ABSTRACT: We present a case of left atrial thrombus mimicking myxoma after orthotopic heart transplantation. Multimodality imaging established the diagnosis of atrial myxoma, and the patient was treated accordingly, but the definite diagnosis after surgical excision and histology showed left atrial thrombus. This report demonstrates the limitations of multimodality diagnosis in tumors with features highly suggestive of an atrial myxoma.
Keywords: Left Atrial Myxoma, Heart Transplantation, Atrial Mass, Atrial Thrombus.
EDUCATIONAL FORUM
Left Atrial Thrombus Mimicking Myxoma After Orthotopic Heart Transplantation: Is the Multimodality Imaging Always Sufficient?
Sociedade Brasileira de Cirurgia Cardiovascular
Received: 23 September 2024
Accepted: 06 October 2024
Differentiation between thrombus and masses in the atria is challenging. Identification of intracardiac masses on noninvasive imaging is clinically important because it determines and guides the treatment for the structure.
Left atrial cardiac myxoma is the most common primary cardiac tumor, representing 20% to 40% of intracardiac masses. The most common location for myxomas is the left atrium, attached to the atrial septum at the fossa ovalis, however they may be found in all four chambers of the heart[1].
Another important cardiac mass is intracardiac thrombus. In rare situations, a thrombus may organize and attach to the atrial septum and have a similar appearance as other cardiac masses[2]. Cardiac transplant patients are at increased risk for these complications as chronic immunosuppression increases the risk of malignancy, and various other factors often predispose them to thrombus formation. However, the correct diagnosis can sometimes be difficult with certainty only being achieved after histology examination[3].
In this educational forum, we report a case of left atrial thrombus 16 years after orthotopic heart transplantation mimicking myxoma.
A 60-year-old patient underwent orthotopic heart transplantation in 2008 for end-stage heart failure secondary to dilated cardiomyopathy. The donor heart was from an 18-year-old man who had died as a result of brain injury after a road traffic accident. After heart transplantation, the recipient had two episodes of acute rejection which were treated with pulse steroid therapy, and he was diagnosed with cardiac allograft vasculopathy with non-significant coronary artery disease. Immunosuppression treatment consisted of prednisone, everolimus, and tacrolimus. In 2021, he underwent right nephrectomy due to Grawitz carcinoma. Neither the donor nor the recipient had a family history of cardiac tumors. In the year 2024, in a follow-up echocardiography, a rapidly growing left atrial mass measuring 39 × 28 × 31 mm located at the posterior atrial wall was diagnosed for the first time. Later, the patient underwent multimodality imaging where the diagnosis of left atrial myxoma was established (Figure 1). On the contrary, histology confirmed the diagnosis of organized left atrial thrombus. Based on the preoperative evaluation, the tumor was treated as left atrial myxoma, and the patient underwent urgent redo-surgery with the use of aortobicaval cardiopulmonary bypass. The pedicle of the left atrial tumor was attached to the posterior atrial wall, on the recipient’s site. The tumor was completely excised, and a suture was placed on the tumor’s stalk on the atrial wall (Figures 2A, 2B). The postoperative course was uneventful and on postoperative day eight, he was discharged. Histology examination showed organized left atrial thrombus (Figures 2C, 2D).
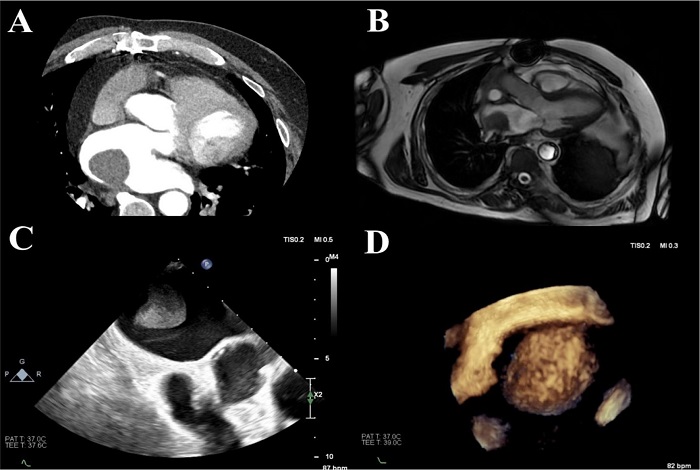
Fig. 1
Multimodality imaging showing the left atrial tumor. A) Computed tomography. B) Magnetic resonance imaging. C) 2D-transesophageal echocardiography. D) 3D-transesophageal echocardiography.
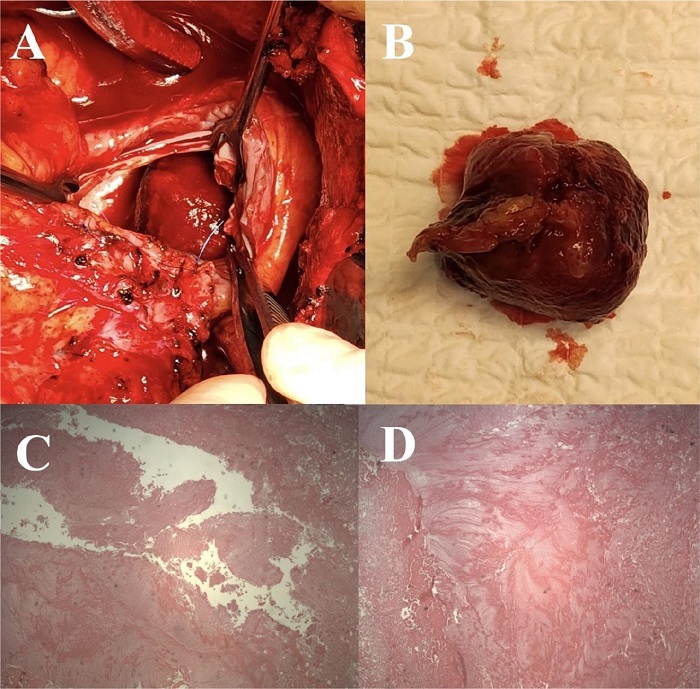
Fig. 2
A) Intraoperative view of the tumor. B) Tumor after resection. C and D) Histology showing the organized left atrial thrombus.
An informed consent was signed from the patient to present this report.
A. Is multimodality imaging always sufficient in the differential diagnosis of left atrial thrombus mimicking myxoma?
Question A. We herein report a case of a patient with a cardiac mass where multimodality imaging was insufficient to unequivocal diagnosis. The established diagnosis was posttransplant left atrial myxoma, and the patient was treated accordingly and underwent urgent surgical resection. The definite diagnosis after histology examination was organized left atrial thrombus. This report demonstrates the limitations of multimodality imaging, where in tumors with features highly suggestive of an atrial myxoma, it is insufficient to provide the correct diagnosis.
To our knowledge, there are very rare prior similar cases. Hale A et al.[2] and Neuman Y et al.[4] presented similar cases where the definite diagnosis was established after pathological examination. On the other hand, Baumwol J et al.[3] presented a case series of post-cardiac transplantation atrial masses (one case with atrial myxoma and two cases with organized atrial thrombus), where preoperative multimodality imaging established an accurate diagnosis, and the patients were treated accordingly.
One feature of this case that may have favored the diagnosis of thrombus over myxoma on noninvasive imaging is the rapid appearance and growth of the mass. Rapid growth is more commonly associated with thrombus but have been seen in myxomas, growth rate can range from 1.3 to 6.9 mm/month[5,6].
Typical treatment for myxomas includes surgical excision to prevent serious complications such as embolization and mitral valve obstruction[1], and based on the preoperative diagnosis of atrial myxoma, our patient underwent urgent surgical excision.
Thrombus formation as a complication of orthotopic heart transplantation is considered uncommon and classically related to biatrial technique[7,8]. Nevertheless, left atrial thrombus following bicaval anastomosis, as in our case, has seldom been described. Benedicio AM et al.[9] reported an incidence of atrial thrombosis after bicaval technique of 6% in their sample with female predominance. A similar case report was also reported by Fardman A et al.[10].
Remaining sutures, enlarged left atrium, history of atrial fibrillation, and immunosuppressive therapy may play a role in thrombus formation[10].
According to the literature, the diagnosis of posttransplant left atrial thrombosis is made in asymptomatic patients during routine follow-up echocardiographic or computed tomography examination[9,10]. In our case, the patient was asymptomatic, and the diagnosis was made during a routine follow-up echocardiographic examination. Systemic surveillance after heart transplantation may have a crucial role in the early diagnosis and treatment of this potentially devastating complication.
Treatment options include anticoagulation or cardiac surgery[8]. Our patient underwent an urgent redo surgery with thrombus excision. At the time of the diagnosis, he didn’t receive any antithrombotic or anticoagulation treatment. He was discharged on aspirin treatment.
Differentiation between thrombus and masses in the atria is challenging. Our case emphasizes the insufficiency of advanced multimodality imaging techniques to provide accurate diagnosis in tumors with features highly suggestive of an atrial myxoma. The patient underwent 3D- transesophageal echocardiography, cardiac computed tomography, and magnetic resonance imaging.
The case reported stands out because it shows the limitations of multimodality imaging where in cases of left atrial tumors with features highly suggestive of an atrial myxoma, it is insufficient to provide the correct diagnosis, which is made after examination of the pathology specimen.
Although multimodality imaging has a central role in the differential diagnosis of left atrial tumors, in cases of tumors with features highly suggestive of an atrial myxoma, it has some limitations.
Correspondence Address:Panagiotis Artemiou, https://orcid.org/0000-0001-5760-5308, Department of Cardiac Surgery, Faculty of Medicine, Comenius University, National Institute of Cardiovascular Diseases, Pod krasnou horkou 1, Bratislava, Slovakia, Zip Code: 83101, E-mail: panayiotisartemiou@yahoo.com
Fig. 1
Multimodality imaging showing the left atrial tumor. A) Computed tomography. B) Magnetic resonance imaging. C) 2D-transesophageal echocardiography. D) 3D-transesophageal echocardiography.
Fig. 2
A) Intraoperative view of the tumor. B) Tumor after resection. C and D) Histology showing the organized left atrial thrombus.
