A 72-year-old male with a history of hypertension and dyslipidemia presented with
stable angina. An echocardiogram revealed preserved biventricular function. Nuclear
myocardial perfusion imaging demonstrated ischemia in the anterior and lateral
coronary territories. Coronary angiography revealed severe multivessel disease,
including significant stenosis of the distal left main proximal LAD, proximal obtuse
marginal 1 (OM1), and posterolateral artery (PL). Fractional flow reserve assessment
of the right coronary artery revealed a value > 0.8, excluding hemodynamically
significant lesions.
Preoperative Planning
After discussion with the heart team and the patient, a hybrid revascularization
approach was selected. This involved robot-assisted CABG with BIMA grafting,
with the right internal mammary artery (RIMA) anastomosed to the LAD and the
left internal mammary artery (LIMA) grafted to the OM1, followed by PCI for the
PL lesion.
Patient Preparation
Patient preparation is critical for a successful robotic BIMA harvest. Under
general anesthesia, a double-lumen endotracheal tube facilitates single-lung
ventilation. The patient is positioned supine with a slight left chest elevation
with a roll under the left scapula, ensuring optimal access to the left thoracic
cavity. Both arms are secured alongside the torso. Defibrillator pads are placed
on the right infraclavicular area and the left posterior chest. The groins are
made available to access if needed, and the cardiopulmonary bypass (CPB) machine
and a perfusionist are on standby during the procedure if required. The legs are
exposed for potential saphenous vein harvest.
Surgical Technique
Port Placement and Robotic Setup
In the left thorax, the ports are inserted. A 12 mm camera port is inserted
in the fifth intercostal space (ICS) along the anterior axillary line,
usually close to the nipple. With the camera inserted from the 12 mm port,
two 8 mm instrument ports are placed, one in the third ICS and the other in
the seventh ICS, forming a triangular layout. This configuration ensures the
optimal maneuverability of robotic instruments. Special attention must be
taken regarding the port inserted into the third ICS, as it may interact
with the left shoulder and, therefore, can limit its range of movement. For
this case, we also inserted in the fourth ICS a laparoscopic 5 mm port for
vascular clip applier. The Da Vinci XI robotic system (Intuitive Surgical
Inc., California, United States of America) is positioned on the patient's
right side. With a 0-degree or 30-degree angulation, the camera provides
high-definition, magnified views of the operative field. For most portions
of the BIMA harvest, bipolar microtissue forceps are attached to the left
robotic arm and spatula cautery to the right arm.
Right Internal Mammary Artery Harvesting
The RIMA is approached first, as a harvested LIMA would likely be damaged
with the robotic instruments working on the RIMA bed. The left lung is
deflated. Access to the RIMA bed involves creating a substernal plane
extending to the right pleura. The right pleura is kept intact as much as
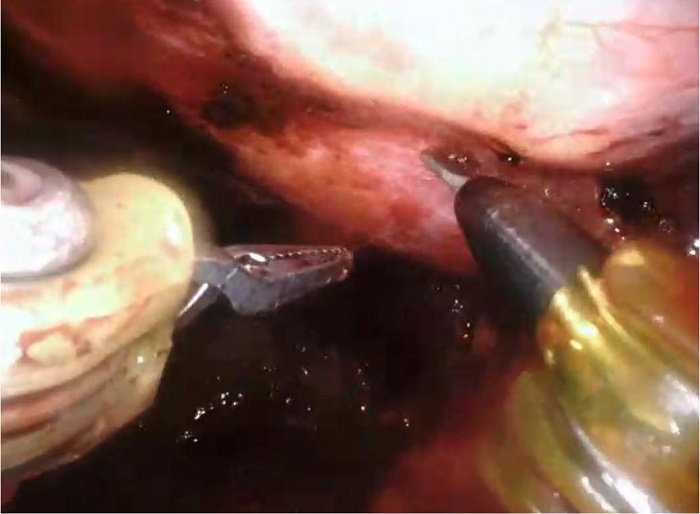
possible to avoid right lung protrusion. Dissection begins by identifying
the pulsating artery beneath the endothoracic fascia. The parietal pleura
and fascia are carefully incised using monopolar cautery, exposing the RIMA
along its length. The artery is skeletonized using sweeping movements of
robotic instruments. The small branches are cauterized using a monopolar
cautery spatula, or for large branches, we use the bipolar cautery micro
forceps. The larger branches can also be clipped and divided with robotic
scissors only with the Da Vinci Si, as the Xi has no clipping instruments.
It is crucial to dissect and transect the proximal mammary vein to allow
very proximal RIMA dissection. This can be performed with the help of a
retractable spatula introduced under the xyphoid to push on the mediastinal
fat close to the innominate vein. Video
1 shows the RIMA harvest.
Left Internal Mammary Artery Harvesting
The LIMA is dissected after the RIMA. The right lung may be fully ventilated,
and the left may be ventilated at low volumes with CO2 inflation at 12 mmHg.
The LIMA dissection mirrors the technique used for RIMA, employing the same
robotic instruments and movements. Adjustments in port angulation or
positioning may be required to optimize access. Heparin is administered once
both mammary arteries are freed, and the distal end of them are clipped and
divided. Once the mammary arteries are cut, they systematically have a
torsion movement leading to a 360° twist. To avoid this, it is paramount to
clip the distal end of the mammary on the mediastinal fat. Video 2 shows the LIMA harvest.
Left Mini Anterolateral Thoracotomy for Coronary Graft
Anastomosis
Once BIMA are harvested, a 4 - 6 cm long anterolateral thoracotomy is made
(Figure 1), which usually englobes
the 12 mm portal insertion incision. Before fully opening the ICS, a small
hole is made in the ICS, and digital palpation is done to feel the apex of
the heart, which indirectly shows us that we are in a good spot regarding
surgical exposure. Usually, the fifth ICS is opened, but if necessary, the
fourth or sixth ICS may be opened to achieve adequate surgical exposure.
After opening the ICS, a mini-thoracotomy retractor is placed. The first
step is the mammary recovery. Each mammary is exposed with two 6-0 Prolene®
sutures. One on each side of the mammary to avoid any twist. The flow in the
mammary is accessed. The pericardium is then opened longitudinally.
 Fig. 1
Postoperative incision and port insertion sites.
Fig. 1
Postoperative incision and port insertion sites.
The next step is the distal anastomoses. Blood pressure should be brought up
to allow manipulation of the heart with hemodynamic stability. We aim for a
systolic blood pressure of 140 - 150 mmHg. The sequence of distal
anastomoses is dictated by the surgeon’s preference and the potential degree
of ischemia in each territory. We routinely start with LAD anastomosis.
The Octopus® NUVO (Medtronic, Minnesota, United States of America) adequately
exposes and stabilizes the coronary target. Complementarily, pericardium
stay sutures may be placed to optimize coronary exposure in special for the
lateral and inferior walls. The Octopus® NUVO is applied using the 6 mm
incision at the sixth/seventh ICS. The stabilizer holder is fixed on the
table arms to obtain maximal stabilization. CPB can be used with femoral
cannulation in cases of inadequate exposure of the target vessels or
hemodynamic instability. If the patient presents hemodynamic stability with
adequate coronary exposure, we proceed to the distal anastomosis off-pump.
For coronary bleeding control, a temporary suture is placed around the
coronary artery to be grafted, proximally to the planned arteriotomy. This
occludes the coronary for a short period and allows better visualization. A
blower is also used to improve the visibility of the coronary. After
arteriotomy, an intracoronary shunt can be placed, and the suture around the
coronary artery may be removed. Then, the distal anastomosis is performed
with a 7-0 or 8-0 Prolene® suture with standard instruments. We check all
bypass grafts with a Doppler flow probe. Protamine is administered after
confirmation of adequate graft flow and hemostasis.
By the end of the procedure, a drain is inserted in the left pleural space
via the incision where the 8 mm portal for the left robotic arm was placed.
The left lung is reinflated, and the proper lie of the grafts and the chest
tube should be checked during lung reexpansion. The ICS is reapproximated,
and the subcutaneous tissue and skin are closed. Intercostal nerve
infiltration with anesthetic drugs is an option to optimize immediate
postoperative pain control.
Procedural Considerations
Carbon dioxide insufflation pressures are maintained between 6 and 12 mmHg
throughout the procedure to enhance visibility. Blood pressure and
saturation are closely monitored to avoid hemodynamic instability,
especially during port placement, RIMA harvest, and pleural insufflation.
Conversion to sternotomy is an option in cases of inadequate visualization,
bleeding, or hemodynamic compromise. The safety and effectiveness of the
procedure must never be jeopardized by the minimally invasive nature of the
robotic approach. Adequate training and experience with robotic systems are
essential for surgeons performing these procedures to minimize risks and
complications.
Postoperative Course
The patient’s recovery was uneventful. He was extubated within six hours
postoperatively. We routinely start aspirin 81 mg within two hours after surgery
and clopidogrel within six hours. On the second postoperative day, the patient
underwent PCI in the PL balloon angioplasty, followed by a successful stent
implantation. The surgical distal anastomosis was checked, and angiography
confirmed widely patent grafts (RIMA to LAD and LIMA to OM1). The patient was
discharged on postoperative day four and remained symptom-free at short-term
follow-up.
 Hugo Monteiro Neder Issa hmonteiro@ottawaheart.ca
Hugo Monteiro Neder Issa hmonteiro@ottawaheart.ca