DISRUPTIVE INNOVATION: LOW-COST CLINICS IN NORTHEAST BRAZIL
 Ezequiel Alves Lobo ezequiellobo2013@gmail.com
José Iran Batista de Melo Filho irandemelo.idm@gmail.com
Jessie Coutinho de Souza Tavares jessie.tavares@aluno.uece.br
Elda Fontenele Tahim fontineletahim@gmail.com
Ezequiel Alves Lobo ezequiellobo2013@gmail.com
José Iran Batista de Melo Filho irandemelo.idm@gmail.com
Jessie Coutinho de Souza Tavares jessie.tavares@aluno.uece.br
Elda Fontenele Tahim fontineletahim@gmail.com
DISRUPTIVE INNOVATION: LOW-COST CLINICS IN NORTHEAST BRAZIL
Revista Pensamento Contemporâneo em Administração, vol. 15, núm. 3, pp. 1-14, 2021
Universidade Federal Fluminense
Recepción: 22 Junio 2021
Aprobación: 03 Noviembre 2021
Resumen: A characterization of innovation for companies that are already entering or entering the market shows a dynamic movement in a circular movement that, both can generate new organizations and create a new market for existing organizations, or eliminate them, concretizing or process of creative destruction. The paper approach was directed to the concept of disruptive innovation and its characterization in popular health clinics. A research, multi-method, exploratory and descriptive was carried out through structured interviews, using as a method to analyze lexicometry and its modalities. From data analysis, it was identified that popular clinics have disruptive potential.
Resumo: A caracterização da inovação nas empresas que já estão ou que ingressam no mercado demonstra um movimento dinâmico e não circular, que tanto pode gerar novas organizações como trazer um novo mercado para organizações já existentes ou até mesmo eliminá-las, concretizando o processo da destruição criativa. O enfoque deste artigo, é direcionado para o conceito da inovação disruptiva e sua caracterização nas clínicas populares de saúde. A pesquisa é multimétodos, exploratória e descritiva. Foi realizada mediante entrevistas estruturadas, utilizando-se como método a análise de lexiometria e suas modalidades. A partir da análise dos dados, foi identificado que as clínicas populares possuem potencial disruptivo.
Palavras-chave: Inovação Disruptiva, Setor de saúde, Clínicas Populares.
Keywords: Disruptive Innovation, Health sector, Popular Clinics
Introduction
The aggressively competitive and volatile nature of the current business environment requires organizations to make frequent adjustments to their corporate strategies: not even the best strategy will guarantee success in the long run or create perennial stability. In other words, both small and large firms may need to reinvent themselves at regular intervals to secure market leadership and survive. Innovation is one way of increasing the organization’s market share and penetrating new segments, enabling it to satisfy a wider range of consumer demands (Vieira, 2010; Hamel, 2000).
Some innovations are considered ‘disruptive’, an expression coined by Clayton Christensen in a study from the mid-1990s on the hard disk drive industry, which allowed him to define the main components of the construct. According to the author, disruption refers to a sudden and substantial change in established procedures, products or business networks, usually by way of a new technology or startup intended to boost a sector and change its competitive patterns (Christensen et al., 2018)
To Christensen et al. (2007), disruptive innovation comprises ‘sustaining disruption’ (improvements to already established products or services), ‘low-end disruption’ (reordering of existing markets) and ‘new-market disruption’ (creation of new markets).
Within the health sector, disruptive innovation tends to be of the low-end type. Put another way, it enables the migration of the health care model from the provision of cutting-edge services for select consumers, maintained by constant investments, to the provision of accessible and affordable services to broader audiences (Christensen et al., 2009).
The innovative model was initially implemented in the US health sector, with the primary objective of shifting a pernicious economic trend. As shown by analyses of the country’s GDP, health-related investments represent a very significant part of the US economy. While this may at first sound reassuring, the size of these investments is not reflected in the accessibility of health care services to the general public (Christensen et al., 2007).
This spurred the interest of private firms in the US in making a wide range of services (some of which in the health care sector) more accessible and affordable. Repercussions of this development may also be seen in Brazil. According to Costa (2016), the Brazilian health sector had long felt the need for an egalitarian and sustainable alternative to bridge the gap between expensive private health insurance and the universal free-of-charge but inefficient public health care system (SUS), while incorporating the benefits of new technology.
As a result, low-cost private clinics have mushroomed in the country, especially in the Northeast, targeting low-income users without private health insurance (approximately 150 million individuals). The purpose of this study was to analyze the emergence on the Brazilian market of the model of low-cost clinics as an expression of disruptive innovation.
Theoretical framework
Before looking into the actual phenomenon analyzed in this study, we will summarize the main elements of our theoretical framework. Among other things, we will review the definition of innovation in light of neo-Schumpeterian economics and provide a short description of the concept of disruptive innovation and related constructs.
Innovation
As explained by Schumpeter (1984), the capitalist system generates economic development mainly by encouraging competitiveness. Innovation, as defined by this author, fertilizes the economic system through a perpetual flow of new combinations of goods, services, products, processes and organizational forms. As such, innovation is the main factor responsible for the remarkable diversity of products on the market and for their ongoing improvement.
In short, the academic literature defines innovation as the creation of new commodities, products or services or as a cardinal change in an existing product or service. The definition is compatible with the original notion of innovation as the ability of an organization to exercise leadership or monopoly in a given segment by way of the introduction of novel products (Schumpeter, 1984; Knight, 1967).
Drucker (1986) endorsed this interpretation, but favored an approach focused on the satisfaction of consumer needs. Abernathy and Clark (1985) contextualized innovation within the market perspective, defining it as the introduction of a product or process radically different from previous practices.
Other authors have revised or updated the concept of innovation by linking it more specifically to technology (Krugman, 1979; Dubickis & Gaile-Sarkane, 2015; Huang et al., 2016; Chaym et al., 2018), that is, to the adoption of novel technologies intended to boost competitiveness and expand markets (Chaym et al. 2018; Hamel & Prahalad, 1994). In this paper, we will look at innovation as a disruptive phenomenon and show how it applies to the model of low-cost clinics implemented in Fortaleza, a state capital in Northeastern Brazil.
Disruptive innovation
The expression ‘disruptive innovation’ was first used by Christensen (1997) in a study on the hard disk drive industry showing that leading firms were unable to remain prevalent for long in their respective markets. The study brought to the fore three core principles of disruptive innovation: i) in several sectors, the pace of technological development exceeds the demand for high-performance technologies; ii) firms should make a crucial strategic distinction between types of innovation in technologies and business models; and iii) established business models discourage investments in innovative firms (Christensen et al., 2018).
The effect of disruptive innovation on the health sector has also been investigated. According to Christensen et al. (2007), the sector accounts for one out of every seven dollars spent by US citizens. For example, innovations in glucose and pregnancy testing and angioplasty procedures not only generated a significant market opportunity but also brought consumers/patients closer to non-specialized health care workers who had previously been unable to provide services at this level of sophistication.
The above authors believe innovation in health care is triggered by the question of accessibility. Improvements in access over the last decade have not only encouraged interaction between patients and non-specialized health care workers but, as the latter become proficient in procedures which in the past required more extensive training, specialists are relieved from routine work to focus their attention on more challenging tasks (Christensen et al., 2007).
In Brazil, the debate on disruptive innovation in health care has raised important issues like digital disease detection and databases for medical record management. In a recent study, Duarte, Pedroso, Bellido, Moreira and Viacava (2015) evaluated the health information system of the SUS in light of Diamandis’s 6 Ds of exponentials (digitization, deception, disruption, demonetization, dematerialization and democratization).
The concept of disruptive innovation was further popularized with the publication in 1997 of a book by Christensen titled ‘The Innovator’s Dilemma’. Since then, the expression has become a household name in the daily life of organizations and academia when referring to products and services creating entirely new markets or breaking established business practices (Vieira, 2010).
As pointed out by Corsi and Di Minin (2014), disruptive innovation is born out of the demand for products or services which at the time are unaffordable to most consumers. The disruption occurs not when the new technology is introduced but when it is made available at a low price. Once a product or service has been marketed, it may become the object of disruptive innovation by incorporating features like low cost, simplicity and accessibility at lower levels of the consumer pyramid (Dan & Chieh, 2010).
With regard to market practices, Teece (2010) believes firms should make efforts to keep step with the constant flow of changes in the technological landscape, not only through the development of new products and services, but also through value creation.
To be successful in this process of readjustment, firms should adopt innovation-friendly business models (Gassmann et al., 2013). In addition, Schiavi and Behr (2018) suggest that disruptive innovation models emerge when, to remain competitive, firms are forced to restructure organizationally and rethink their products and services.
Research on disruptive innovation is still far from exhaustive (Foss & Saebi, 2017). As a contribution to current knowledge in this field, the present study was designed based on the disruptive innovation framework of Christensen et al. (2018), illustrated below:
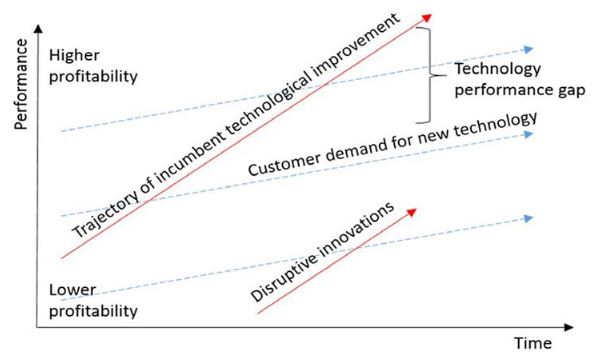
Figure 1:
Disruptive innovation model
Source: Christensen et al. 2018.
As shown in Figure 1, in the lower market strata consumers with small purchasing power display a growing demand for new technology. This happens because most firms focus on high-tech products for a select upscale market. Disruptive innovations emerge in the context of restrictions and advance over time, following a trajectory of technological improvement demanded by more exacting consumers, thereby filling the technology performance gap (Christensen et al., 2018).
According to Christensen and Raynor (2013), disruptive innovations may be classified as ‘new-market’ or ‘low-end’. The latter occur when a large group of consumers are unable to purchase expensive high-tech products developed by market leaders. In response, entrants on the market develop similar products or services with much less costly features, greater convenience and ease of use, meeting the same consumer needs.
New-market innovations provide a combination of features which attract marginalized consumers. They may be more accessible or smaller, or may satisfy the demands of consumers who would usually be found at the bottom of the consumer pyramid where access to certain products and services is precluded. This type of consumption is more centralized and may be slow in the early stages.
Such neglected markets are more abundant in developing countries, which are therefore the primary target of disruptive innovations (Hart & Christensen, 2002; Bencke et al., 2017). The business models adopted in low-income markets favor the emergence of low-cost innovations targeting the lower tiers of the consumer pyramid, an example of which may be low-cost private clinics. This is not to say that disruptive innovations cannot migrate to high-income markets (Bencke et al., 2017).
Regardless of the scenario, both new-market and low-end innovations involve the targeting of specific consumer groups by entrants marketing disruptive technologies (Vieira, 2010). As the disruptive innovations capture more investments, incremental innovations appear which improve products and services toward greater quality and maturity. Eventually, a shift occurs in market leadership.
Unlike other forms of innovation, disruptive innovations not only require technological standards which are often unavailable in developing countries, but also target heterogeneous low-income consumer groups which vary greatly from one region to another (Nogami & Veloso, 2017).
Low-cost clinics as a socioeconomic phenomenon
Duarte et al. (2015) identified two phenomena which have impacted and reshaped the Brazilian health care system and health care policies in general: the decentralization of regulatory and decision-making powers to the state and municipal level and the proliferation of non-public health care services.
Factors like the inefficiency of the established bureaucratic model, developments in the economic sector, expansion of services, internationalization of the Brazilian health care sector and changes in the labor market (to some extent responsible for system shortcomings) all contributed to lay the groundwork for a new network of negotiation, contracts, market consortia and, consequently, new business opportunities (Duarte et al., 2015).
From an integrated perspective, Jurca (2018) attributes the economic inclusion of low-income consumers in the private health care sector to the lack of homogeneity in public health care services, favoring the emergence of private alternatives, such as low-cost clinics.
The first low-cost clinics in Ceará appeared in the 1990s. They sprung up in the wake of changes in access to consultations at Santa Casa, a semi-public philanthropic hospital in downtown Fortaleza (the state capital). Physicians from this hospital saw the opportunity to open low-cost clinics in the vicinity primarily for workers without private health coverage who were unwilling to wait for months to secure treatment through the public health care system (Godoy & Silva, 2018).
Godoy and Silva (2018) consider as one of the main advantages of low-cost clinics the availability of a wide array of specialists (on the average, some 35 medical and non-medical specialties), if compared to the SUS. Low-cost clinics constitute a ‘third option’, breaking the long-standing dichotomy between expensive private health insurance and free-of-charge but ineffective public health care.
Methods
This is a descriptive and exploratory study with a combined qualitative and quantitative approach. According to Gerring (2017), the combination of qualitative and quantitative aspects empowers the study and allows for a greater diversity of methods. The conjugation of different categories of data in the same analysis is a trend in field studies, showing that the multimethod approach is a possible solution to methodological dilemmas.
Information on selected qualitative variables was collected through semi-structured interviews. Qualitative interviews are a common method in field studies of applied social sciences (Bauer & Gaskell, 2002). Once thoroughly analyzed, the contents of the interviews make it possible to understand the interaction between the agents and the problematic.
The study population consisted of users of low-cost clinics in Fortaleza. Prior to inclusion in the study, the subjects were informed of the purpose of the investigation and reassured of the confidentiality of all personal information. Sampling was done by convenience, i.e., we used a non-probability sample determined by ease of access. The clinics were selected by the interviewer (Stake, 2011).
The collected information was submitted to lexicometry analysis. As explained by Damasceno (2008), lexicometry is an objective, descriptive, inductive and scientific method which allows to treat qualitative data statistically. The method involves evaluating a limited textual corpus for topology and word combinations in order to establish the trajectory of the discourse and describe each lexical element.
The lexicometry modalities employed included descending hierarchical classification in which text segments and words are correlated to create a hierarchy of word classes which in turn allows to make inferences regarding content in the textual corpus, name classes, understand groups of discourse and ideas, and detect similarities. Thus, correlations between structures and objects with common traits may be identified and used to build models descriptive of the concepts involved (Damasceno, 2008). The lexicometry analysis was performed with the open software Iramuteq (v. 0.7 alpha 0.2) which is designed to run quantitative tests on qualitative data.
To produce meaningful, reliable and tangible results, the study was based on well-defined constructs and variables, categorized and employed with the study objectives in mind. To do so, we adopted the constructs of Christensen et al. (2018) for the relationship between consumers and disruptive innovation, choosing specific variables as point of departure, as expounded in the section on theoretical framework and illustrated in Figure 2.
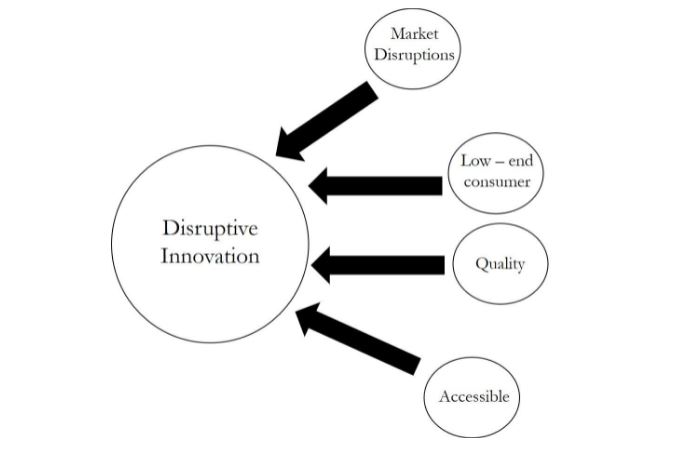
Figure 2:
Construct of disruptive innovation in relation to consumers
Source: Based on Christensen et al. (2018).
In our results, we attempted to identify the following categories:
| Categories Identified |
| Market Disruptions |
| Low-end consumer |
| Quality |
| Accessible |
Analysis of results
Description of the Brazilian health sector
The Brazilian private health care sector covers health insurance, hospital services, outpatient services and diagnostic facilities. Hospital services include inpatient curative procedures, mental health care and preventive medicine provided by general or referral facilities like clinics specialized in orthopedics, otorhinolaryngology, pediatrics and so forth (IBGE, 2017).
Private diagnostic and outpatient services serve as support for medical and dental evaluations and treatments administered at clinics, primary care facilities, polyclinics, geriatric centers and even in the home. Among other things, diagnostic services cover lab testing, pathology, dialysis, hemotherapy, radiology, radiodiagnosis, radiotherapy, chemotherapy, endoscopy, electroencephalography and echocardiography.
Some private health care services are rendered by autonomous professionals, including nurses, nutritionists, psychologists, physiotherapists, optometrists and dentists. Patients can also get treatment at centers of rehabilitation, psychology and nutrition, in addition to strictly alternative modalities such as acupuncture, chromotherapy and shiatsu.
According to the IBGE (2017), worldwide health care spending is growing faster than inflation. In Brazil, spending in 2012 increased 6.6% above the level of inflation, corresponding to ~8% of the GDP and an international per capita purchasing power parity of USD 1,318.
In 2015, the total consumption of products and services on the Brazilian private health care market was BRL 546 billion. This may be segregated into government spending (BRL 231 billion) and spending by families and non-profit institutions (BRL 315 billion). Most of this amount was spent on health care services (79.2%), followed by medication (19.0%) and other medical, optical and dental supplies. Table 2 shows the rapid increase in health care spending from 2010 to 2015, according to institutional sector.
| Products | Final Consumption per institutional sector (expressed in million BRL) | |||||
| 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | |
| Families | ||||||
| Total | 165 432 | 184 577 | 211 282 | 239 986 | 278 874 | 307 054 |
| Medications for human consumption | 62 071 | 66 064 | 72 718 | 79 022 | 88 509 | 92 517 |
| Pharmaceutical products | 119 | 130 | 144 | 160 | 172 | 174 |
| Medical and dental devices and instruments | 316 | 370 | 438 | 491 | 570 | 656 |
| Other medical, dental and optical supplies including prostheses | 5 105 | 5 505 | 6 000 | 7 088 | 8 271 | 9 271 |
| Private Hearth Care | 92 821 | 112 508 | 131 982 | 153 225 | 181 352 | 204 436 |
| Government | ||||||
| Total | 139 710 | 152 563 | 164 889 | 189 198 | 215 299 | 231 448 |
| Medications for human consumption | 7 042 | 7 297 | 7 325 | 8 469 | 9 422 | 10 884 |
| Public health care | 105 612 | 117 275 | 126 536 | 148 871 | 170 348 | 184 284 |
| Private health care | 27 056 | 27 991 | 31 028 | 31 858 | 35 529 | 36 280 |
| Nonprofit institutions providing care for families | ||||||
| Total | 4 301 | 4 552 | 4 615 | 5 998 | 7 175 | 7 583 |
| Private health care | 4 301 | 4 552 | 4 615 | 5 998 | 7 175 | 7 583 |
As the consumption of health care products and services increase, so does the availability of jobs. Thus, health care-related jobs grew 3.5% in the period, while jobs in other sectors decreased by 3.8%. Among all sectors, the greatest number of jobs are found in public and private health care. The percentage representation of the sector on the job market rose from 5.3% in 2010 to 6.4% in 2015.
Table 3 shows the evolution in job availability in the health care sector compared to all other sectors. Despite the economic downturn in many segments, the health care sector has continued expanding.
| Sector/activity | Jobs | |||||
| 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | |
| Health – related activities | 5 228 775 | 5 455 108 | 5 733 939 | 6 049 668 | 6 337 473 | 6 559 191 |
| Manufacture of pharmaceutical products | 90 675 | 93 221 | 92 060 | 95 120 | 100 062 | 91 798 |
| Manufacture of medical, dental and optical instruments and supplies | 59 979 | 62 514 | 70 011 | 66 993 | 66 700 | 68 458 |
| Sales of pharmaceutical hygiene, medical and dental products | 1 027 451 | 1 060 688 | 1 112 543 | 1 169 287 | 1 222 467 | 1 204 022 |
| Private health care | 2 294 668 | 2 451 934 | 2 617 872 | 2 688 997 | 2 969 721 | 3 082 956 |
| Public health care | 1 562 737 | 1 585 717 | 1 645 234 | 1 839 563 | 1 780 378 | 1 903 462 |
| Public health care – education and preventions | 193 265 | 201 034 | 196 219 | 189 708 | 199 145 | 208 495 |
| Nom-heath-related activities | 92 887 443 | 94 105 049 | 95 226 329 | 96 487 730 | 99 135 205 | 95 385 885 |
Data from the National Agency of Supplementary Health (ANS, 2018) confirm the growth trend in the health care sector, especially private health care, with 47.3 million Brazilians insured as of December 2017. In the preceding month alone, 108.551 new users acquired private health insurance.
However, for a broad segment of Brazilian consumers, private health insurance (or conventional walk-in appointments without insurance) is unaffordable while, on the other hand, the long waiting time in public health care (SUS) is impracticable. This wide gap on the supply side marginalized millions of potential users until the appearance of feasible alternatives.
Enter low-cost clinics to meet the needs of this large and neglected segment of consumers. The new concept offered an alternative to private health insurance, public health care (SUS), and coverage by non-profit organizations.
Analysis of texts
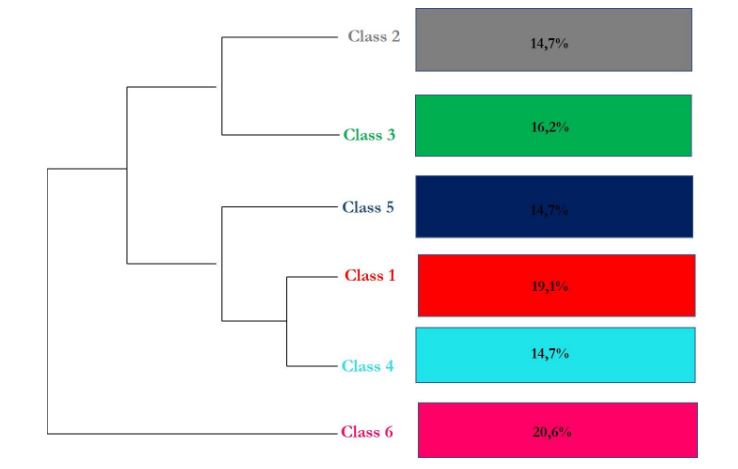
Figure 3:
Descending hierarchical classification expressed in percentage.
Source: The authors (2019).
Two main branches were considered: Sub corpus A (“Quality of low-cost clinics”) was represented by Class 6 (“Quality”) and focused on statements regarding quality, especially service quality at the clinics, price levels in relation to users’ purchasing power, the availability of medical specialties, and the care received. This perspective considers the capture of previously neglected consumers with no history of private health insurance (Godoy & Silva, 2018; Jurca, 2018; Christensen et al., 2018).
Sub corpus B (“Disruption by low-cost clinics”) consisted of statements regarding low-cost clinics (Class 1), SUS (Class 2), SUS compared to low-cost clinics (Class 3), price accessibility (Class 4), and low-cost clinics as an option for low-end consumers (Class 5). The five classes view low-cost clinics as an option for users who refrain from using the ineffective public health care system but have never owned private health insurance (though some may have received insurance as a benefit associated with formal employment in the past). The identification of low-cost clinics as a new-market disruptive innovation allowed us to evaluate the relationship between Sub corpus B and the variable ‘market disruption’ in the construct of Figure 2 (Vieira, 2010; Bencke et al., 2017; Christensen et al., 2018, Christensen et al., 2009).
Figure 4 helps visualize the 6 classes. The words in the respective lists were identified with a chi-squared test. The ideas elicited by the words highlight the differences between the classes.
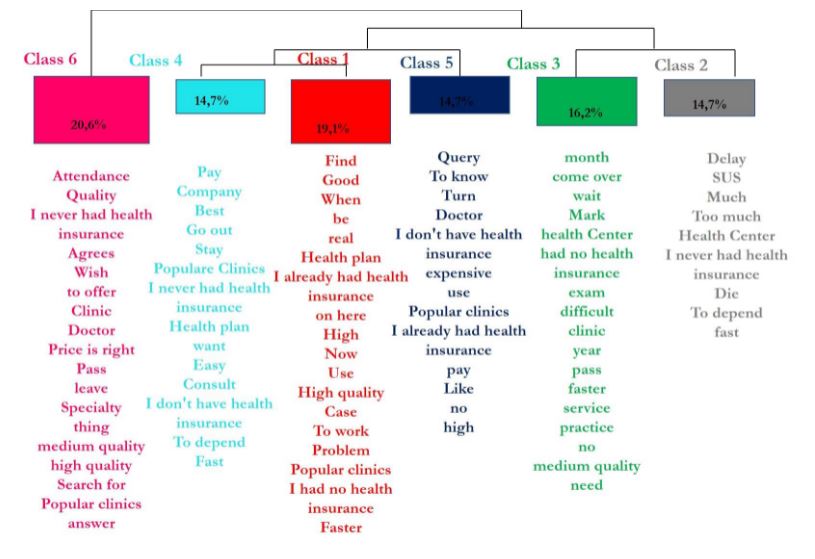
Figure 4:
Descending hierarchical classification with lists of words identified with the chi-squared test
Source: The authors (2019).
Using factorial correspondence analysis, the words were associated with the text. Based on the incidence of words and classes, the elements were disposed in a cartesian diagram (Figure 5). Note that the words of each class appear in a centralized segment which expands towards the periphery, showing the extent of the differences between the classes.
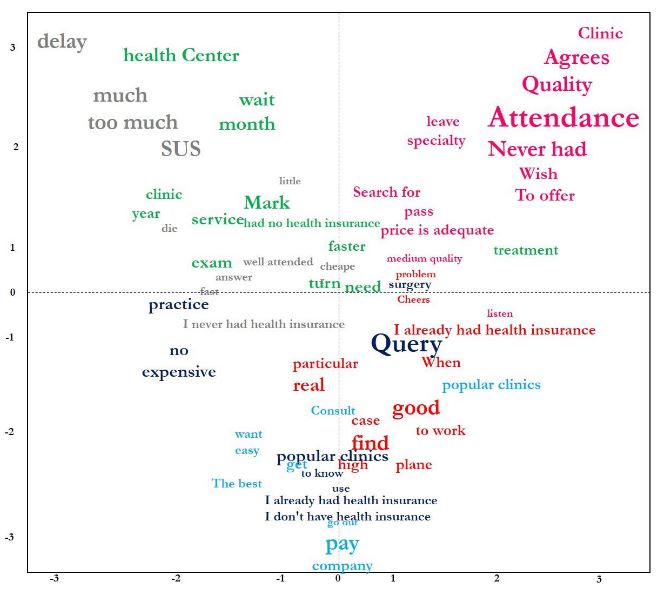
Figure 5:
Factorial correspondence analysis
Source: The authors (2019).
The words and phrases in Classes 1, 4 and 5 (e.g., “I have no insurance”, “low-cost clinics” and “appointment”) are more closely related, making it possible to associate these classes with the variable ‘low-end consumer’ in the construct in Figure 2, and confirming that low-cost clinics are seen as an alternative for consumers without health insurance. This supports the characterization of the business model as a new-market disruptive innovation and supports the association with the variable ‘accessible’ in the construct in Figure 2 (Christensen et al., 2018).
Classes 2 and 3 projects into the upper left quadrant. The words and phrases in these classes include “SUS”, “I have no insurance”, “delay”, “wait”, “die”, “cheaper” and “faster”. This allows to infer that low-cost clinics are viewed as an affordable third option for low-end consumers who were previously marginalized by the private health care system and unable to wait for SUS appointments, once again warranting the association with the variable ‘accessible’ in the construct in Figure 2 (Christensen et al., 2018; Jurca, 2018).
Class 6 is clearly separated from the other classes, with almost all words and phrases (e.g., “quality”, “fitting price”, “wish”) in the upper right quadrant, allowing to associate it with the variable ‘quality’ in the construct in Figure 2 and to affirm that ‘accessible price’ and ‘service’ are viewed as quality traits by these users.
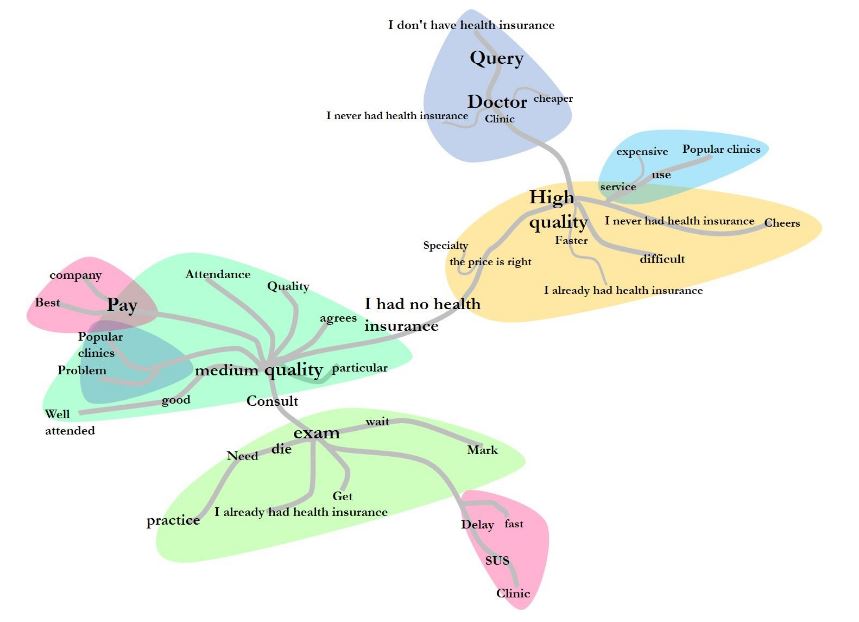
Figure 6:
Analysis of similarities between interviews
Source: the authors (2019).
Our analysis of similarities (Figure 6) shows how the words and phrases are interconnected and thus helps visualize the content structure of the textual corpus. Seven items stand out: ‘average quality’, ‘high quality’, ‘pay’, ‘diagnostic testing’, ‘delay’, ‘no insurance’, and ‘SUS’. Each one originates a branch of words with a significant incidence of occurrence (e.g., ‘easy’, ‘service’, ‘quality’, ‘agree’, ‘company’, ‘specialties’, ‘faster’, ‘health’, ‘use’, low-cost clinics’, ‘cheaper’, ‘appointment’ and ‘physician’).
Final considerations
The content of the interviews is compatible with the literature on disruptive innovation reviewed for this study. According to Corsin and Di Minin (2014), disruption occurs when technology is made available at a lower cost. Here, we return to the variables indicated by Christensen et al (2018) in the relationship between disruptive innovation and consumer: “market disruptions”, “low-income consumer”, “quality” and “accessible”.
Thus, ‘accessible’ was expressed in affordable prices which some interviewees identified as a condition for high quality); ‘market disruption’ was identified as the introduction of alternative health care for the uninsured who are unable to wait for SUS appointments, offering prompt service and ease of access to testing and specialized care; ‘quality’ was associated with fair prices, service and specialties; ‘low-end or marginalized consumers’ were uninsured SUS users invited to attend low-cost clinics offering diagnostic testing and appointments with specialists.
As for the effect of market disruption, the interviewees may be segregated into two groups: those who had already had health insurance and those who had not. This indicates that low-cost clinics are a new-market type of disruptive innovation, corroborating the perspective of Christensen and Raynor (2013) on the development of products or services with lower cost resources, which meets the needs of low-income consumers proposed by new companies who have entered the market.
The interviewees who reported having health insurance in the past did so in association with lost employment benefits. Thus, the introduction of the model of low-cost clinics is clearly a new-market innovation (Christensen et al., 2015), with companies segmenting and targeting neglected markets and achieving a status of adequate functioning, in this case by providing faster and cheaper specialized medical and diagnostic services.
Among the study limitations was the lack of logistic support to extend sampling to cities other than Fortaleza (considering the size of the country). Among the contributions is the relevance of our findings to investors and entrepreneurs who are thus made aware of their role in the introduction and development of an innovative model and the need for running adjustments to remain competitive in the sector. In addition, our analysis of disruptive innovation in the health care sector represents an important contribution to the scarce literature on this specific topic and favors the integration of organizations and universities.
Future investigations might employ exploratory factor analysis to evaluate the association between the variables in the construct, or confirmatory factor analysis to test hypotheses involving these variables. Finally, other segments of the service sector might be sampled for cross-sectional comparisons with regard to disruptive innovation.
References
Abernathy, W. J., & Clark, K. B. (1985). Innovation: Mapping the winds of creative destruction. Research Policy, 22(2), 102-102.
Agência Nacional de Saúde Suplementar (ANS) (2018). ANS divulga dados do setor referentes a dezembro/2017. Rio de Janeiro. Acesso em: http://www.ans.gov.br/aans/noticias-ans/numeros-do-setor/4291-ans-divulga-dados-do-setor-referentes-a-dezembro-2017#:~:text=Os%20dados%20s%C3%A3o%20referentes%20a,com%20o%20m%C3%AAs%20de%20novembro.
Bencke, F. F., Gilioli, R. M., & Royer, A. (2017). Disruptive innovation: an analysis of the empirical research published in brazil. Brazilian Journal of Management & Innovation, 5(2), 159-180.
Bauer, M. W. & Gaskell, G. (2002). Pesquisa qualitativa com texto, imagem e som: um manual. Petrópolis: Editora Vozes.
Christensen, C. M., McDonald, R., Altman, E. J., & Palmer, J. E. (2018). Disruptive innovation: An intellectual history and directions for future research. Journal of Management Studies, 55(7), 1043-1078.
Christensen, C. M. (1997). The innovator’s dilemma: When technologies cause great firms to fail. Boston: Harvard Business School Press.
Christensen, C. M., Anthony, S. D., & Roth, E. A. (2007). O futuro da inovação. Rio de Janeiro: Elsevier.
Christensen, C. M., Grossman, J. H., & Hwang, J. (2009). Inovação na Gestão da Saúde: Solução Disruptivas para Reduzir Custos e Aumentar Qualidade. São Paulo: Bookman Editora.
Christensen, C., & Raynor, M. (2013). The innovator's solution: Creating and sustaining successful growth. Boston: Harvard Business Review Press.
Christensen, C. M., Raynor, M. E., & McDonald, R. (2015). What is disruptive innovation. Harvard business review, 93(12), 44-53.
Chaym, C. D., Barroso, W. D. A., Melo, J. M. G. N., Benayon, P. A., & Moreira, A. F. (2018). Produção de Conhecimento em Ciência, Tecnologia & Inovação: uma avaliação dos Doutores formados pela Rede Nordeste de Biotecnologia. Revista Gestão em Análise, 7(2), 133-150.
Corsi, S., & Di Minin, A. (2014). Disruptive innovation… in reverse: Adding a geographical dimension to disruptive innovation theory. Creativity and Innovation Management, 23(1), 76-90.
Costa, L. S. (2016). Inovação nos serviços de saúde: apontamentos sobre os limites do conhecimento. Cadernos de Saúde Pública, 32(2), 1 – 12.
Dan, Y., & Chieh, H. C. (2008). A reflective review of disruptive innovation theory. International Journal of Management Reviews, 12(4), 402 - 414
Dubickis, M., & Gaile-Sarkane, E. (2015). Perspectives on innovation and technology transfer. Procedia-Social and Behavioral Sciences, 213, 965-970.
Duarte, C. M. R., Pedroso, M. D. M., Bellido, J. G., Moreira, R. D. S., & Viacava, F. (2015). Regionalização e desenvolvimento humano: uma proposta de tipologia de Regiões de Saúde no Brasil. Cadernos de Saúde Pública, 31, 1163-1174.
Drucker, P. F. (1986). Innovation and Entrepreneurship. New York: Harper Collins Publisher.
Damasceno, E. A. (2008). Lexicometria, geração de descritores, construção de ontologias e ensino de línguas: implicações e perspectivas. Múltiplas Perspectivas em Linguísticas. Uberlância.Edufu.
Foss, N. J., & Saebi, T. (2017). Fifteen years of research on business model innovation: How far have we come, and where should we go?. Journal of Management, 43(1), 200-227.
Gassmann, O., Frankenberger, K., & Csik, M. (2013). The St. Gallen business model navigator.
Gerring, J. (2017). Qualitative methods. Annual Review of Political Science, 20 (5), 15-36.
Godoy, C. V., & da Silva, J. B. (2018). O fenômeno de expansão das clínicas médicas populares: ressignificação do bairro centro em Fortaleza-Ceará. Revista Brasileira de Geografia Médica e da Saúde, 14(28), 32-49.
Hamel, G. (2000). Leading the Revolution. Boston: Harvard Business School.
Hamel, G., & Prahalad, C. K. (1994). Competing for the future. Harvard business review, 72(4), 122-128.
Huang, K. E., Wu, J. H., Lu, S. Y., & Lin, Y. C. (2016). Innovation and technology creation effects on organizational performance. Journal of Business Research, 69(6), 2187-2192.
Hart, S. L., & Christensen, C. M. (2002). The great leap: Driving innovation from the base of the pyramid. MIT Sloan management review, 44(1), 51.
Instituto Brasileiro de Geografia e Estatística (IBGE) (2017). Conta satélite de saúde 2010-2015. Rio de Janeiro. Acesso em: https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=2101690.
Jurca, R. D. L. (2018). Individualização social, assistência médica privada e consumo na periferia de São Paulo. Doctoral dissertation, University of Sao Paulo. Retrieved from: https://teses.usp.br/teses/disponiveis/6/6135/tde-04052018113137/publico/RicardodeLimaJurcaSIMPLIFICADA.pdf.
Knight, K. E. (1967). A descriptive model of the intra-firm innovation process. The journal of business, 40(4), 478-496.
Krugman, P. (1979). A model of innovation, technology transfer, and the world distribution of income. Journal of political economy, 87(2), 253-266.
Nogami, V. K., & Veloso, A. R. (2017). Disruptive innovation in low-income contexts: challenges and state-of-the-art national research in marketing. Revista de Administração e Inovação, 14(2), 162-167.
Schiavi, G., & Behr, A. (2018). Emerging technologies and new business models. Innovation & Management Review, 15(4), 338-355.
Stake, R. E. (2011). Pesquisa Qualitativa: estudando como as coisas funcionam. Porto Alegre: Artmed.
Schumpeter, J. A. (1984). Capitalismo, socialismo e democracia. Rio de Janeiro: Zahar Editores.
Teece, D. J. (2010). Business models, business strategy and innovation. Long range planning, 43(3), 172-194.
Vieira, S. F. A. (2010) Inovação Disruptiva no Ensino Superior. Encontro da Associação Nacional de Pós-Graduação e Pesquisa em Administração, Rio de Janeiro. Acesso em: http://www.anpad.org.br/diversos/trabalhos/EnANPAD/enanpad_2010/GCT/2010_G CT1848. pdf.