Carátula del artículo
Is Incentive Spirometry Superior to Standard Care in Postoperative
Cardiac Surgery on Clinical Outcomes and Length of Hospital and Intensive Care
Unit Stay? A Systematic Review with Meta-Analysis
Hiago Vinicius Costa Silva
Universidade Federal do Amapá, Brazil
Adriana Claudia Lunardi
Universidade Cidade de São Paulo, Brazil
Universidade de São Paulo, Brazil
Ana Carolina Pereira Nunes Pinto
Universidade Federal do Amapá, Brazil
University of Pittsburgh, United States of America
Juliana Ribeiro Fonseca Franco de Macedo
Catholic University of Louvain, Belgium
 Elinaldo da Conceição dos Santos drelinaldo@yahoo.com.br
Elinaldo da Conceição dos Santos drelinaldo@yahoo.com.br
Universidade Federal do Amapá, Brazil
Brazilian Journal of Cardiovascular Surgery, vol. 39, núm. 3, e20220319, 2024
Sociedade Brasileira de Cirurgia Cardiovascular
Recepción: 05 Abril 2023
Aprobación: 16 Mayo 2023
INTRODUCTION
Cardiac surgery is a frequent surgical procedure. Each year, Australian hospitals
perform > 12,000 cardiac surgeries, and a single Brazilian hospital has already
performed > 2,900 of these procedures[1,2]. In the United
States of America, the cost of cardiac surgery is approximately 1% to 2% of the
health budget[3]. The majority of
patients undergo coronary artery bypass grafting (CABG), and 74.6% of surgeries are
scheduled[4]. Complex
cardiac surgery and prolonged hospital length of stay (LOS) may present a high risk
of complications and mortality; postoperative mortality has been documented at 4%
(valve operations) within the first seven days and 6.4% (overall mortality) within
the first postoperative month[4].
Approximately 10.2% to 27.3% of CABG patients present at least one complication,
70.6% after valve surgery, and 84.2% after combined surgery (CABG + valve
surgery)[5,6]. Regarding the complications, 2.2% are major
adverse cardiovascular events[7],
7.5% are reintubated during the intensive care unit (ICU) stay, which increases the
rate of complications[8], 23.2%
remain hospitalized in an ICU for more than two days after surgery, and 59.7% remain
hospitalized for more than seven days[6]. It seems that when the complication rate increases, hospital
LOS and mortality also increase (12% in the ICU and 15.1% in the 30-day period),
mainly in older adults[5,9].
Among the prophylactic strategies to decrease these rates of negative outcomes,
respiratory care seems to reduce pulmonary complications and minimize postoperative
pulmonary dysfunction[10]. As one
of the respiratory care techniques, incentive spirometry (IS) is a low-cost,
widespread, respiratory exercise technique, used for the prevention and treatment of
postoperative pulmonary complications (PPC) in patients undergoing cardiac
surgery[11]. IS is a
device that provides visual feedback when the patient inhales at a predetermined
flow or volume. The patient is required to place the lips firmly around the
mouthpiece and to inhale slowly to raise the ball (flow-oriented) or piston/plate
(volume-oriented) in the chamber toward the defined target[12].
It has been suggested that patients undergoing cardiac surgery who are more adherent
to IS therapy may benefit from a reduced LOS and a reduction in the mortality
rate[13]. On the other
hand, scientific evidence has suggested that IS does not improve clinical outcomes
in different surgical patients[14]. In order to strengthen the scientific findings, our systematic
review, performed with strict methodological criteria, is intended to clarify these
specific gaps, exclusively in patients undergoing cardiac surgery and assist
clinicians in decision making. Our aim was to assess whether IS is superior to
respiratory care, mobilization exercises, and noninvasive ventilation (NIV) on PPC,
adverse events, mortality, hospital and/or ICU LOS, lung function, oxygenation, and
maximal inspiratory pressure (MIP) in patients undergoing cardiac surgery.
METHODS
Design
We conducted a systematic review following the reporting recommendations proposed
by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (or
PRISMA)[15]. The
protocol was registered in the International Prospective Register of Systematic
Reviews (or PROSPERO) (#CRD42020161009), is available online at https://www.crd.york.ac.uk/prospero/export_record_pdf.php), and
was previously published[16].
Eligibility Criteria
Types of Studies, Participants, and Interventions
We searched for randomized and quasi-randomized controlled trials published
in any year, in any language. The studies included in this review were
required to have enrolled patients aged 18 years or older, who were
breathing spontaneously, undergoing cardiac surgeries, and which evaluated
the effects of postoperative flow or volume-oriented IS on our pre-defined
clinical outcomes. The treatment comparison was made with standard care,
such as respiratory care (maximal inspiratory breathing exercises, coughing
and deep breathing, supported/assisted coughing, huffing technique,
diaphragmatic breathing, fractional inspiration, active cycle of breathing,
and autogenic drainage), NIV, and other therapies (mobilization exercise,
blow bottles, and verbal encouragement). The mobilization exercises
considered in this review were early mobilization programs, active/passive
exercises of upper/lower limbs, and physical therapy.
The controlled trials had to have evaluated at least one of the following
outcomes:
Primary Outcomes
-
PPC: For this systematic review, atelectasis and pneumonia were
considered.
-
Adverse events: Any reaction, harm, or complication associated with
IS reported in the included studies.
-
Mortality: All reported deaths were accepted, regardless of
cause.
Secondary Outcomes
-
LOS: The number of days spent in hospital after cardiac surgical
procedure.
-
Length of ICU stay: The number of days spent in the ICU after cardiac
surgical procedure.
-
Lung function: Variables evaluated were peak of expiratory flow
(PEF), forced expiratory volume in one second (FEV₁), forced vital
capacity (FVC), and vital capacity (VC).
-
Oxygenation: Arterial partial pressure of oxygen (PaO2)
and peripheral and central arterial oxygen saturation
(SO2) were accepted.
-
MIP (cmH₂O): MIP measured with digital or analog manovacuometer or
manometer was accepted.
Database and Search Strategy
The search strategy was sensitive (Supplement
1) to capture all potentially qualifying studies through the Medical
Literature Analysis and Retrieval System Online (or MEDLINE®), Embase®, Cochrane
Central Register of Controlled Trials (or CENTRAL), Physiotherapy Evidence
Database (PEDro), Cumulative Index of Nursing and Allied Health (or CINAHL®),
Latin American and Caribbean Health Sciences Literature (or LILACS), Scientific
Electronic Library Online (or SciELO), and Scopus® databases, as well as in the
OpenGrey database, the main clinical trial registration sites, conferences,
congresses, and symposiums in the area described in the protocol[16]. When necessary, we contacted
the authors of the clinical trials to request additional data. The snowball
technique, which consists of searching the reference lists of the included
studies, was used to optimize the search. The search was performed on July 22
and 24, 2022.
Study Selection and Data Extraction
Two authors independently selected the studies identified by the search strategy
based on eligibility criteria. Duplicate publications were excluded, after which
the authors selected the studies by titles and abstracts. Non-randomized trials
and studies lacking predefined outcomes were excluded. In some cases, it was
necessary to read the full texts. Where reports with the same participants but
different outcome measurements or using different time points for the
assessments were found, both reports were included. However, the two reports
were considered as parts of only one study.
The Rayyan app was used to optimize the process of screening and selecting the
studies[17].
Disagreements between authors regarding the inclusion of the study were resolved
by a third author. Two authors extracted data independently, and disagreements
were also resolved by a third author.
Methodological Rigor of Included Studies and Certainty of Evidence
We assessed the methodological characteristics of the trials using the PEDro
scale[18]. We used
PEDro scores available at https://pedro.org.au/. Where
PEDro scores were not available, two previously trained authors evaluated the
clinical trials using the PEDro scale. The PEDro methodological rigor scale
ranges between 1 and 10, with higher scores indicating higher quality studies.
The studies are classified according to the scores as follows: < 4 are
considered “poor”, 4 to 5 are considered “fair”, 6 to 8 are considered “good”,
and 9 to 10 are considered “excellent”[19]. We assessed the certainty of evidence using the
Classification of Recommendations, Assessment, Development and Evaluation
(GRADE)[20], through
the software GRADEpro in the main outcomes[21].
Data Analysis
When at least two studies were sufficiently homogeneous in terms of participants,
interventions, and outcome measures, we pooled their results in a meta-analysis.
Meta-analyses were performed using an inverse variance method and random effects
model in Review Manager version 5.3 (The Nordic Cochrane Center, Copenhagen,
Denmark)[22].
Continuous variables were analyzed using the weighted mean differences (MD) and
for studies that evaluated the same outcome with different instruments, we used
the standardized mean differences (SMD) with 95% confidence interval
(CI)[23]. Dichotomous
variables were analyzed using risk ratios (RR) with 95% CI.
Trials were pooled according to similarity of intervention, populations, and the
outcomes measured. Separate meta-analyses were conducted to examine the effects
of IS in the following comparisons:
-
IS vs. respiratory care.
-
IS vs. NIV.
-
IS vs. other therapies.
In case of trials that examined the effects of multiple interventions that were
of interest for this review, to avoid double counting the participants, we
included two reasonably independent comparisons. However, we split the “shared”
group sample size (respiratory care) into two smaller sample sizes. For example,
Stock et al. (1984)[24] had
three groups in its clinical trial: intervention group (with 12 participants),
control group 1 (with 13 participants), and control group 2 (with 13
participants). In this situation, the analysis was performed twice; in the first
analysis, the intervention group (with six participants [half the original
sample size]) was analyzed vs. control group 1. In the second
analysis, the intervention group (with six participants [half the original
sample size]) was compared with control group 2.
Therefore, in the included clinical trials with three comparison groups (flow-IS
group vs. volume-IS vs. respiratory care), and
where data were analyzed twice in our study, we initially identified the name of
the main author, and then the year of publication, followed by the letter “a”
(Amin et al 2021a: flow-IS group vs. respiratory care) and in
the second mention, we identified the name of the main author, and then the year
of publication, followed by the letter “b” (Amin et al 2021b: volume-IS group
vs. second standard care)[25].
Assessment of Heterogeneity
As planned, where appropriate data were available, we carried out subgroup
analyses so as to investigate the influence of each comparison on the size of
the treatment. Among the preplanned subgroup analyses, it was possible to
perform subgroup analyses considering the type of device used (flow-oriented or
volume-oriented) in the main comparisons (IS vs. respiratory
care; IS vs. NIV; and IS vs. other
therapies).
To estimate the heterogeneity across the studies in each meta-analysis, the I2
statistic was used. As suggested in the Cochrane Handbook for Systematic Reviews
of Interventions, if heterogeneity was substantial (I2 ≥ 50%), a sensitivity
analysis was considered[26].
Although we intended to perform separate analyses for studies with no blinding
or deficiency in blinding of outcome assessors, with inappropriate randomization
methods, with a large number (> 20%) of patients lost to follow-up, with
imputation of standard deviation, or when adherence was not reported, we could
not perform sensitivity analyses because we did not find enough studies with
appropriate blinding, randomization, or follow-up.
RESULTS
Twenty-three reports of 22 studies were included in this systematic review[27-48]. Twenty-two publications were reported in full; from one
clinical trial, only the abstract was reported. One study with two publications was
included in this systematic review. The reports of this study were named as Jenkins
et al. (1989)[30] and Jenkins et
al. (1990)[31], however, as
planned, they were considered as part of only one study. The authors of the clinical
trial published in abstract format were contacted in an attempt to request
additional data[39], however, we
did not receive any answers. In this case, we used the data available in the
abstract. Twenty-one studies were randomized controlled trials (RCTs) and one was a
quasi-randomized trial. The flow chart of this systematic review is shown in Figure 1.
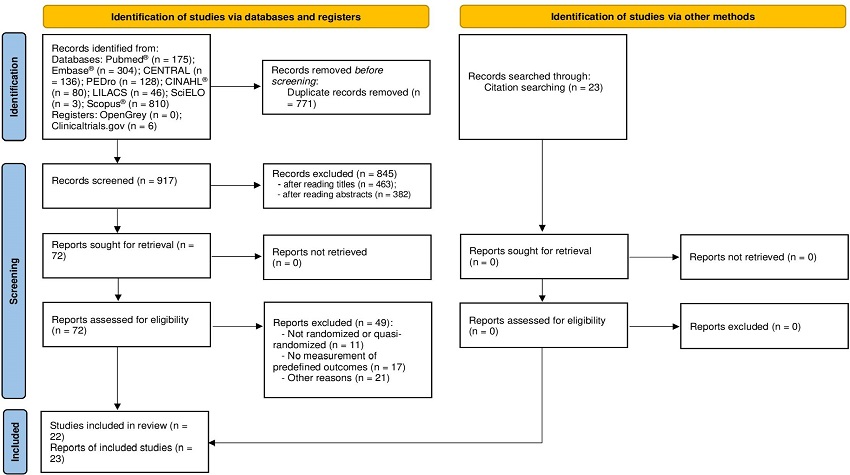 Fig. 1
Flow diagram of systematic review. CENTRAL=Cochrane Central Register
of Controlled Trials; CINAHL®=Cumulative Index of Nursing and Allied
Health; LILACS=Latin American and Caribbean Health Sciences Literature;
PEDro=Physiotherapy Evidence Database; SciELO=Scientific Electronic
Library Online.
Fig. 1
Flow diagram of systematic review. CENTRAL=Cochrane Central Register
of Controlled Trials; CINAHL®=Cumulative Index of Nursing and Allied
Health; LILACS=Latin American and Caribbean Health Sciences Literature;
PEDro=Physiotherapy Evidence Database; SciELO=Scientific Electronic
Library Online.
Included Studies
Overall, we included 21 randomized trials and one quasi-randomized controlled
trial in this systematic review. The studies involved 1,677 patients, with ages
ranging from 38.3 to 65 years[31,45], sample
sizes ranging from 16 to 270 participants[43,46], and study
follow-up time ranging from two days to hospital discharge (Table 1)[33,39,40,42]. Regarding the characteristics of the surgery and
intervention, 74% of patients underwent CABG, 48% of patients received treatment
using volume-oriented IS, 39% of patients used flow-oriented IS, and three
studies did not have enough information to determine whether the type of
spirometer was flowor volume-oriented (Table
2)[39,46,48]. The hospital LOS ranged from 6.5 to 12.5 days, and
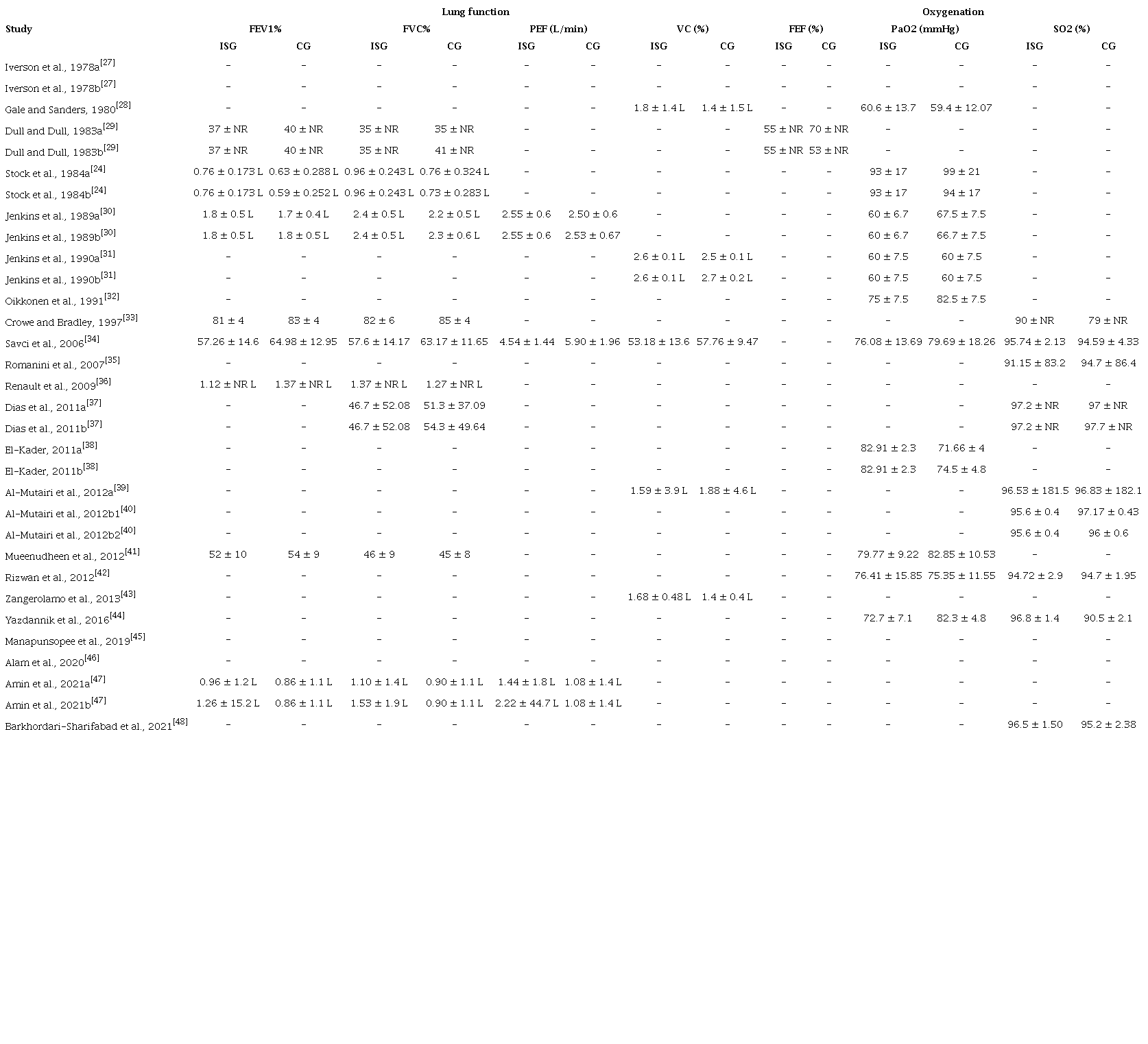
the length of ICU stay ranged from 2.61 to 6.87 days (Table 3). PaO2 ranged on average from 59.4 mmHg
to 99 mmHg[24,28], and SO2 from 79 to
97.7%[35,39].
Table 1
Characteristics of the studies included in the systematic
review.
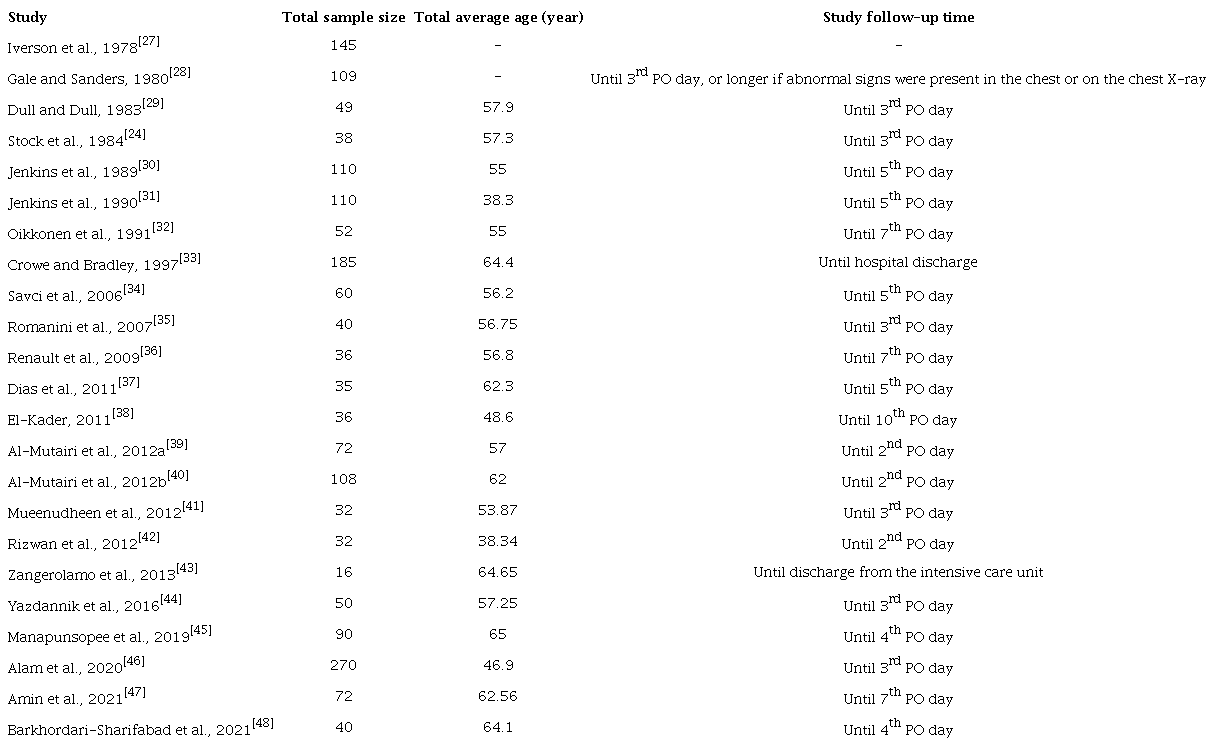
Table 2
Characteristics of the surgery and intervention.
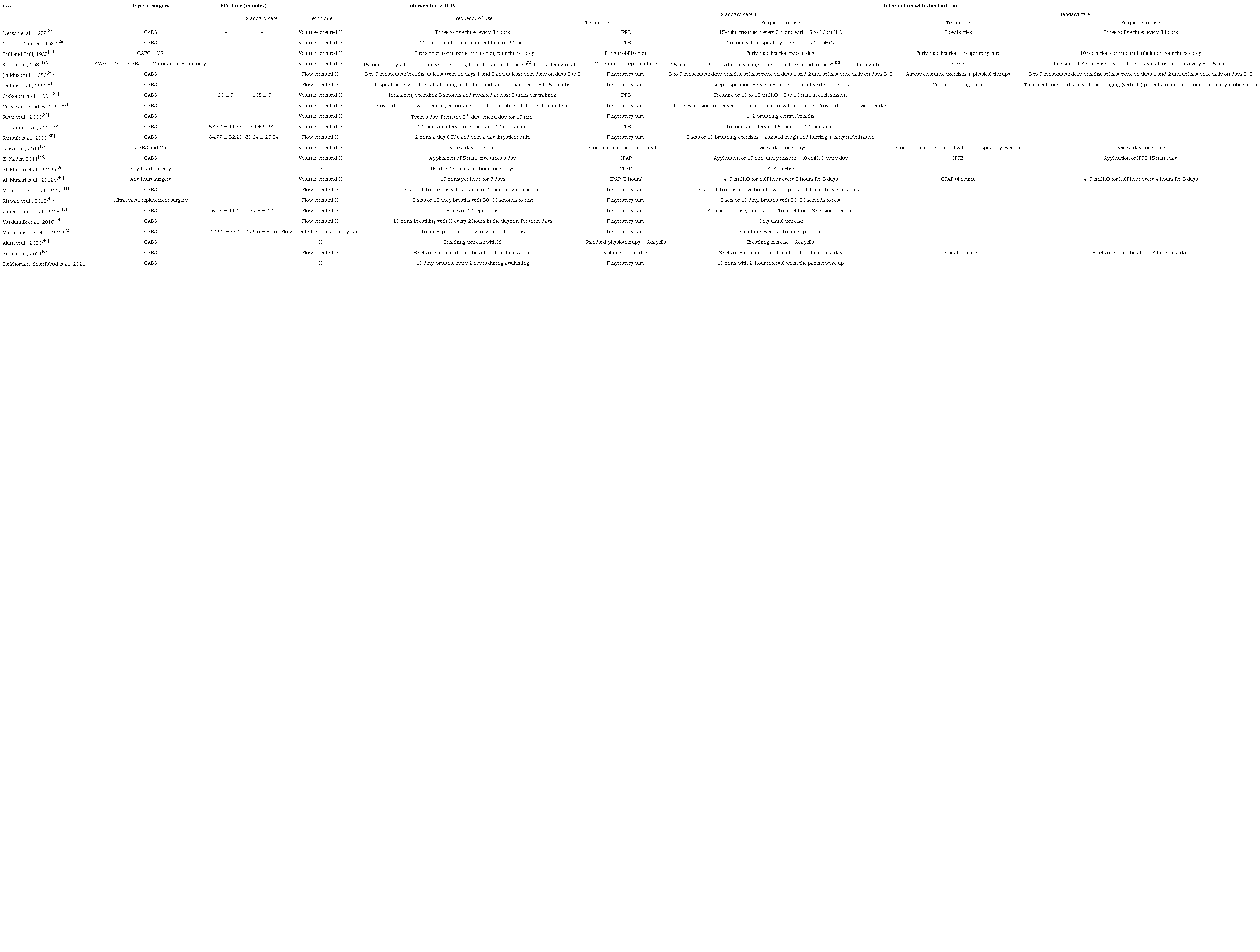
Table 3
Summary of findings for clinical outcomes.
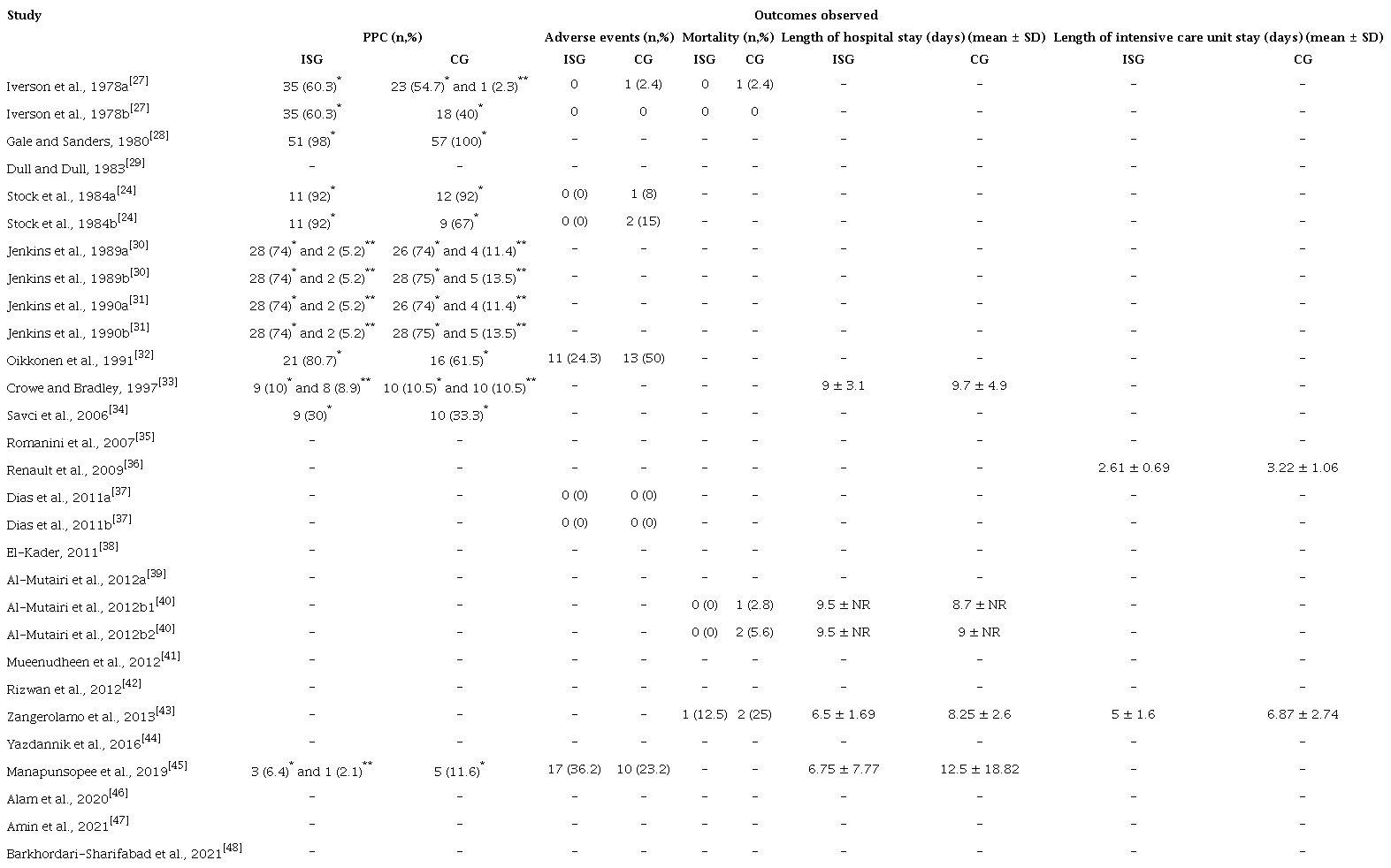 * Atelectasis** Pneumonia
* Atelectasis** Pneumonia
Considering the primary outcomes analysis, among the included studies, nine
clinical trials reported PPC rate[24,27,28,30-34,45], five reported adverse events
rate[24,27,32,37,45], and three reported mortality
rate (Table 3)[26,40,43].
With respect to the secondary outcomes analysis, four trials reported
LOS[33,40,43,45], two reported ICU
LOS[36,43], eight reported parameters of lung
function[24,29,30,33,34,36,41,47], ten reported
PaO2, nine reported SO2, and one reported reintubation
rate. No trials evaluated the use of antibiotics (which was an outcome of
interest for this review[16]).
For these continuous outcomes, results were reported differently across studies,
and we performed transformations where it was adequate. In two clinical trials,
PaO2 was converted from kilopascals to millimeters of mercury and
in one clinical trial the standard deviation was estimated using the Revman
calculator[28,31,32]. For some studies the standard deviation was also
estimated using the Revman calculator[24,37,39,47]. In one clinical trial, LOS was registered as median,
with minimum and maximum, and this was converted to mean and standard deviation
for our analysis[45,49] (Table 4). For some studies, transformations were not
possible. For instance, one clinical trial recorded forced expiratory flow
without standard deviation[29], and insufficient information to estimate the standard
deviation. Therefore, we did not pool the results in the meta-analysis. When
results were presented using different measures, such as those from studies
reporting lung function, which reported values both as a percentage of predicted
values and as absolute values in liters, then results were pooled using the
SMD.
Table 4
Summary of findings for clinical outcomes.
Assessment of Methodological Rigor
Among the included studies, in general, the PEDro score ranged from 2 to 7
points, with a mean and standard deviation of 4.5±1.1. For seven trials, the
scores were not available on the PEDro platform, therefore, the scores were
independently graded by two authors[27,39,42-44,47,48]. After the evaluation of the
two authors, three inconsistencies were observed, one on item 11 and two on item
8[27,42,44]. In
this situation, a third author was consulted to arbitrate. Considering the PEDro
scale, the following percentages of studies did not meet the criteria: on item
1, 21.7%; on item 2, 8.7%; on item 3, 95.7%; on item 4, 13%; on items 5 and 6,
100%; on item 7, 78.2%; on item 8, 52.1%; on item 9, 95.7%; and on item 11,
8.7%. On item 10, all studies met the criteria. In the classification of the
PEDro scale, 16 (69.6%) studies were judged as having “fair”[24,27,28,30,31,35,37-44,47,48], four (17.4%) as
“good”[32-34,45], three (13%) as “poor”[29,36,46], and zero (0%) as “excellent”
quality (Table 5). Considering the low
methodological rigor of the studies included in this review, we were not able to
perform sensitivity analysis including only high-quality studies.
Table 5
Quality assessment of the clinical trials using the Physiotherapy
Evidence Database (or PEDro) scale.
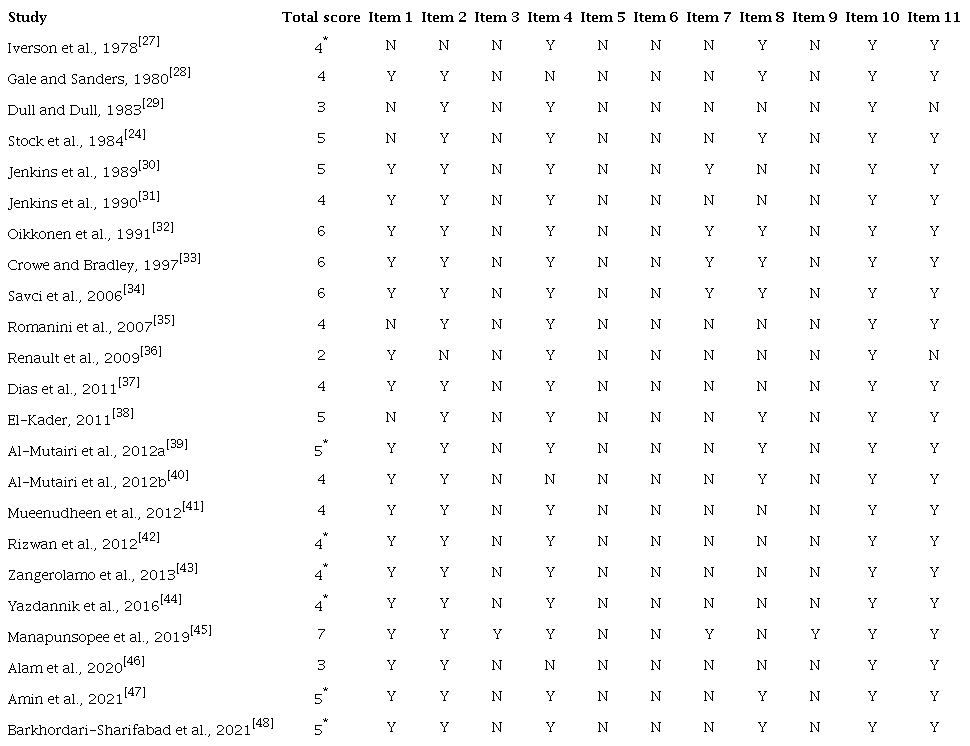 * =Score assessed by authors
* =Score assessed by authors
Comparisons of Interventions
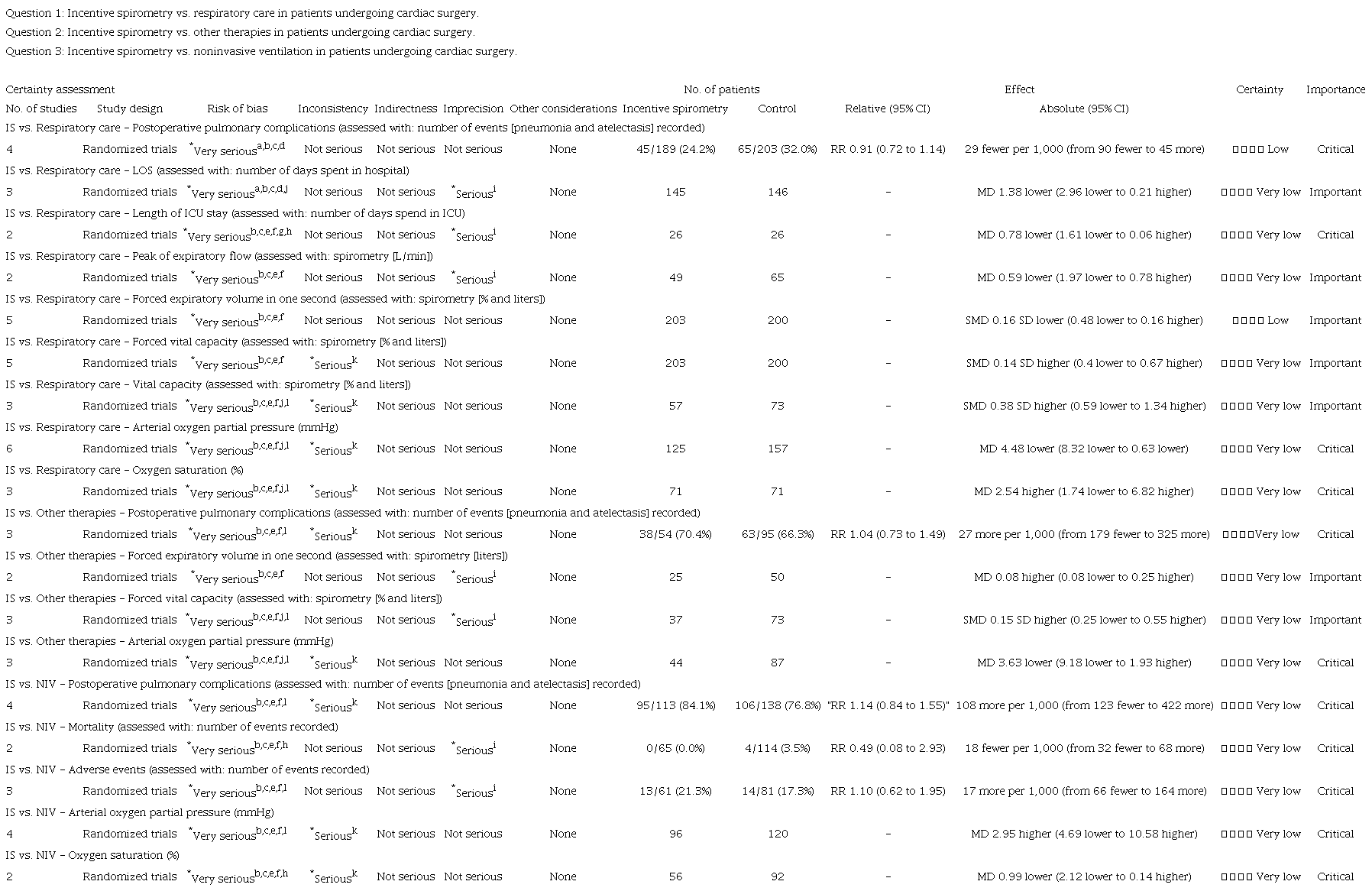
We rated the certainty of the evidence for each outcome in all comparisons using
the GRADE approach[21]. The
details of each evaluation can be found in Supplement 2.
Incentive Spirometry vs. Respiratory Care
Primary Outcomes
There may be a small difference or no difference on PPC rate between IS and
respiratory care (RR 0.91; 95% CI 0.72 to 1.14) (low certainty of evidence)
(Supplement 3 - Figure 2A). The evidence is of very low
certainty for the other primary outcomes. Only one trial evaluated the
mortality rate[43]. This
trial also used flow IS and compared its effects to the effects of
respiratory care (Supplement 3 -
Figure 2B). In the same way, only
one trial evaluated the adverse events[45]. This trial used flow IS and compared its effects
to the effects of respiratory care (Supplement 3 - Figure
2C).
Secondary Outcomes
We found low certainty of evidence that there may be a small or no difference
on FEV1 between IS and respiratory care (SMD -0.16; 95% CI -0.48 to 0.16)
(Supplement 3 - Figure 3D). The evidence is of very low
certainty for all the other secondary outcomes of this comparison. For these
outcomes, no differences in LOS (MD -1.38; 95% CI -2.96 to 0.21), length of
ICU stay (MD -0.78; 95% CI -1.61 to 0.06), PEF (MD -0.60; 95% CI -1.97 to
0.78), FVC (SMD 0.14; 95% CI -0.40 to 0.67), VC (SMD 0.38; 95% CI -0.59 to
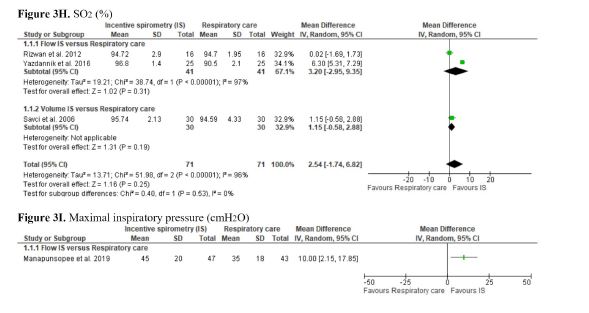
1.34), and SO2 (MD 2.54; 95% CI -1.74 to 6.82) were observed,
comparing IS and respiratory care (Supplement 3 - Figures 3A,
3B, 3C, 3E, 3F, and 3H). However, in the subgroup analysis of VC, flow IS was
superior compared to respiratory care. The Amin et al. (2021)[47] study was not included in
the PEF meta-analysis as it did not have sufficient extractable data. The
Barkhordari-Sharifabad et al. (2021)[48] study was not included in the SO2
meta-analysis as it was unclear whether it used flow-oriented IS or
volume-oriented IS.
The meta-analysis showed that IS leads to lower recovery of PaO2
than respiratory care (MD -4.48; 95% CI -8.32 to -0.63) (very low certainty
of evidence). In the subgroup analyses, flow-oriented IS was inferior to
recovery PaO2 compared to respiratory care (Supplement 3 - Figure
3G). Two trials evaluated MIP[36,45], however, only one had sufficient extractable data (Supplement 3 - Figure 3I)[45].
Incentive Spirometry vs. Other Therapies
Primary Outcomes
The evidence for the primary outcomes of IS vs. other
therapies is of very low certainty. We found no differences on PPC between
IS and other therapies (RR 1.04; 95% CI 0.73 to 1.49) (Supplement 3 - Figure
4A). Only one study evaluated adverse events (Supplement 3 - Figure 4B).
Secondary Outcomes
The evidence for the secondary outcomes is also of very low certainty. No
difference was observed between IS and other therapies regarding FEV1 (MD
0.08; 95% CI -0.08 to 0.25), FVC (SMD 0.15; 95% CI -0.25 to 0.55), and PaO2
(MD -3.63; 95% CI -9.18 to 1.93) (very low certainty of evidence) (Supplement 3 - Figures 5B, 5C,
and 5E). Only one study evaluated
PEF[30], and
another study evaluated VC (Supplement
3 - Figure 5A, 5D)[31].
Incentive Spirometry vs. NIV
Primary Outcomes
Four trials compared the effects of IS vs. NIV on PPC, and
three trials on mortality and adverse events. The evidence for the primary
outcomes of IS vs. NIV is of very low certainty. All trials
used volume-oriented IS. No differences were found between volume-oriented
IS and NIV on PPC (RR 1.14; 95% CI 0.84 to 1.55), mortality (RR 0.49; 95% CI
0.08 to 2.93), and adverse events (RR 1.10; 95% CI 0.62 to 1.95) (Supplement 3 - Figures 6A, 6B,
and 6C).
Secondary Outcomes
The evidence for secondary outcomes is also of very low certainty. No
differences were found between IS and NIV on PaO2 (MD 2.95; 95%
CI -4.69 to 10.58) or on SO2 (MD -0.99; 95% CI -2.12 to 0.14)
(Supplement 3 - Figures 7D, 7E). Only one trial compared the effects of IS and NIV
on FEV1, FVC, VC, and MIP. All trials used volume-oriented IS (Supplement 3 - Figures 7A, 7B,
7C, and 7F). A single study recorded the reintubation rate,
with zero reintubation in the IS group and one reintubation in the standard
care group[32].
DISCUSSION
To the best of our knowledge, this is the first systematic review with meta-analysis
to investigate the effects of IS exclusively in patients undergoing cardiac surgery,
performing sub-analysis to pool the studies according to the type of IS used as
respiratory care. The results showed that the use of IS was not superior to
respiratory care, other therapies, and NIV on the outcomes evaluated. On the other
hand, IS was inferior to respiratory care for recovery PaO2. In the
subgroup analysis, flow-oriented IS was inferior to respiratory care on recovery
PaO2. However, flow-oriented IS was superior to respiratory care on
VC. Overall, the methodological rigor of the clinical trials included in this review
was “fair” and the certainty of evidence ranged from “very low” to “low”.
In general, although our meta-analysis showed that IS is not different from
respiratory care, other therapies, or NIV, except for PaO2 (in IS
vs. respiratory care) for which we cannot make any positive or
negative statements about effectiveness after cardiac surgery, the majority of the
included studies present severe methodological problems and inadequate sample size.
In addition, over the years studies have investigated the effects of IS on PPC,
adverse events, and mortality after surgical procedures on the thorax, showing
different results, some in agreement with and others contrary to our
findings[11,50,51].
Our results are in line with a previous Cochrane systematic review that included
seven RCTs with a total of 592 patients to assess the effects of IS for preventing
pulmonary complications after CABG[51]. This review found no evidence of a benefit from IS in
reducing pulmonary complications and in decreasing the negative effects on pulmonary
function in patients undergoing CABG. Of note, besides including only patients that
had undergone CABG, this review is outdated and did not perform the certainty of
evidence evaluation. The inclusion of a broader and updated body of knowledge and
GRADE assessments in our review is of particular importance, as it facilitates
decision making of physiotherapists working in the frontline.
A clinical trial investigated the effects of IS after cardiac surgery in 90 patients;
47 patients were treated with flow-oriented IS + deep breathing exercise, and 43
patients received only deep breathing exercise (control group)[45]. Patients who received IS + deep
breathing exercise had no reduction in atelectasis, pneumonia, pneumothorax, and
pleural effusion. However, the control group had fewer adverse events (dyspnea)
(P-value = 0.03)[45]. On the other hand, one thing is certain, although, to date,
the clinical efficacy on PPC is not proven, IS is widely used and
investigated[52].
A preliminary trial[53] that
investigated the effectiveness of IS (flow-oriented device) on respiratory motion in
healthy subjects suggested that two weeks of respiratory training using IS is useful
for improving respiratory motion and pulmonary function. A clinical trial[54] with 260 surgical patients
(non-cardiac patients) showed that IS (flow-oriented and volume-oriented) and
diaphragmatic breathing exercise better preserve pulmonary function and diaphragm
excursion. If these findings are also demonstrated in patients after cardiac surgery
using IS, this method will represent an easily accessible and low-cost device to be
used in the treatment of these patients.
A broad range of different types of IS devices and treatment protocols were used in
the studies included in this review. However, we were unable to determine which of
them is more effective. Although we planned to perform other subgroup analyses, we
were also unable to identify whether the type of surgery, the severity of the
disease, or details of the intervention, such as frequency, duration, and time the
intervention started could influence the effect of intervention. Due to the
heterogeneity of the RCTs regarding the combinations of interventions and
comparisons, different comparisons had to be made, and we were only able to perform
a few comprehensive meta-analyses. Therefore, the precision of effect estimates was
jeopardized.
Furthermore, due to several methodological limitations in the included studies and
conflicting results, further well-designed trials, with long-term follow-up, and
which report the rate of core outcome results, such as PPC, adverse events,
mortality, lung function, and LOS, are needed, as well as in the ICU. New RCTs
should be standardized to provide more homogeneous and reliable data to properly
compare the results. For example, studies should evaluate the same IS device,
delivered using standardized protocols, for treating similar types of surgeries.
Of note, some limitations should be underscored. In addition, there is a need for
clear and complete reporting of outcome data for the interventions being compared.
All trials included in this review had important methodological limitations.
Although blinding of participants and personnel may be very difficult from a
practical perspective, several other factors such as the lack of blinding of outcome
assessors, loss to follow-up, and the absence of intention-to-treat analyses were
common methodological limitations in the available studies.
Overall, due to the serious risk of bias and imprecision, the overall certainty of
the available evidence is very low, and several questions persist. Thus, it is
unclear whether IS used alone or in combination with other therapies is effective
when compared to other interventions used alone or in combination.
Moreover, although some studies concluded that IS was safe, the available information
on adverse events was insufficient to perform a comprehensive meta-analysis that
could provide more accurate results on the safety of IS. The evidence is currently
insufficient to support or refute the routine use of IS after cardiac surgeries. The
results of the six ongoing RCTs are necessary to provide more precise and reliable
information on which to base further trials and protocols, and to guide clinical
decision-making processes on the use of IS after cardiac surgeries.
We believe the strengths of this systematic review include transparency, rigid
methods, assessment of the quality of evidence for each outcome, and extensive and
careful searches, with no restrictions on language or publication date. We searched
the gray literature database and ongoing studies and performed a rigorous critical
assessment of the current body of evidence. Furthermore, the assessment of certainty
of evidence using the GRADE approach is paramount in pointing out limitations in
current trials and upon which to base further high quality RCTs. Another strong
point of this review was the separate analysis by the type of IS (flowor
volume-oriented IS), when possible. This high-quality review underlines that there
is an urgent need to conduct high-quality RCTs in this field.
Limitations
We consider as limitations of this systematic review the inclusion of biased
clinical trials, such as those with lack of blinding of outcome assessors, or
without adequate randomization; substantial heterogeneity among studies that
made them unsuitable for meta-analysis; or studies with small samples that do
not allow us to provide accurate estimates of the effects. As another
limitation, we were unable to explain the heterogeneity in the meta-analysis of
the PaO2 and SO2 outcomes.
CONCLUSION
This meta-analysis revealed that IS was not superior to standard respiratory care for
PPC and clinical outcomes, therefore its use should not be widely recommended until
high-quality further studies are performed to ensure this clinical guidance.
Apéndices
Supplement 1
Search strategy
Supplement 2
Assessment of certainty of evidence.
Supplement 3
Meta-analyses of the results
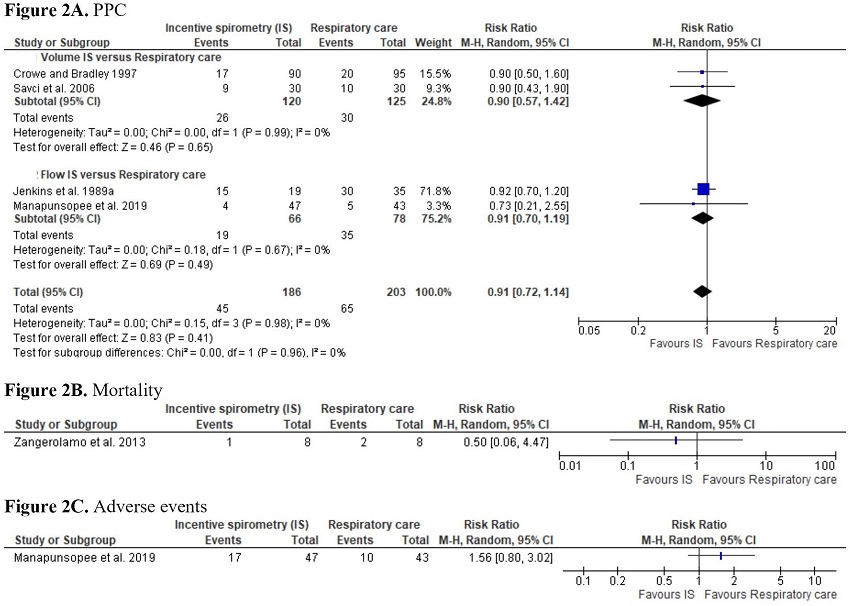 Fig. 2
Meta-analyses of the results for the primary outcomes of incentive
spirometry vs. respiratory care. CI=confidence interval;
PPC=postoperative pulmonary complications
Fig. 2
Meta-analyses of the results for the primary outcomes of incentive
spirometry vs. respiratory care. CI=confidence interval;
PPC=postoperative pulmonary complications
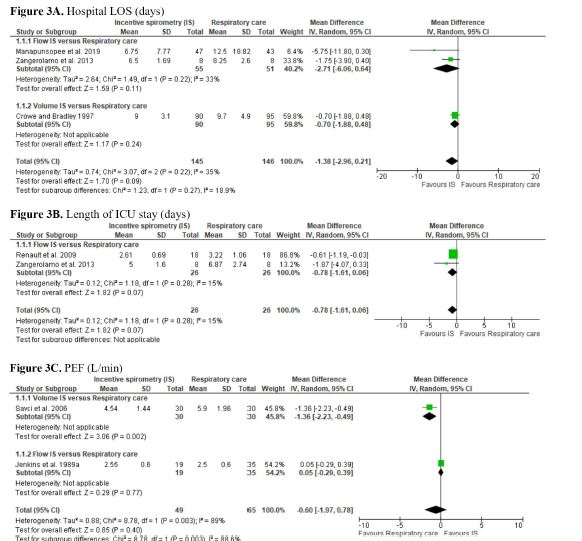 Fig. 3
Meta-analyses of the results for the secondary outcomes of incentive
spirometry vs. respiratory care. CI=confidence interval; FEV1=forced
expiratory volume in one second; FVC=forced vital capacity;
ICU=intensive care unit; LOS=length of stay; PaO2=partial
pressure of oxygen; PEF=peak of expiratory flow; SD=standard
deviation; SO2=oxygen saturation; VC=vital capacity
Fig. 3
Meta-analyses of the results for the secondary outcomes of incentive
spirometry vs. respiratory care. CI=confidence interval; FEV1=forced
expiratory volume in one second; FVC=forced vital capacity;
ICU=intensive care unit; LOS=length of stay; PaO2=partial
pressure of oxygen; PEF=peak of expiratory flow; SD=standard
deviation; SO2=oxygen saturation; VC=vital capacity
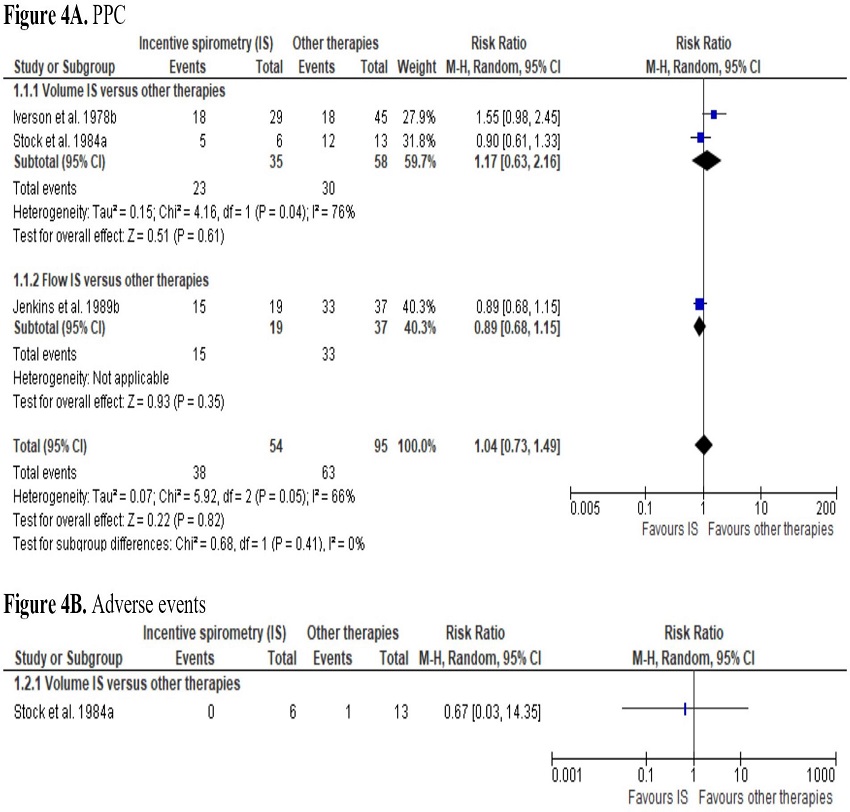 Fig. 4
Meta-analyses of the results for the primary outcomes of incentive
spirometry vs. other therapies. CI=confidence interval;
PPC=postoperative pulmonary complications
Fig. 4
Meta-analyses of the results for the primary outcomes of incentive
spirometry vs. other therapies. CI=confidence interval;
PPC=postoperative pulmonary complications
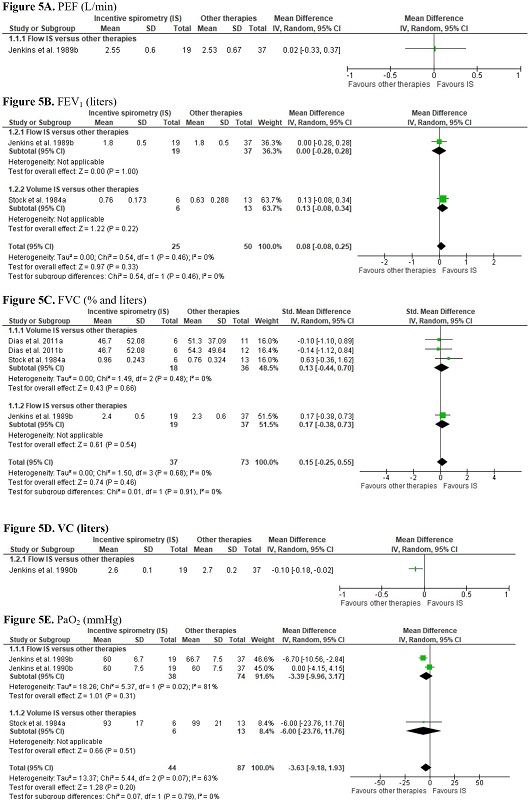 Fig. 5
Meta-analyses of the results for the secondary outcomes of incentive
spirometry vs. other therapies. CI=confidence interval; FEV1=forced
expiratory volume in one second; FVC=forced vital capacity;
PaO2=partial pressure of oxygen; PEF=peak of expiratory flow;
SD=standard deviation; VC=vital capacity
Fig. 5
Meta-analyses of the results for the secondary outcomes of incentive
spirometry vs. other therapies. CI=confidence interval; FEV1=forced
expiratory volume in one second; FVC=forced vital capacity;
PaO2=partial pressure of oxygen; PEF=peak of expiratory flow;
SD=standard deviation; VC=vital capacity
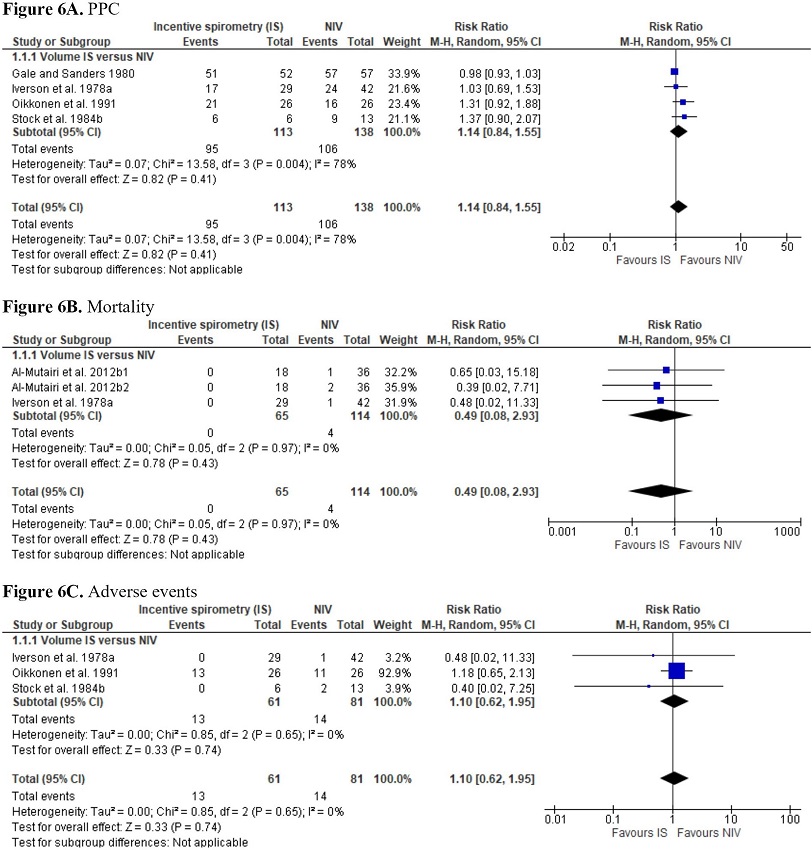 Fig. 6
Meta-analyses of the results for the primary outcomes of incentive
spirometry vs. noninvasive ventilation (NIV). CI=confidence
interval; PPC=postoperative pulmonary complications
Fig. 6
Meta-analyses of the results for the primary outcomes of incentive
spirometry vs. noninvasive ventilation (NIV). CI=confidence
interval; PPC=postoperative pulmonary complications
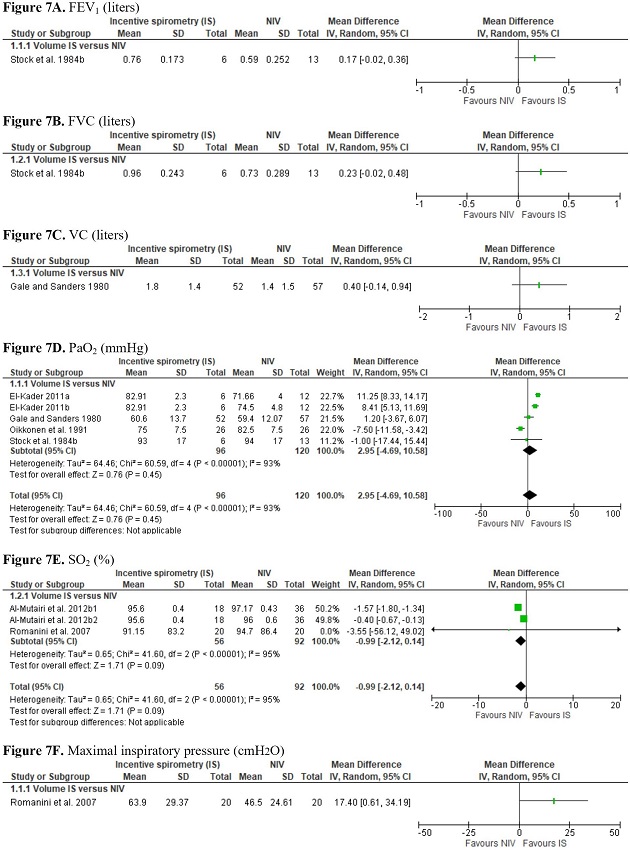 Fig. 7
Meta-analyses of the results for the secondary outcomes of incentive
spirometry vs. noninvasive ventilation (NIV). CI=confidence
interval; FEV₁=forced expiratory volume in one second; FVC=forced
vital capacity; PaO2=partial pressure of oxygen;
SD=standard deviation; SO2=oxygen saturation; VC=vital
capacity
Fig. 7
Meta-analyses of the results for the secondary outcomes of incentive
spirometry vs. noninvasive ventilation (NIV). CI=confidence
interval; FEV₁=forced expiratory volume in one second; FVC=forced
vital capacity; PaO2=partial pressure of oxygen;
SD=standard deviation; SO2=oxygen saturation; VC=vital
capacity
REFERENCES
Health AIo. Elective surgery waiting times 2017-18. Canberra: AIHW;
2019.
Mejia OAV, Lisboa LAF, Caneo LF, Arita ET, Brandão CMA, Dias RR, et
al. Analysis of >100,000 cardiovascular surgeries performed at the heart
institute and a new era of outcomes. Arq Bras Cardiol. 2020;114(4):603-12.
doi:10.36660/abc.20190736.
Lee JJ, Park NH, Lee KS, Chee HK, Sim SB, Kim MJ, et al. Projections
of demand for cardiovascular surgery and supply of surgeons. Korean J Thorac
Cardiovasc Surg. 2016;49(Suppl 1):S37-S43.
doi:10.5090/kjtcs.2016.49.S1.S37.
Gomes WJ, Moreira RS, Zilli AC, Bettiati LC Jr, Figueira FAMDS, D'
Azevedo SSP, et al. The Brazilian registry of adult patient undergoing
cardiovascular surgery, the BYPASS project: results of the first 1,722 patients.
Braz J Cardiovasc Surg. 2017;32(2):71-6. Erratum in: Braz J Cardiovasc Surg.
2017;32(5):442. doi:10.21470/1678-9741-2017-0053.
Chen X, Hou L, Zhang Y, Liu X, Shao B, Yuan B, et al. The effects of
five days of intensive preoperative inspiratory muscle training on postoperative
complications and outcome in patients having cardiac surgery: a randomized
controlled trial. Clin Rehabil. 2019;33(5):913-22.
doi:10.1177/0269215519828212.
Patra C, Chamaiah Gatti P, Panigrahi A. Morbidity After cardiac
surgery under cardiopulmonary bypass and associated factors: a retrospective
observational study. Indian Heart J. 2019;71(4):350-5.
doi:10.1016/j.ihj.2019.07.004.
Akintoye E, Sellke F, Marchioli R, Tavazzi L, Mozaffarian D. Factors
associated with postoperative atrial fibrillation and other adverse events after
cardiac surgery. J Thorac Cardiovasc Surg. 2018;155(1):242-51.e10.
doi:10.1016/j.jtcvs.2017.07.063.
Taboada M, Rey R, Martínez S, Soto-Jove R, Mirón P, Selas S, et al.
Reintubation in the ICU following cardiac surgery: is it more difficult than
first-time intubation in the operating room?: a prospective observational study.
Eur J Anaesthesiol. 2020;37(1):25-30.
doi:10.1097/EJA.0000000000001019.
Curiel-Balsera E, Mora-Ordoñez JM, Castillo-Lorente E,
Benitez-Parejo J, Herruzo-Avilés A, Ravina-Sanz JJ, et al. Mortality and
complications in elderly patients undergoing cardiac surgery. J Crit Care.
2013;28(4):397-404. doi:10.1016/j.jcrc.2012.12.011.
Ball L, Costantino F, Pelosi P. Postoperative complications of
patients undergoing cardiac surgery. Curr Opin Crit Care. 2016;22(4):386-92.
doi:10.1097/MCC.0000000000000319.
Overend TJ, Anderson CM, Lucy SD, Bhatia C, Jonsson BI, Timmermans
C. The effect of incentive spirometry on postoperative pulmonary complications:
a systematic review. Chest. 2001;120(3):971-8.
doi:10.1378/chest.120.3.971.
Restrepo RD, Wettstein R, Wittnebel L, Tracy M. Incentive
spirometry: 2011. Respir Care. 2011;56(10):1600-4.
doi:10.4187/respcare.01471.
Eltorai AEM, Baird GL, Eltorai AS, Healey TT, Agarwal S, Ventetuolo
CE, et al. Effect of an incentive spirometer patient reminder after coronary
artery bypass grafting: a randomized clinical trial. JAMA Surg.
2019;154(7):579-88. doi:10.1001/jamasurg.2019.0520.
Sullivan KA, Churchill IF, Hylton DA, Hanna WC. Use of incentive
spirometry in adults following cardiac, thoracic, and upper abdominal surgery to
prevent post-operative pulmonary complications: a systematic review and
meta-analysis. Respiration. 2021;100(11):1114-27.
doi:10.1159/000517012.
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred
reporting items for systematic reviews and meta-analyses: the PRISMA statement.
PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097.
Santos EC, Pinto ACPN, Macedo JRFF, Lunardi AC. Effect of incentive
spirometry after cardiac surgery: protocol for a systematic review. Fisioter
Bras. 2020;21(1):117-25. doi:10.33233/fb.v21i1.3625.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and
mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
doi:10.1186/s13643-016-0384-4.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M.
Reliability of the PEDro scale for rating quality of randomized controlled
trials. Phys Ther. 2003;83(8):713-21.
Gonzalez GZ, Moseley AM, Maher CG, Nascimento DP, Costa LDCM, Costa
LO. Methodologic quality and statistical reporting of physical therapy
randomized controlled trials relevant to musculoskeletal conditions. Arch Phys
Med Rehabil. 2018;99(1):129-36. doi:10.1016/j.apmr.2017.08.485.
Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et
al. Grading quality of evidence and strength of recommendations. BMJ.
2004;328(7454):1490. doi:10.1136/bmj.328.7454.1490.
GRADEpro GDT: GRADEpro Guideline Development Tool [Software].
McMaster University, 2020 (developed by Evidence Prime, Inc.). Available from
gradepro.org.
Review Manager 5 (RevMan 5) [Computer program]. Version 5.3.
Copenhagen: Nordic Cochrane Centre, Cochrane, 2014.
Murad MH, Wang Z, Chu H, Lin L. When continuous outcomes are
measured using different scales: guide for meta-analysis and interpretation.
BMJ. 2019;364:k4817. doi:10.1136/bmj.k4817.
Stock MC, Downs JB, Cooper RB, Lebenson IM, Cleveland J, Weaver DE,
et al. Comparison of continuous positive airway pressure, incentive spirometry,
and conservative therapy after cardiac operations. Crit Care Med.
1984;12(11):969-72. doi:10.1097/00003246-198411000-00010.
Higgins JPT, Eldridge S, Li T (editors). Chapter 23: Including
variants on randomized trials. In: Higgins JPT, Thomas J, Chandler J, Cumpston
M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews
of Interventions version 6.2 (updated February 2021).
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch
VA (editors). Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed.
Chichester UK: The Cochrane Collaboration and John Wiley & Sons Ltd., 2019.
703 p.
Iverson LI, Ecker RR, Fox HE, May IA. A comparative study of IPPB,
the incentive spirometer, and blow bottles: the prevention of atelectasis
following cardiac surgery. Ann Thorac Surg. 1978;25(3):197-200.
doi:10.1016/s0003-4975(10)63521-7.
Gale GD, Sanders DE. Incentive spirometry: its value after cardiac
surgery. Can Anaesth Soc J. 1980;27(5):475-80.
doi:10.1007/BF03007047.
Dull JL, Dull WL. Are maximal inspiratory breathing exercises or
incentive spirometry better than early mobilization after cardiopulmonary
bypass? Phys Ther. 1983;63(5):655-9. doi:10.1093/ptj/63.5.655.
Jenkins SC, Soutar SA, Loukota JM, Johnson LC, Moxham J.
Physiotherapy after coronary artery surgery: are breathing exercises necessary?
Thorax. 1989;44(8):634-9. doi:10.1136/thx.44.8.634.
Jenkins SC, Soutar SA, Loukota JM, Johnson LC, Moxham J. A
comparison of breathing exercises, incentive spirometry and mobilisation after
coronary artery surgery. Physiother Theory Pract. 1990;6:117-26.
doi:10.3109/09593989009037789.
Oikkonen M, Karjalainen K, Kähärä V, Kuosa R, Schavikin L.
Comparison of incentive spirometry and intermittent positive pressure breathing
after coronary artery bypass graft. Chest. 1991;99(1):60-5.
doi:10.1378/chest.99.1.60.
Crowe JM, Bradley CA. The effectiveness of incentive spirometry with
physical therapy for high-risk patients after coronary artery bypass surgery.
Phys Ther. 1997;77(3):260-8. doi:10.1093/ptj/77.3.260.
Savcı S, Sakınç S, İnce DI, Arikan H, Can Z, Buran Y, et al. Active
cycle of breathing techniques and incentive spirometer in coronary artery bypass
graft surgery. Fizyoter Rehabil. 2006;17(2):61-9.
Romanini W, Muller AP, Carvalho KA, Olandoski M, Faria-Neto JR,
Mendes FL, et al. The effects of intermittent positive pressure and incentive
spirometry in the postoperative of myocardial revascularization. Arq Bras
Cardiol. 2007;89(2):94-9, 105-10.
doi:10.1590/s0066-782x2007001400006.
Renault JA, Costa-Val R, Rosseti MB, Houri Neto M. Comparison
between deep breathing exercises and incentive spirometry after CABG surgery.
Rev Bras Cir Cardiovasc. 2009;24(2):165-72.
doi:10.1590/s0102-76382009000200012.
Dias CM, Vieira Rde O, Oliveira JF, Lopes AJ, Menezes SL, Guimarães
FS. Three physiotherapy protocols: effects on pulmonary volumes after cardiac
surgery. J Bras Pneumol. 2011;37(1):54-60.
doi:10.1590/s1806-37132011000100009.
El-Kader SMA. Blood gases response to different breathing modalities
in phase I of cardiac rehabilitation program after coronary artery bypass graft.
Eur J Gen Med. 2011;8(2):85-91. doi.org/10.29333/ejgm/82706.
Almutairi F, Fallows S, Mason-Whitehead E. Continuous positive
airway pressure (cpap) had better outcomes when compared with incentive
spirometry (IS) to re-open collapse alveoli after cardiac surgery: randomized
study. Am J Respir Crit Care Med. 2012;185:A4869.
doi:10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A4869.
Al-Mutairi FH, Fallows SJ, Abukhudair WA, Islam BB, Morris MM.
Difference between continuous positive airway pressure via mask therapy and
incentive spirometry to treat or prevent post-surgical atelectasis. Saudi Med J.
2012;33(11):1190-5.
Mueenudheen TP, Moiz JA, Gupta VP. A comparative study on the
effects of incentive spirometry and deep breathing exercise on pulmonary
functions after uncomplicated coronary artery bypass grafting surgery. Indian J
Physiother Occup Ther. 2012;6(2):63-7.
Rizwan A, Jalwan J, Mukherjee S. To compare the immediate effect of
deep breathing exercise and incentive spirometry on ABG after mitral valve
replacement surgery. Indian J Physiother Occup Ther.
2012;6(4):12-7.
Zangerolamo TB, Barrientos TG, Baltieri L, Moreno M,
Pazzianotto-Forti EM. Effects of flow-oriented incentive spirometry after
myocardial revascularization. Rev Bras Cardiol.
2013;26(3):180-5.
Yazdannik A, Bollbanabad HM, Mirmohammadsadeghi M, Khalifezade A.
The effect of incentive spirometry on arterial blood gases after coronary artery
bypass surgery (CABG). Iran J Nurs Midwifery Res. 2016;21(1):89-92.
doi:10.4103/1735-9066.174761.
Manapunsopee S, Thanakiatpinyo T, Wongkornrat W, Chuaychoo B,
Thirapatarapong W. Effectiveness of incentive spirometry on inspiratory muscle
strength after coronary artery bypass graft surgery. Heart Lung Circ.
2020;29(8):1180-6. doi:10.1016/j.hlc.2019.09.009.
Alam M, Hussain S, Shehzad MI, Mushtaq A, Rauf A, Ishaq S. Comparing
the effect of incentive spirometry with acapella on blood gases in physiotherapy
after coronary artery bypass graft. Cureus. 2020;12(2):e6851.
doi:10.7759/cureus.6851.
Amin R, Alaparthi GK, Samuel SR, Bairapareddy KC, Raghavan H,
Vaishali K. Effects of three pulmonary ventilation regimes in patients
undergoing coronary artery bypass graft surgery: a randomized clinical trial.
Sci Rep. 2021;11(1):6730. doi:10.1038/s41598-021-86281-4.
Zerang F, Amouzeshi A, Barkhordari-Sharifabad M. Comparison of the
effect of incentive spirometry and deep breathing exercises on hemodynamic
parameters of patients undergoing coronary artery bypass graft surgery: a
clinical trial. J Vasc Nurs. 2022;40(3):134-9.
doi:10.1016/j.jvn.2022.08.002.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance
from the median, range, and the size of a sample. BMC Med Res Methodol.
2005;5:13. doi:10.1186/1471-2288-5-13.
Freitas ER, Soares BG, Cardoso JR, Atallah AN. Incentive spirometry
for preventing pulmonary complications after coronary artery bypass graft.
Cochrane Database Syst Rev. 2007;(3):CD004466. Update in: Cochrane Database Syst
Rev. 2012;9:CD004466. doi:10.1002/14651858.CD004466.pub2.
Freitas ER, Soares BG, Cardoso JR, Atallah ÁN. Incentive spirometry
for preventing pulmonary complications after coronary artery bypass graft.
Cochrane Database Syst Rev. 2012;2012(9):CD004466.
doi:10.1002/14651858.CD004466.pub3.
Eltorai AEM, Baird GL, Pangborn J, Eltorai AS, Antoci V Jr, Paquette
K, et al. Financial impact of incentive spirometry. Inquiry.
2018;55:46958018794993. doi:10.1177/0046958018794993.
Kotani T, Akazawa T, Sakuma T, Nagaya S, Sonoda M, Tanaka Y, et al.
Effects of incentive spirometry on respiratory motion in healthy subjects using
cine breathing magnetic resonance imaging. Ann Rehabil Med. 2015;39(3):360-5.
doi:10.5535/arm.2015.39.3.360.
Alaparthi GK, Augustine AJ, Anand R, Mahale A. Comparison of
diaphragmatic breathing exercise, volume and flow incentive spirometry, on
diaphragm excursion and pulmonary function in patients undergoing laparoscopic
surgery: a randomized controlled trial. Minim Invasive Surg. 2016;2016:1967532.
doi:10.1155/2016/1967532.
Notas
Notas
This study was carried out at the Universidade Federal do Amapá, Macapá, Amapá,
Brazil.
Notas
No financial support.
Declaración de intereses
No conflict of interest.
Notas de autor
Correspondence Address: Elinaldo da Conceição dos Santos, https://orcid.org/0000-0002-4039-2980, Department of Biological
and Health Sciences, Universidade Federal do Amapá, Rodovia Josmar Chaves Pinto,
S/N, Jardim Marco Zero, Macapá, AP, Brazil, Zip Code: 68902-280, E-mail:
drelinaldo@yahoo.com.br