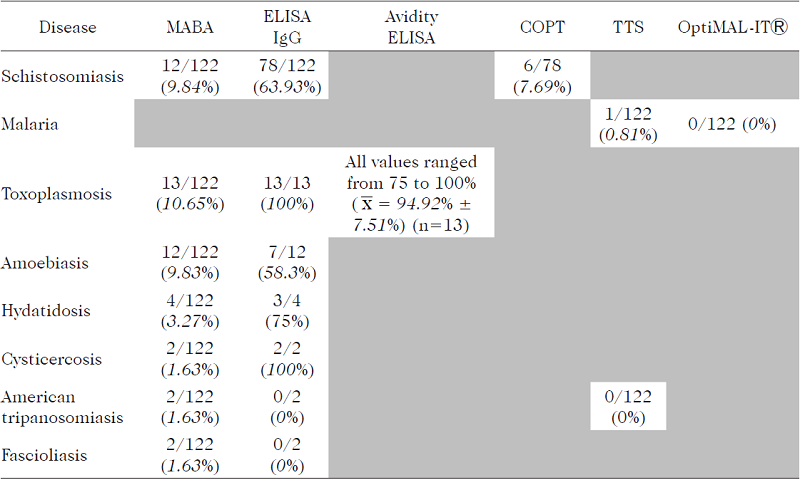
MABA: Multiple Antigen Blot Assay. ELISA: Enzymelinked Immunoabsorbent Assay. COPT: Circumoval Precipi tin Test. TTS: Thick and thin blood smear.
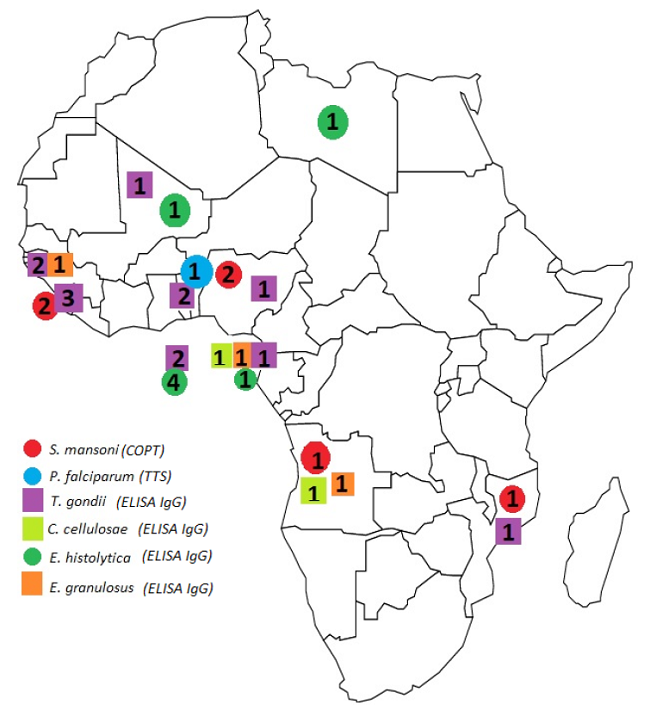
Fig. 3
Number of positive individuals using the confirmatory tests according to their country of origin. (Note: countries and/or diseases without positive cases using the confirmatory tests were excluded from the figure).
Malaria: Only one asymptomatic individual (0.81%) was positive for P. falciparum while testing negative on the rapid test. This patient was a 23 year old male from Togo. The parasite load for this patient was 1680 parasites/µL of blood, as determined by microscopy. In the epidemiological questionnaire, patients were asked about previous malarial episodes. Eighty one (66.39%) claimed to have had previous malaria episodes, 34 (27.86%) of them claimed to have had more than three episodes, but only five (4.09%) knew which species infected them.
Toxoplasmosis: 10.65% of the studied population was confirmed as having chronic toxoplasmosis infection, by both MABA and ELISA. All samples tested with Avidity ELISA had values ranging from 75 to 100% ( x = 94.92% ± 7.51%). Five were female and 8 were male; whose ages ranged from 20 to 27 years old. These individuals came from Sierra Leone (3), Benin (2), Guinea Bissau (2), Saint Thomas and Prince (2), Equatorial Guinea (1), Mali (1), Mozambique (1) and Nigeria (1).
Amoebiasis: 9.83% had positive serol ogy for amoebiasis using MABA. More than half of them (58.3%) had seropositivity by ELISA, which represents 5.74% of the total population (five were male and two female) with ages between 20 and 27years old. These individuals came from Equatorial Guinea (1), Lybia (1), Mali (1) and St Thomas and Prince (4).
Hydatidosis: Out of the four positive cases using MABA (3.27%), three were seropositive with ELISA (2.46% of the total population), being one female and two males, whose ages ranged from 21 to 26years old. These seropositive individuals were originally from Angola, Equatorial Guinea and GuineaBissau.
Cysticercosis: Using MABA, 1.63% of the studied population had positive serology for cysticercosis. All of them were seropositive by ELISA. One of them was a 25 year old female who came from Angola, and the other was a 21 year old male from Equatorial Guinea.
Trypanosomiasis: In the absence of antigen from African trypanosomes, individuals were evaluated with a soluble antigen from T. cruzi. None of the two patients who resulted positive with MABA for American trypanosomiasis had positive serology for the reference ELISA test. The TTS stained with Giemsa were negative for circulating trypanosomes.
Fascioliasis: Neither of the two patients who resulted positive with MABA for fascioliasis, had positive serology using ELISA.
The results obtained in this study are intended to be analyzed with the purpose of developing a comprehensive screening pro tocol in specific migratory populations. Regarding the eight parasitosis studied, particular emphasis will be put on the discussion of schistosomiasis and malaria due to their burden, importance and endemicity in both continents, Africa and America.
MABA is still a preliminary test and its results differ from SMPELISA, the screening reference test (12,17) for schistosomiasis. The large proportion of patients with posi tive serology for schistosomiasis using SMP ELISA (78 patients 63.93%) seems to indi cate that over half of the studied population might have had previous contact with the bodies of water infested with this or other re lated Schistosoma species, most likely with mansoni due to the high sensitivity and specificity of SMPELISA to this species in particular (12).
COPT results are a relevant epidemiological finding. It is alarming that almost 5% of the studied population carries an active schistosomiasis infection, considering the strong disability this disease may inflict in its host. Positive cases were originally from Angola, Mozambique, Nigeria and Sierra Le one, all endemic countries for Schistosoma species.
The COPT is highly specific for the de tection of S. mansoni (12,17), though Hilly er et al (1980) demonstrated that human infection with other Schistosoma species can be diagnosed by the COPT using S. mansoni eggs (18). This is why both a Kato Katz test applied to a serial stool sample and a urinaly sis should be obtained to confirm the species responsible for the infection of this group of students. However, their dispersal to differ ent localities within Venezuela did not allow for further evaluation.
If a schistosomiasis mansoni case is confirmed, the risk of creating a new epidemic focus carries great epidemiological importance, and subsequently would require national, regional and local efforts to man age the cases. Diagnosing nonendemic species in Venezuela, such as S. haematobium,
using COPT is less likely, yet still conceivable. Since the snail, Bulinus spp., the inter mediate host for that species, is not endem ic in America, yet its introduction through migration should not be ruled out. Finally, a coinfection with both S. mansoni and S. haematobium is also a possibility to bear in mind, as stated in previous reports (19, 24). The emphasis made to the screening of schistosomiasis in travelers is due to increasing evidence of the exceptional influence of migration on the disease (25, 26). The es calating number of reports of patients who have acquired the infection while traveling is concerning (25). It has become clearer that migration shapes multiple aspects of the dis ease, including, but not limited, to risk and patterns of transmission and its clinical presentation.
Naturally, the chances of schistosomiasis transmission occurring, increases the longer an individual spends in any of Venezuela’s endemic regions (27). Hence, special emphasis should be put on migrants who in tend to stay for longer visits. However, travelers who stay for shorter periods of time should not be disregarded, as new patterns of transmission have been described among internal travelers who did ecotourism in Brazil (28). Finally, clinical presentation tends to differ from nonimmune tourists, when compared to locals, as it is explained by Corachan, which increases the difficulty of its diagnosis (29).
Therefore, the endorsement for new di agnostic and screening approaches for schistosomiasis is imperative. Special emphasis ought to be made to enhance preventive measures in migrants, particularly those who come from endemic regions. Furthermore, all travelers, regardless of the duration of their stay, are advised to prevent schistosomiasis infection not only for themselves, but for the population surrounding them. Regarding the six patients with active schistosomiasis infection revealed by COPT, it has not been possible to contact them so far for further study and treatment, since they were sent to different health institutions for training in different states of the country.
Malaria is recognized as a “priority global health issue” due to its high prevalence in both Africa and Venezuela. As stated by the World Malaria Report published in 2015 by the WHO, there were an estimated 214 million new cases of malaria around the world (30). In countries where malaria is controlled, such as the United States of America, most cases are reported in recent travelers (31).
The TTS showed one patient (0,81%), originally from Togo, infected with P. falciparum. Despite being a single positive pa tient, it is considered to be one of the major findings of the present study. Interestingly enough, in the OptiMALITⓇ rapid test, all patients resulted negative. The sensitivity of this test for P. falciparum is considerably less than for P. vivax (15), which might explain the negative result, despite the parasite load of this patient (1680 parasites/µL of blood). Nevertheless, this asymptomatic patient responded rapidly to therapy with artesunate/ mefloquine.
Years after the screening, another rap id test (the SD BIOLINEⓇ malaria Ag Pf/ Pv rapid test) was performed, this time using the serum -instead of blood- of the patient infected with P. falciparum, according to TTS. In this case, the patient’s serum is tested positive for P. falciparum. Persistent circulating antigens in serum may explain this phenomenon.
In the questionnaire applied, out of the 122 patients, 34 referred having had more than three malaria episodes in the past, which reflects the high prevalence of this parasitosis in Africa. The high frequency of asymptomatic carriers in areas of high trans mission, especially in SubSaharan countries would require evaluation of this group of students with more sensitive diagnostic tests, such as PCR (32).
When considering the risk of transmission of the disease that implies the arrival of that single case, many factors are to be taken into account. Since in Africa there are other Plasmodium species that are not present on American continent, such as P. ovale, it is possible that this species could be introduced to Venezuela, since we have at least eleven species of the genus Anopheles incriminated as vectors for malaria (33).
Lastly, the possibility of introducing multidrug resistant (MDR) strains of Plasmodium is also feasible. Since the 1980’s, studies have demonstrated the presence of chloroquineresistant malaria in many areas in Africa (34). According to Wongsrichanalai et al. (35), some regions of the African continent are said to be emerging MDR areas because of the change in the first line of treatment from chloroquine to sulfadoxine pyrimethamine after developing chloroquine resistance. This evidence suggests a progressive decrease in the efficiency of the drug. In the Fairhust et al. study, artemisinin resistance is discussed as a possibility warned by the WHO in 2005 (36) and demonstrated recently (37). Being a widely known issue, these drugresistant strains brought from Africa to an endemic region represents a great danger to a very receptive country like Venezuela.
Regarding amoebiasis, seven patients (5.73%) exhibited seropositivity using ELI SA, which it is considered the standard refer ence test for present or past extra intestinal infection. However, Cedeño et al. described (38) that IgG may also be an indicator of intestinal infection, since the parasite induces the production of antibodies by the host, secondary to the presence of the protozoa in the colonic microulcers. Following the acute infection, antiEntamoeba histolytica antibodies remain positive in serum for years (39).
Considering that all individuals were asymptomatic, the possibility of an active infection seems unlikely. Hence, the authors concluded that the positive serology is possibly due to previous contact with the pathogen, which is highly prevalent in African countries. Crossreactivity is exception ally rare when using ELISA for E. histolytica, so while conceivable, it is extremely unlikely (40).
Even though none of these subjects had an active intestinal amoebiasis infec tion, positive serologic tests indicate that they have been previously exposed to the parasite and may be asymptomatic carriers, thus capable of transmitting the disease. Ad ditionally, Venezuela has high prevalence for amoebiasis (38). Special efforts are needed to prevent these patients from acquiring the disease during their stay.
Concerning toxoplasmosis, using both MABA and ELISA, 13 patients (10.65%) test ed IgG positive and IgM negative for toxoplasmosis, with an Avidity ELISA of over 75%. These results suggest that the contact with the parasite occurred over three months ago, becoming a chronic toxoplasmosis infection (41). In the present study, eight out of the 13 positive patients were female. This parasitosis, unlike the previous ones, does not pose a risk to the recipient population, since there is no transmission between humans except for vertical transmission and it is much less likely by transplants and trans fusions.
With regard to hydatidosis, 3 patients (2.45%) were found to have seropositivity for the disease. According to Eris et al. (42) ELISA is an acceptable screening test, with high specificity, but with the disadvantage of having variable sensitivity (43, 44). Therefore, to establish a proper diagnosis, at least two immunologic studies are needed. None of these tests can differentiate a present from a past infection, hence an imaging study is encouraged to classify the status of the infection. Since the liver is the most commonly affected organ (80% of cases) (45), an abdominal ultrasonography is en couraged, bearing in mind that other locations (e.g. lung) may also be affected. All three patients were asymptomatic, meaning that they either may be asymptomatic carriers or might have had seroconversion as an unknown antecedent. ELISA’s crossreactivity is another reasonable possibility, which might be caused by other parasitic diseases (e.g. taeniasis), bronchopulmonary cancer, and liver cirrhosis, among others (42).
As far as cysticercosis is concerned, using both MABA and ELISA, two patients (1.63%) exhibited seropositivity for Cysticercus cellulosae. ELISA has a specificity ranging from 91100%. Therefore, there is a low risk of falsepositive results in symptomatic populations (46, 48). It is reasonable to be lieve that the subjects in this study had pre vious contact with the parasite and may even carry the disease, considering that the tae niasis/cysticercosis complex is an endemic disease in both Latin America and SubSaharan Africa (49) and that 80% (50) of all neurocysticercosis cases are asymptomatic. Regardless, these subjects need further re search, including a Western Blot, lumbar puncture, and imaging tests (MRI or CT) to confirm active infection with C. cellulosae. The epidemiological background and the re sults showed by ELISA are not enough evidence to conclude that they have a cysticercosis infection (51).
In this study, the prevalence of cysticercosis among migrants is relatively low (<2%). This data is in concordance with Brutoo et al (52), who explains that this dis ease is rare among occasional immigrants. It seems unjustified to screen asymptomatic travelers for cysticercosis. Infected patients are incapable of transmitting the disease un less they are coinfected with Taenia solium. These patients should have been screened for taeniasis as well. A stool examination would have been of great value to this study. De termining the prevalence of taeniasis in this population would help to visualize the risk for cysticercosis infection in the Venezuelan population. It is therefore concluded that screening taeniasis rather than cysticercosis in migratory populations is a more suitable measure to determine the risk of transmission of cysticercosis.
Two patients (1.63%) tested positive for fascioliasis using MABA, though when using ELISA as a confirmatory test, both were negative. One of the patients was originally from Angola and the other from Ethiopia. Angola is an endemic country for fascioliasis (53), yet even in areas with high prevalence of bovines, there are no reported cases in humans. With regard to Ethiopia, there are communi ties, particularly in the northwestern area, that have reports of high prevalence among humans (54) and cattle (55). It is unlikely that these subjects were infected with Fasciola spp, since both were asymptomatic and denied having had previous episodes of the infection. Being a severe disease with relatively low prevalence, it is improbable that these patients represent a significant risk to the population.
According to the WHO and PAHO, laboratory diagnosis of American trypanosomiasis or Chagas’ disease must be based on two positive conventional tests with different principles (56, 57). The main conventional tests are immunofluorescence assays (IFA), indirect hemagglutination assays (IHA) and ELISA (57). The existence of common anti gens between T. cruzi and African trypanosomes, such as phospholipase A, MASPs, is known (58, 60). In view of the nonavailability of antigens from humancirculating species in Africa, we used a crude antigen from cruzi for the purpose of detecting possible cases of African trypanosomiasis.
In this study, 1.63% of the population tested positive for American trypanosomia sis using MABA as a preliminary screening test. When using ELISA as a conventional test, neither of these patients resulted positive. Being patients originally from Mali, the possibility of having had contact in the past with African trypanosomiasis was considered. Despite the fact that Mali has not had any cases reported of African trypanosomia sis for over a decade (61), crossreactivity was considered regarding the preliminary results. However, the evidence is not sufficient to attribute the positive cases to cross reactivity; hence another conventional test is advised to be performed. The TTS of all individuals were negative for circulating trypanosomes. However, this test is of low sensitivity in chronic cases. Even if these patients had past contact with African trypanosomiasis, there is no vector (Glossina spp) that could transmit this disease in the Americas, representing no risk for Venezuela’s public health.
According to the author’s unpublished data, a significant number of Bolivian stu dents of a different cohort of the same ELAM program were diagnosed and treated for Chagas’ disease. This is another example of an infected mobile population introducing different strains of parasites where the recipient country has epidemiological conditions for their establishment.
MABA is currently a preliminary test, yet with a promising future. The possibility of using simultaneous multidiagnostic techniques with only a minimum volume as a drop of blood, would have not only a good receptivity on the part of the evaluated individuals, but would also allow for the evaluation of many other diseases of great importance in public health (HIV, other sexually transmit ted diseases, hepatitis, TB, etc.) that were not evaluated in this study. Further studies for other infectious diseases are under consideration.
In this study, the results between MABA and ELISA were compared using only the results from schistosomiasis, considering all patients were screened with both immunologic tests for the same disease, due to its great importance in terms of morbidity and epidemiological impact. The results from McNemar’s test and OR calculation show an increased probability of 23 times (CI95 7.54 114.25) of an individual to be positive by MABA if it is positive by SMPELISA. Further associations are to be analyzed regarding this subject.
Some of the differences observed among the different immunological tests and diseases can be explained by the techniques themselves. Even when the antigens used are the same, ELISA plates and MABA nitrocellulose membranes are different sup port systems. However, there is no doubt that further studies with larger populations are needed in order to adequately validate MABA testing in this context.
A comprehensive screening protocol for multiple parasitosis among asymptomatic migrants is necessary. In the frame of the results presented in this study, Venezuela’s current screening systems require imminent optimization, despite having an adequate legislation regarding this topic (6).
Specific migratory populations who stay longer than conventional tourists, including: international students, refugees, athletes, coaches, technical personnel and managers of companies, military person nel, pilots, sailors, construction workers and symptomatic tourists, are to be screened at both their arrival and departure from their destination. However, screening systems must be carefully designed and thoroughly executed, since unnecessary screening leads to misuse and wasting of resources and is generally unpleasant for patients. Early diagnosis would diminish the costs for the pub lic health system and prevent further deaths and lifelong disabilities.
The arbitrary selection of eight parasitic diseases present in Africa, and in most Venezuela, serves to exemplify the importance of early detection of possible infectious agents in order to establish health protocols to prevent these and other infectious agents from having a national impact on public health. Not only thinking about the pathologies that can be introduced, but also preventing people from acquiring them during their stay.
Schistosomiasis is an important traveler’s disease, which is endemic in Venezuela. These two major reasons justify its screen ing. Furthermore, an estimated 244 million people are diagnosed with malaria each year, and almost 90% of the lethal cases occur in Africa. For this reason alone, malaria must be screened for all migrants who have visited an endemic region in the last week or more. Additionally, Venezuela is an endemic coun try with increasing incidence, which adds to the list of reasons that justifies its screening. Screening the remaining entities (amoebiasis, toxoplasmosis, fascioliasis, hydatidosis, cysticercosis, and trypanosomiasis) is justified in cases where there is a specific clinical and/or epidemiological fact suggesting infection with either of these parasitosis. These have relatively low prevalence in the asymptomatic population, with the exception of toxoplasmosis which has exceptional persontoperson transmission. This explains why screening tests should be performed only when necessary, despite ELISA having relatively high positive predictive values for these entities (42, 62, 65).
Despite the fact that this study was based on parasitosis alone, other IDs are of routine screening (e.g. HIV, hepatitis B, hepatitis C, syphilis and tuberculosis) and it is encouraged that these would be included in any comprehensive screening protocol for migratory populations. Diseases in current epidemic outbreaks should also be included, especially in symptomatic populations (e.g. dengue fever, chikungunya, zika, etc).
Historically, Venezuela had in the past an institution (Instituto Técnico de Inmi gración y Colonización) that controlled migration processes (66). It is advised that institutions that ensure public health create comprehensive policies that prevent the import of IDs to their countries, in order to diminish the globalization of IDs.
Proposing a comprehensive screening protocol as a migratory policy with the information collected in this study, is beyond ambitious, yet necessary. It is implausible to standardize which diseases should be screened to whom, understanding that each case is unique and that there are many factors to bear in mind that may influence the presence of an infection in an asymptomatic individual. For instance, diseases screened in this study were selected acknowledging the singularity of the epidemiology of both Africa and Venezuela.
Taking this into account, the main recommendation is to encourage organizations, corporations, schools or any entity that participates in any kind of international exchange program for any reason, to examine these groups of people based on medical ad vice, implementing a 714 days quarantine, even when being asymptomatic individuals.
In the case of Venezuela, according to this study’s results, it is advised that immigrants coming from endemic regions for schistosomiasis be screened using SMPELI SA, performing a COPT in case of positivity. If an individual arrives from a malaria endemic region, immunochromatographic rapid tests are advised since TTS are time consuming and depend on the person analyzing the sample. However, when rapid test results negative but high risk factors for malaria are present, TTS are recommended.
This study attempts to show the impact of migration in the dynamics of IDs and to generate a screening proposal for asymptomatic migrants, who are often assumed to be healthy. This underestimates the importance of IDs’ transmission, not only during the mi grant’s arrival, but also during their stay.
We thank all the African students who took part in this investigation, and the Escuela Latinoamericana “Salvador Allende.” As for all the health professionals that helped to collect the data used for this publication, we are grateful. We also thank Dr. Mariela Losada, Mr. Andrés Picón and Dr. Renzo Di Natale for English improvements and suggestions.
Corresponding author: Oscar Noya González. Sección de Biohelmintiasis, Instituto de Medicina Tropical, Univer sidad Central de Venezuela, Av. Los Ilustres, Ciudad Universitaria, Los Chaguaramos, 1051. Caracas, Venezuela. Email: noyaoo@yahoo.com
Fig. 1
Number of individuals according to their country of origin in Africa.
Fig. 2
Representative “CrossMABA” of this stu dy. Numbers from 1 to 19 correspond each to specific antigens for different diseases. Letters from A to S correspond to patients sera.
LABORATORY RESULTS OF 122 AFRICAN MEDICAL STUDENTS EVALUATED FOR EIGHT DIFFERENT PARASITIC DISEASES
MABA: Multiple Antigen Blot Assay. ELISA: Enzymelinked Immunoabsorbent Assay. COPT: Circumoval Precipi tin Test. TTS: Thick and thin blood smear.
Fig. 3
Number of positive individuals using the confirmatory tests according to their country of origin. (Note: countries and/or diseases without positive cases using the confirmatory tests were excluded from the figure).
