ABSTRACT:
We present a clinical case of mitral insufficiency in a 59-year-old patient with
dextrocardia and complete transposition of the viscera. The patient underwent
mitral valve posterior leaflet repair and annuloplasty. During the operation, a
“mirror inversion” of the equipment and surgery team position was carried out.
The special feature of the operation was due to the fact that the aorta and
great vessels in the wound were mirror-image. The postoperative period proceeded
without complications. Being aware of the patient’s dextrocardia and hence
organizing the surgical procedure appropriately, we could achieve good results
in radical surgery for valvular heart disease.
Keywords: Dextrocardia, Situs Inversus Totalis, Mitral Valve Posterior Leaflet Chord Rupture, Mitral Insufficiency, Mitral Valve Repair.
Carátula del artículo
Personalized Surgical Tactics for an Adult Patient with Mitral
Insufficiency and Dextrocardia with Situs Inversus Totalis
 Boris N. Kozlov
Boris N. Kozlov
Tomsk National Research Medical
Center, Russian Federation
Konstantin A. Petlin
Tomsk National Research Medical
Center, Russian Federation
Evgeniya V. Lelik
Tomsk National Research Medical
Center, Russian Federation
Natalya L. Afanasieva
Tomsk National Research Medical
Center, Russian Federation
Yulia A. Arsenyeva
Tomsk National Research Medical
Center, Russian Federation
Yulia N. Chernykh
Tomsk National Research Medical
Center, Russian Federation
Elena B. Kim ekim@cardio-tomsk.ru
Tomsk National Research Medical
Center, Russian Federation
Brazilian Journal of Cardiovascular Surgery, vol. 41, no. 3, e20240234, 2026
Sociedade Brasileira de Cirurgia Cardiovascular
Received: 09 July 2024
Revised document received: 03 October October December 2024
Accepted: 23 April 2025
INTRODUCTION
Dextrocardia is a rare condition that occurs in 1/8,000 to 1/25,000 newborns, its
incidence among both sexes is approximately the same. Among all congenital
cardiovascular defects, dextrocardia accounts for no more than 3%[1].
There are scarce data on cardiac surgery for dextrocardia[2-6]. In this
report, we present a rare clinical case of surgical treatment of a patient, who had
a congenital anomaly of dextrocardia and a complete transposition of the viscera,
with mitral insufficiency caused by the ruptured chord of the posterior mitral
leaflet. Such heart anatomy contributes to certain challenges in a traditional
setup, which include performing usual surgical “right-hander’s” procedures with the
left hand, adding complexity for a surgeon to approach the mitral valve. In these
settings, the good exposure of the mitral valve is practically unfeasible.
Therefore, the surgery requires special considerations, such as rearranging the
surgical team and equipment in a "mirror-image" setup, including the
longer cardiopulmonary bypass (CPB) lines, due to the reversed anatomical
orientation. All these listed factors increase the risk of errors associated with
the human factor and related to the activities of the surgeon, the assistant, and
the operating nurse. Therefore, we present our positive experience with operating
room and equipment transformation, which can be reproduced in other clinics.
CASE PRESENTATION
A 59-year-old male patient was electively admitted to the Cardiac Surgery Department
of the Cardiology Research Institute in January 2024, presenting with complaints of
dyspnea during walking.
Complete transposition of the viscera was detected in this patient at the age of 12
during a medical examination at school. He had no complaints at that time, was
actively involved in sports, and did not seek medical assistance. Notably, the
patient was the first-born of twins; however, the second twin died at birth due to
an undetermined cause. Upon analyzing the family history, the patient did not recall
any obvious congenital defects among his immediate relatives. Furthermore, his two
children also do not have any congenital anomalies.
Upon admission to the Cardiac Surgery Department, the physical examination revealed
notable findings: the apical impulse was palpable on the right at the midclavicular
line; the borders of relative cardiac dullness were displaced, with the left border
along the left edge of the sternum, the upper border in the third intercostal space
to the right of the sternum, and the right border along the right midclavicular line
in the fifth intercostal space. Additionally, the liver edge was palpable in the
left hypochondrium.
Taking dextrocardia into account while recording electrocardiogram (ECG), the
principles of electrode placement were deliberately changed, namely: the red
electrode was placed on the left hand, the yellow one on the right hand. The chest
leads were placed sequentially in a mirror-image position on the right side: V3R,
V4R, V5R, V6R, V1, and V2 were swapped. ECG showed sinus rhythm with a heart rate of
90 bpm, normal electrical cardiac axis, and transition zone at V2-V3 (Figure 1).
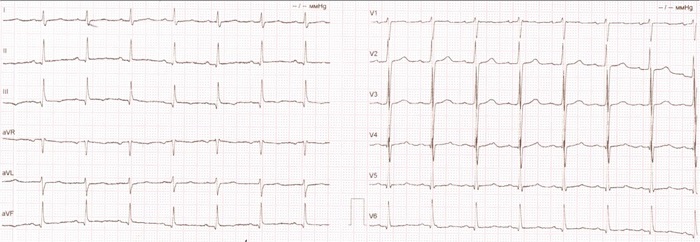 Fig. 1
Electrocardiogram records before surgery.
Fig. 1
Electrocardiogram records before surgery.
The chest x-ray showed a complete transposition of the viscera. The pulmonary pattern
was deformed due to hilar fibrosis without focal infiltrative changes.
Transthoracic echocardiography (Figure 2) showed
the mirror-imaged arrangement of the studied organs in comparison with the typical
ultrasound image, i.e., the left-developed right-sided heart. A
slight left atrial enlargement was detected (52*57 mm in the four-chamber view)
without chamber hypertrophy, with normal left ventricular contractility (left
ventricular ejection fraction in B-mode was 66%). A slightly dilated mitral annulus
(36 mm) was detected; the ruptured chord of the posterior mitral leaflet in P3
segment and grade 2 mitral regurgitation were visualized. The effective regurgitant
orifice was 21 mm. Other valves were functioning normally. The pericardium was not
changed. The performed carotid Doppler sonography showed that the carotid artery
wall was thickened; heterogeneous plaques of up to 10% were detected in carotid
bifurcation, and the internal carotid artery orifices were on both sides.
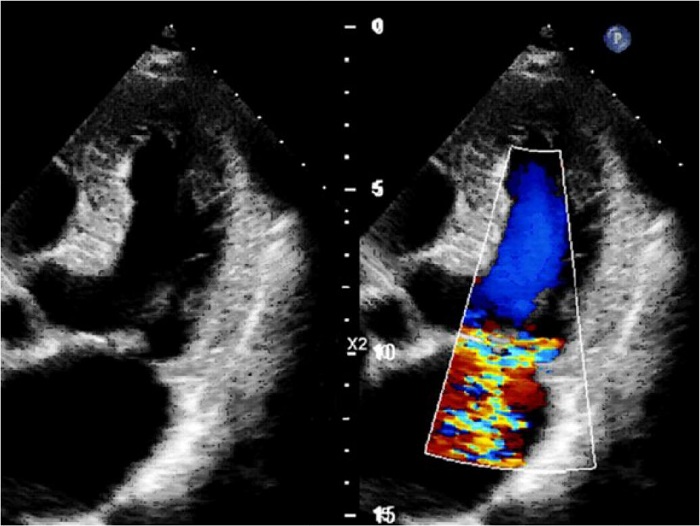 Fig. 2
Transthoracic Doppler echocardiography demonstrating severe mitral
regurgitation.
Fig. 2
Transthoracic Doppler echocardiography demonstrating severe mitral
regurgitation.
Surgical Technique
The patient underwent invasive coronary angiography showing no signs of coronary
atherosclerosis.
Thus, based on the preoperative examination, a myxomatous degeneration of the
mitral valve was diagnosed with the ruptured chord of the posterior mitral
leaflet in P3 segment and severe mitral regurgitation against the background of
complete transposition of the viscera.
When setting out for the upcoming surgery, it was considered reasonable to
perform an additional multislice computed tomography (Figures 3 A, B, C, and D).
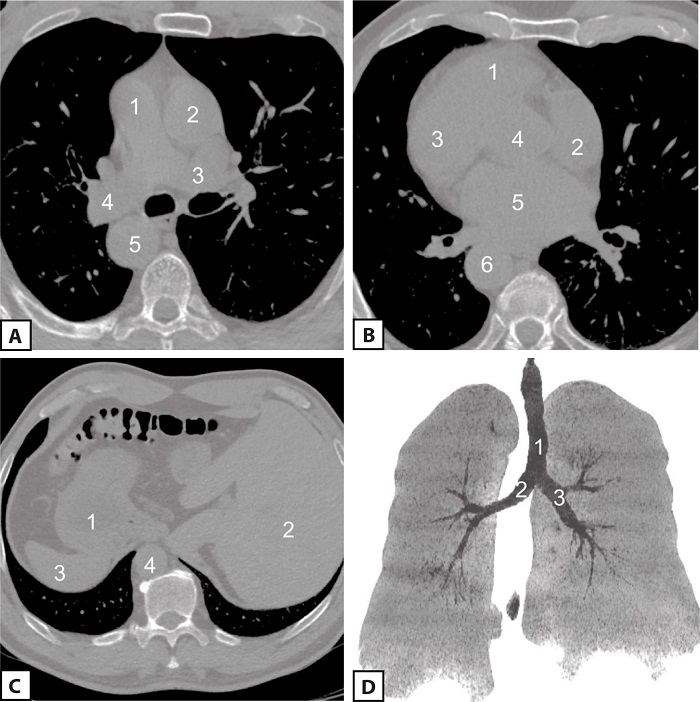 Fig. 3
Preoperative multislice computed tomography (MSCT). A) Chest MSCT
scan at the level of great vessels (1, pulmonary artery trunk; 2,
ascending aorta; 3, left pulmonary artery; 4, right pulmonary
artery; 5, descending thoracic aorta); B) chest MSCT scan at the
level of heart chambers (1, right ventricle; 2, right atrium; 3,
left ventricle; 4, an outlet of the left ventricle; 5, left atrium;
6, descending thoracic aorta); C) upper-abdominal MSCT scan (1,
stomach; 2, liver; 3, spleen; 4, descending thoracic aorta); D) lung
MSCT scan (1, trachea; 2, left lung developed on the right side; 3,
right lung developed on the left side).
Fig. 3
Preoperative multislice computed tomography (MSCT). A) Chest MSCT
scan at the level of great vessels (1, pulmonary artery trunk; 2,
ascending aorta; 3, left pulmonary artery; 4, right pulmonary
artery; 5, descending thoracic aorta); B) chest MSCT scan at the
level of heart chambers (1, right ventricle; 2, right atrium; 3,
left ventricle; 4, an outlet of the left ventricle; 5, left atrium;
6, descending thoracic aorta); C) upper-abdominal MSCT scan (1,
stomach; 2, liver; 3, spleen; 4, descending thoracic aorta); D) lung
MSCT scan (1, trachea; 2, left lung developed on the right side; 3,
right lung developed on the left side).
Due to dextrocardia and complete transposition of the viscera in the patient,
certain organizational measures were to be taken. During the operation, a
“mirror inversion” of the equipment (CPB machine, operating table, screens) and
the position of the surgical team (operating surgeon, assistants, perioperative
nurse) was carried out in the operating room (Figures 4 A, B, and C).
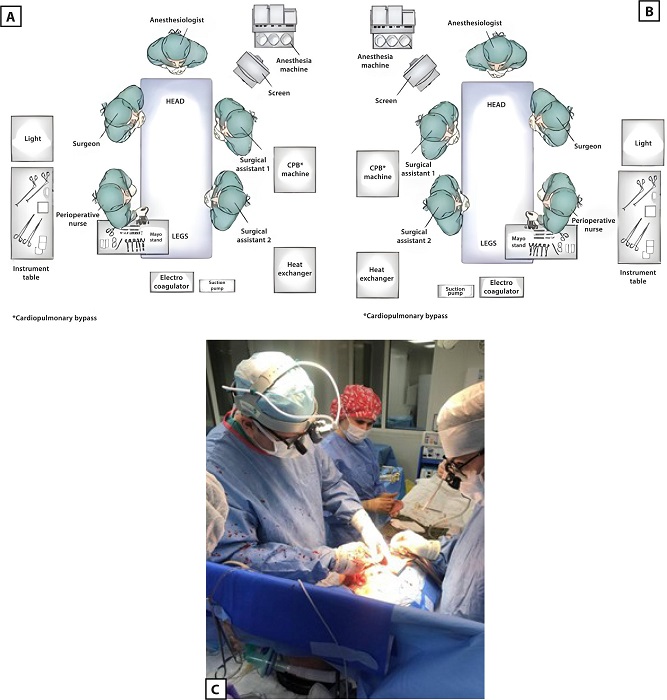 Fig. 4
The surgical team and equipment arrangement in the operating
room. A) A pictorial diagram of the surgical team and equipment
position for the patient with a normal heart location; B) a
pictorial diagram of the surgical team and equipment position for
the patient with dextrocardia; C) photograph taken during the
surgical procedure. CPB=cardiopulmonary bypass.
Fig. 4
The surgical team and equipment arrangement in the operating
room. A) A pictorial diagram of the surgical team and equipment
position for the patient with a normal heart location; B) a
pictorial diagram of the surgical team and equipment position for
the patient with dextrocardia; C) photograph taken during the
surgical procedure. CPB=cardiopulmonary bypass.
The patient underwent posterior mitral valve leaflet repair and mitral valve
annuloplasty under CPB and antegrade cold cardioplegia. The surgical access was
gained typically via median sternotomy. The special technical feature was that
the aorta and great vessels in the wound were mirrored from the normal position.
Purse string sutures for cannulation of the aorta and vena cava were technically
placed in a standard manner, but the placement itself was in the left parts of
the surgical wound, i.e., “non-standard” (Figure 5).
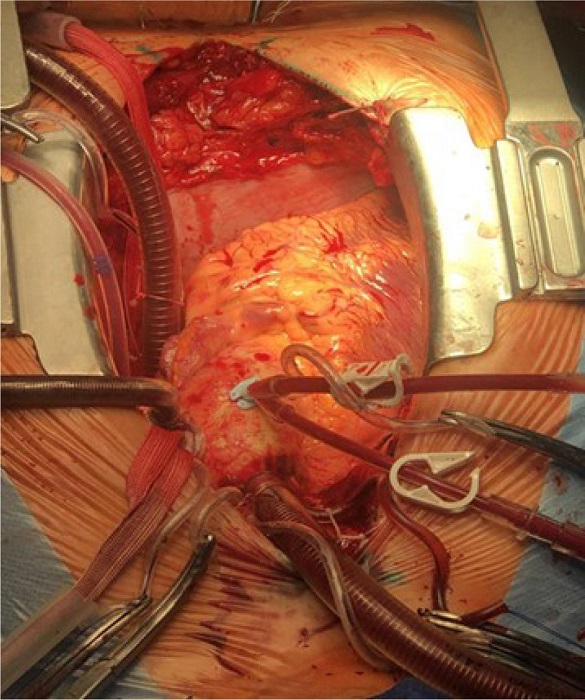 Fig. 5
An intraoperative photograph shows a still frame of dextrocardia
with visible right atrial venous cannulation on the left side of
torso and adjacent distal ascending aortic cannulation.
Fig. 5
An intraoperative photograph shows a still frame of dextrocardia
with visible right atrial venous cannulation on the left side of
torso and adjacent distal ascending aortic cannulation.
Access to the mitral valve was obtained through atriotomy performed on the left
flank of the surgical wound. After the mitral valve revision and identification
of changes (the fibrous ring was not dilated, the posterior leaflet of the
mitral valve was thickened, the ruptured chord was at P3 segment), posterior
mitral valve leaflet repair was performed. A support C-Ring was inserted in
mitral position. An intraoperative transesophageal echocardiography confirmed
that mitral regurgitation was not observed.
The postoperative period was uneventful. On day 10 after surgery, the patient was
discharged from the hospital in a satisfactory condition.
DISCUSSION
The abnormal right-sided location of the heart in the chest was first described by
the Italian anatomist and surgeon Hieronymus Fabricius, in 1606. There are
dextrocardia with situs viscerum inversus totalis - the complete reversal of
internal organs (observed in our patient) - and isolated dextrocardia characterized
by a right thoracic heart with normal locations of the stomach, liver, and
spleen[2-4]. If the normal blood flow in the vessels and
chambers of the heart is maintained, then this cardiac anomaly does not require any
treatment. This is confirmed by the case we describe. The patient, up to 57 years of
age, led an active sports lifestyle. However, the very fact of identifying
dextrocardia in a patient should be an alert for cardiologists in terms of possible
concomitant defects in the development of the heart, systemic dysplasias, which
require dynamic monitoring and regular assessment of intracardiac structures and
possible cardiac complications. For example, myxomatous degeneration of the mitral
valve leaflets, which is described herein, was caused by a congenital defect of
connective tissue[5]. The surgical
technique for a patient with dextrocardia is not distinctive, but cardiac surgeons
may encounter technical issues due to the mirror-image transposition of the internal
organs and intracardiac structures. According to Rammos K et al.[7], complications can arise with CPB
connecting because the vena cava and right atrium are located more posteriorly than
normal, and surgeons may be confused by mirror-image findings. Some authors
describing cardiac surgery in dextrocardia and transposition of the internal organs
note the particular nature of surgical interventions in such patients, especially in
such emergency cases as acute aortic dissection[6-9,10]. Additionally, there may be a problem when
performing usual surgical “right-hander’s” procedures with the left hand. Some
authors recommend that the surgeon stand to the left of the patient, which provides
excellent exposure because the patient’s anatomy is mirror transformed[11,12].
Dealing with this rare condition, it is very important for the surgeon to have
spatial abilities in order to better plan the course of the upcoming operation, to
imagine three-dimensional models of the heart, internal organs, and their topography
relative to each other[6,7], as well as predict possible
risks.
CONCLUSION
The combination of degenerative mitral valve disease with mitral insufficiency and
situs inversus in an adult patient is a rare clinical case. Full awareness of the
cardiac surgery team of dextrocardia in the patient as well as the appropriate
organization of the surgical procedure allowed us to achieve desired immediate
results in radical surgery for valvular heart disease, which ensures clinical
stability in the patient not only at the hospital stage but also in the long-term
postoperative period.
Our positive experience will be useful for other clinics to apply our scheme
regarding the surgical team’s new configuration in practice.
REFERENCES
Gutgesell HP. Cardiac malposition and heterotaxy. In: Garson A,
Timothy JJ, Fisher DJ, Nesh SR, eds. The science and practice of pediatric
cardiology. 2nd ed. Baltimore: Williams & Wilkins. 1998; p.
1539-61.
Maldjian PD, Saric M. Approach to dextrocardia in adults: review.
AJR Am J Roentgenol. 2007;188(6 Suppl):S39-49; quiz S35-8.
doi:10.2214/AJR.06.1179.
Offen S, Jackson D, Canniffe C, Choudhary P, Celermajer DS.
Dextrocardia in adults with congenital heart disease. Heart Lung Circ.
2016;25(4):352-7. doi:10.1016/j.hlc.2015.09.003.
Kennedy MP, Omran H, Leigh MW, Dell S, Morgan L, Molina PL, et al.
Congenital heart disease and other heterotaxic defects in a large cohort of
patients with primary ciliary dyskinesia. Circulation. 2007;115(22):2814-21.
doi:10.1161/CIRCULATIONAHA.106.649038.
Shumakov DV, Tarayan MV, Dontsov VV, Zybin D. Surgical repair of
intermediate atrioventricular septal defect, double orifice of left
atrioventricular valve in adult patient with dextrocardia: a case report C Exp
Surg Petrovsky J. 2021;9(3s):115-20.
doi:10.33029/2308-1198-2021-9-3suppl-115-120.
Niino T, Shiono M, Inoue T, Hata M, Sezai A, Negishi N. A case of
acute aortic dissection type A in a patient with situs inversus. Ann Thorac
Surg. 2003;75(6):1963-5. doi:10.1016/s0003-4975(02)05007-5.
St Rammos K, Bakas AJ, Panagopoulos FG. Mitral valve replacement in
a Jehovah's witness with dextrocardia and situs solitus. J Heart Valve Dis.
1996;5(6):673-4.
Kim DK, Lee JM, Heo SY, Jung JP, Park CR, Lee YJ, et al. Acute type
A aortic dissection in a patient with situs inversus totalis. Korean J Thorac
Cardiovasc Surg. 2020;53(5):321-3. doi:10.5090/kjtcs.20.006.
Shahani R, Ahmed A, Rosell FM, Iribarne A. Coronary artery bypass
grafting in a patient with multivessel disease and dextrocardia with situs
inversus totalis. Tex Heart Inst J. 2024;51(1):e238382.
doi:10.14503/THIJ-23-8382.
Chernov II, Magomedov GM, Kozmin DY, Enginoev ST. Replacement of the
aortic valve, ascending aorta and arch in a patient with dextrocardia and
transposition of internal organs: a clinical case. Russ J Cardiol.
2022;27(2S):4969. doi:10.15829/1560-4071-2022-4969.
Chakravarthy M, Jawali V, Nijagal D. Off-pump coronary artery bypass
surgery in dextrocardia: a report of two cases. Ann Thorac Cardiovasc Surg.
2008;14(3):187-91.
Saad RA, Badr A, Goodwin AT, Dunning J. Should you stand on the left
or the right of a patient with dextrocardia who needs coronary surgery? Interact
Cardiovasc Thorac Surg. 2009;9(4):698-702.
doi:10.1510/icvts.2009.216317.
Notes
Notes
Sources of Funding The authors declare no external funding to this study.
This study was carried out at the Cardiovascular Surgery Department, Cardiology
Research Institute, Tomsk National Research Medical Center, Russian Academy of
Sciences, Russian Federation.
Author notes
Potential Conflict of Interest The authors declare that there is no conflict of interest in this study.
Correspondence Address: Elena B. Kim, Cardiovascular Surgery
Department, Cardiology Research Institute, Tomsk National Research Medical
Center, Russian Academy of Sciences, 111a Kievskaya St., Tomsk, Russian
Federation, Zip Code: 634012, E-mail: ekim@cardio-tomsk.ru