ABSTRACT
Introduction: Despite its survival benefits, bilateral internal thoracic artery (BITA)
grafting is not commonly utilized due to concerns over deep sternal wound
infection (DSWI). We observed the role of routine use of BITA and off-pump
coronary artery bypass grafting (OPCABG) in the incidence of DSWI and
associated risk factors.
Methods: Between January 2010 and December 2020, 1,207 patients were treated with
isolated coronary artery bypass grafting. In all cases, OPCABG was
attempted, and BITA was used whenever there was a need for a second arterial
graft for the left coronary artery. DSWI was defined as a wound infection
requiring surgical intervention and/or the administration of antibiotics.
Multiple linear regression analysis was employed to model the risk of
DSWI.
Results: The incidence of DSWI was 0.58%. Mortality rate was higher in DSWI group than
in no-DSWI group (28.57% vs. 1.25%; P<0.001). No significant difference
in DSWI incidence was observed when BITA (70.6%) or single internal thoracic
artery (29.4%) were used (P=0.680). The prevalence of diabetes (100% vs.
40.7%; P=0.001), hyperlipidemia (100% vs. 85.9%; P=0.045), and obesity
(71.4% vs. 26.8%; P-0.017) was significantly elevated in DSWI group, when
compared with no-DSWI group. Diabetes (P=0.0001), unstable angina
(P=0.0064), previous myocardial infarction > 30 days (P=0.0009), left
ventricular ejection fraction < 50% (P=0.0074), and emergency surgery
(P=0.0002) were independent risk factors.
Conclusion: The results of routine use of skeletonized BITA after OPCABG were
satisfactory regarding DSWI incidence and operative mortality in a
single-center experience.
Keywords: Wound Infection, angina, unstable, anti-Bacterial Agents, coronary Artery Bypass, off-Pump, coronary Vessels.
Carátula del artículo
Deep Sternal Wound Infection After Beating Heart Coronary Artery
Bypass Surgery with Routine Use of Skeletonized Bilateral Internal Thoracic
Artery
 Daniel M. S. Magalhães danielmagalhaes@alumni.usp.br; danielmagalhaes@alumni.usp.br
Daniel M. S. Magalhães danielmagalhaes@alumni.usp.br; danielmagalhaes@alumni.usp.br
Hospital Unimed João Pessoa - Alberto Urquiza
Wanderley, Brazil
Hospital Memorial São Francisco, Brazil
Maurilio O. Deininger
Hospital Unimed João Pessoa - Alberto Urquiza
Wanderley, Brazil
Hospital Memorial São Francisco, Brazil
Orlando Gomes de Oliveira
Hospital Unimed João Pessoa - Alberto Urquiza
Wanderley, Brazil
Hospital Memorial São Francisco, Brazil
John Allexander De Freitas
Hospital Unimed João Pessoa - Alberto Urquiza
Wanderley, Brazil
Hospital Memorial São Francisco, Brazil
Eugênia di Giuseppe Deininger
Hospital Unimed João Pessoa - Alberto Urquiza
Wanderley, Brazil
Hospital Memorial São Francisco, Brazil
Brazilian Journal of Cardiovascular Surgery, vol. 38, no. 4, pp. 1-6, 2023
Sociedade Brasileira de Cirurgia Cardiovascular
Received: 09 December 2021
Accepted: 17 May 2022

INTRODUCTION
Deep sternal wound infection (DSWI) is a serious complication after coronary artery
bypass grafting (CABG), which increases its morbidity and mortality. Several
retrospective clinical trials have documented an increased risk of these
complications associated with bilateral internal thoracic artery (BITA) harvesting,
especially in patients with diabetes, chronic obstructive pulmonary disease (COPD),
and obesity[1].
The incidence of DSWI seems to be caused by the sternal ischemia that occurs after
harvesting the BITA pedicle. Anatomical studies confirmed a decrease in sternal
blood flow resulting from BITA dissection, and this was demonstrated by
postoperative flow studies[2]. In
order to minimize sternal complications, techniques such as skeletonized internal
thoracic artery (ITA) dissection and low-energy electrocautery have been
used[3]. Since these
techniques were adopted, a reduction in wound infections has been reported when BITA
grafts were removed, even in high-risk patients[3,4,5].
Despite the demonstrated benefits of BITA over the single internal thoracic artery
(SITA) in reintervention-free long-term survival, many surgeons still resist routine
adoption of BITA grafting[6,7]. The technical challenge, the
longer time spent, and the risk of infection are the main factors for restricting
this technique to only 4-5% of CABG procedures worldwide[8,9].
Some authors demonstrated that off-pump coronary artery bypass grafting (OPCABG),
using skeletonized BITA, reduced postoperative complications, including wound
infection, when compared to the conventional technique[10,11].
We hypothesize that OPCABG with BITA can be used routinely even in high-risk
patients, including those with diabetes, COPD, and obesity, despite the risk of
DSWI. This study retrospectively analyzed, over 10 years, all patients undergoing
CABG in a single center, to identify the incidence of DSWI and associated risk
factors.
METHODS
In this study, we performed a retrospective analysis of data from the hospital
records of all patients undergoing isolated CABG in our service, in order to
identify serious complications of the surgical wound. All patients were operated on
by the same team of experienced surgeons.
The eligibility criterion was isolated CABG, therefore, patients undergoing combined
procedures were excluded from this study. It was intended to perform OPCABG in all
cases. From January 2010 to December 2020, a total of 2,211 patients underwent
cardiac surgery, of which 1,207 (54.59%) were treated with isolated CABG.
Graft Selection
It was based on the following strategies: 1) patients with severe multivessel
disease (> 75%) involving the left coronary arteries or left main obstruction
superior to 50% received BITA grafts; and 2) for minor lesions or to
revascularize the right coronary artery, great saphenous veins grafts were used
as additional conduits; ITA arteries were harvested in a skeletonized fashion
with a conventional monopolar scalpel at low energy levels. The graft
arrangement included: in situ, composite, or aortocoronary
bypass. Distal anastomosis was generally performed with 8-0 polypropylene
suture. The right internal thoracic artery (RITA) was most often anastomosed to
the region of the left anterior descending artery, crossing anteriorly the
aorta, and the left internal thoracic artery was usually anastomosed to the
circumflex artery system in this set. For complete myocardial revascularization,
saphenous vein or radial artery grafts were used as additional conduits.
Perioperative Management
A few hours before surgery, the hairs around the surgical site were removed with
clippers, and all patients were washed with a 2% chlorhexidine soap solution. In
the operating room, traditional surgical scrubbing with a 2% chlorhexidine
solution was performed. Before the skin incision, cefazolin (2 g) was initially
administered, and additional doses (1 g) were administered every three hours
during the procedure. The presternal space was closed with two layers of
absorbable monofilament suture, followed by a continuous absorbable skin suture.
Intravenous prophylactic antibiotics were administered after surgery for two
days. During the procedure, blood glucose was routinely measured every two
hours. An intravenous insulin infusion was given when blood glucose exceeded 150
mg/dL.
Deep Sternal Wound Infection
DSWI was defined as a wound infection involving muscle, bone, and/or the
mediastinum that meets any of the following conditions: open wound, with
excision of tissue or re-exploration of mediastinum, positive culture, or
treatment with antibiotics - based on the United States of America Centers for
Disease Control guidelines -, and included patients who received required wound
debridement and re-stitching[12]. For analysis purposes, all patients who were readmitted
at any time in their evolution due to DSWI were considered.
Statistical Analysis
Continuous variables are expressed as mean and standard deviation. The
differences between groups were compared using Student’s t-test
for normally distributed continuous data, or the Mann-Whitney U test for
non-normally distributed continuous variables, and using the Fisher’s exact test
for categorical variables. Multivariate analyses were performed by forward
stepwise linear regression model. When dealing with continuous variables, in
which the relationship with the outcome was not linear, we determined cutoff
points, such as age, for example.
RESULTS
Preoperative Characteristics
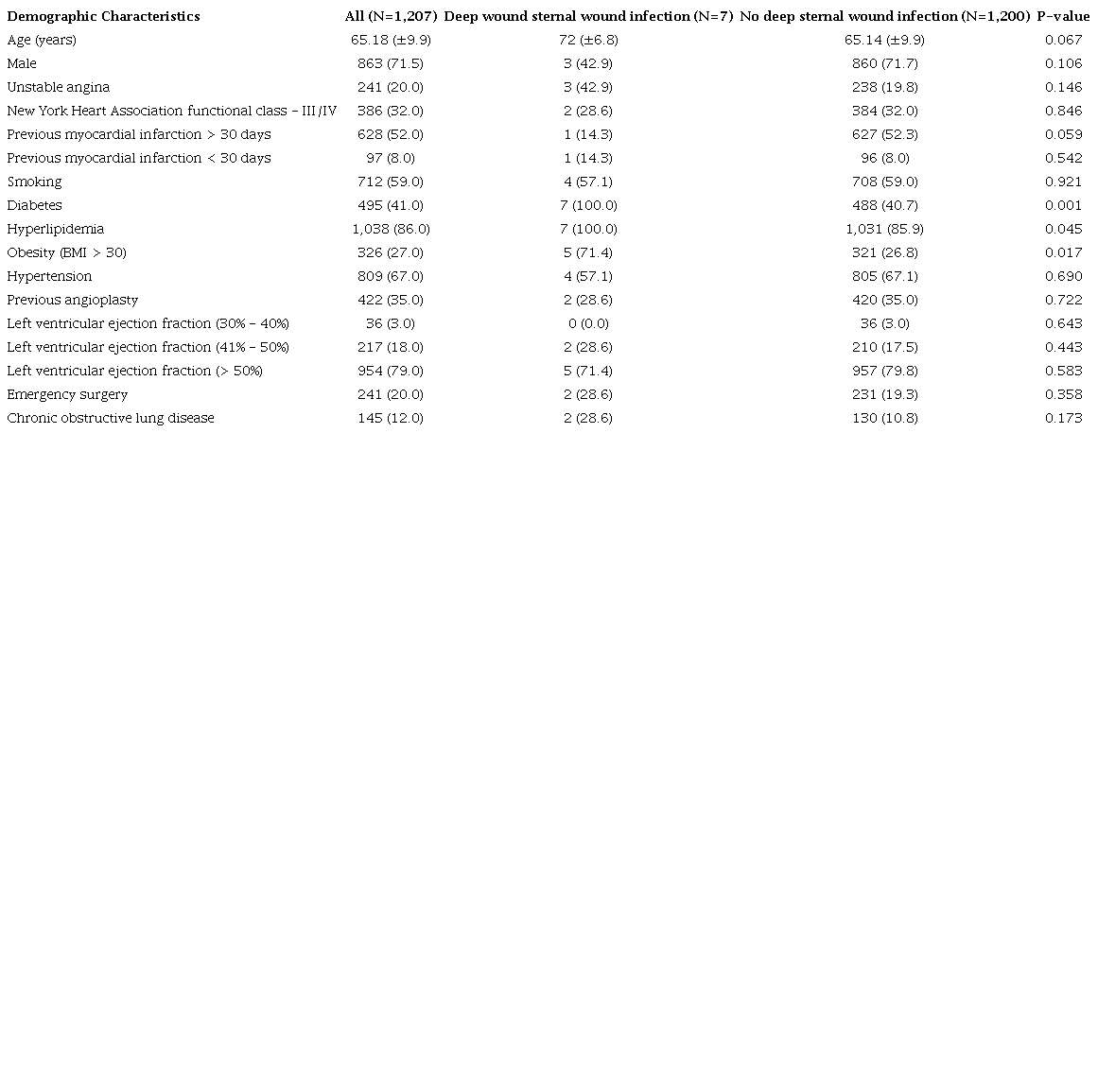
A total of 1,207 patients were treated with isolated CABG, and only seven had
DSWI (0.58%). Table 1 shows preoperative
characteristics. The mean age was 72±6.8 years in DSWI vs.
65.14±9.9 years in no-DSWI group (P=0.067). The prevalence of
diabetes mellitus (100% vs. 40.7%; P=0.001),
hyperlipidemia (100% vs. 85.9%; P=0.045), and
obesity (71.4% vs. 26.8%; P=0.017) were
significant elevated in DSWI group, when compared with no-DSWI group.
Table 1
Demographic characteristics
Operative Characteristics
Ninety-seven percent of surgeries were performed by OPCABG, with a conversion
rate of 2.7% (Table 2). No significant
difference was observed in DSWI incidence when surgery was converted from OPCABG
(14.3% in DSWI group vs. 2.7% in no-DSWI group;
P=0.209). No significant difference in DSWI incidence was
observed when BITA (70.6%) or SITA (29.4%) were used (P=0.680).
A no-touch aorta surgery was performed in 32.8%. In 65.1% of cases, RITA was
used anteriorly crossing the aorta. The total number of distal anastomoses was
3,386 (mean of 2.8 anastomoses per patient). The operative mortality (in
hospital) was significantly higher in patients with DSWI (28.57%) when compared
with no-DSWI patients (1.25%; P<0.001).
Table 2
Surgical aspects.

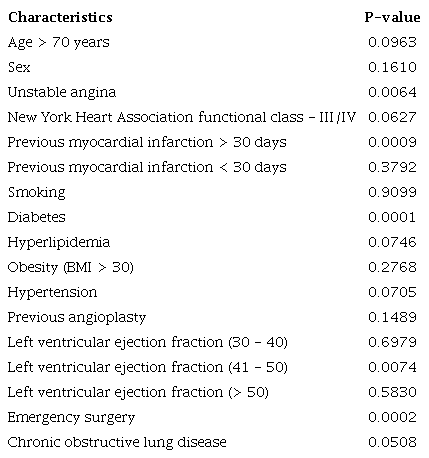
Risk
Linear regression analysis demonstrated that diabetes, unstable angina, previous
myocardial infarction, left ventricular ejection fraction < 50%, and
emergency surgery were strong independent risk factors for DSWI (Table 3).
Table 3
Linear regression analysis.
DISCUSSION
The present study using data from a single center showed satisfactory results of
isolated OPCABG with a higher rate of BITA graft use (70.6%) and low incidence of
DSWI (0.58%) and hospital mortality (1.4%).
The main reason why cardiovascular surgeons are hesitant to perform BITA grafts is
DSWI, especially in patients with multiple preoperative risk factors such as
diabetes mellitus, low ejection fraction, lung disease, and chronic kidney
disease[13-15]. In fact, the present study showed that the rate
of severe postoperative complications, including in-hospital mortality, was
significantly higher in patients with DSWI (28.57%) compared to no-DSWI patients
(1.25%) (P<0.001), demonstrating the severity of this
complication. However, the survival benefits of the BITA graft for these high-risk
patients have been also reported compared to the SITA graft surgery[6,7]. Therefore, a proper risk assessment of the DSWI is essential
to minimize risk and maximize the long-term benefits derived from using BITA. The
incidence of DSWI in the present cohort (0.58%) was acceptable compared to reports
from various centers or national cohorts (1.4%-5.2%)[4,15,16]. The high prevalence of diabetes
(41% in this cohort vs. 18.2%-33.3% in patients undergoing BITA
graft in previous studies)[6,8,9,17,18], previous percutaneous coronary intervention (35%
vs. 3.2% -16.7 in patients undergoing BITA graft in previous
studies)[14,19,20], and the higher mean age (65.1±9.9 years
vs. 56.0-60.1±5.5 years) are in agreement with the selection
profile in which all patients were listed consecutively, better representing the
“real-world” situation[6,8,18,21]. Regarding
patients with diabetes, the incidence of DSWI receiving BITA grafts ranges from 2.9
to 11.6%[4,15,20,22] and in the present study it was
1.71%, which confirms the low incidence of DSWI in this cohort, even in high risk
patients. OPCABG was performed in 97.3% of patients in this study. It is expected
that OPCABG reduces the systemic perioperative inflammatory response; however,
OPCABG has not been identified as an independent factor to reduce DSWI[17,20]. Despite a low conversion rate from OPCABG to on-pump CABG
(2.7%), no significant difference was observed in DSWI incidence when surgery was
converted from OPCABG (14.3% in DSWI group vs. 2.7% in no-DSWI
group; P=0.209). The absence of difference may be related to the
small number of converted cases. A larger number of patients would be needed to
identify whether conversion would be a risk factor for DSWI. A recent sub-analysis
of the Arterial Revascularization Trial clearly demonstrated that a skeletonized
BITA reduces the risk of DSWI compared to a pedicled BITA[20]. Even with a high rate use of BITA (70.6%) in
this study, there was no significant increase in DSWI compared to similar
studies[14,18,20] or
compared to SITA use (P=0.683), perhaps due to careful graft
dissection by experienced surgeons, but this may not be applicable to surgeon
training centers, for example. A lower incidence of DSWI in this cohort could be
influenced by skeletonized use in all cases. The mean age was higher in DSWI group
(72±6.8 years) vs. 65.14±9.9 years in no-DSWI group
(P=0.067), despite not having reached a statistically
significant difference. Perhaps a study with a greater number of cases could have
shown a difference, since age is an additional risk factor for complications. The
prevalence of diabetes mellitus (100% vs. 40.7%;
P=0.001), hyperlipidemia (100% vs. 85.9%;
P=0.045), and obesity (71.4% vs. 26.8%;
P-0.017) were significant elevated in DSWI group, when compared
with no-DSWI group. These findings are in agreement with some previous
studies[14,18,20]. Often,
obese diabetic patients are excluded from studies using BITA, due to the higher risk
of infectious complications.
In the present risk model, diabetes mellitus has been recognized as the main risk
factor for DSWI[16-18,22].
Preoperative hemodynamic status, such as an ejection fraction < 60%, is an
independent risk factor for DSWI. These results are reasonable because a low output
status has been recognized as a risk factor for infection[17,20].
Unstable angina and emergency surgery were independent risk factors too for DSWI in
this study. These results may be in agreement with the greater severity of these
patients, including the possible use of dual antiplatelet therapy at the time of
surgery and a poor diabetes control, which can lead to longer surgical time and
higher incidence of bleeding and infection.
Limitations
We must note several limitations in this study. It was a retrospective study
using a single-center hospital database with no mortality long-term results. The
results of this study may be biased because it is a single center, with a
relatively low volume of surgeries and with a unique team of dedicated and
experienced surgeons, which may not represent the “real-world” in high-volume
institutions. Therefore, the choice of patients who will undergo BITA must be
done carefully in most centers.
CONCLUSION
We reported the results and risks of DSWI after OPCABG BITA grafting from a single
center; the results of routine use of BITA grafting were acceptable, and the
incidence of hospital death after DSWI was higher than that with no-DSWI. The
current data and risk model are informative to evaluate the risk of DSWI when
performing OPCABG BITA grafting. Additional long-term prospective and multicenter
studies are still needed to validate the routine use of BITA for all patients.
REFERENCES
Balachandran S, Lee A, Denehy L, Lin KY, Royse A, Royse C, et al.
Risk factors for sternal complications after cardiac operations: a systematic
review. Ann Thorac Surg. 2016;102(6):2109-17.
doi:10.1016/j.athoracsur.2016.05.047.
Sajja LR, Mannam G. Internal thoracic artery: anatomical and
biological characteristics revisited. Asian Cardiovasc Thorac Ann.
2015;23(1):88-99. doi:10.1177/0218492314523629.
Sajja LR. Strategies to reduce deep sternal wound infection after
bilateral internal mammary artery grafting. Int J Surg. 2015;16(Pt B):171-8.
doi:10.1016/j.ijsu.2014.11.017.
Raza S, Sabik JF 3rd, Masabni K, Ainkaran P, Lytle BW, Blackstone
EH. Surgical revascularization techniques that minimize surgical risk and
maximize late survival after coronary artery bypass grafting in patients with
diabetes mellitus. J Thorac Cardiovasc Surg. 2014;148(4):1257-64; discussion
1264-6. doi:10.1016/j.jtcvs.2014.06.058.
Peterson MD, Borger MA, Rao V, Peniston CM, Feindel CM.
Skeletonization of bilateral internal thoracic artery grafts lowers the risk of
sternal infection in patients with diabetes. J Thorac Cardiovasc Surg.
2003;126(5):1314-9. doi:10.1016/s0022-5223(03)00808-0.
Lytle BW, Blackstone EH, Sabik JF, Houghtaling P, Loop FD, Cosgrove
DM. The effect of bilateral internal thoracic artery grafting on survival during
20 postoperative years. Ann Thorac Surg. 2004;78(6):2005-12; discussion 2012-4.
doi:10.1016/j.athoracsur.2004.05.070.
Puskas JD, Sadiq A, Vassiliades TA, Kilgo PD, Lattouf OM. Bilateral
internal thoracic artery grafting is associated with significantly improved
long-term survival, even among diabetic patients. Ann Thorac Surg.
2012;94(3):710-5; discussion 715-6.
doi:10.1016/j.athoracsur.2012.03.082.
Tabata M, Grab JD, Khalpey Z, Edwards FH, O'Brien SM, Cohn LH, et
al. Prevalence and variability of internal mammary artery graft use in
contemporary multivessel coronary artery bypass graft surgery: analysis of the
society of thoracic surgeons national cardiac database. Circulation.
2009;120(11):935-40. doi:10.1161/CIRCULATIONAHA.108.832444.
LaPar DJ, Crosby IK, Rich JB, Quader MA, Speir AM, Kern JA, et al.
Bilateral internal mammary artery use for coronary artery bypass grafting
remains underutilized: a propensity-matched multi-institution analysis. Ann
Thorac Surg. 2015;100(1):8-14; discussion 14-5.
doi:10.1016/j.athoracsur.2015.02.088.
Kinoshita T, Asai T, Suzuki T. Off-pump bilateral skeletonized
internal thoracic artery grafting in patients with chronic kidney disease. J
Thorac Cardiovasc Surg. 2015;150(2):315-21.e3.
doi:10.1016/j.jtcvs.2015.04.058.
Sajja LR, Mannam G, Dandu SB, Sompalli S. Reduction of sternal wound
infections in diabetic patients undergoing off-pump coronary artery bypass
surgery and using modified pedicle bilateral internal thoracic artery harvest
technique. J Thorac Cardiovasc Surg. 2012;144(2):480-5.
doi:10.1016/j.jtcvs.2012.03.024.
Benedetto U, Altman DG, Gerry S, Gray A, Lees B, Pawlaczyk R, et al.
Pedicled and skeletonized single and bilateral internal thoracic artery grafts
and the incidence of sternal wound complications: insights from the arterial
revascularization trial. J Thorac Cardiovasc Surg. 2016;152(1):270-6.
doi:10.1016/j.jtcvs.2016.03.056.
Aldea GS, Bakaeen FG, Pal J, Fremes S, Head SJ, Sabik J, et al. The
society of thoracic surgeons clinical practice guidelines on arterial conduits
for coronary artery bypass grafting. Ann Thorac Surg. 2016;101(2):801-9.
doi:10.1016/j.athoracsur.2015.09.100.
Dai C, Lu Z, Zhu H, Xue S, Lian F. Bilateral internal mammary artery
grafting and risk of sternal wound infection: evidence from observational
studies. Ann Thorac Surg. 2013;95(6):1938-45.
doi:10.1016/j.athoracsur.2012.12.038.
Kieser TM, Lewin AM, Graham MM, Martin BJ, Galbraith PD, Rabi DM, et
al. Outcomes associated with bilateral internal thoracic artery grafting: the
importance of age. Ann Thorac Surg. 2011;92(4):1269-75; discussion 1275-6.
doi:10.1016/j.athoracsur.2011.05.083.
Gatti G, Soso P, Dell'Angela L, Maschietto L, Dreas L, Benussi B,
Luzzati R, Sinagra G, et al. Routine use of bilateral internal thoracic artery
grafts for left-sided myocardial revascularization in insulin-dependent diabetic
patients: early and long-term outcomes. Eur J Cardiothorac Surg.
2015;48(1):115-20. doi:10.1093/ejcts/ezu360.
Itagaki S, Cavallaro P, Adams DH, Chikwe J. Bilateral internal
mammary artery grafts, mortality and morbidity: an analysis of 1 526 360
coronary bypass operations. Heart. 2013;99(12):849-53.
doi:10.1136/heartjnl-2013-303672.
Vrancic JM, Piccinini F, Camporrotondo M, Espinoza JC, Camou JI,
Nacinovich F, et al. Bilateral internal thoracic artery grafting increases
mediastinitis: myth or fact? Ann Thorac Surg. 2017;103(3):834-9.
doi:10.1016/j.athoracsur.2016.06.080.
Benedetto U, Caputo M, Gaudino M, Marsico R, Rajakaruna C, Bryan A,
et al. Right internal thoracic artery or radial artery? A propensity-matched
comparison on the second-best arterial conduit. J Thorac Cardiovasc Surg.
2017;153(1):79-88.e4. doi:10.1016/j.jtcvs.2016.08.060.
Ohira S, Miyata H, Yamazaki S, Numata S, Motomura N, Takamoto S, et
al. Deep sternal wound infection after bilateral internal thoracic artery
grafting: insights from a Japanese national database. J Thorac Cardiovasc Surg.
2019;157(1):166-73.e1. doi:10.1016/j.jtcvs.2018.06.101.
Nakano J, Okabayashi H, Hanyu M, Soga Y, Nomoto T, Arai Y, et al.
Risk factors for wound infection after off-pump coronary artery bypass grafting:
should bilateral internal thoracic arteries be harvested in patients with
diabetes? J Thorac Cardiovasc Surg. 2008;135(3):540-5.
doi:10.1016/j.jtcvs.2007.11.008.
Saito A, Miyata H, Motomura N, Ono M, Takamoto S; Japan
Cardiovascular Surgery Database Organization. Propensity-matched analysis of
bilateral internal mammary artery vs single internal mammary artery in 7702
cases of isolated coronary artery bypass grafting. Eur J Cardiothorac Surg.
2013;44(4):711-7. doi:10.1093/ejcts/ezt157.
Notes
Notes
No financial support.
Conflict of interest declaration
No conflict of interest.
Author notes
This study was carried out at the Hospital Unimed João Pessoa - Alberto
Urquiza Wanderley and Hospital Memorial São Francisco, João Pessoa, Paraíba,
Brazil.
Correspondence Address: Daniel Magalhães, https://orcid.org/0000-0002-7845-6257, Rua Giácomo Porto, 99.
901 - Miramar, João Pessoa, PB, Brazil, Zip Code: 58032-110, E-mail:
danielmagalhaes@alumni.usp.br

