Carátula del artículo
Mid-term Outcomes of Transcatheter Aortic Valve Replacement
vs. Surgical Aortic Valve Replacement in Low-to-Moderate
Risk Patients with Severe Aortic Stenosis: A Systematic Review and
Meta-analysis
 Capela António Dicazeco Pascoal
Capela António Dicazeco Pascoal
Universidade Agostinho Neto, Angola
Hilária Saugo Faria
Universidade Federal de Santa
Maria, Brazil
Antonino de Jesus Francisco
Universidade Agostinho Neto, Angola
Clara de Andrade Pontual Peres
Universidade de Pernambuco, Brazil
Luiz Fernando Tavares
Universidade Federal de Alfenas, Brazil
Barbara Bombassaro Masiero
Pontifícia Universidade Católica
do Rio Grande do Sul, Brazil
Mohamed Doma
Alexandria Faculty of Medicine, Egypt
Valdano Manuel valdanympub@gmail.com
Complexo Hospitalar de Doenças
Cardio-Pulmonares Cardeal Dom Alexandre do Nascimento, Angola
Brazilian Journal of Cardiovascular Surgery, vol. 41, no. 1, e20240250, 2026
Sociedade Brasileira de Cirurgia Cardiovascular
Received: 22 July 2024
Revised document received: 12 January 2025
Accepted: 17 March 2025
INTRODUCTION
Aortic stenosis (AS), the most prevalent heart valve disease in the elderly, is
characterized by a hemodynamically significant narrowing of the aortic valve and it
stands as a major contributor to global morbidity and mortality[1-3]. Its prevalence is increasing rapidly because of the aging
population, therefore, it is estimated that there are, now, more than 291,000
candidates for aortic valve replacement in North America and Europe[4,5]. The benefit of transcatheter aortic valve replacement (TAVR)
in patients who are inoperable is already well-established[6-8]. Surgical aortic valve replacement (SAVR) is one of the most
common cardiac procedures and it is a definitive therapy that considerably improves
symptoms and long-term survival of patients with severe AS. The procedure has been
the gold standard for more than 50 years, and its operational mortality has been
described as low: 0.5% to 1% in specialized institutions, with promising long-term
results[9,10].
The perioperative risk of mortality associated with SAVR tends to increase with age,
reaching up to approximately 10% in patients aged 85 to 90 years[11]. Although surgery is still
considered an intervention of choice in patients with a low risk of surgical
complications and severe AS, TAVR is continually gaining ground in the lower-risk
groups[6]. Approximately
90% of patients undergoing aortic valve replacement are considered to be at low and
moderate surgical risk[12,13]. Several factors are influential
in this current scenario, including the high prevalence of patients requiring valve
replacement and technological advances in valve replacement that allows a minimally
invasive approach under local anesthesia[14-16].
Although previous meta-analyses have demonstrated that TAVR is not inferior to SAVR
in patients with low to moderate surgical risk, they primarily included studies with
shorter follow-up periods, limiting the assessment of mid-term outcomes[17,18]. To address this gap, the present systematic review and
meta-analysis aimed to comprehensively compare the mid-term safety and efficacy of
TAVR vs. SAVR in patients with AS at low to moderate surgical risk
by evaluating two critical endpoints: all-cause mortality and disabling stroke,
using more recent evidence with extended follow-up data.
METHODS
This systematic review with meta-analysis was registered in the International
Prospective Register of Systematic Reviews (or PROSPERO) under protocol
CRD42024501903. It was designed and conducted according to the Cochrane Handbook for
Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (or PRISMA) Statement guidelines[19,20].
Eligibility Criteria
Only fully published manuscripts meeting all the following eligibility criteria
were included: (1) randomized controlled trials (RCTs); (2) including
low-to-moderate surgical risk patients with severe AS; (3) comparing
transcatheter vs. surgical aortic valve; (4) studies with
follow-up ≥ 4 years; (5) availability of studies in English; and (6)
reporting any of the clinical outcomes of interest. A minimum of a four-year
follow-up was chosen based on the preliminary review of the literature which
found substantial heterogeneity in follow-up between different studies (a few
weeks to years). We excluded: (1) overlapping populations, defined as studies
with overlapping institutions and recruitment periods; (2) non-randomized
studies; (3) studies with no outcomes of interest; (4) conference abstracts; and
(5) no control group. There were no restrictions based on the year of
publication. In case of missing data from individual studies, the corresponding
authors were contacted for specific study results.
Search Strategy and Data Extraction
We systematically searched PubMed®, Embase, and Cochrane Central Register
of Controlled Trials for RCTs meeting the eligibility criteria from inception to
May 2024. The search strategy consisted of “(aortic valve replacement OR
Aortic stenosis) AND (TAVI OR TAVR OR Aortic Transcatheter OR Transcatheter
Aortic valve implantation) AND (Surgical Aortic valve replacement OR Surgical
Aortic Valve Replacement OR Surgical Aortic Valve implantation)”. The
references from all included studies, previous systematic reviews, and
meta-analyses were also searched manually for any additional study[21].
The search strategy was conducted by two authors (C.A.D.P. and C.A.P.P.). The
studies found in the databases and the references of the articles were
incorporated into the Rayyan reference management (Rayyan Systems Inc.,
Montreal, Canada). Duplicate articles were manually excluded. Any disagreements
were resolved through consensus by the senior author (V.M.). The baseline
characteristics were extracted by other two authors (H.S.F. and C.A.P.P). The
outcome data following predefined search criteria and quality assessment was
extracted by other two authors (C.A.D.P and L.F.T.).
Endpoints and Subgroup Analyses
The main outcomes of interest were: (1) all-cause mortality and (2) disabling
stroke. Subgroup analyses based on the participants’ surgical risk and
the studies’ follow-up time were used to reduce heterogeneity.
Quality Assessment
Quality assessment of RCTs was performed by two independent authors (A.J.F. and
H.S.F.) using the Cochrane Collaboration’s tool for assessing risk of
bias in RCTs (RoB 2), in which studies are scored as high, low, or unclear risk
of bias in five domains: selection, performance, detection, attrition, and
reporting biases[22].
Disagreements were resolved by the senior author (V.M.).
Statistical Analysis
In order to compare treatment effects for categorical endpoints, a risk ratio
(RR) with 95% confidence intervals (CI) was pooled using the Mantel-Haenszel
method with the Der Simonian and Laird random-effects model. We assessed
heterogeneity with I² statistics and Cochrane Q test; I² > 25%
was considered significant for heterogeneity. P-values <
0.05 were considered statistically significant. Review Manager 5.1.7 (Cochrane
Center, The Cochrane Collaboration, Denmark) and R software (version 4.3.2, R
Foundation for Statistical Computing, Vienna, Austria) were used for statistical
analysis. Aiming to explore the robustness of the results and identify outliers,
leave-one-out sensitivity analyses were conducted by systematically removing
each study from the research and recalculating the results for outcomes with
significant heterogeneity.
RESULTS
Study Selection and Baseline Characteristics
As detailed in Figure 1, the initial search
yielded 1,281 results. After the removal of duplicate records and ineligible
studies, 26 articles remained and were fully reviewed based on inclusion
criteria. Of these, a total of six RCTs were included, comprising 6,498
patients[23-28]. Study characteristics are
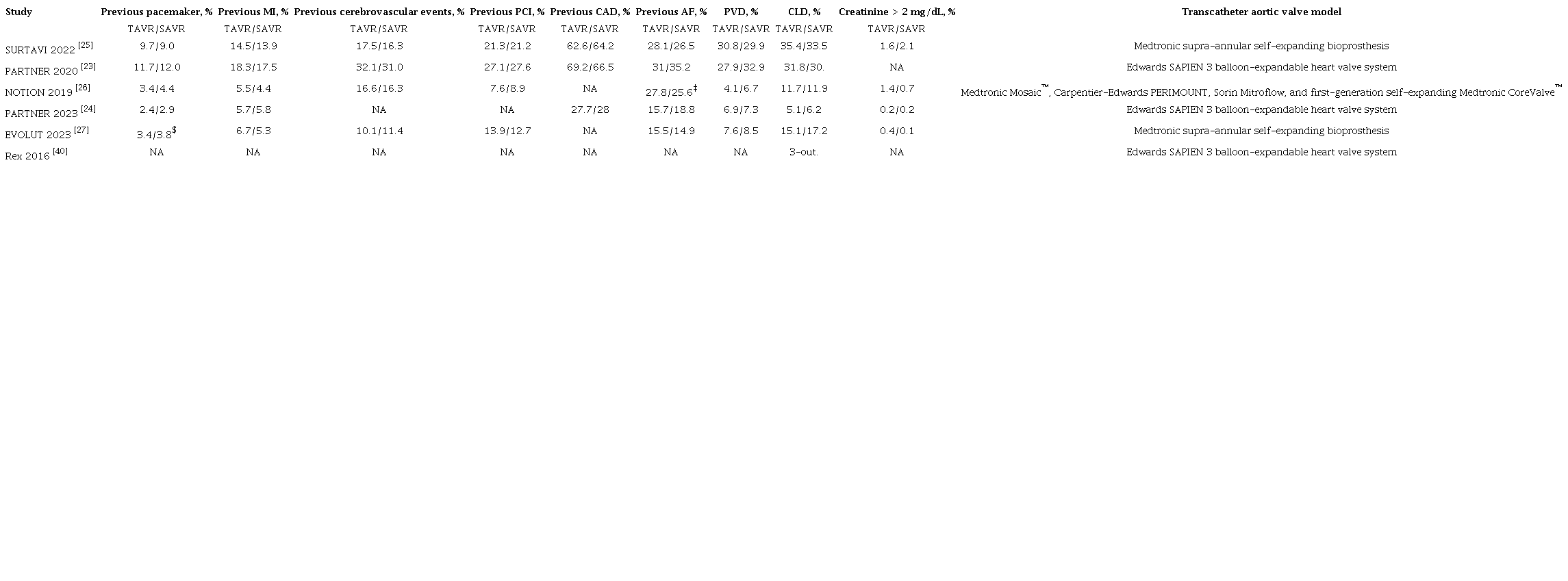
reported in Table 1. A total of 3,286
(51%) patients were treated with TAVR. The follow-up ranged between four and
five years. The mean patient age was 78.4 years. There were 2,170 (66%) and
1,905 (59.3%) male patients in the TAVR and SAVR group, respectively. The mean
Society of Thoracic Surgeons (STS) score of the included studies was 3.86.
Table 1
Baseline characteristics of included studies.
 * Data are presented as mean ± standard deviation;** The article did not specify the type of diabetes DM=diabetes mellitus; NYHA=New York Heart Association; SAVR=surgical
aortic valve replacement; STS=Society of Thoracic Surgeons;
TAVR=transcatheter aortic valve replacement‡ The article included atrial fibrillation and atrial flutter in the
same data;$ The article included pacemaker and defibrillator in the same data AF=atrial fibrillation; CAD=coronary artery disease; CLD=chronic lung
disease; MI=myocardial infarction; NA=data not available;
PCI=percutaneous coronary intervention; PVD=peripheral vascular
disease; SAVR=surgical aortic valve replacement; TAVR=transcatheter
aortic-valve replacement
* Data are presented as mean ± standard deviation;** The article did not specify the type of diabetes DM=diabetes mellitus; NYHA=New York Heart Association; SAVR=surgical
aortic valve replacement; STS=Society of Thoracic Surgeons;
TAVR=transcatheter aortic valve replacement‡ The article included atrial fibrillation and atrial flutter in the
same data;$ The article included pacemaker and defibrillator in the same data AF=atrial fibrillation; CAD=coronary artery disease; CLD=chronic lung
disease; MI=myocardial infarction; NA=data not available;
PCI=percutaneous coronary intervention; PVD=peripheral vascular
disease; SAVR=surgical aortic valve replacement; TAVR=transcatheter
aortic-valve replacement
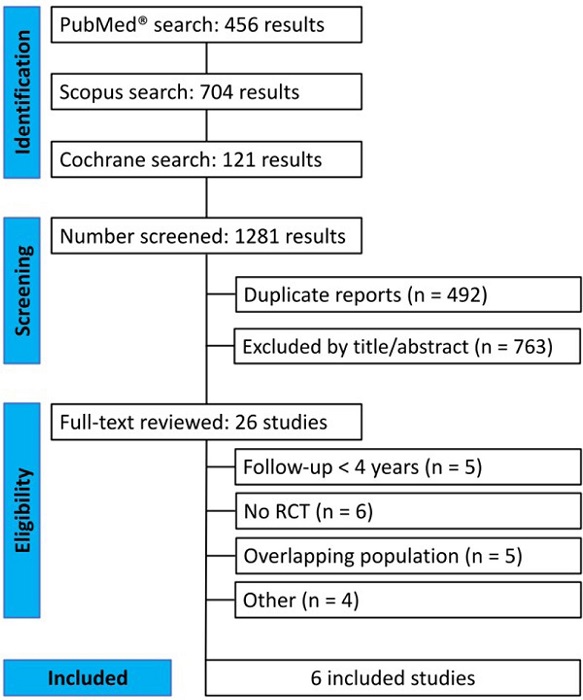 Fig. 1
Preferred Reporting Items for Systematic Reviews and
Meta-Analysis (or PRISMA) flow diagram of study screening selection.
RCT=randomized controlled trial.
Fig. 1
Preferred Reporting Items for Systematic Reviews and
Meta-Analysis (or PRISMA) flow diagram of study screening selection.
RCT=randomized controlled trial.
Pooled Analyses of All Studies
There was no statistically significant difference between groups in all-cause
mortality (RR 1.08; 95% CI 0.94 - 1.25; P = 0.30; I2
= 45%) (Figure 2), cardiovascular mortality
(RR 1.09; 95% CI 0.96 - 1.23; P = 0.17; I2 = 0%),
stroke (RR 1.04; 95% CI 0.85 - 1.26; P = 0.73; I2 =
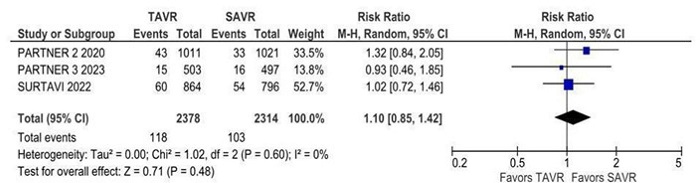
18%), disabling stroke (RR 0.95; 95% CI 0.75 - 1.21; P = 0.67;
I2 = 9%) (Figure 3),
non-disabling stroke (RR 1.10; 95% CI 0.85 - 1.42; P = 0.71;
I2 = 0%), endocarditis (RR 1.33; 95% CI 0.85 - 2.09;
P = 0.21; I2 = 0%) (Supplementary Figure 1), myocardial infarction (RR 1.11; 95%
CI 0.76 - 1.63; P = 0.58; I2 = 50%), and
rehospitalization (RR 1.07; 95% CI 0.85 - 1.36; P = 0.55;
I2 = 76%).
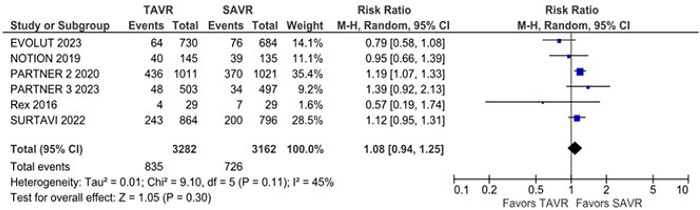 Fig. 2
All-cause mortality was not significantly different between
surgical aortic valve replacement (SAVR) and transcatheter aortic
valve replacement (TAVR). CI=confidence interval.
Fig. 2
All-cause mortality was not significantly different between
surgical aortic valve replacement (SAVR) and transcatheter aortic
valve replacement (TAVR). CI=confidence interval.
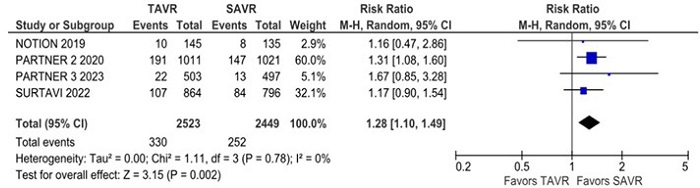 Fig. 3
Disabling stroke was not significantly different between groups.
CI=confidence interval; SAVR=surgical aortic valve replacement;
TAVR=transcatheter aortic valve replacement.
Fig. 3
Disabling stroke was not significantly different between groups.
CI=confidence interval; SAVR=surgical aortic valve replacement;
TAVR=transcatheter aortic valve replacement.
Non-cardiovascular mortality was significantly higher in the TAVR group compared
with the SAVR group (RR 1.28; 95% CI 1.10 - 1.49; P = 0.002;
I2 = 0%) (Figure 4). The
rate of new pacemaker implantation was also significantly higher in the TAVR
group compared with the SAVR group (RR 2.22; 95% CI 1.42 - 3.45;
P = 0.0004; I2 = 91%) (Figure 5). New atrial fibrillation was significantly lower
in the TAVR group compared with the SAVR group (RR 0.40; 95% CI 0.31 - 0.52;
P = 0.00001; I2 = 68%) (Figure 6).
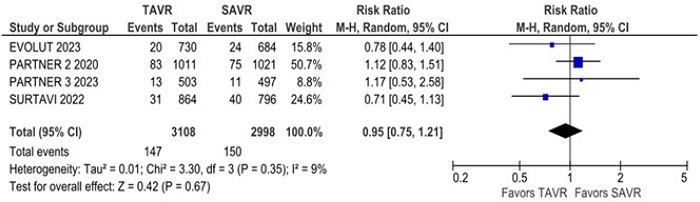 Fig. 4
Non-cardiovascular mortality was significantly higher in the
transcatheter aortic valve replacement (TAVR) group. CI=confidence
interval; SAVR=surgical aortic valve replacement.
Fig. 4
Non-cardiovascular mortality was significantly higher in the
transcatheter aortic valve replacement (TAVR) group. CI=confidence
interval; SAVR=surgical aortic valve replacement.
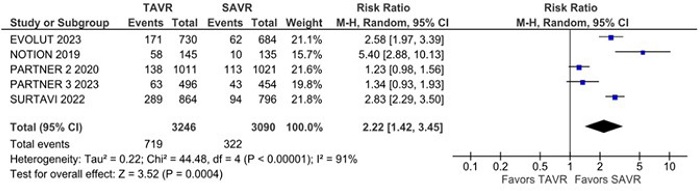 Fig. 5
New pacemaker implantation was significantly higher in the
transcatheter aortic valve replacement (TAVR) group. CI=confidence
interval; SAVR=surgical aortic valve replacement.
Fig. 5
New pacemaker implantation was significantly higher in the
transcatheter aortic valve replacement (TAVR) group. CI=confidence
interval; SAVR=surgical aortic valve replacement.
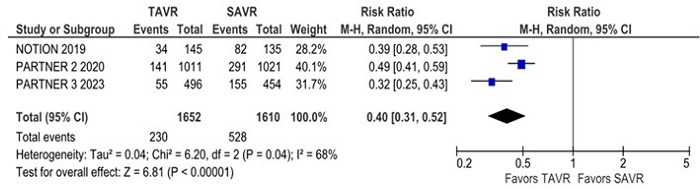 Fig. 6
New atrial fibrillation was significantly lower in the
transcatheter aortic valve replacement (TAVR) group. CI=confidence
interval; SAVR=surgical aortic valve replacement.
Fig. 6
New atrial fibrillation was significantly lower in the
transcatheter aortic valve replacement (TAVR) group. CI=confidence
interval; SAVR=surgical aortic valve replacement.
Subgroup Analysis
The risk of all-cause mortality was significantly higher in the TAVR group
compared with the SAVR group over five years of follow-up (RR 1.28; 95% CI 1.10
- 1.49; P = 0.002; I2 = 0%) (Figure 7). There was no statistically significant difference
in all-cause mortality between TAVR and SAVR in patients at low surgical risk
(RR 0.96; 95% CI 0.71 - 1.29; P = 0.77; I2 =
44%).
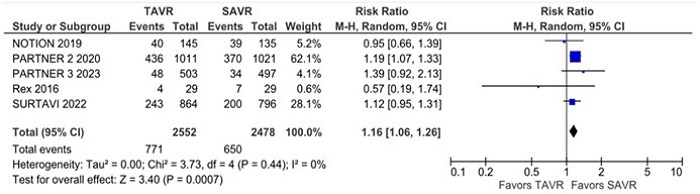 Fig. 7
Subanalysis of studies with five years of follow up, all-cause
mortality was significantly higher in the transcatheter aortic valve
replacement (TAVR) group. CI=confidence interval; SAVR=surgical
aortic valve replacement.
Fig. 7
Subanalysis of studies with five years of follow up, all-cause
mortality was significantly higher in the transcatheter aortic valve
replacement (TAVR) group. CI=confidence interval; SAVR=surgical
aortic valve replacement.
The leave-one-out analysis demonstrated the robustness of the pooled results for
stroke (Supplementary Figure 2). However,
the leave-one-out analysis for all-cause mortality showed that the omission of
the EVOLUT trial reduced heterogeneity to 0% and led to statistically
significant results (Supplementary Figure
3).
Quality Assessment
Individual RCT appraisal is reported in Supplementary Table 1. We used version 2 of the Cochrane Risk of
Bias assessment tool (RoB 2) to assess the individual overall risk of bias
publication of the RCTs in this meta-analysis. Two studies were classified as
low risk of bias, whereas three studies were evaluated as having some concerns
in risk of bias mainly due to deviations from intended interventions. One study
was evaluated at high risk due to the selection of the reported results, as the
article did not report all outcomes pre-specified in its protocol (Supplementary Table 1).
High rates of heterogeneity were present in this analysis for outcomes, such as
all-cause mortality, myocardial infarction, and rehospitalization. The present
variation in data is possible due to the different types of prostheses used in
each study, variability in healthcare settings, variability in medical expertise
(years of practice), differences in patients-associated comorbidities, and
inclusion of studies with less methodological rigor marked as “some
concerns” or “high concerns” for risk of bias.
DISCUSSION
This systematic review with meta-analysis of RCTs comprising > 6,000
low-to-moderate risk patients with severe AS compared mid-term outcomes between SAVR
and TAVR. Our main findings were: (1) there was no significant difference between
groups in terms of all-cause mortality, stroke, endocarditis, myocardial infarction,
and rehospitalization; (2) there was a higher risk of non-cardiovascular death and
new pacemaker implantation in the TAVR group compared with the SAVR group; and (3)
there was a reduced risk of atrial fibrillation in the TAVR group when compared with
the SAVR group.
Despite the established efficacy and safety of TAVR in high-risk cases, the extension
of its application to those with lower or intermediate surgical risk requires a
thorough evaluation of outcomes in mid and long-term follow-up. Our results suggest
that the use of TAVR over a mid-term follow-up showed similar risk in all-cause
mortality and stroke rates when compared with SAVR in patients with AS. These
findings align with results from previous meta-analyses with shorter
follow-up[17,18,29–31]. In the
PARTNER 2 trial, there was no significant difference in all-cause mortality or
disabling stroke when compared with SAVR[23]. These findings were subsequently corroborated by the
PARTNER 3, SURTAVI, and NOTION trials[24-26], all of which
confirmed no significant differences between the groups for all-cause mortality.
A recent meta-analysis including low-surgical-risk patients demonstrated a reduction
in the risk of all-cause mortality and disabling stroke at one year in the TAVR
group. However, a mid-term analysis with an average follow-up of 4.3 years showed no
difference between the groups for these same outcomes[32]. Nevertheless, a subgroup analysis of studies
with five years of follow-up showed a significantly higher risk of all-cause
mortality in the TAVR group when compared with the SAVR group. These findings are
consistent with the PARTNER 2 study, which showed an increased risk of all-cause
mortality in the TAVR group when compared with the SAVR group[23]. These different results between
the individual studies may be explained by the use of different transcatheter
systems that present different clinical performance and durability. The device
(SAPIEN XT) used in the PARTNER 2 study is no longer in clinical practice and it was
related to higher mortality and neurological events in the medium and long term when
compared with other newer devices[23,33]. Therefore, our
results of all-cause mortality over five years may be justified by the durability of
the prostheses used in the TAVR group.
In addition, our leave-one-out sensitivity analysis for all-cause mortality showed
that omitting the EVOLUT trial significantly reduced heterogeneity from 40% to 0%,
with a statistically significant difference unfavoring TAVR when compared with SAVR
in patients with AS and low to moderate surgical risk. The EVOLUT trial demonstrated
the greatest benefit of TAVR over SAVR for all-cause mortality among included
studies[27]. This may be
explained by the use of a high-performance valve with advanced technology and higher
loss to follow-up in the SAVR group. A previous meta-analysis compared mid-term
outcomes between the two techniques including low, intermediate, and high-risk
patients, and it showed that the advantages of TAVR over SAVR are not consistent
over time, with longer follow-up revealing results favoring surgery[34].
Increased survival rates with TAVR in high-risk patients is largely due to reduced
cardiovascular mortality[16].
However, non-cardiovascular and non-categorizable causes contributed significantly
to the mortality of these patients. Our findings suggest a higher risk of death from
non-cardiovascular causes for TAVR when compared with SAVR in patients with AS and
low to moderate surgical risk (RR 1.28). Although several clinical trials showed a
greater number of deaths from non-cardiovascular causes in the TAVR group when
compared with the SAVR group in patients with AS and low to moderate surgical risk,
these results were not statistically significant[25,26]. A
previous meta-analysis identified infections/sepsis as the leading cause of
non-cardiovascular death within 30 days and the second cause of death after 30
days[30]. Although TAVR is
a minimally invasive procedure, patients generally present factors alone or in
combination that predispose to infection, including age; poor lung, kidney, and
immune function; diabetes; and need for ventilation and central venous access and
monitoring[35].
Our analysis revealed no difference in rehospitalization between the TAVR and SAVR
groups in patients with AS and low to moderate surgical risk. In the PARTNER 3
study, 1,000 patients with severe AS and low surgical risk were randomized to TAVR
or SAVR. In the intention-to-treat analysis during five years of follow-up, there
was no difference in rehospitalization between the groups[24]. The same results were found in the SURTAVI
study, which showed no difference in readmission between the groups[26]. However, these results differ
from the PARTNER 2 study, which showed a higher risk of readmission for TAVR when
compared to SAVR at five years in patients with AS and low to moderate surgical
risk[23]. Previous
literature identified valve stenosis or regurgitation for TAVR and endocarditis for
SAVR as the main causes of hospitalization[36]. Our findings may be explained by the fact that the
studies used different devices for TAVR. Different transcatheter models are
associated with different risks of complications, often requiring
reintervention[26].
The findings of this systematic review with meta-analysis show a higher risk of
pacemaker implantation in the TAVR group when compared with SAVR in patients with AS
and low to moderate surgical risk, which is consistent with previously published
literature[17,26,27,37]. Despite the
high risk of pacemaker implantation in the TAVR group, this risk varies between
different studies, from 5.40 to 1.23. The NOTION study was the first RCT to study
low-risk patients and it was the study with the highest risk of pacemaker
implantation[26].
Subsequent studies showed an increasingly lower risk of pacemaker
implantation[23,25,27]. The PARTNER 2 and 3 trials showed the lowest risks for
pacemaker implantation[23,24]. Several factors may influence
this variation in risks, such as studies using different devices for TAVR. In the
PARTNER studies, different from the NOTION study, third-generation devices were
used. SAPIEN 3, which is the latest transcatheter heart valve in the Edwards family,
incorporates a number of new and improved features and it also appeared to have a
more favorable clinical profile in terms of clinical and valve performance with
fewer complications, including a lower risk of implanting a new pacemaker[38].
Literature has shown differences in clinical outcomes when comparing different
transcatheter valve systems with surgical valves. The second-generation
balloon-expandable transcatheter valve has a higher risk of structural valve
degeneration than the surgical valve[38,39]. The
third-generation balloon-expandable transcatheter heart valve (SAPIEN 3, Edwards
Lifesciences) appeared to have a more favorable clinical profile in terms of
clinical outcomes and valve performance[33].
Our results showed a reduced incidence of atrial fibrillation in the TAVR group when
compared with the SAVR group in patients with AS and low to moderate surgical risk.
In the PARTNER 2 study, 2023 patients with symptomatic severe AS and intermediate
surgical risk were randomized to TAVR or SAVR and followed for five years. The risk
of atrial fibrillation was twice as high in the SAVR group when compared with the
TAVR group, and the same results were reported in previous literature. Other
statistically non-significant results from our analyses also deserve comment: TAVR
may not be associated with fewer outcomes of endocarditis and myocardial infarction
when compared with SAVR in a medium follow-up period, and these results are
consistent with previous reports[23,24,26].
SAVR is a safe technique with significantly low operative mortality in selected
elderly patients, but it increases with the number and severity of comorbidities,
imposing an important limitation on SAVR[10]. Medium- and long-term outcomes vary widely, with survival
rates ranging from 37.4% to 64%[40-42]. These results are significantly
influenced by the patient’s age and the presence of comorbidities. Structural
valve degeneration, which limits its durability, represents the main limitation of
biological tissue[10]. It is
evident that following the advent of TAVR, SAVR outcomes have significantly
improved, likely because higher-risk patients were increasingly referred for
TAVR[43]. TAVR is a
minimally invasive and safe technique, but certain complex anatomical
characteristics such as the access site, pathway, and valve implantation site can
hinder its successful use or even contraindicate TAVR[44]. Although initially tested in high-surgical-risk
patients, its use has expanded to those with moderate and even low risk. Due to its
minimally invasive nature, TAVR avoids sternotomy and cardiopulmonary bypass,
potentially reducing resource utilization by accelerating patient recovery and
shortening hospital stays[45]. The
NOTION study recruited participants in the early 2010s and used the self-expanding
CoreValve™ system, showing a similar risk of the composite endpoint for TAVR
and SAVR at five and eight years. Among studies with mid-term follow-up, the EVOLUT
Low Risk trial demonstrated a lower risk of all-cause mortality in the TAVR group
(6.3%) when compared to the SAVR group (12.4%). This study utilized self-expanding
aortic valves, Evolut™ R and Evolut™ PRO. In the PARTNER 3 trial,
which investigated the balloon-expandable SAPIEN 3 valve, the four-year mortality
rate was slightly higher in the TAVR group (7.4%) when compared to the SAVR group
(5.9%)[24,27,38].
The overall composite endpoint rate in the NOTION study was higher than in the EVOLUT
LOW RISK and PARTNER 3 studies. This is likely related to a higher mean STS score
among NOTION participants, as well as the use of non-contemporary valve technology
and medical therapy. Recently, a systematic review and network meta-analysis
compared different transcatheter heart valves with SAVR. The study showed a similar
risk of all-cause mortality among the groups. However, the risk of disabling stroke
was lower with mechanically expandable valves when compared to balloon-expandable
valves and SAVR, and it was also lower with self-expanding valves when compared to
SAVR in the long term. On the other hand, mechanically expandable valves were
associated with a higher risk of pacemaker implantation when compared to other
systems and SAVR[46].
Limitations
This systematic review with meta-analysis has some limitations. Most importantly,
none of the studies were blinded — a fundamental limitation arising from
the nature of the interventions. There was, also, some variability in the
follow-up time between studies. To minimize such heterogeneities, we performed
subgroup analysis in studies comparing TAVR vs. SAVR with a
follow-up higher than four years. Furthermore, there were important differences
in the types of prostheses used in the studies. This difference, unfortunately,
can impact negatively on the clinical applicability of our results across
diverse contexts. Finally, significant heterogeneity was found in the outcome of
all-cause mortality. However, the leave-one-out sensitivity analysis showed the
robustness of the overall findings.
CONCLUSION
The results of this meta-analysis, including over 6,000 patients with AS and low to
moderate surgical risk, suggest TAVR is non-inferior to SAVR regarding all-cause
mortality or stroke in the mid-term period. Although both procedures are safe, the
choice of treatment must be individualized and made together with the patient and
the heart valve team.
Appendices
 Supplementary Figure 1
Forest plot for endocarditis comparing transcatheter aortic valve
replacement (TAVR) with surgical aortic valve replacement (SAVR).
CI=confidence interval.
Supplementary Figure 1
Forest plot for endocarditis comparing transcatheter aortic valve
replacement (TAVR) with surgical aortic valve replacement (SAVR).
CI=confidence interval.
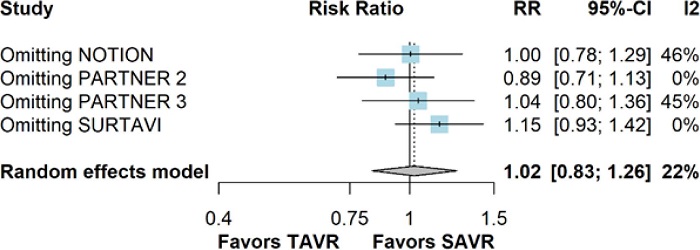 Supplementary Figure 2
Leave-one-out analysis for stroke. CI=confidence interval;
RR=risk ratio; SAVR=surgical aortic valve replacement;
TAVR=transcatheter aortic valve replacement.
Supplementary Figure 2
Leave-one-out analysis for stroke. CI=confidence interval;
RR=risk ratio; SAVR=surgical aortic valve replacement;
TAVR=transcatheter aortic valve replacement.
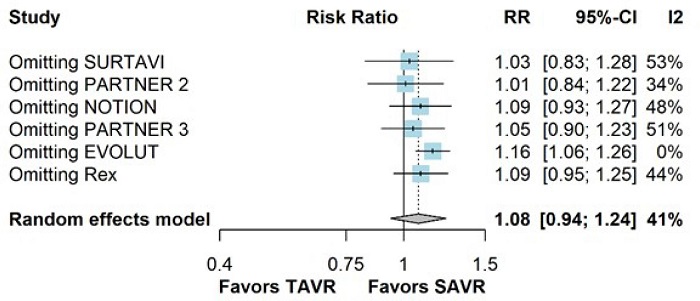 Supplementary Figure 3
Leave-one-out analysis for all-cause mortality. CI=confidence
interval; RR=risk ratio; SAVR=surgical aortic valve replacement;
TAVR=transcatheter aortic valve replacement.
Supplementary Figure 3
Leave-one-out analysis for all-cause mortality. CI=confidence
interval; RR=risk ratio; SAVR=surgical aortic valve replacement;
TAVR=transcatheter aortic valve replacement.
Supplementary Table 1
Critical appraisal of individual studies according to the Cochrane
Collaboration’s tool for assessing risk of bias in randomized
trials.

ACKNOWLEDGMENTS
The authors would like to thank Camila Guida, MD, for the careful review of this
manuscript.
REFERENCES
Iung B, Delgado V, Rosenhek R, Price S, Prendergast B, Wendler O, et
al. Contemporary presentation and management of valvular heart disease: the
EURObservational research programme valvular heart disease II survey.
Circulation. 2019;140(14):1156-69.
doi:10.1161/CIRCULATIONAHA.119.041080.
Sinning JM, Baumgart D, Werner N, Klauss V, Baer FM, Hartmann F, et
al. Five-year results of the multicenter randomized controlled open-label study
of the CYPHER sirolimus-eluting stent in the treatment of diabetic patients with
de novo native coronary artery lesions (SCORPIUS) study: a German multicenter
investigation on the effectiveness of sirolimus-eluting stents in diabetic
patients. Am Heart J. 2012;163(3):446-53, 453.e1.
doi:10.1016/j.ahj.2011.12.010.
Yadgir S, Johnson CO, Aboyans V, Adebayo OM, Adedoyin RA, Afarideh
M, et al. Global, regional, and national burden of calcific aortic valve and
degenerative mitral valve diseases, 1990-2017. Circulation.
2020;141(21):1670-80. doi:10.1161/CIRCULATIONAHA.119.043391. Erratum in:
Circulation. 2020;141(21):e836.
doi:10.1161/CIR.0000000000000848.
Bhatia N, Basra SS, Skolnick AH, Wenger NK. Aortic valve disease in
the older adult. J Geriatr Cardiol. 2016;13(12):941-4.
doi:10.11909/j.issn.1671-5411.2016.12.004.
Osnabrugge RL, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun
CM, et al. Aortic stenosis in the elderly: disease prevalence and number of
candidates for transcatheter aortic valve replacement: a meta-analysis and
modeling study. J Am Coll Cardiol. 2013;62(11):1002-12.
doi:10.1016/j.jacc.2013.05.015.
Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al.
2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur
Heart J. 2017;38(36):2739-91. doi:10.1093/eurheartj/ehx391.
Kodali S, Thourani VH, White J, Malaisrie SC, Lim S, Greason KL, et
al. Early clinical and echocardiographic outcomes after SAPIEN 3 transcatheter
aortic valve replacement in inoperable, high-risk and intermediate-risk patients
with aortic stenosis. Eur Heart J. 2016;37(28):2252-62.
doi:10.1093/eurheartj/ehw112.
Latif A, Ahsan MJ, Lateef N, Kapoor V, Mirza MM, Anwer F, et al.
Outcomes of surgical versus transcatheter aortic valve replacement in
nonagenarians- a systematic review and meta-analysis. J Community Hosp Intern
Med Perspect. 2021;11(1):128-34.
doi:10.1080/20009666.2020.1843235.
Kvidal P, Bergström R, Hörte LG, Ståhle E.
Observed and relative survival after aortic valve replacement. J Am Coll
Cardiol. 2000;35(3):747-56. doi:10.1016/s0735-1097(99)00584-7.
Rodriguez-Gabella T, Voisine P, Dagenais F, Mohammadi S, Perron J,
Dumont E, et al. Long-term outcomes following surgical aortic bioprosthesis
implantation. J Am Coll Cardiol. 2018;71(13):1401-12.
doi:10.1016/j.jacc.2018.01.059.
Assmann A, Minol JP, Mehdiani A, Akhyari P, Boeken U, Lichtenberg A.
Cardiac surgery in nonagenarians: not only feasible, but also reasonable?
Interact Cardiovasc Thorac Surg. 2013;17(2):340-3; discussion 343.
doi:10.1093/icvts/ivt125.
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd,
Fleisher LA, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline
for the management of patients with valvular heart disease: a report of the
American college of cardiology/American heart association task force on clinical
practice guidelines. Circulation. 2017;135(25):e1159-95.
doi:10.1161/CIR.0000000000000503.
Thourani VH, Suri RM, Gunter RL, Sheng S, O'Brien SM, Ailawadi
G, et al. Contemporary real-world outcomes of surgical aortic valve replacement
in 141,905 low-risk, intermediate-risk, and high-risk patients. Ann Thorac Surg.
2015;99(1):55-61. doi:10.1016/j.athoracsur.2014.06.050.
Oguri A, Yamamoto M, Mouillet G, Gilard M, Laskar M, Eltchaninoff H,
et al. Clinical outcomes and safety of transfemoral aortic valve implantation
under general versus local anesthesia: subanalysis of the French aortic national
CoreValve and Edwards 2 registry. Circ Cardiovasc Interv. 2014;7(4):602-10.
doi:10.1161/CIRCINTERVENTIONS.113.000403.
Grube E, Buellesfeld L, Mueller R, Sauren B, Zickmann B, Nair D, et
al. Progress and current status of percutaneous aortic valve replacement:
results of three device generations of the CoreValve Revalving system. Circ
Cardiovasc Interv. 2008;1(3):167-75.
doi:10.1161/CIRCINTERVENTIONS.108.819839.
Grube E, Schuler G, Buellesfeld L, Gerckens U, Linke A, Wenaweser P,
et al. Percutaneous aortic valve replacement for severe aortic stenosis in
high-risk patients using the second- and current third-generation self-expanding
CoreValve prosthesis: device success and 30-day clinical outcome. J Am Coll
Cardiol. 2007;50(1):69-76. doi:10.1016/j.jacc.2007.04.047.
Elmaraezy A, Ismail A, Abushouk AI, Eltoomy M, Saad S, Negida A, et
al. Efficacy and safety of transcatheter aortic valve replacement in aortic
stenosis patients at low to moderate surgical risk: a comprehensive
meta-analysis. BMC Cardiovasc Disord. 2017;17(1):234.
doi:10.1186/s12872-017-0668-1.
Garg A, Rao SV, Visveswaran G, Agrawal S, Sharma A, Garg L, et al.
Transcatheter aortic valve replacement versus surgical valve replacement in
low-intermediate surgical risk patients: a systematic review and meta-analysis.
J Invasive Cardiol. 2017;29(6):209-16.
Escaned J, Cao D, Baber U, Nicolas J, Sartori S, Zhang Z, et al.
Ticagrelor monotherapy in patients at high bleeding risk undergoing percutaneous
coronary intervention: TWILIGHT-HBR. Eur Heart J. 2021;42(45):4624-34.
doi:10.1093/eurheartj/ehab702.
European Union Clinical Trials Register. Left Ventricular Thrombus
Formation after Acute Myocardial Infarction – a randomized multi-center
trial comparing 2 different anti-thrombotic regimens [Internet]. EudraCT number:
2011-004265-32. Amsterdam (NL): European Medicines Agency; 2011 [cited 2025 Aug
31]. Available from: https://www.clinicaltrialsregister.eu/ctr-search/trial/2011-004265-32/NL
ToetsingOnline. GLOBAL LEADERS: Comparative effectiveness of 1 month
of ticagrelor plus aspirin followed by ticagrelor monotherapy versus a
current-day intensive dual antiplatelet therapy in all-comers patients
undergoing percutaneous coronary intervention with bivalirudin and BioMatrix
family drug-eluting stent use [Internet]. Trial ID: NL-OMON44752. Rotterdam
(NL): ECRI/Cardialysis; 2013 [cited 2025 Aug 31]. Available from: https://www.trialregister.nl/trial/44752
European Union Clinical Trials Register. Randomized Evaluation of
short-term DUal anti platelet therapy in patients with acute coronary syndrome
treated with the COMBO dual-therapy stEnt (REDUCE) [Internet]. EudraCT number:
2013-005571-40; Trial ID: NCT02118870. Zwolle (NL): Diagram B.V.; 2014 [cited
2025 Aug 31]. Available from: https://www.clinicaltrialsregister.eu/ctr-search/trial/2013-005571-40/DE/
Makkar RR, Thourani VH, Mack MJ, Kodali SK, Kapadia S, Webb JG, et
al. Five-year outcomes of transcatheter or surgical aortic-valve replacement. N
Engl J Med. 2020;382(9):799-809. doi:10.1056/NEJMoa1910555.
Mack MJ, Leon MB, Thourani VH, Pibarot P, Hahn RT, Genereux P, et
al. Transcatheter aortic-valve replacement in low-risk patients at five years. N
Engl J Med. 2023;389(21):1949-60. doi:10.1056/NEJMoa2307447.
Van Mieghem NM, Deeb GM, Søndergaard L, Grube E, Windecker S,
Gada H, et al. Self-expanding transcatheter vs surgical aortic valve replacement
in intermediate-risk patients: 5-year outcomes of the SURTAVI randomized
clinical trial. JAMA Cardiol. 2022;7(10):1000-8.
doi:10.1001/jamacardio.2022.2695.
Søndergaard L, Ihlemann N, Capodanno D, Jørgensen TH,
Nissen H, Kjeldsen BJ, et al. Durability of transcatheter and surgical
bioprosthetic aortic valves in patients at lower surgical risk. J Am Coll
Cardiol. 2019;73(5):546-53. doi:10.1016/j.jacc.2018.10.083.
Forrest JK, Deeb GM, Yakubov SJ, Gada H, Mumtaz MA, Ramlawi B, et
al. 4-year outcomes of patients with aortic stenosis in the evolut low risk
trial. J Am Coll Cardiol. 2023;82(22):2163-5.
doi:10.1016/j.jacc.2023.09.813.
Seiffert M, Vonthein R, Baumgartner H, Borger MA, Choi YH, Falk V,
et al. Transcatheter aortic valve implantation versus surgical aortic valve
replacement in patients at low to intermediate surgical risk: rationale and
design of the randomised DEDICATE Trial. EuroIntervention. 2023;19(8):652-8.
doi:10.4244/EIJ-D-23-00232.
Forrest JK, Deeb GM, Yakubov SJ, Rovin JD, Mumtaz M, Gada H, et al.
2-year outcomes after transcatheter versus surgical aortic valve replacement in
low-risk patients. J Am Coll Cardiol. 2022;79(9):882-96.
doi:10.1016/j.jacc.2021.11.062.
Xiong TY, Liao YB, Zhao ZG, Xu YN, Wei X, Zuo ZL, et al. Causes of
death following transcatheter aortic valve replacement: a systematic review and
meta-analysis. J Am Heart Assoc. 2015;4(9):e002096.
doi:10.1161/JAHA.115.002096.
Mc Morrow R, Kriza C, Urbán P, Amenta V, Amaro JAB, Panidis
D, et al. Assessing the safety and efficacy of TAVR compared to SAVR in
low-to-intermediate surgical risk patients with aortic valve stenosis: an
overview of reviews. Int J Cardiol. 2020;314:43-53.
doi:10.1016/j.ijcard.2020.04.022.
Rahman H, Ghosh P, Nasir F, Khan MA, Rehman N, Sharma S, et al.
Short- and intermediate-term outcomes of transcatheter aortic valve replacement
in low-risk patients: a meta-analysis and systematic review. Int J Cardiol Heart
Vasc. 2024;53:101458. doi:10.1016/j.ijcha.2024.101458.
Halapas A, Chrissoheris M, Bouboulis N, Skardoutsos S, Nikolaou I,
Pattakos S, et al. The SAPIEN-XT and SAPIEN-3 Valves: how to implant and obtain
the best outcomes. Hellenic J Cardiol. 2015;56 Suppl A:9-14.
Barili F, Freemantle N, Musumeci F, Martin B, Anselmi A, Rinaldi M,
et al. Five-year outcomes in trials comparing transcatheter aortic valve
implantation versus surgical aortic valve replacement: a pooled meta-analysis of
reconstructed time-to-event data. Eur J Cardiothorac Surg. 2022;61(5):977-87.
doi:10.1093/ejcts/ezab516.
Falcone M, Russo A, Mancone M, Carriero G, Mazzesi G, Miraldi F, et
al. Early, intermediate and late infectious complications after transcatheter or
surgical aortic-valve replacement: a prospective cohort study. Clin Microbiol
Infect. 2014;20(8):758-63. doi:10.1111/1469-0691.12470.
Summers MR, Leon MB, Smith CR, Kodali SK, Thourani VH, Herrmann HC,
et al. Prosthetic valve endocarditis after TAVR and SAVR: insights from the
PARTNER trials. Circulation. 2019;140(24):1984-94.
doi:10.1161/CIRCULATIONAHA.119.041399.
Khan AR, Khan S, Riaz H, Luni FK, Simo H, Bin Abdulhak A, et al.
Efficacy and safety of transcatheter aortic valve replacement in intermediate
surgical risk patients: a systematic review and meta-analysis. Catheter
Cardiovasc Interv. 2016;88(6):934-44. doi:10.1002/ccd.26465.
Facchin M, Mojoli M, Covolo E, Tarantini G. The SAPIEN 3 valve:
lights and shadows. Minerva Med. 2014;105(6):497-500.
Rotman OM, Bianchi M, Ghosh RP, Kovarovic B, Bluestein D. Principles
of TAVR valve design, modelling, and testing. Expert Rev Med Devices.
2018;15(11):771-91. doi:10.1080/17434440.2018.1536427.
Rex CE, Heiberg J, Klaaborg KE, Hjortdal VE. Health-related
quality-of-life after transapical transcatheter aortic valve implantation. Scand
Cardiovasc J. 2016;50(5-6):377-382. doi:
10.1080/14017431.2016.1235725.
Ueyama H, Kuno T, Ando T, Hayashida K, Takagi H. Network
meta-analysis of surgical aortic valve replacement and different transcatheter
heart valve systems for symptomatic severe aortic stenosis. Can J Cardiol.
2021;37(1):27-36. doi:10.1016/j.cjca.2020.02.088.
David TE, Armstrong S, Maganti M. Hancock II bioprosthesis for
aortic valve replacement: the gold standard of bioprosthetic valves durability?
Ann Thorac Surg. 2010;90(3):775-81.
doi:10.1016/j.athoracsur.2010.05.034.
Jamieson WR, Burr LH, Miyagishima RT, Germann E, Macnab JS, Stanford
E, et al. Carpentier-Edwards supra-annular aortic porcine bioprosthesis:
clinical performance over 20 years. J Thorac Cardiovasc Surg.
2005;130(4):994-1000. doi:10.1016/j.jtcvs.2005.03.040.
Martin E, Dagenais F, Voisine P, Dumont E, Charbonneau E, Baillot R,
et al. Surgical aortic valve replacement outcomes in the transcatheter era. J
Thorac Cardiovasc Surg. 2015;150(6):1582-8.
doi:10.1016/j.jtcvs.2015.08.077.
Saad M, Seoudy H, Frank D. Challenging anatomies for TAVR-bicuspid
and beyond. Front Cardiovasc Med. 2021;8:654554.
doi:10.3389/fcvm.2021.654554.
Kilinc AY, Ucar M. Transcatheter aortic valve replacement technique
and current approaches. In: Rao PS, editor. Aortic valve disease – recent
advances [Internet]. London: IntechOpen; 2023 [cited 2025 Aug 31]. p. [approx.
7]. doi:10.5772/intechopen.111904.
Notes
Notes
Artificial Intelligence Usage The authors declare that no generative artificial intelligence tools were used in
the writing, editing, or analysis of this manuscript. All content was produced
solely by the authors
Sources of funding There were no external funding sources for this study.
This study was carried out at the Universidade Agostinho Neto, Luanda,
Angola.
Conflict of interest declaration
Potential conflict of interest No potential conflict of interest relevant to this article was reported.
Author notes
Editor-in-chief Paulo Roberto B. Evora (in memoriam)
Correspondence Address: Valdano Manuel, Complexo
Hospitalar de Doenças Cardio-Pulmonares Cardeal Dom, Alexandre do
Nascimento, Av. Pedro de Castro Van-Dunem Loy, 21, Luanda, Angola, Zip Code:
15150, E-mail: valdanympub@gmail.com