Carátula del artículo
Midterm Results of Neocuspidization of the Aortic Valve with Ozaki
Technique in Adults
 Seguel S. Enrique enseguel@udec.cl
Seguel S. Enrique enseguel@udec.cl
Guillermo Grant Benavente Hospital of
Concepción, Chile
Universidad de Concepción, Chile
Reyes M. Rodrigo
Universidad de Concepción, Chile
Guillermo Grant Benavente Hospital of
Concepción, Chile
González L. Roberto
Universidad de Concepción, Chile
Guillermo Grant Benavente Hospital of
Concepción, Chile
Rubilar P. Héctor
Universidad de Concepción, Chile
Sepúlveda P. Camila
Universidad de Concepción, Chile
Barril M. Gustavo
Pontifical Catholic University of
Chile, Chile
Stockins L. Aleck
Universidad de Concepción, Chile
Guillermo Grant Benavente Hospital of
Concepción, Chile
Brazilian Journal of Cardiovascular Surgery, vol. 41, no. 1, e20240126, 2026
Sociedade Brasileira de Cirurgia Cardiovascular
Received: 01 April 2024
Revised document received: 03 May 2024
Accepted: 07 May 2024
INTRODUCTION
Many prosthetic models have been developed with the aim of achieving the ideal valve
substitute. Among other characteristics, this substitute should have good
hemodynamics (low gradient, no insufficiency), be easy to implant with a
reproducible technique, not alter blood components or be thrombogenic, be durable
over time, and resistant to infections.
Currently used mechanical prostheses possess some of these characteristics: they are
easy to implant, have a low rate of structural deterioration, excellent
hemodynamics, and long-term durability. However, they require lifelong anticoagulant
treatment to prevent thrombus formation and embolisms[1,2].
Tissue animal prostheses do not require anticoagulation, but they have limited
durability, especially in younger patients and in situations of suboptimal
hemodynamics such as small aortic roots and/or rings[3-5].
Aortic homografts allow for the replacement of the diseased valve with one extracted
from a cadaver, but their availability is limited, which prevents their implantation
in all centers[6].
The Ross procedure uses the patient's own pulmonary valve as an aortic
substitute and a homograft (or another substitute) to replace the pulmonary valve.
Although this technique has shown excellent long-term results, it is technically
more demanding, and few centers have experience with it[7,8].
The valve reconstruction procedure known as AvNeo®, or aortic
neocuspidization, was proposed by Dr. Shigeyuki Ozaki in Japan[9].
Surgery is performed under general anesthesia with standard invasive monitoring for
aortic valve replacement. All patients undergo transesophageal echocardiography. The
pericardium is accessed through a median sternotomy. The anterior pericardium is
dissected, freeing the pleurae up to the phrenic nerves and the mediastinal fat from
the diaphragm to the innominate vein. A portion of pericardium of approximately 10
× 10 cm is resected, stretched, and fixed on a medical grade acetate sheet to
remove the remaining tissue (Figures 1A and
B). The pericardium is treated with a 0.6%
glutaraldehyde solution for 10 minutes and washed in physiological saline for six
minutes three times.
 Fig. 1
A) Exposure of the anterior pericardium. B) Stretched and fixed
pericardium on the sheet for treatment with glutaraldehyde. C) Marking
of the neo-cusps on the pericardium, which are subsequently cut out for
use (D).
Fig. 1
A) Exposure of the anterior pericardium. B) Stretched and fixed
pericardium on the sheet for treatment with glutaraldehyde. C) Marking
of the neo-cusps on the pericardium, which are subsequently cut out for
use (D).
During this time, the patient is connected to cardiopulmonary bypass (CPB), and the
heart is protected in the usual manner. The aortic valve is accessed through an
aortotomy, resected, and the annulus is decalcified.
The distance between the commissures of each cusp is measured using
AvNeo® system gauges (JOMDD Inc., Tokyo, Japan), designed by
Dr. Ozaki. Subsequently, the cusps are drawn on the pericardium according to the
measurements using the system template, and each cusp is individually trimmed (Figures 1C and D).
Each cusp is sutured to the native annulus using continuous polypropylene suture. The
commissures are fixed with separate polypropylene sutures reinforced with
Teflon™ pledgets that remain on the outside of the aortic wall (Figure 2).
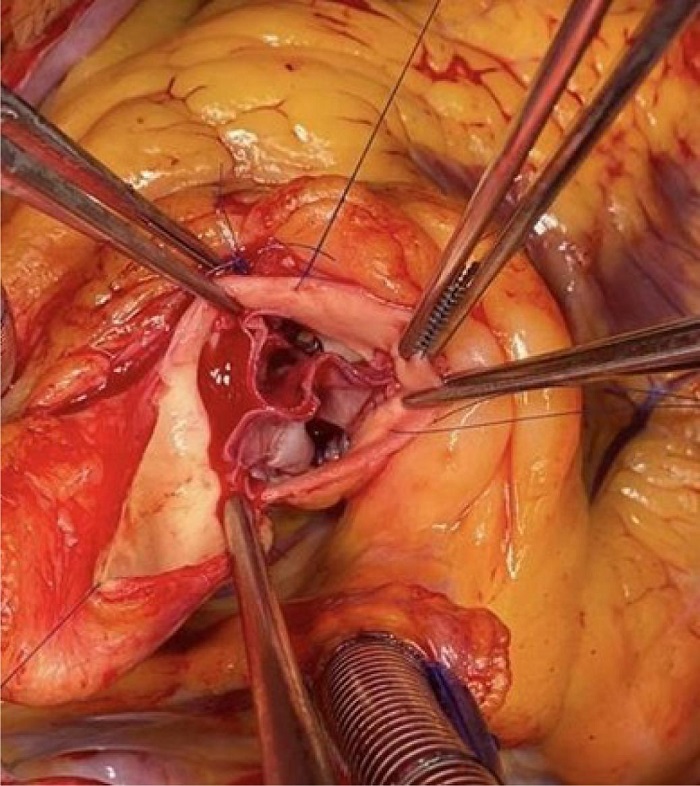 Fig. 2
Final appearance of the valve with the three neo cusps sutured to the
aortic annulus.
Fig. 2
Final appearance of the valve with the three neo cusps sutured to the
aortic annulus.
A transesophageal echocardiogram is performed after coming off CPB to assess valve
morphology, valve area, coaptation surface of the cusps, absence of insufficiency,
and transvalvular gradient (Figure 3).
 Fig. 3
Final echocardiographic appearance in short-axis and long-axis views,
showing the morphology of the valve and the wide coaptation
surface.
Fig. 3
Final echocardiographic appearance in short-axis and long-axis views,
showing the morphology of the valve and the wide coaptation
surface.
Technical details can be found in our previous communication[10].
According to Dr. Ozaki, the technique can be performed in almost all cases, except
those requiring root replacement or patients with endocarditis with ring
destruction. It does not require anticoagulation, and only aspirin use (100 mg/day)
for six months after surgery is recommended. Reported results show good
hemodynamics, excellent survival, and a low rate of midterm
reinterventions[11].
Patients
This is a descriptive study of patients who underwent aortic valve
neocuspidization with the Ozaki technique at Hospital Guillermo Grant Benavente
(Concepción, Chile) between March 2019 and December 2023 (n=56).
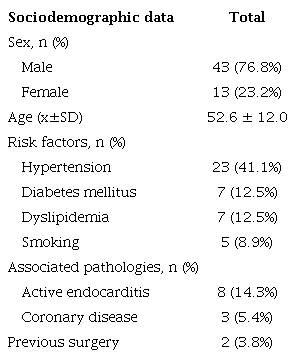
Forty-three male patients (76.8%) with a mean age of 52.6 ± 12 years
(range 19 – 80) were included. Eight patients had active endocarditis,
seven on native valve. The mitral valve was involved in three of them, and
another was associated with a ventricular septal defect (VSD) and tricuspid
endocarditis. Three patients had associated coronary artery disease, and one had
a perimembranous VSD. Two patients had previous surgery (subaortic membrane and
aortic valve replacement with biological prosthesis). The calculated operative
risk with European System for Cardiac Operative Risk Evaluation (EuroSCORE) II
was 2.3 ± 3.7%[12].
Excluding patients with endocarditis, the average EuroSCORE II was 1.3 ±
0.5% (Table 1).
Table 1
Preoperative characteristics of patients.
 SD=standard deviation
SD=standard deviation
Valve pathology included stenosis in 41 and insufficiency in 15 patients. Valve
morphology was bicuspid in 35 patients. For patients with aortic stenosis,
maximum gradient was 81.6 ± 35 mmHg, mean gradient was 51.3 ± 18
mmHg, aortic jet velocity was 51.3 ± 18 m/s, and valve area was 0.74
± 0.2 cm2. The average left ventricular ejection fraction was 57.6
± 12.6% (range 27 – 68%) (Table
2).
Table 2
Preoperative echocardiogram.
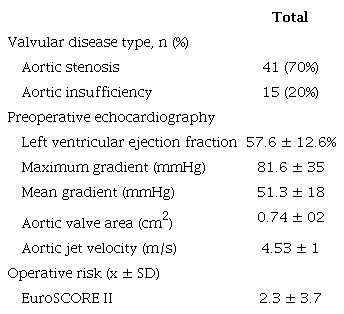 EuroSCORE=European System for Cardiac Operative Risk Evaluation;
SD=standard deviation
EuroSCORE=European System for Cardiac Operative Risk Evaluation;
SD=standard deviation
The most used neo-cusp sizes were 27 mm for the left cusp, 25 mm for the right
cusp, and 27 mm for the non-coronary cusp.
There were eight associated surgeries: three mitral repairs, three coronary
bypasses, one tricuspid repair and closure of a perimembranous VSD, and one VSD
closure.
Aortic cross-clamping and bypass times were 95.2 ± 23.7 and 102 ±
23.1 minutes, respectively. For patients without associated surgery, the times
were 90.5 ± 17.2 and 97.7 ± 19.1 minutes, respectively (Table 3).
Table 3
Surgeries and operative results.
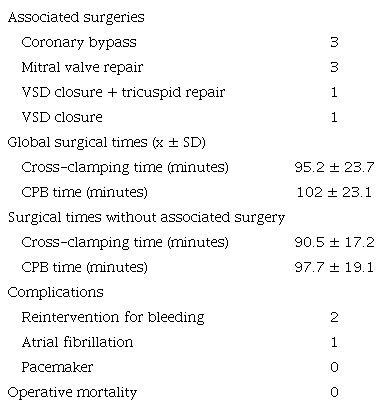 CPB=cardiopulmonary bypass; SD=standard deviation; VSD=ventricular
septal defect
CPB=cardiopulmonary bypass; SD=standard deviation; VSD=ventricular
septal defect
Postoperative echocardiography showed good valve morphology, low transaortic
gradient, and absence of aortic insufficiency in all cases except three
patients. One showed moderate valvular insufficiency at the commissural level.
Commissural closure was performed with a suture, and subsequent control showed
absence of insufficiency. Two patients had severe central insufficiency due to
poor cusp coaptation, and the valve was replaced with biological prostheses in
both cases.
One patient with active endocarditis was reoperated for postoperative bleeding.
And one patient experienced transient atrial fibrillation.
There were no infectious, renal, neurological, or mechanical ventilation > 48
hours. There was no need for pacemakers or other cardiovascular
complications.
The average length of in-hospital stay was 7.7 days, but if only patients without
endocarditis are considered, the average length of stay was six days.
There was no operative mortality. Follow-up was completed until December 31,
2023. The average follow-up was 17.4 ± 12.1 months (Table 4).
Table 4
Follow-up.
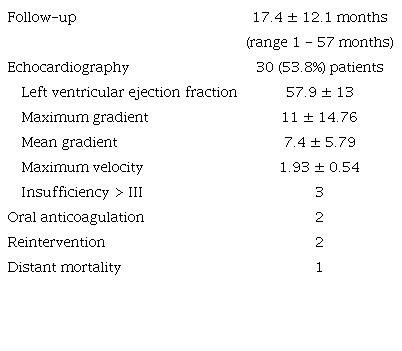
Two patients were on anticoagulation for atrial fibrillation.
There were no cases of endocarditis or cerebrovascular accidents during
follow-up. Transthoracic echocardiography was performed at 12 months of
follow-up in 30 patients. Valve morphology was adequate, without calcifications
or deterioration of the cusps. The mean gradient was 7.4 mmHg, and the peak
gradient was 11 mmHg. One patient had moderate aortic insufficiency. It was
decided to follow them clinically and echocardiographically before intervening.
Two patients had severe insufficiency secondary to detachment of one of the
neo-cusps at the commissural level (Figure
4). Valve replacement with prostheses was performed at two and four
months post-surgery. Figure 5 shows freedom
from aortic insufficiency > 3 and freedom from reintervention.
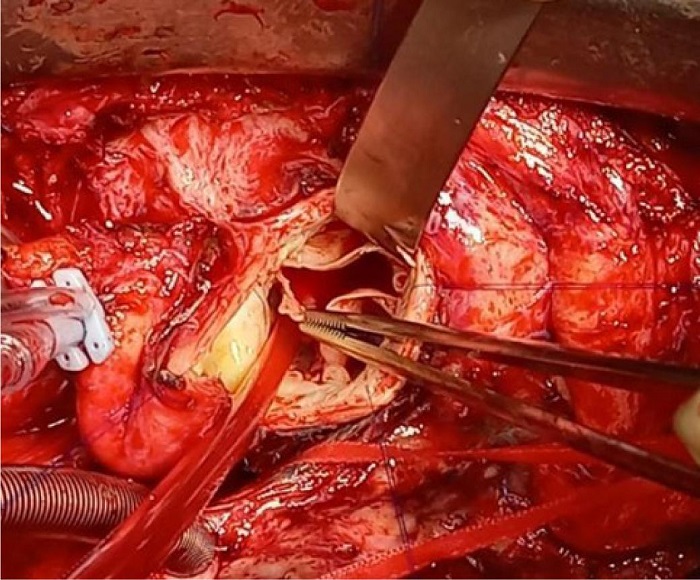 Fig. 4
Patient reoperated due to aortic insufficiency in the
postoperative period. Partial detachment of a cusp at the commissure
level is observed (arrow).
Fig. 4
Patient reoperated due to aortic insufficiency in the
postoperative period. Partial detachment of a cusp at the commissure
level is observed (arrow).
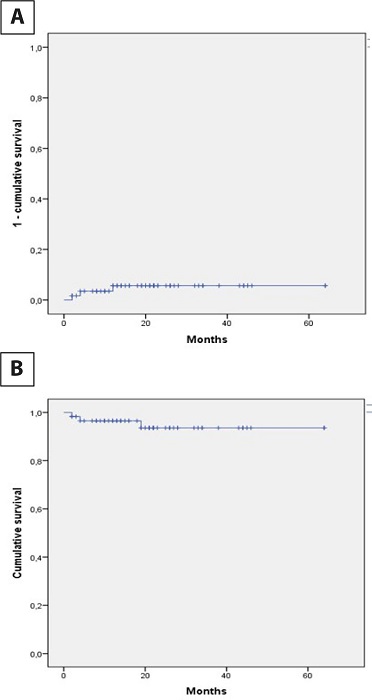 Fig. 5
A) Curve of appearance of aortic insufficiency > 3. B) Curve
of freedom from reinterventions.
Fig. 5
A) Curve of appearance of aortic insufficiency > 3. B) Curve
of freedom from reinterventions.
Clinically, all other patients were in functional capacity I.
One patient died 52 months after surgery due to diabetic ketoacidosis. There were
no deaths from cardiovascular causes during follow-up.
QUESTIONS
-
Which are the advantages of AvNeo®?
-
Which patients can potentially benefit from this technique?
-
What are the disadvantages with this technique?
-
How to deal with bicuspid valves?
-
Is the technique recommended for all patients?
-
What were the observed midterm results?
Discussion of Questions
Question A. The autologous pericardial neocuspidization proposed by
Dr. Ozaki offers several advantages over current valve substitutes: it utilizes
autologous pericardium, potentially reducing immune response; the cusps are
sutured directly to the annulus, allowing for a larger effective orifice area;
it lacks a rigid support, maintaining aortic ring mobility; and it has a wide
coaptation surface, with a lower risk of insufficiency. Being biological tissue,
it does not require anticoagulation[13-15].
It is standardized, making the technique reproducible, and according to its
author, applicable to almost all valve anatomies and pathologies[9,10,15].
Question B. Patient selection considered those with potential
benefit over standard valve replacement. Excluding the first two cases (aged 71
and 80 years), we included young or middle-aged patients (average age 51.2
years, range 19–68 years) who did not desire mechanical prosthetic
replacement. In our setting, the alternative in these cases is biological
prosthesis replacement, which will likely have a shorter duration than expected
in patients > 65 years and will likely require reintervention in the
future[3,4,16].
Question C. The approach requires complete sternotomy for adequate
pericardial dissection. This goes against the current trend of performing valve
replacement surgery using minimally invasive techniques. Aortic replacement by
partial sternotomy or thoracotomy has shown to decrease perioperative bleeding
incidence, mechanical ventilation time, and intensive care unit stay, but has
not shown an impact on reducing operative mortality in the general
population[17-19]. These benefits are likely
more significant in a higher-risk population, such as the elderly. In a low-risk
population, complete sternotomy does not add additional risk and would allow for
longer valve substitute durability.
Question D. For bicuspid valve cases, annular decalcification was
performed, and a biological prosthesis sizer was used to mark the new
commissures with reference to the commissure between the right and left cusps.
Subsequently, the cusps were measured using these marks as a reference. This
allows for the implantation of three neo-cusps of similar sizes, achieving a
more symmetric valve anatomy. Attention should be paid to the fact that in these
patients, the non-coronary cusp annulus usually has a deeper nadir than the
others. To avoid distortion in the final height of the neo-cusps (as occurred in
one case), this cusp should be sutured to the aortic wall approximately at the
level of the nadirs of the right and left cusps.
Question E. Because the technique requires separate implantation of
each cusp and construction of the commissures, aortic cross-clamping and CPB
times are longer than those of a routine valve replacement. This should be
considered when selecting the patient and not including patients with
ventricular dysfunction, where prolonged ischemic time could result in
myocardial damage and difficulty in weaning from bypass.
Two cases had severe postoperative insufficiency. In both cases, the native
valves were tricuspid, with annular dilation. Likely, the neo-cusp measurements
were inadequate, and smaller sizes were selected than required for those ring
sizes, resulting in lack of cusp coaptation. To avoid prolonging cross-clamping
and CPB times, replacement with biological prostheses was decided in both
cases.
The rate of complications and operative mortality was low, and the hospital stay
for elective patients was short, as expected for a series of selected, low-risk
patients (excluding patients with endocarditis, the average EuroSCORE II was
1.3%).
Question F. The follow-up for this series is still brief. The clinical evolution
of the patients has been very good. Echocardiograms have shown excellent valve
morphology, with good cusp mobility and low transvalvular gradients.
Mylonakis et al.[20], in a
meta-analysis published in 2023 including 1,891 adult and pediatric patients,
observed that the average effective orifice area was 2.08 ± 0.5
cm2/m2, and the maximum gradient was 15.7 ± 7.4
mmHg. The rate of moderate insufficiency observed was 0.25%.
Three cases presented aortic insufficiency on postoperative follow-up: one
patient was admitted for decompensated heart failure two months after surgery,
was medically compensated, and underwent an echocardiogram showing severe aortic
insufficiency due to cusp prolapse. A second case consulted at four months after
surgery for dyspnea. Echocardiography also showed severe insufficiency, and
reoperation was decided. In the reoperation of both cases, partial detachment (5
mm) of the non-coronary cusp at a commissural level was confirmed. Valve
replacement with biological prostheses was decided in the first case and
mechanical in the second. However, it is likely that the cusp could have been
repaired by a surgeon with more experience with the technique.
In the third case, a murmur was auscultated on clinical follow-up.
Echocardiography showed moderate to severe aortic insufficiency due to
non-coronary cusp coaptation deficiency. This patient is asymptomatic, there has
been no ventricular dilatation, and systolic function is normal. Clinical and
echocardiographic follow-up was decided.
At the time of follow-up, there were no deaths from cardiovascular causes in our
series. This is likely due to the selection of young patients for the
technique.
In Mylonakis' meta-analysis, with an average follow-up of 38.1 ± 23.8
months, mortality was 1.91%, and freedom from reintervention survival was
96.7%.
In Dr. Ozaki's series, which included 850 patients (average age 71 years,
average follow-up of 53.7 months), actuarial survival was 85.9%, the
reintervention rate was 4.2%, and the incidence of moderate to severe valvular
insufficiency was 7.3% at 10 years.
In a study comparing 627 patients from Dr. Ozaki's series with 627 matched
patients from the Cleveland Clinic's Perimount® aortic
valve replacement registry, it was observed that patients undergoing the
technique had lower gradients (17 mmHg vs. 28 mmHg,
P<0.001), a higher rate of insufficiency (3.6%
vs. 1%, P=0.006), with similar
reintervention-free survival at six years of follow-up[21].
BRIEF CONSIDERATIONS OF THE CASES REPORTED
This study involves a group of selected patients with low operative risk and good
ventricular function, which limits the generalization of the findings to higher-risk
populations or those with ventricular dysfunction. Additionally, the experience of
the surgical team may influence the results, potentially not reflecting the reality
in other centers with less or more experience in the technique of aortic valve
neocuspidization.
Since aortic valve disease is a chronic condition that may require long-term
monitoring, it is crucial to evaluate medium- and long-term outcomes to fully
understand the effectiveness and durability of this surgical technique.
Despite these limitations, the immediate and midterm results of aortic valve
neocuspidization surgery are encouraging. The technique proves to be reproducible
and offers good outcomes in selected patients, especially those who wish to avoid
the use of anticoagulants, such as young patients.
Further studies with a larger number of patients, longer-term follow-up, and in more
diverse populations are needed to confirm these findings and the theoretical
advantages of the technique over biological prostheses (durability, hemodynamic
behavior, reinterventions) and to establish the definitive role of this technique in
the treatment of aortic valve disease.
LEARNING POINTS
-
AVNeo® may offer a promising option, by preserving native
anatomy, avoiding prosthetic materials and anticoagulation.
-
Long-term data and further research are still needed to determine which
patients can potentially benefit from this technique.
REFERENCES
DeWall RA, Qasim N, Carr L. Evolution of mechanical heart valves.
Ann Thorac Surg. 2000;69(5):1612-21.
doi:10.1016/s0003-4975(00)01231-5.
Bouhout I, Stevens LM, Mazine A, Poirier N, Cartier R, Demers P, et
al. Long-term outcomes after elective isolated mechanical aortic valve
replacement in young adults. J Thorac Cardiovasc Surg. 2014;148(4):1341-6.e1.
doi:10.1016/j.jtcvs.2013.10.064.
Malvindi PG, Luthra S, Olevano C, Salem H, Kowalewski M, Ohri S.
Aortic valve replacement with biological prosthesis in patients aged 50-69
years. Eur J Cardiothorac Surg. 2021;59(5):1077-86.
doi:10.1093/ejcts/ezaa429.
Saleeb SF, Newburger JW, Geva T, Baird CW, Gauvreau K, Padera RF, et
al. Accelerated degeneration of a bovine pericardial bioprosthetic aortic valve
in children and young adults. Circulation. 2014;130(1):51-60.
doi:10.1161/CIRCULATIONAHA.114.009835.
Chikwe J, Filsoufi F. Durability of tissue valves. Semin Thorac
Cardiovasc Surg. 2011;23(1):18-23.
doi:10.1053/j.semtcvs.2011.04.008.
Ross DN. Homograft replacement of the aortic valve. Lancet.
1962;2(7254):487. doi:10.1016/s0140-6736(62)90345-8.
Al-Halees Z, Pieters F, Qadoura F, Shahid M, Al-Amri M, Al-Fadley F.
The Ross procedure is the procedure of choice for congenital aortic valve
disease. J Thorac Cardiovasc Surg. 2002;123(3):437-41; discussion 441-2.
doi:10.1067/mtc.2002.119705.
Reece TB, Welke KF, O'Brien S, Grau-Sepulveda MV, Grover FL,
Gammie JS. Rethinking the ross procedure in adults. Ann Thorac Surg.
2014;97(1):175-81. doi:10.1016/j.athoracsur.2013.07.036.
Ozaki S, Kawase I, Yamashita H, Uchida S, Nozawa Y, Matsuyama T, et
al. Aortic valve reconstruction using self-developed aortic valve plasty system
in aortic valve disease. Interact Cardiovasc Thorac Surg. 2011;12(4):550-3.
doi:10.1510/icvts.2010.253682.
Reyes M R, González L R, Seguel S E, Stockins L A, Jadue T A,
Alarcón C E. Reconstrucción de válvula aórtica con
pericardio autólogo según técnica de Ozaki Rev Med Chil.
2021;149(12):1806-11. doi:10.4067/s0034-98872021001201806.
Ozaki S, Kawase I, Yamashita H, Uchida S, Takatoh M, Kiyohara N.
Midterm outcomes after aortic valve neocuspidization with glutaraldehyde-treated
autologous pericardium. J Thorac Cardiovasc Surg. 2018;155(6):2379-87.
doi:10.1016/j.jtcvs.2018.01.087.
Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR,
et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734-44; discussion
744-5. doi:10.1093/ejcts/ezs043.
Bloch O, Golde P, Dohmen PM, Posner S, Konertz W, Erdbrügger
W. Immune response in patients receiving a bioprosthetic heart valve: lack of
response with decellularized valves. Tissue Eng Part A. 2011;17(19-20):2399-405.
doi:10.1089/ten.TEA.2011.0046.
Cheng A, Dagum P, Miller DC. Aortic root dynamics and surgery: from
craft to science. Philos Trans R Soc Lond B Biol Sci. 2007;362(1484):1407-19.
doi:10.1098/rstb.2007.2124.
Ricciardi G, Biondi R, Tamagnini G, Giglio MD. Aortic valve
reconstruction with ozaki technique. Braz J Cardiovasc Surg. 2022;37(1):118-22.
doi:10.21470/1678-9741-2020-0476.
Anselmi A, Flecher E, Chabanne C, Ruggieri VG, Langanay T, Corbineau
H, et al. Long-term follow-up of bioprosthetic aortic valve replacement in
patients aged ≤60 years. J Thorac Cardiovasc Surg.
2017;154(5):1534-41.e4. doi:10.1016/j.jtcvs.2017.05.103.
Rodríguez-Caulo EA, Guijarro-Contreras A, Guzón A,
Otero-Forero J, Mataró MJ, Sánchez-Espín G, et al. Quality
of life after ministernotomy versus full sternotomy aortic valve replacement.
Semin Thorac Cardiovasc Surg. 2021;33(2):328-34.
doi:10.1053/j.semtcvs.2020.07.013.
Glauber M, Ferrarini M, Miceli A. Minimally invasive aortic valve
surgery: state of the art and future directions. Ann Cardiothorac Surg.
2015;4(1):26-32. doi:10.3978/j.issn.2225-319X.2015.01.01.
Rodriguez EA, Otero JJ, Matar MJ, Sanchez G, Porras C, Guzon A, et
al. Mejora de la morbilidad postoperatoria en recambio valvular aórtico
aislado con miniesternotomía: estudio pareado por puntuación de
propensión. Cir Cardiov. 2016;23(5):229-33.
Mylonas KS, Tasoudis PT, Pavlopoulos D, Kanakis M, Stavridis GT,
Avgerinos DV. Aortic valve neocuspidization using the ozaki technique: a
meta-analysis of reconstructed patient-level data. Am Heart J. 2023;255:1-11.
doi:10.1016/j.ahj.2022.09.003.
Unai S, Ozaki S, Johnston DR, Saito T, Rajeswaran J, Svensson LG, et
al. Aortic valve reconstruction with autologous pericardium versus a
bioprosthesis: the ozaki procedure in perspective. J Am Heart Assoc.
2023;12(2):e027391. doi:10.1161/JAHA.122.027391.
Notes
Notes
Artificial Intelligence Usage The authors declare use of ChatGPT for spelling and grammar correction of the
article abstract. The content produced by the artificial intelligence tool was
revised and edited by the authors as necessary, and they take full
responsibility for the content to be published.
Sources of Funding There were no external funding sources for this study.
This study was carried out at the Department of Surgery, Faculty of Medicine,
Universidad de Concepción, Concepción, Chile.
Conflict of interest declaration
Potential Conflict of Interest Conflict of interest: First author is proctor for AvNeo®
technique for Sanamedi Inc, Japan.
Author notes
Correspondence Address: Enrique Seguel
Soto, Department of Surgery, Faculty of Medicine, Universidad de
Concepción Avenue Roosevelt, Janequeo, Concepción, Chile, Zip
Code:4070386, E-mail: enseguel@udec.cl