Carátula del artículo
Is the Six-Minute Walk Test the Key to Boost Postoperative Clinical
Outcomes in Cardiac Surgery?
 Isadora Salvador Rocco
Isadora Salvador Rocco
Universidade Federal de São Paulo, Brazil
Universidade Federal de São Paulo, Brazil
Walter José Gomes
Universidade Federal de São Paulo, Brazil
Universidade Federal de São Paulo, Brazil
Caroline Bublitz
Universidade Federal de São Paulo, Brazil
Alexandra Ribeiro Monte Sião
Universidade Federal de São Paulo, Brazil
Nelson A. Hossne
Universidade Federal de São Paulo, Brazil
Solange Guizilini sguizilini@unifesp.br
Universidade Federal de São Paulo, Brazil
Universidade Federal de São Paulo, Brazil
Brazilian Journal of Cardiovascular Surgery, vol. 41, no. 1, e20240241, 2026
Sociedade Brasileira de Cirurgia Cardiovascular
Received: 12 July 2024
Revised document received: 17 January 2025
Accepted: 08 April 2025
 CABG=coronary artery bypass grafting; METs=metabolic costs; wMRT=work
corrected mean response time.
CABG=coronary artery bypass grafting; METs=metabolic costs; wMRT=work
corrected mean response time.
The role of the six-minute walk test (6MWT) has expanded to become a valuable tool for
evaluating submaximal exercise capacity in patients with cardiovascular diseases,
serving as an independent predictor for adverse events and mortality[1,2]. The 6MWT unveils the threshold at which symptoms may manifest during
activities, thereby delineating functional limitations. Such information is a
cornerstone for the understanding of a disease's impact and, therefore, to predict
clinical courses. Greater performance during the 6MWT suggests better preservation of
peripheral musculature and reveals the presence of adaptive mechanisms that overcome
underlying oxygen delivery challenges of cardiovascular diseases[3,4]. On the other hand, a poor performance during the test unveils
circulatory deficits followed by consequences in other systems, leading to a worse
prognosis[4,5].
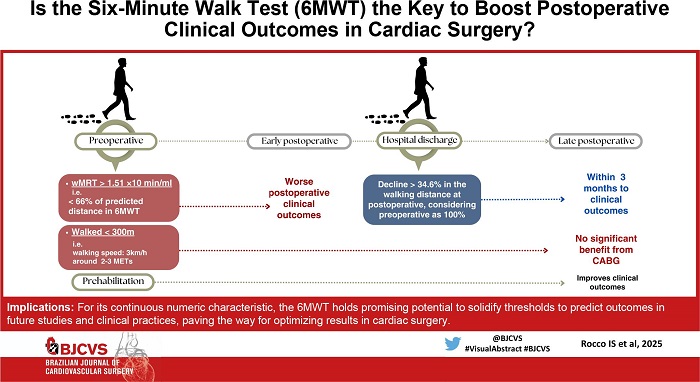
Findings stemming from the seminal Surgical Treatment for Ischemic Heart Failure (STICH)
trial revealed a pivotal insight into the risk stratification for coronary artery bypass
grafting (CABG)[6]. The STICH trial
compared CABG with optimal medical therapy (OMT) in patients with advanced coronary
artery disease and severe left ventricular (LV) dysfunction. After a median of
approximately 10 years of follow-up, patients randomized to CABG had lower all-cause and
cardiovascular mortality compared with those with OMT. A further substudy of the STICH
trial reported that baseline 6MWT distance predicted mortality during late follow-up in
the STICH trial. Patients unable to walk 300 meters had higher mortality during the
first 60 days with CABG and no significant benefit from CABG during total
follow-up[7]. These
observations suggest that patients with ischemic LV dysfunction and poor exercise
capacity have increased early risk, while those with better exercise capacity have
improved survival with CABG.
This brought to debate that patients' clinical condition and fitness matter for the
results of surgery, emphasizing the important role of the 6MWT in determining potential
surgical outcomes. Likewise, our research group made a significant advance to this field
through an in-depth investigation into the physiological response during the transition
from rest to effort in the 6MWT, thereby establishing its predictive ability for early
outcomes following CABG[8]. The same
findings were observed for patients in the preoperative period of valve surgery, where
poor performance of 6MWT was associated with worse results following surgery[9].
Despite these findings around predictive abilities of the 6MWT, it remains conspicuously
absent from the standard preoperative assessment protocols for perioperative management.
Its integration into routine evaluation practices and well-established risk
stratification scores within the cardiac surgery domain has been notably lacking. Recent
updates in risk models, such as the European System for Cardiac Operative Risk
Evaluation 3, emphasizes a proactive approach to enhance predictive ability following
cardiac surgery[10]. Integrating
responses to the 6MWT into these models holds promise for refining risk stratification.
By capturing a patient's physiological response to submaximal effort, this dynamic
evaluation could provide valuable insights and identify patients in need for
prehabilitation interventions, potentially improving the overall success and safety of
cardiac surgeries. Nevertheless, studies in this field are necessary to comprehensively
assess the safety of conducting the 6MWT preoperatively.
Beyond its predictive role, the 6MWT can quantify the acute impact of cardiac procedure
in functional capacity during the postoperative period. Studies have shown an inherent
drop on the distance walked at hospital discharge compared to the preoperative period
that varies around 12 to 17%[11,12]. When the 6MWT is applied earlier,
right after intensive care unit discharge around the fifth postoperative day, this fall
can reach over 30%[13]. Recent
findings of our group have uncovered that a decline exceeding 34.6% is associated with
unfavorable midterm outcomes following CABG. Although these assumptions lack strong
evidence, it brings to light the necessity to investigate the potential role of
systematically evaluating 6MWT performance during both pre and postoperative
periods.
Postoperative assessment using the 6MWT at hospital discharge provides valuable
prognostic information, facilitating effective screening for outpatient care. Beyond
assessing mere walking distance, it serves as a measure of speed, which holds
significance in tailoring postoperative exercise prescription. Additionally, it unveils
the level of metabolic costs (METs) at which patients experience a comfortable walking
speed. For instance, performing 300 meters in six minutes is equivalent to a walking
speed of 3 km/hour, which corresponds to a metabolic expenditure of two to three METs.
This information is crucial for gauging functional limitations and monitoring efficacy
of therapeutics, given that an increase in walking speed, such as reaching 4 - 5
km/hour, may signify a gain of one MET, indicative of 12% improvement in life
expectancy[14].
Literature in this field has established a reasonable causal relationship between
impaired functional capacity and mortality following cardiac surgery[15]. Preoperative 6MWT serves as a
reliable indicator of the patient's physical reserve and, therefore, predicts the
ability to withstand the physiological demands of surgery and subsequent recovery.
Moreover, exercise intolerance impacts postoperative strategies of enhanced recovery,
such as early walking, exposing patients to a higher risk of complications and poor
outcomes. Arthur et al.[16]
demonstrated that a multidimensional preoperative intervention significantly reduced
hospital stay and improved quality of life in low-risk patients undergoing elective
CABG. These assumptions support the importance of integrating exercise training into the
preoperative care to optimize functional status and improve overall prognosis and
surgical outcomes[17,18]. A comprehensive approach of multimodal exercise
modalities including aerobic and resistance exercises, especially inspiratory muscle
training[18], has been
recommended to enhance readiness and improve surgical outcomes.
Finally, incorporating the 6MWT during the perioperative period of cardiac surgery not
only enhances risk stratification, but also contributes significantly to the
decision-making process, ultimately aggregating results to the surgical procedure.
Therefore, the 6MWT should be applied in both pre and postoperative clinical contexts,
during the decision-making process that defines patients eligible for cardiac surgery
and early after surgery at hospital discharge, followed by serial assessments in the
outpatient postoperative setting. For its continuous numeric characteristic, the 6MWT
holds promising potential to solidify thresholds to predict outcomes in future studies
and clinical practices, paving the way for optimizing results in cardiac surgery.
REFERENCES
Grundtvig M, Eriksen-Volnes T, Ørn S, Slind EK, Gullestad L. 6 min
walk test is a strong independent predictor of death in outpatients with heart
failure. ESC Heart Fail. 2020;7(5):2904-11.
doi:10.1002/ehf2.12900.
Shawon MSR, Hsu B, Chard R, Nicholson IA, Elias VL, Nicola LK, et
al. Six-minute walk test distance at time of hospital discharge is strongly and
independently associated with all-cause mortality following cardiac surgery. Sci
Rep. 2024;14(1):2493. doi:10.1038/s41598-024-52601-7.
Jaarsma T, Perkiö Kato N, Ben Gal T, Bäck M, Chialà O, Evangelista
L, et al. Factors associated with lack of improvement in submaximal exercise
capacity of patients with heart failure. ESC Heart Fail. 2021;8(6):4539-48.
doi:10.1002/ehf2.13584.
Kern L, Condrau S, Baty F, Wiegand J, van Gestel AJ, Azzola A, et
al. Oxygen kinetics during 6-minute walk tests in patients with cardiovascular
and pulmonary disease. BMC Pulm Med. 2014;14:167.
doi:10.1186/1471-2466-14-167.
Huzmeli I, Ozer AY, Akkus O, Katayıfcı N, Sen F, Yurdalan SU, et al.
Comparison of functional exercise capacity, quality of life and respiratory and
peripheral muscle strength between patients with stable angina and healthy
controls. J Int Med Res. 2020;48(12):300060520979211.
doi:10.1177/0300060520979211.
Velazquez EJ, Lee KL, Deja MA, Jain A, Sopko G, Marchenko A, et al.
Coronary-artery bypass surgery in patients with left ventricular dysfunction. N
Engl J Med. 2011;364(17):1607-16. doi:10.1056/NEJMoa1100356.
Stewart RA, Szalewska D, She L, Lee KL, Drazner MH, Lubiszewska B,
et al. Exercise capacity and mortality in patients with ischemic left
ventricular dysfunction randomized to coronary artery bypass graft surgery or
medical therapy: an analysis from the STICH trial (Surgical treatment for
ischemic heart failure). JACC Heart Fail. 2014;2(4):335-43.
doi:10.1016/j.jchf.2014.02.009.
Rocco IS, Viceconte M, Pauletti HO, Matos-Garcia BC, Marcondi NO,
Bublitz C, et al. Oxygen uptake on-kinetics during six-minute walk test predicts
short-term outcomes after off-pump coronary artery bypass surgery. Disabil
Rehabil. 2019;41(5):534-40. doi:10.1080/09638288.2017.1401673.
Chen Y, Cai C, Qiao F, Li B, Xu Z, Lu F, et al. Preoperative
6-minute walk test predicts prolonged hospitalization after transcatheter
tricuspid valve replacement. Medicine (Baltimore). 2022;101(51):e32379.
doi:10.1097/MD.0000000000032379.
Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR,
et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734-44; discussion
744-5. doi:10.1093/ejcts/ezs043.
Hirschhorn AD, Richards DA, Mungovan SF, Morris NR, Adams L. Does
the mode of exercise influence recovery of functional capacity in the early
postoperative period after coronary artery bypass graft surgery? A randomized
controlled trial. Interact Cardiovasc Thorac Surg. 2012;15(6):995-1003.
doi:10.1093/icvts/ivs403.
Cordeiro ALL, Mascarenhas HC, Landerson L, Araújo JDS, Borges DL,
Melo TA, et al. Inspiratory muscle training based on anaerobic threshold on the
functional capacity of patients after coronary artery bypass grafting: clinical
trial. Braz J Cardiovasc Surg. 2020;35(6):942-9.
doi:10.21470/1678-9741-2019-0448.
Pauletti HO, Gomes WJ, Rocco IS, Viceconte M, Garcia BCM, Marcondi
NO, et al. Early six-minute walk test may predict midterm outcomes following
coronary artery bypass grafting. Braz J Cardiovasc Surg. 2023;38(4):e20220459.
doi:10.21470/1678-9741-2022-0459.
Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE.
Exercise capacity and mortality among men referred for exercise testing. N Engl
J Med. 2002;346(11):793-801. doi:10.1056/NEJMoa011858.
Bittner V. Functional status and outcome after coronary artery
bypass grafting. JACC Heart Fail. 2014;2(4):344-6.
doi:10.1016/j.jchf.2014.05.002.
Arthur HM, Daniels C, McKelvie R, Hirsh J, Rush B. Effect of a
preoperative intervention on preoperative and postoperative outcomes in low-risk
patients awaiting elective coronary artery bypass graft surgery. A randomized,
controlled trial. Ann Intern Med. 2000;133(4):253-62.
doi:10.7326/0003-4819-133-4-200008150-00007.
Steinmetz C, Bjarnason-Wehrens B, Walther T, Schaffland TF, Walther
C. Efficacy of prehabilitation before cardiac surgery: a systematic review and
meta-analysis. Am J Phys Med Rehabil. 2023;102(4):323-30.
doi:10.1097/PHM.0000000000002097.
Yau DKW, Underwood MJ, Joynt GM, Lee A. Effect of preparative
rehabilitation on recovery after cardiac surgery: a systematic review. Ann Phys
Rehabil Med. 2021;64(2):101391.
doi:10.1016/j.rehab.2020.03.014.
Notes
Notes
Sources of Funding The authors declare no external funding to this study.
This study was carried out at the Cardiovascular Surgery Discipline, Escola
Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, São Paulo,
Brazil.
Author notes
Potential Conflict of Interest The authors declare that there is no conflict of interest in this study.
Correspondence Address: Solange Guizilini, Cardiovascular Surgery
Discipline, Escola Paulista de Medicina, Universidade Federal de São Paulo, Rua
Napoleão de Barros, 715 - 3º andar - Vila Clementino - São Paulo - SP - Brazil,
Zip Code: 04024-002, E-mail: sguizilini@unifesp.br