BRIEF COMMUNICATION
Intravital Microscopy Evidence That Methylene Blue Should Be a Vasopressor-Sparing Agent in Sepsis Vasoplegia

Intravital Microscopy Evidence That Methylene Blue Should Be a Vasopressor-Sparing Agent in Sepsis Vasoplegia
Brazilian Journal of Cardiovascular Surgery, vol. 39, no. 3, e20230066, 2024
Sociedade Brasileira de Cirurgia Cardiovascular
Received: 18 February 2023
Accepted: 04 September 2023
Funding
Funding source: CAPES
Contract number: 2017/21539-7
Contract number: 2018/23718-8
Funding
Funding source: FAPESP
Contract number: 2019/21721-4
Funding statement: Financial support: This study was funded by the CAPES (Christiane Becari 2017/21539-7, 2018/23718-8); Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (M. Barbosa 2019/21721-4); Conselho Nacional de Desenvolvimento Científico e Tecnológico, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo.
ABSTRACT: Microvasculature failure is expected in sepsis and at higher amine concentrations. Therefore, special attention focused individually on microcirculation is needed. Here, we present that methylene blue can prevent leukocytes from adhering to the endothelium in a rat model of lipopolysaccharide-induced endotoxemia. As hypothesis evidence, an intravital microscopy image is presented.
Keywords: Methylene Blue, Microcirculation, Microvessels, Endothelium, Lipopolysaccharides.
INTRODUCTION
Gomes[1] first described vasoplegic syndrome in heart surgery patients have been undergoing treatment with methylene blue (MB) for it. Evora et al (1996)[2] were the ones who suggested the use of MB for treatment. In 1996, Andrade et al.[3] first documented this therapeutic approach in heart surgery patients. MB successfully treats vasopressor-refractory septic shock vasoplegia by inhibiting endothelial nitric oxide and improving responsiveness to amines. However, only one relevant study has explored the microcirculatory effects of MB[4].
Intravital Microscopy Method
This study involved adult male Hannover rats under controlled conditions approved by the Committee on Ethics in Animal Experimentation of the Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo (2/2015). We anesthetized the animals, exteriorized the mesentery, and examined postcapillary venules with diameters of 10-18 micrometers. We evaluated leukocytes adhering to the endothelium within 10-micrometer venule lengths. Furthermore, we considered leukocytes adhered for up to 30 seconds for the microcirculatory protective effect (Figures 1 and 2).
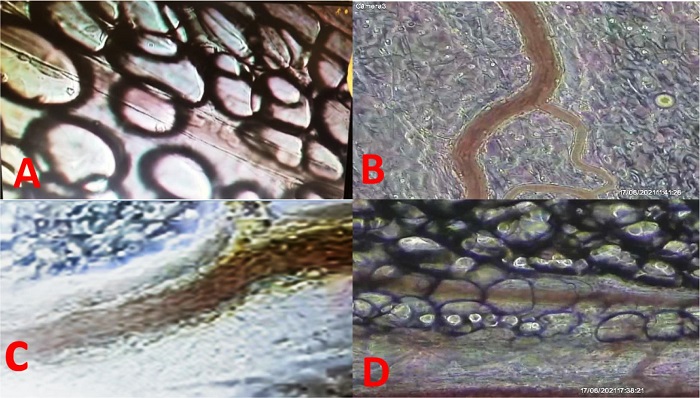
Fig. 1
Methylene blue (MB) inhibiting neutrophil leukocyte rolling/adhesion after lipopolysaccharide (LPS) intravenous dose. (A) Postcapillary venules of saline group (saline at zero and 15 min); (B) postcapillary venules of LPS group (LPS at zero and saline at 15 min); (C) postcapillary venules of only MB (MB at zero and saline at 15 min); (D) postcapillary venules of MB after LPS doses (LPS at zero and MB at 15 min). # Intra peritoneal image of postcapillary venules. (A) Control (roller mean = 52.4, adhesion mean = 1.3); (B) LPS + salina (roller mean = 816, adhesion mean = 9.4); (C) LPS + MB (roller mean = 28.1, adhesion mean = 3.2); (D) MB + LPS (roller mean = 76.4, adhesion mean = .6).
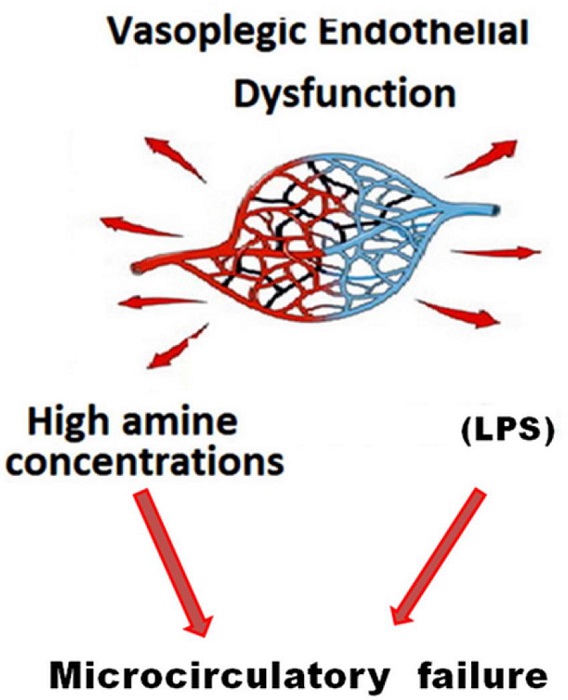
Fig. 2
Schematic representation of microcirculatory damage consequent to lipopolysaccharide (LPS) and high doses of amine.
The technique is particularly useful for studying microcirculation. It allows researchers to observe blood flow through capillaries and venules, providing insights into blood perfusion, oxygen exchange, and interactions between blood cells and vessel walls.
COMMENTS
We state that the medical literature underestimates the importance of cyclic guanosine monophosphate. Combining three concepts could yield better results against high mortality rates in critically ill patients: (1) using “broad-spectrum vasopressors”, (2) employing vasopressor-sparing strategies, and (3) protecting microcirculation.
MB should serve as a vasopressor-sparing agent. We need progressively minor concentrations of amines to maintain blood pressure (around 65 mmHg). Additionally, using high amine concentrations independently of blood pressure becomes reasonable. We anticipate the disclosure, hoping that new research groups interested in the subject will emerge. Therefore, we firmly believe that the briefly discussed concepts will incorporate as paradigms in vasodilatory shock treatment.
“Microcirculatory protection” is an old concept. It assumes that microvasculature failure is unavoidable even with arterial pressure under control, with increasing amine concentrations. Therefore, special attention focused individually on microcirculation is needed. The image presented, corresponding to the record of an experiment, has been checked and reproduced in our laboratory. With the hope of motivating different research groups, we decided the hypothesis disclosure. Chances are that the briefly discussed hypothetical concepts can be incorporated as paradigms in treating vasodilatory shock[5-7].

REFERENCES
Gomes WJ, Carvalho AC, Palma JH, Gonçalves I Jr, Buffolo E. Vasoplegic syndrome: a new dilemma. J Thorac Cardiovasc Surg. 1994;107(3):942-3.
Evora PR, Ribeiro PJ, de Andrade JC. Methylene blue administration in SIRS after cardiac operations. Ann Thorac Surg. 1997;63(4):1212-3. doi: 10.1016/s0003-4975(97)00198-7.
Andrade JCS, Batista Filho ML, Evora PRB, et al. Methylene blue administration in the treatment of the vasoplegic syndrome after cardiac surgery. Rev Bras Cir Cardiovasc. 1996;11:107-14.
Nantais J, Dumbarton TC, Farah N, Maxan A, Zhou J, Minor S, Lehmann C. Impact of methylene blue in addition to norepinephrine on the intestinal microcirculation in experimental septic shock. Clin Hemorheol Microcirc. 2014;58(1):97-105. doi: 10.3233/CH-141874.
Evora PRB, Braile DM. "Vasopressor Support Sparing Strategies": a Concept to be Incorporated as a Paradigm in the Treatment of Vasodilatory Shock. Braz J Cardiovasc Surg. 2019;34(1):I-II. doi: 10.21470/1678-9741-2019-0600.
Buckley MS, Barletta JF, Smithburger PL, Radosevich JJ, Kane-Gill SL. Catecholamine Vasopressor Support Sparing Strategies in Vasodilatory Shock. Pharmacotherapy. 2019;39(3):382-398. doi: 10.1002/phar.2199.
Evora PRB, Soares ROS, Bassetto S, Auxiliadora-Martins M, Silva FLDS, Basile A Filho. After Thirty Years, We Still Cannot Understand Why Methylene Blue is not a Reference to Treat Vasoplegic Syndrome in Cardiac Surgery. Braz J Cardiovasc Surg. 2021;36(3):406-11. doi: 10.21470/1678-9741-2021-0955. Erratum in: Braz J Cardiovasc Surg. 2022 Mar 10;37(1):144.
Notes
Author notes
Correspondence Address: Paulo Roberto B. Evorahttps://orcid.org/0000-0001-9631-946X Bandeirantes Av., 3900, Ribeirão Preto, SP, Brazil, Zip Code: 14049-900, E-mail: prbevora@fmrp.usp.br
Conflict of interest declaration