ORIGINAL ARTICLE
Received: 16 June 2024
Accepted: 18 July 2024
DOI: https://doi.org/10.21470/1678-9741-2024-0202
ABSTRACT
Introduction: Previous studies found that patients with a history of cancer either have similar outcomes or face an increased risk of early morbidity following cardiac surgery. However, the applicability of these findings to clinical practice may be constrained by the heterogeneity of cancer patients. To refine our understanding, this study focuses specifically on the in-hospital outcomes of patients with non-metastatic malignant solid tumors (NMST) undergoing coronary artery bypass grafting (CABG).
Methods: Patients who underwent CABG were identified in National/Nationwide Inpatient Sample from Q4 2015-2020. Exclusion criteria included age < 18 years, concomitant procedures, and other malignancies. A 1:3 propensity-score matching was employed to address differences in demographics, socioeconomic status, primary payer status, hospital characteristics, comorbidities, and admission status between patients with and without NMST. In-hospital outcomes after CABG were evaluated.
Results: There were 2,139 patients with NMST who underwent CABG and who were matched to 6,580 out of 164,351 patients without NMST. Patients with and without NMST had comparable mortality (2.25% vs. 2.16%, P=0.80). However, NMST patients have a higher risk of hemorrhage/hematoma (63.48% vs. 58.27%, P<0.01) and a higher rate of transfer out (28.75% vs. 25.36%, P<0.01). In addition, patients with NMST had longer time from admission to operation (P<0.01), a longer length of stay (P<0.01), and higher hospital charges (P<0.01).
Conclusion: Patients with NMST have comparable short-term outcomes after CABG, except for a higher risk of postoperative bleeding. Thus, CABG could be performed safely for NMST patients, despite long-term prognosis of these patients may require further investigation.
Keywords: Coronary Artery Bypass, Thoracic Surgery, Neoplasms, Risk, Mortality, Morbidity, Length of Stay.
INTRODUCTION
Coronary artery disease (CAD), affecting an estimated 16.5 million Americans, stands as a primary cause of mortality in the United States of America[1]. As a prevalent coronary revascularization treatment of CAD, coronary artery bypass grafting (CABG) is performed in over 200,000 patients annually in the country[2].
Over the past two decades, there has been a significant increase in both the number and life expectancy of cancer survivors[3,4]. This trend has led to a corresponding rise in the incidence of comorbid cancer among patients undergoing CABG[5]. The decision-making process for determining CABG candidacy can be intricate in patients with a history of cancer. These individuals often have a higher risk profile due to systemic illness, potential reductions in life expectancy, and the impacts of cancer therapies on their overall health. Furthermore, the physiological stress induced by major surgeries like CABG can influence oncological outcomes by modifying the immune response[6].
Previous research suggests that patients with a history of cancer either have outcomes similar to those without cancer or face an increased risk of early morbidity but not mortality following cardiac surgery[5,7,8]. However, the applicability of these findings to clinical practice may be constrained by the heterogeneity of cancer patients in these studies. To refine our understanding, this study focuses specifically on the in-hospital outcomes of patients with non-metastatic malignant solid tumors (NMST) undergoing CABG. The National/Nationwide Inpatient Sample (NIS) dataset, the largest national inpatient registry in the United States of America, was used to provide a robust, population-based analysis.
METHODS
Data Source
The NIS database from the last quarter of 2015 to 2020 was used. Patients who underwent CABG were identified using the International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS) codes of 0210xxx. Patients with NMST were further selected by International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes of C00-C14, C15-C26, C30-C41, C43-C49, C4A, C50-C58, C60-C76, C7A, D46.9, E31.21, E31.22, and E31.23 by the Elixhauser Comorbidity[9].
Exclusion criteria included those who have age < 18 years, concomitant procedures including aortic valve replacement (ICD-10-PCS 02RFxxx) and mitral valve replacement (ICD-10-PCS 02RGxxx), and other malignancy including lymphoma (ICD-10-CM C81-C86, C88, C90.0, C90.2, C90.3, C96.0, C96.2, C96.4, C96.9, C96.A, C96.Z, D47.Z9), leukemia (ICD-10-CM C90.1, C91-C95), solid tumor without metastasis in situ (ICD-10-CM D00-D07, D09), and metastatic cancer (ICD-10-CM C77-C79, C7B, C80.0)[9]. Patients with and without NMST were stratified into two cohorts in this study.
Preoperative Factors
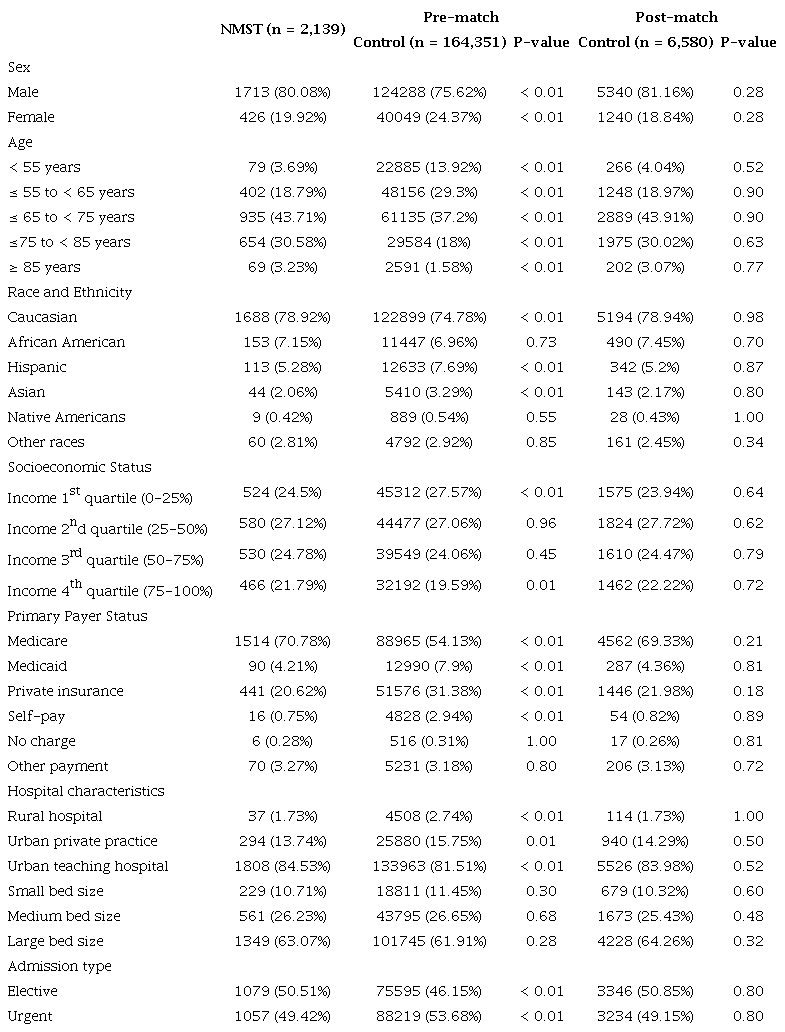
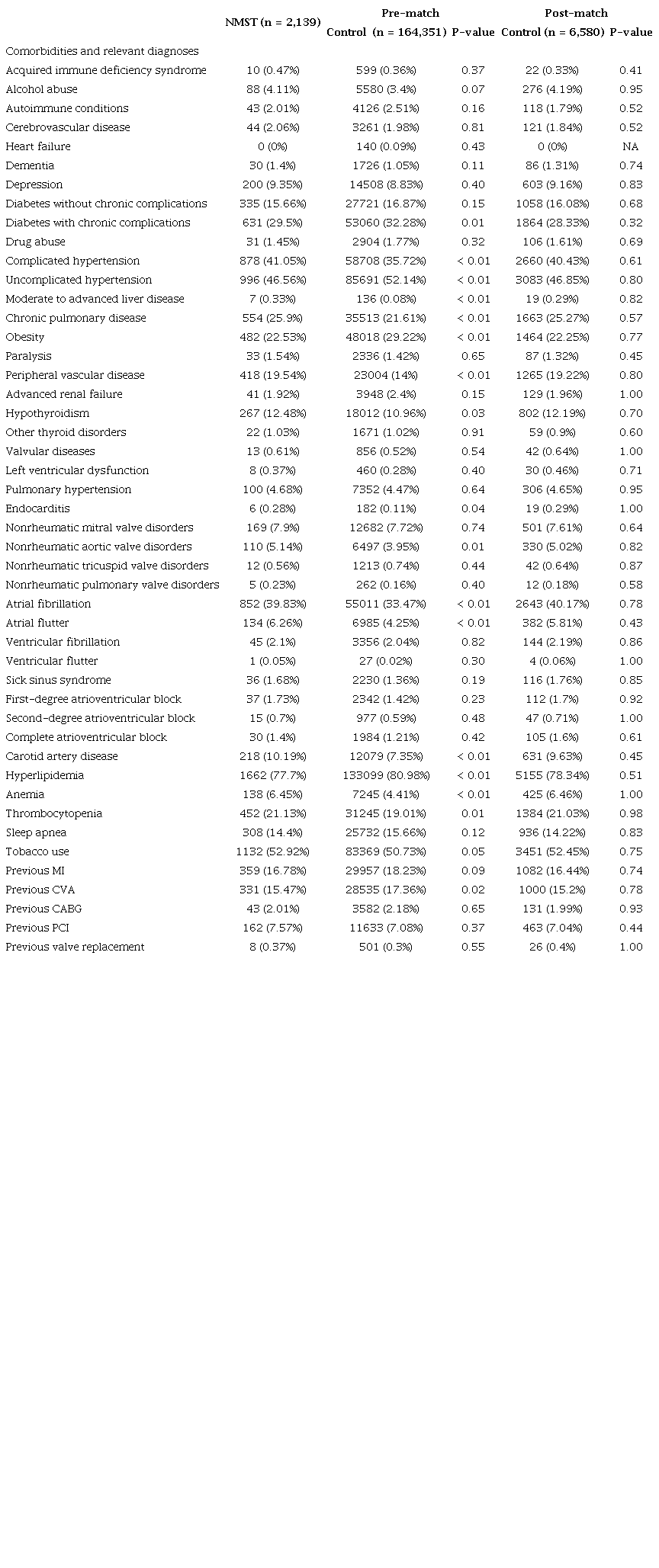
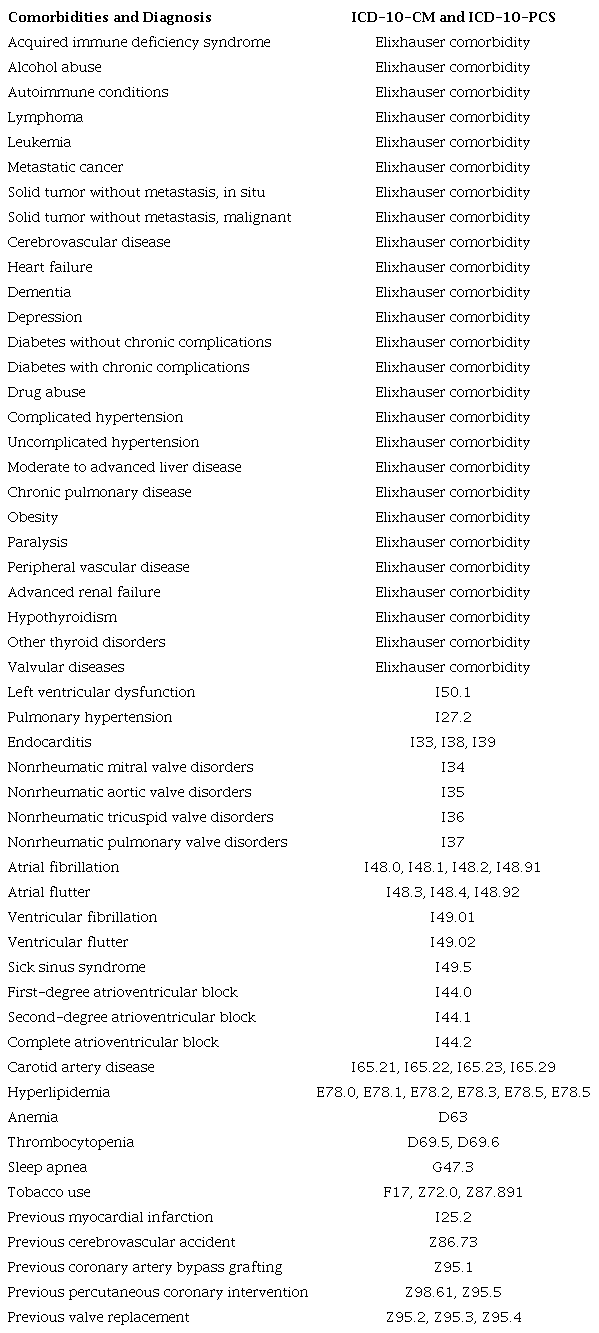
Preoperative factors in patients with and without NMST are shown in Table 1 and Table 2. Table 1 lists demographics (sex, age, and race and ethnicity), socioeconomic status, primary payer status, hospital characteristics, transfer status, and admission status. The average household income from the patient's ZIP code was estimated. Patients were then stratified into four quartiles based on the income of their neighborhood. Hospital characteristics included hospital bed size, location, and teaching status. American Hospital Association's yearly survey, hospital location, and teaching status of the hospital were used to stratify the hospital bed sizes into small, medium, and large. Table 2 includes the patient’s comorbidities and relevant diagnoses. Comorbidities were identified by Elixhauser measure and by ICD-10-CM codes as listed in Table S1[9].
Comparing demographics, primary payer status, hospital characteristics, and admission type between patients with and without NMST who underwent CABG before and after 1:3 propensity-score matching.
Comparing comorbidities and relevant diagnoses between patients with and without NMST who underwent CABG before and after 1:3 propensity-score matching.
The International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) and International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS) codes for comorbidities and relevant diagnosis.
Postoperative Outcomes
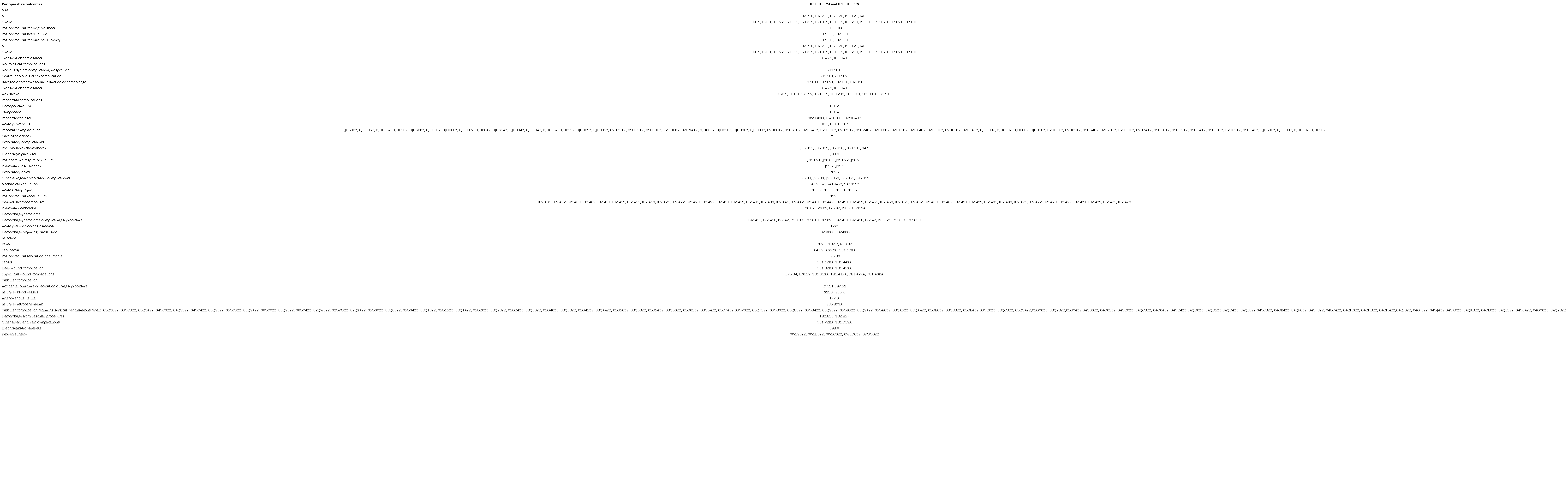
In-hospital outcomes after CABG were examined (Table 3). The outcomes included mortality, major adverse cardiovascular event (MACE), myocardial infarction (MI), stroke, transient ischemic attack (TIA), neurological complications, pericardial complications, pacemaker implantation, cardiogenic shock, respiratory complications, mechanical ventilation, acute kidney injury (AKI), postprocedural renal failure, venous thromboembolism (VTE), pulmonary embolism (PE), hemorrhage/hematoma, infection, sepsis, deep wound complication, superficial wound complication, vascular complication, diaphragmatic paralysis, and reopen surgery for bleeding control. Moreover, transfer out to other facilities, time from admission to operation, hospital length of stay (LOS), and total hospital charge were compared between patients with and without NMST. The ICD-10-CM/PCS codes used to define the outcomes are shown in Table S2.
The International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) and International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS) codes for perioperative outcomes.
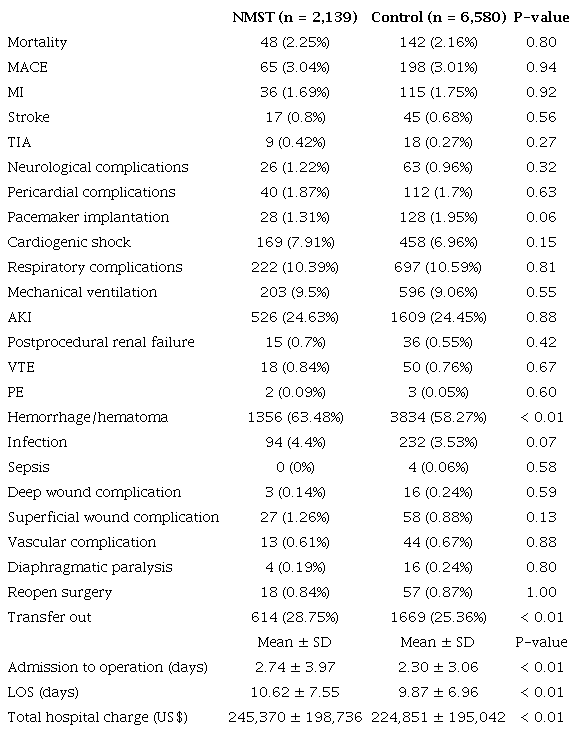
Comparing in-hospital outcomes between patients with and without NMST who underwent CABG after 1:3 propensity-score matching.
Ethics Approval
This study was exempt from the IRB approval by The George Washington University as it analyzed retrospective, deidentified NIS data.
Statistical Analysis
Fisher's exact test was used to compare the preoperative factors between patients with and without NMST. To account for differences in the preoperative factors between the NMST and non-NMST patients as well as a significant difference in their sample sizes, a 1:3 ratio (NMST: non-NMST) propensity-score matching was carried out using the Greedy Matching algorithm with a 2% caliper. After the propensity-score matching, Fisher's exact test was used to examine binary postoperative outcomes while two-tailed independent t-tests were used to compare continuous variables.
All statistical analyses were conducted using SAS, version 9.4. A P-value < 0.05 was considered statistically significant. The authors had full access to the NIS dataset and took responsibility for the integrity of all analyses. This is a retrospective study that used a de-identified NIS dataset. As a result, it was exempted from The George Washington University Institutional Review Board (or IRB) review.
RESULTS
There were 2,139 patients with NMST who underwent CABG from the last quarter of 2015 to 2020. During the same time, there were 164,351 patients without NMST who underwent CABG, and 6,580 of them were matched to those with NMST.
Table 1 summarizes demographics, primary payer status, hospital characteristics, and admission type between patients with and without NMST who underwent CABG. Compared to those without NMST, patients with NMST were more likely to be males (80.08% vs. 75.62%, P<0.01), have age > 75 years (75-85 years, 43.71% vs. 37.20%, P<0.01; > 85 years, 3.23% vs. 1.58%, P<0.01), be Caucasian (78.92% vs. 74.78%, P<0.01), have income at the highest quartile (75-100%) (21.79% vs. 19.59%, P=0.01), use Medicare (70.78% vs. 54.13%, P<0.01), stay in an urban teaching hospital (84.53% vs. 81.51%, P<0.01), and under elective admission (50.51% vs. 46.15%, P<0.01). In contrast, patients with NMST were less likely to be females (19.92% vs. 24.37%, P<0.01), have age < 65 years (55-65 years, 18.79% vs. 29.30%, P<0.01; < 55 years, 3.69% vs. 13.92%, P<0.01), be Hispanic (5.28% vs. 7.69%, P<0.01) or Asian (2.06% vs. 3.29%, P<0.01), have income at the lowest quartile (0-25%) (24.50% vs. 27.57%, P<0.01), use Medicaid (4.21% vs. 7.90%, P<0.01), private insurance (20.62% vs. 31.38%, P<0.01), or self-pay (0.75% vs. 2.94%, P<0.01) as the primary payer, stay in a rural hospital (1.73% vs. 2.74%, P<0.01) or an urban private practice (13.74% vs. 15.75%, P=0.01), or under urgent admission (49.42% vs. 53.68%, P<0.01). All preoperative differences were matched by 1:3 propensity-score matching.
Table 2 shows the comparison of comorbidities and relevant diagnoses between patients with and without NMST who underwent CABG. Patients with NMST were more likely to have complicated hypertension (41.05% vs. 35.72%, P<0.01), moderate to advanced liver disease (0.33% vs. 0.08%, P<0.01), chronic pulmonary disease (25.90% vs. 21.61%, P<0.01), peripheral vascular disease (19.54% vs. 14.00%, P<0.01), hypothyroidism (12.48% vs. 10.96%, P=0.03), endocarditis (0.28% vs. 0.11%, P=0.04), nonrheumatic aortic valve disorders (5.14% vs. 3.95%, P=0.01), atrial fibrillation (39.83% vs. 33.47%, P<0.01), atrial flutter (6.26% vs. 4.25%, P<0.01), anemia (6.45% vs. 4.41%, P<0.01), and thrombocytopenia (21.13% vs. 19.01%, P=0.01). In contrast, patients with NMST were less likely to have diabetes with chronic complications (29.50% vs. 32.28%, P=0.01), uncomplicated hypertension (46.56% vs. 52.14%, P<0.01), obesity (22.53% vs. 29.22%, P<0.01), hyperlipidemia (77.70% vs. 80.98%, P<0.01), or previous cerebrovascular accident (15.47% vs. 17.36%, P=0.02). All differences in the comorbidities and relevant diagnoses between NMST and non-NMST patients were matched by propensity-score matching.
Table 3 summarizes the in-hospital outcomes between patients with and without NMST who underwent CABG after 1:3 propensity-score matching. Patients with and without NMST had comparable mortality (2.25% vs. 2.16%, P=0.80). However, NMST patients have a higher risk of hemorrhage/hematoma (63.48% vs. 58.27%, P<0.01) and a higher rate of transfer out (28.75% vs. 25.36%, P<0.01). In addition, patients with NMST had longer time from admission to operation (2.74 ± 3.97 vs. 2.30 ± 3.06 days, P<0.01), longer LOS (10.62 ± 7.55 vs. 9.87 ± 6.96 days, P<0.01), and higher total hospital charges (US$245,370 ± 198,736 vs. US$224,851 ± 195,042, P<0.01). Other in-hospital outcomes, including the rates of MACE, MI, stroke, TIA, neurological complications, pericardial complications, pacemaker implantation, cardiogenic shock, respiratory complications, mechanical ventilation, AKI, postprocedural renal failure, VTE, PE, infection, sepsis, deep wound complication, superficial wound complication, vascular complication, diaphragmatic paralysis, and reopen surgery, were not different between patients with and without NMST.
DISCUSSION
The study conducted a population-based analysis of the in-hospital outcomes of patients with NMST who underwent CABG. It was found that patients with NMST had comparable mortality and morbidity rates, except for a higher risk of hemorrhage/hematoma. Additionally, NMST patients exhibited a higher rate of transfer out, an extended duration from admission to operation, longer LOS, and increased total hospital charges.
A small case series study by Zhang et al.[8] demonstrated that CABG is an effective treatment for CAD patients with malignancy. Previous population-based studies indicated that cancer patients undergoing CABG generally had comparable outcomes, with the exception of a higher incidence of postoperative major bleeding[5,10]. This aligns with the findings of the current study, where NMST patients were at an increased risk of hemorrhage/hematoma after CABG, while other in-hospital outcomes were similar to those of non-NMST patients.
Several factors may contribute to the heightened risk of bleeding in patients with NMST. Open surgery can prompt the release of pro-inflammatory cytokines that can disrupt fibrinogen and platelet function[11]. These disturbances can be associated with altered coagulative states in NMST patients[11]. Additionally, the introduction of new anticoagulation and antifibrinolytic drugs for certain cancer patients might play a role[12,13]. While these drugs can reduce ischemic risk, they may also increase the risk of bleeding in some cancer patients[12,13]. Furthermore, the use of specific anti-cancer therapies, such as selective estrogen receptor modulators in breast cancer and androgen deprivation therapy in prostate cancer, could lead to elevated bleeding risk[12,13].
Despite the increased risk of bleeding, it is important to note that in-hospital mortality, cardiac complications, and other organ system complications were not elevated in NMST patients. This observation can be valuable for preoperative risk stratification, suggesting that CABG can be relatively safe for NMST patients, despite their long-term prognosis is still needed in future studies.
Additionally, in NMST patients, a significant delay was observed from admission to operation, even after adjusting for all preoperative factors. This delay could arise from the need for preoperative stabilization, considering their potential elevated risk profile and systemic illness. Moreover, the evaluation and decision-making process for CABG in NMST patients could be more complex, which could contribute to the postponement of surgical intervention. This delay, coupled with a higher rate of complications in NMST patients, may result in prolonged LOS and, consequently, increased total hospital charges.
Limitations
This study has several limitations to acknowledge. Firstly, as an administrative database, the NIS does not have detailed data for the malignancy, such as tumor, node, and metastasis (or TNM) staging, cancer grade, or the use of chemotherapy, radiation therapy, and/or immunotherapy. Additionally, the NIS lacks information on various factors that could influence revascularization outcomes, including ejection fraction, specifics of coronary segments, stenosis diameter, lesion presence, coronary artery dominance, and small vessel disease[14,15]. This lack of data also precludes the calculations of surgical risk scores, such as the Society of Thoracic Surgeons score[16] or the European System for Cardiac Operative Risk Evaluation (or EuroSCORE) score[17]. Furthermore, the NIS database is limited to in-hospital outcomes, where follow-up after discharge is not recorded. This restricts the analysis of this study to short-term outcomes and does not provide insights into the long-term prognosis of NMST patients after CABG.
CONCLUSION
In summary, this study conducted a population-based analysis to compare the in-hospital outcomes of CABG between patients with and without NMST. It was found that patients with NMST had comparable mortality and morbidity rates, with the exception of a higher risk of hemorrhage/hematoma. In addition, NMST patients had a higher rate of transfer out, longer time from admission to operation, longer LOS, and increased total hospital charges. Therefore, this study can aid in preoperative risk stratification for patients with NMST; CABG could be performed relatively safely for these patients while additional attention should be given to postoperative bleeding, and the long-term prognosis of NMST patients may require further investigation.
ACKNOWLEDGMENTS
The authors acknowledge Dr. Richard Amdur, PhD, for giving statistical support for this project.
REFERENCES
Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics-2018 update: a report from the American heart association. Circulation. 2018;137(12):e67-e492. doi:10.1161/CIR.0000000000000558. Erratum in: Circulation. 2018;137(12):e493. doi:10.1161/CIR.0000000000000573.
Jacobs JP, Shahian DM, D'Agostino RS, Jacobs ML, Kozower BD, Badhwar V, et al. The society of thoracic surgeons national database 2017 annual report. Ann Thorac Surg. 2017;104(6):1774-81. doi:10.1016/j.athoracsur.2017.10.014.
Leong DP, Cirne F, Aghel N, Baro Vila RC, Cavalli GD, Ellis PM, et al. Cardiac interventions in patients with active, advanced solid and hematologic malignancies: JACC: CardioOncology state-of-the-art review. JACC CardioOncol. 2023;5(4):415-30. doi:10.1016/j.jaccao.2023.05.008.
Pushparaji B, Donisan T, Balanescu DV, Park JK, Monlezun DJ, Ali A, et al. Coronary revascularization in patients with cancer. Curr Treat Options Cardiovasc Med. 2023;25(6):143-58. doi:10.1007/s11936-023-00982-9.
Guha A, Dey AK, Kalra A, Gumina R, Lustberg M, Lavie CJ, et al. Coronary artery bypass grafting in cancer patients: prevalence and outcomes in the United States. Mayo Clin Proc. 2020;95(9):1865-76. doi:10.1016/j.mayocp.2020.05.044.
Onuma AE, Zhang H, Gil L, Huang H, Tsung A. Surgical stress promotes tumor progression: a focus on the impact of the immune response. J Clin Med. 2020;9(12):4096. doi:10.3390/jcm9124096.
Lorusso R, Vizzardi E, Johnson DM, Mariscalco G, Sciatti E, Maessen J, et al. Cardiac surgery in adult patients with remitted or active malignancies: a review of preoperative screening, surgical management and shortand long-term postoperative results. Eur J Cardiothorac Surg. 2018;54(1):10-8. doi:10.1093/ejcts/ezy019.
Zhang MK, Zhang HW, Wu QY, Xue H, Fan LX. Coronary artery bypass grafting in patients with malignancy: a single-institute case series of eight patients. BMC Surg. 2022;22(1):359. doi:10.1186/s12893-022-01805-7.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8-27. doi:10.1097/00005650-199801000-00004.
Marui A, Kimura T, Nishiwaki N, Mitsudo K, Komiya T, Hanyu M, et al. Comparison of five-year outcomes of coronary artery bypass grafting versus percutaneous coronary intervention in patients with left ventricular ejection fractions≤50% versus >50% (from the CREDO-Kyoto PCI/CABG registry cohort-2). Am J Cardiol. 2014;114(7):988-96. doi:10.1016/j.amjcard.2014.07.007.
Weledji EP. The role of cytokines in enhanced recovery after surgery. IJS Short Reports. 2021;6(1):e21. doi:10.1097/SR9.0000000000000021.
Guha A, Dey AK, Jneid H, Addison D. Acute coronary syndromes in cancer patients. Eur Heart J. 2019;40(19):1487-90. doi:10.1093/eurheartj/ehz267.
Mangano DT, Miao Y, Vuylsteke A, Tudor IC, Juneja R, Filipescu D, et al. Mortality associated with aprotinin during 5 years following coronary artery bypass graft surgery. JAMA. 2007;297(5):471-9. doi:10.1001/jama.297.5.471.
Authors/Task Force members; Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European society of cardiology (ESC) and the European association for cardio-thoracic surgery (EACTS)developed with the special contribution of the European association of percutaneous cardiovascular interventions (EAPCI). Eur Heart J. 2014;35(37):2541-619. doi:10.1093/eurheartj/ehu278.
Zheng Z, Xu B, Zhang H, Guan C, Xian Y, Zhao Y, et al. Coronary artery bypass graft surgery and percutaneous coronary interventions in patients with unprotected left main coronary artery disease. JACC Cardiovasc Interv. 2016;9(11):1102-11. doi:10.1016/j.jcin.2016.03.039.
ACSD Operative Risk Calculator - STS [Internet]. [cited 2023 Oct 23]. Available from: https://www.sts.org/resources/acsd-operative-risk-calculator
Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734-44; discussion 744-5. doi:10.1093/ejcts/ezs043.
Notes
Author notes
Correspondence Address: Renxi Li https://orcid.org/0000-0003-1691-6278, The George Washington University School of Medicine and Health Sciences, 2300 I St NW, Washington, D.C., United States of America, Zip Code: 20052, E-mail: renxili@gwu.edu
Conflict of interest declaration
