Artículos de revisión
Systematic review about 10 interventions in dermatitis. A document from the Latin American Society of Allergy, Asthma, and Immunology
Revisión sistemática sobre 10 intervenciones en dermatitis. Un documento de la Sociedad Latinoamericana de Alergia Asma e Inmunología
 Mario Roberto Sánchez
Bruno Barreto
Luis Felipe Ensina
Silvia Antonieta Uriarte-Obando
Raúl Lázaro Castro-Almarales
Romina Adorni
Milagros Lázaro
Ariel Callero-Viera
Iris Ale
Leidy Álvarez
Mario Roberto Sánchez
Bruno Barreto
Luis Felipe Ensina
Silvia Antonieta Uriarte-Obando
Raúl Lázaro Castro-Almarales
Romina Adorni
Milagros Lázaro
Ariel Callero-Viera
Iris Ale
Leidy Álvarez
Systematic review about 10 interventions in dermatitis. A document from the Latin American Society of Allergy, Asthma, and Immunology
Revista alergia México, vol. 66, no. 4, pp. 426-455, 2019
Colegio Mexicano de Inmunología Clínica y Alergia, A.C.
Received: 13 June 2019
Accepted: 19 October 2019
Abstract: The Latin American Society of Allergy, Asthma, and Immunology (SLAAI) conducted a systematic search in the Medline and LILACS’ database in order to get articles linked to 10 current questions about dermatitis. The assessment of the quality of the evidence and the strength of the recommendations was made through the GRADE system. The completeness and transparency of the recommendations for this clinical guide were assessed with the AGREE Reports Verification Checklist. The final document was shared with physicians, allergists, dermatologists, and pediatricians, and with patients and academic institutions such as universities and medical scientific societies for external assessment. According to the review, clinical scales should be used to measure the severity of the dermatitis, and some interventions such as the use of probiotics may benefit the patient; nevertheless, more studies are required before this management option can be used in the everyday practice. Other interventions such as dietary restrictions and the use of antihistamines seem to be well-founded only in particular cases and they should not be a general recommendation for all patients. This practical guide presents recommendations for the treatment of atopic dermatitis; these recommendations can be helpful for medical staff, patients, and health systems.
Keywords: Allergy, Allergen, Atopy, Dermatitis, Eczema, Probiotics, Antihistamines, Dupilumab, Microbiota.
Resumen : La Sociedad Latinoamericana de Asma, Alergia e Inmunología realizó una búsqueda sistemática en la base de datos de Medline y LILACS para obtener artículos relacionados con 10 preguntas actuales sobre dermatitis. La evaluación de la calidad de la evidencia y la fuerza de las recomendaciones se realizaron a través del sistema GRADE. La integridad y la transparencia de las recomendaciones se evaluaron con la lista de verificación de informes AGREE. El documento final se compartió con médicos, alergólogos, dermatólogos y pediatras, pacientes e instituciones académicas, como universidades y sociedades médicas científicas, para su evaluación externa. Conforme a la revisión, se debe usar escalas clínicas para evaluar la gravedad de la dermatitis; algunas intervenciones como el uso de probióticos pueden beneficiar al paciente, sin embargo, se requieren más estudios antes de utilizarlas en la práctica diaria. La restricción de la dieta y el uso de antihistamínicos parecen tener fundamento solo en casos particulares y no deben indicarse a todos los pacientes. Esta guía práctica presenta recomendaciones para el tratamiento de la dermatitis atópica que pueden ser útiles para el personal médico, los pacientes y los sistemas de salud.
Palabras clave: Alergia, Alérgeno, Atopia, Dermatitis, Eccema, Probióticos, Antihistamínicos, Dupilumab, Microbiota.
Background
Atopic dermatitis (AD) affects a large portion of the population, particularly children under 5 years.1,2,3,4 It usually precedes the development of other allergic diseases such as food allergy, asthma, rhinitis, and/or conjunctivitis, therefore, it is considered as an important risk factor for these diseases.5,6
AD has a great impact on the quality of life of patients. The frequency of physiological or psychiatric problems in patients with moderate to severe dermatitis is higher than those in patients with diabetes mellitus.7 The economic cost of skin hydration, physician visits, and drug treatment has increased in the last years.8,9,10 Therefore, the evaluation and management of AD should be comprehensive and must include all the stakeholders: patients, relatives, and health care systems.
Although there are excellent guidelines offering an appropriate approach to manage this disease,11,12 transparent evidence-based guidelines following the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) approach13 are needed.14 Since each patient must receive personalized treatment, the recommendations presented here may not be appropriate for all patients, nevertheless, they offer a kickoff for disease management based on current scientific evidence.
Methods
-
Update objectives: to evaluate some commonly used interventions in dermatitis and new practical interventions.
-
Target population: patients with AD regardless their age, but it is focused on under-6 children because they are the population with the highest AD incidence.15
-
Implementation place: these recommendations are to be implanted on outpatient clinical management.
-
Target users: general practitioners, family doctors, dermatologists, allergists, and pediatricians.
-
Clinical aspects covered: evaluation of topical and systemic dermatitis management interventions. Prevention and acute management. Outpatient management.
-
Clinical aspects not covered: management in hospitalization and/or emergencies.
Definitions
According to the recommendation of the WAO (World Allergy Organization),16 it is better to use the term “eczema” than “dermatitis”, while confirmatory immunological studies are done; also, WAO recommends limiting the use of the term “atopic eczema” when a mediation IgE is demonstrated in the pathophysiology of the disease, and “non-atopic eczema” when it is discarded. In many countries, the term “dermatitis” is used as an equivalent to “eczema”, so, in this guideline and in the bibliographic search we use both.17,18,19
Staff conformation
Since the first revision of the Dermatitis-SLAAI (Sociedad Latinoamericana de Asma, Alergia e Inmunología) Guidelines in 2015,20 new evidence has accumulated about some interventions in AD.
For this update, a stakeholder group with allergists, dermatologists, pediatricians, epidemiologists, and immunologists, developed the review protocol and made an open invitation to SLAAI members to participate.21 Subsequently, those members who correctly performed the protocol tasks and writing the guide were included in the staff.
Protocol to the guide update
This guideline update was focused on new information about some practical interventions in dermatitis. Characteristics of the epidemiology, classification, and pathogenesis of the disease are discussed in detail in the 2015 Consensus.20 ARIA (Allergic Rhinitis and its Impact on Asthma) report protocol was used as a model22 and the update protocol was based on PRISMA recommendations (see supplementary material).23
By using the Delphi process,24 the panel staff reached an agreement on the topics that required an update and on new topics that deserved to be included, and performed a systematic review of the literature to identify and summarize the evidence for each one of them (see supplementary material). Each topic is presented as a clinical question, and the answer to each question includes a conclusion with the strength of the recommendation according to the GRADE system.14 The AGREE Reporting Checklist was used to evaluate the completeness and transparency of the guideline recommendations.
For external validation and to assess the clarity of the concepts and their applicability, the manuscript was presented to allergists, dermatologists, general physicians from academic and external scientific institutions, and groups of patients. External recommendations were then discussed again by the staff and included in the manuscript.
Questions and outcomes of interest
The guideline panel deemed the following outcomes to be important to patients: cutaneous symptoms like pruritus and eczema, quality of life, work/school performance, and serious adverse effects. In general, these variables were considered critical for the decisions to be made, regarding the answer to each question. The questions chosen were:
- 1. How should we classify atopic dermatitis in clinical practice?
- 2. Can atopic dermatitis be prevented?
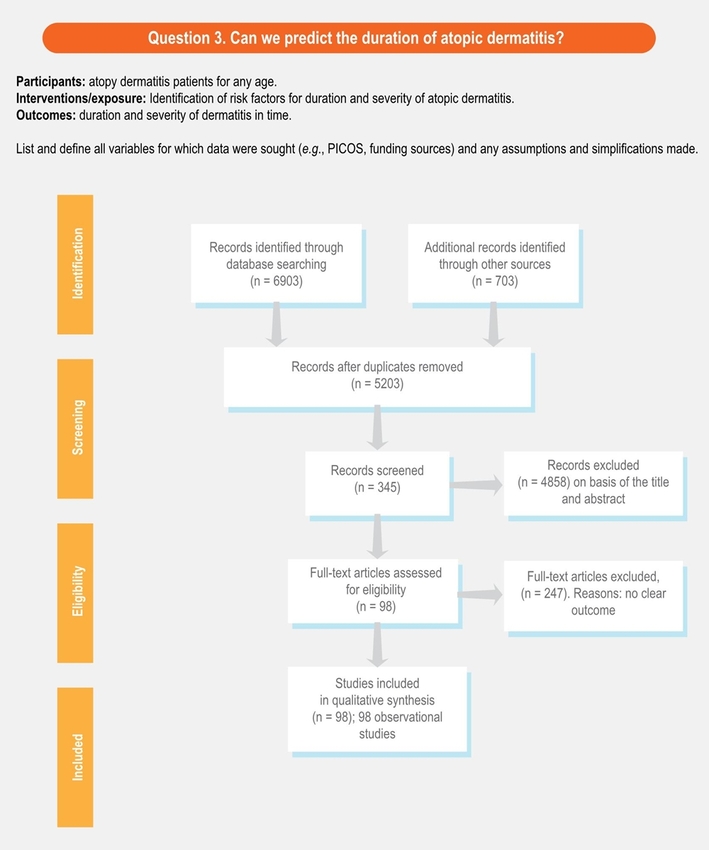
- 3. Can we predict the duration of atopic dermatitis?
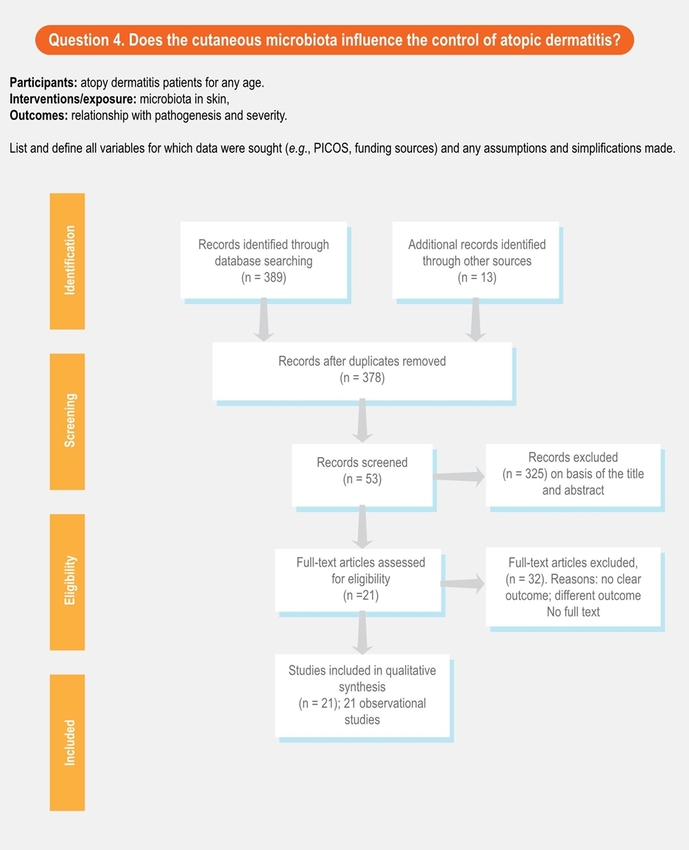
- 4. Does the cutaneous microbiota influence the control of atopic dermatitis?
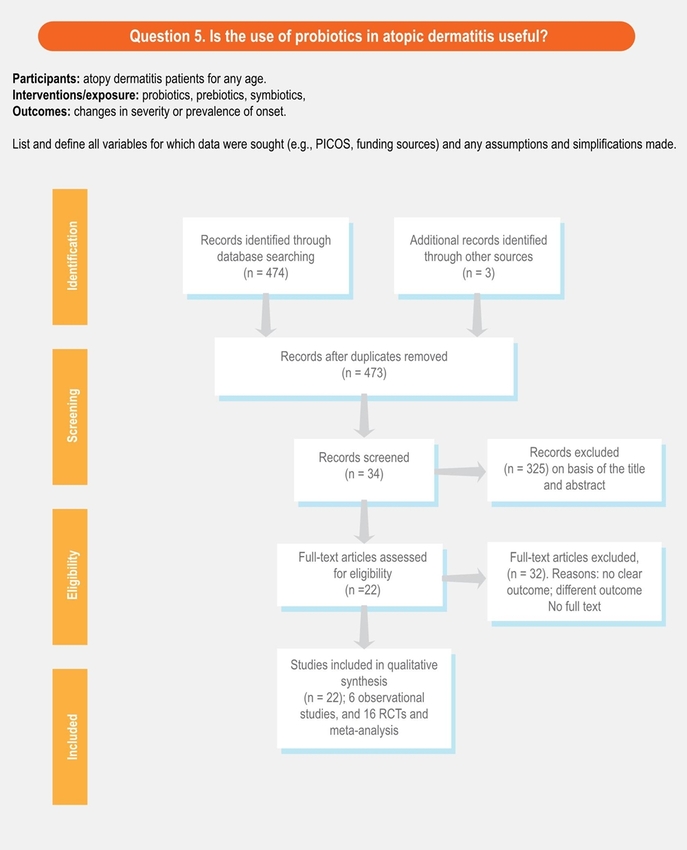
- 5. Is the use of probiotics in atopic dermatitis useful?
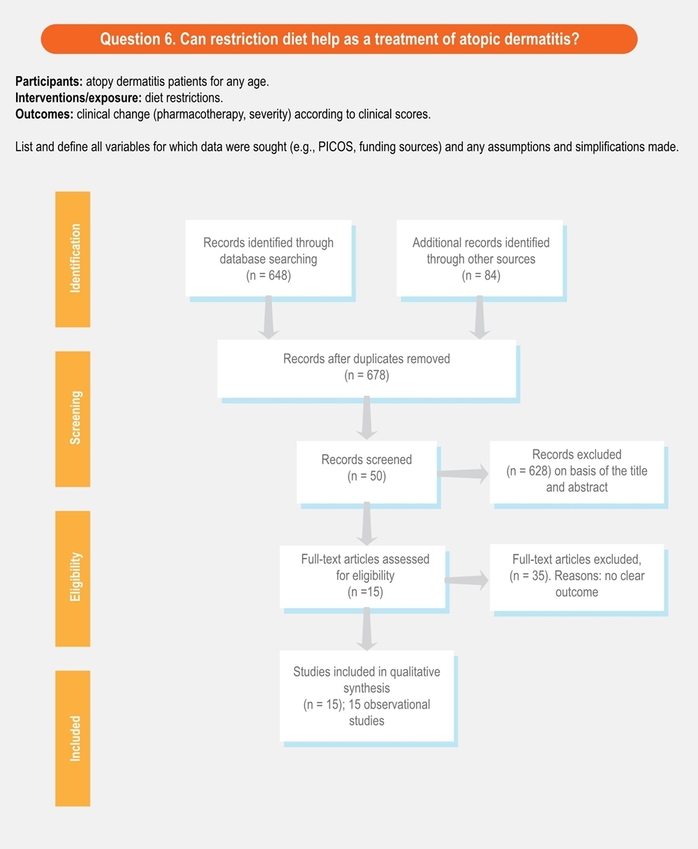
- 6. Can restriction diet help as a treatment of atopic dermatitis?
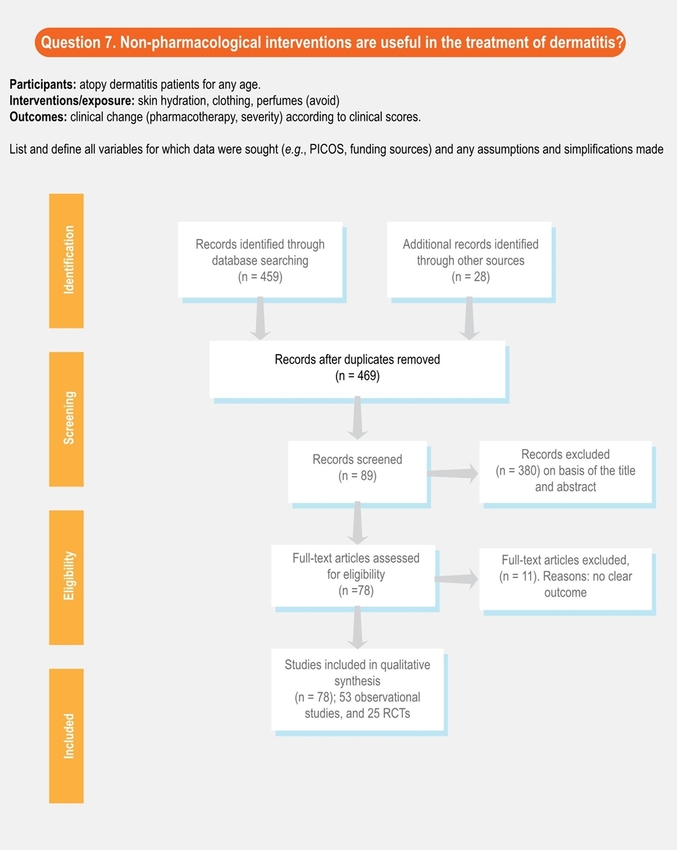
- 7. Are non-pharmacological interventions useful in the treatment of dermatitis?
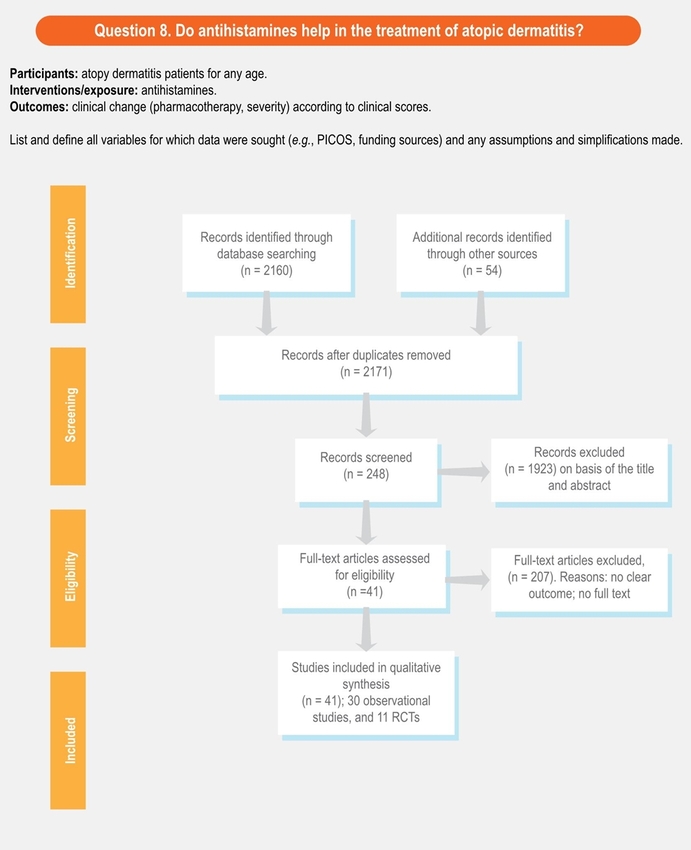
- 8. Do antihistamines help in the treatment of atopic dermatitis?
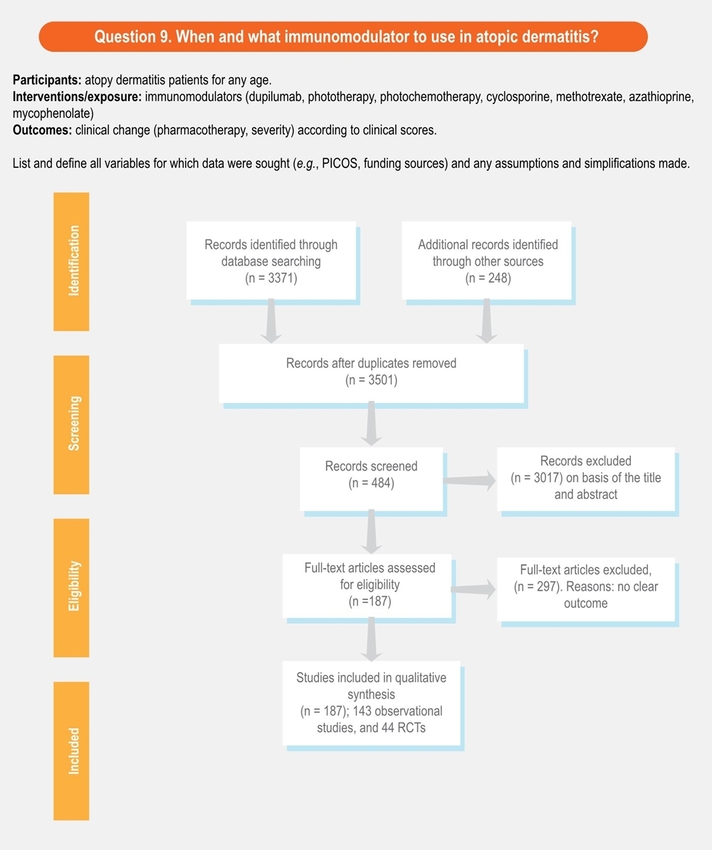
- 9. When and which immunomodulator should be used in atopic dermatitis?
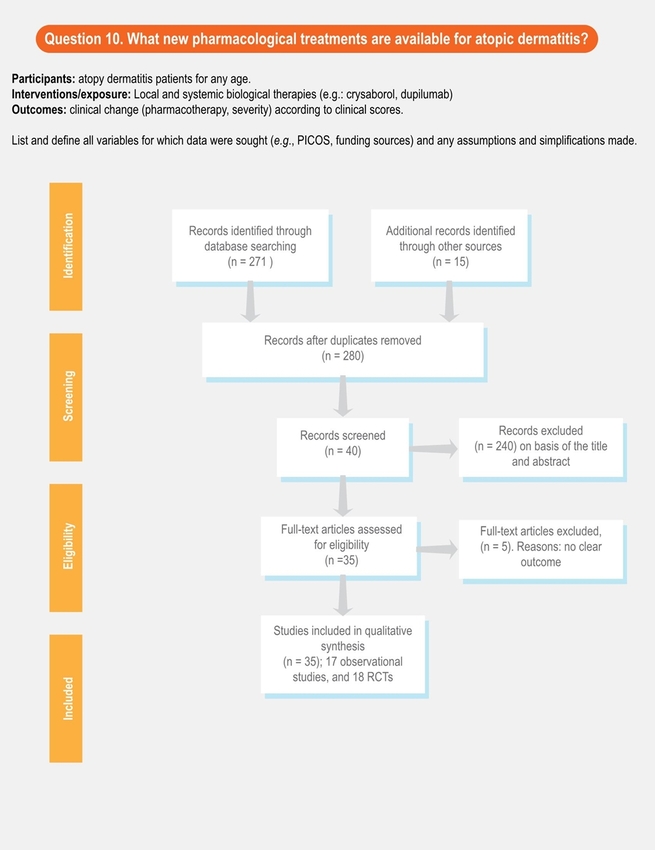
- 10. What new pharmacological treatments are available for atopic dermatitis?
Bibliographic search and evidence review
We systematically searched articles from December 2000 to December 2018 from the Medline and LILACs electronic databases. Titles and abstracts, and subsequently full-text articles were screened in duplicate to assess eligibility. Articles in English, Spanish and Portuguese were reviewed.
Studies were included if they provided empirical data related to the panel staff questions (clinical trials, cohort studies, case-control studies). We excluded narrative reviews and case reports. We shared the bibliography collected among the team members; in case any staff member considered it was necessary to include an additional reference, this was discussed.
Clinical recommendations
We prepared evidence summaries for each question according to the GRADE approach.14,25 The certainty of the evidence was categorized into four levels: strong, moderate, low, and very low. Specific criteria for evidence classification are presented in figure 1.
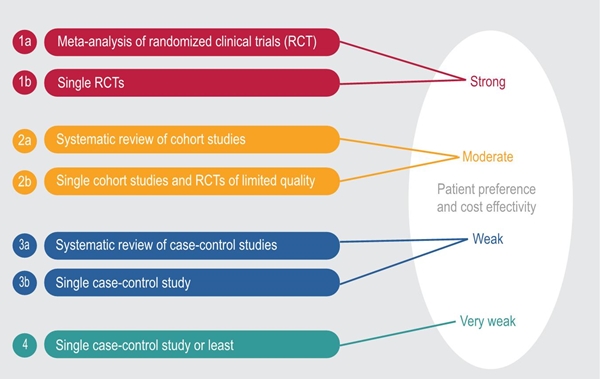
Figure 1
Classification of the evidence. The recommendation was classified based on the grade of evidence and the interpretation of the committee. We considered patient preferences and cost effectivity.
For each question, we summarized all information including a concise description of desirable and undesirable health effects.26,27 The answer to each question was reviewed by the panel staff, who provided feedback by means of electronic communications. The answers were modified accordingly when it was necessary. Recommendations and their strength were decided by consensus.
Results
Limitations from the systematic review
The protocol for this systematic review was not previously registered in any database, which limits the reproducibility of the results. However, since in the guide we considered the patients’ opinions and the reality of the clinical practice in different countries, these variables, that influenced the recommendation, could not be reproduced only with the bibliographic search. In supplementary material 1 and 2, an approach of the search carried out for each question is presented. However, a standardized evaluation to avoid the risk of bias was not used.
Limitations from articles
There is a considerable heterogeneity among the studies, patients’ characteristics, evaluation of clinical control, and the safety of each intervention. Additionally, many studies indicated the response to treatment without clarifying the doses of the drug, the treatment length, measurement of treatment efficacy, the speed of the effect, and/or follow-up period. We provide the rationale for the recommendations and the consideration of some factors that influenced the recommendations.
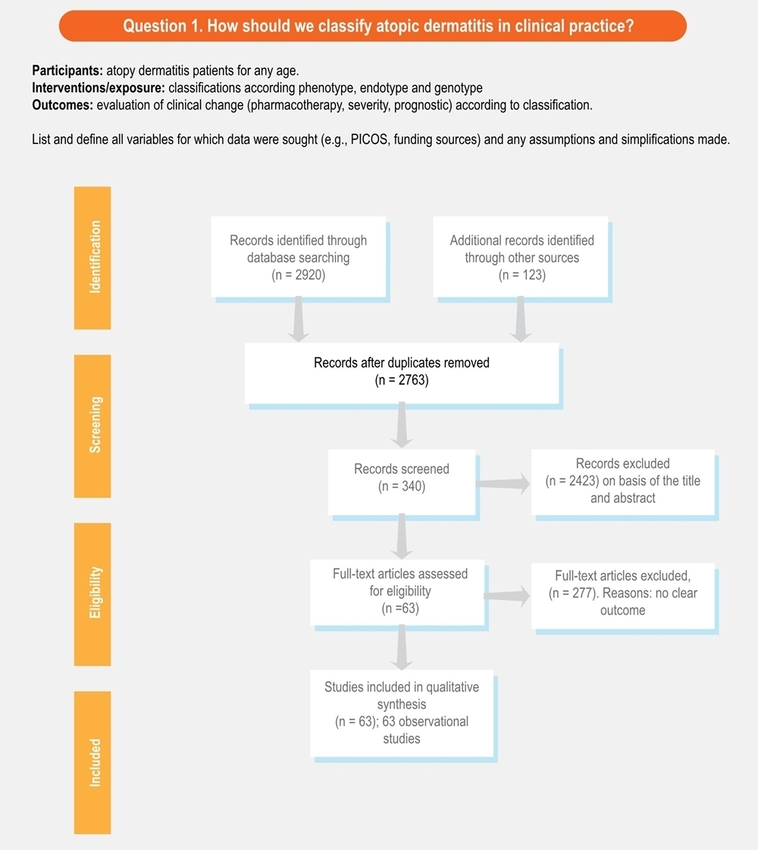
1. How should we classify atopic dermatitis in clinical practice?
Recommendation. Severity classification is available to all physicians and it is useful to define interventions (high, 1a). Atopy-based classification (yes/no) seems to be useful for the prognostic of duration in children (moderate 1a).
Explanation. AD can be classified in several ways.20 Some classification proposals according to endotypes have been done,28,29 but their utility in clinical practice is unclear. The presence or not of atopy seems to be associated with the patient’s clinical characteristics and the probability of remission or not, thus, the classification of allergic or non-allergic eczema according to the skin prick test result or IgE serum can be useful in the clinical practice.
The classification of the severity is established with different scoring scales, such as: Severity Scoring Atopic Dermatitis (SCORAD) and Eczema Area and Severity Index. These scores are defined according to three parameters: extension of the disease and type of injury; some scales also include pruritus and sleep disturbance as perceived by the patient. We recommend the use of these or any other validated clinical scale since they allow physicians to classify the severity of the patient, the degree of affectation and allow the decision making regarding the most appropriate medical intervention.
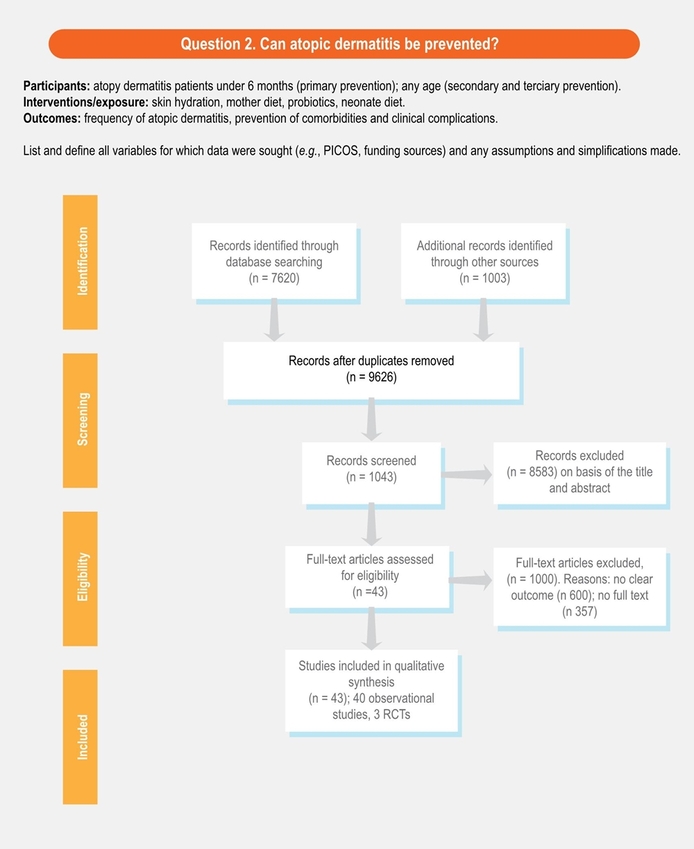
2. Can atopic dermatitis be prevented?
Recommendation. Primary prevention: early skin hydration (first six months of life) seems to decrease the risk of dermatitis (strong 1b). Secondary prevention: skin hydration and inflammation control improve the clinical control of dermatitis, and some evidence suggests that these interventions could modify the severity of eczema (moderate 2b).
Explanation. Primary prevention: the increase of IgA levels with breast milk30 and the use of milk hydrolyzed formulas in high-risk infants reduced the cumulative prevalence of eczema.31 Although these results are supported by some studies, other research studies do not reproduce these results, so their implementation cannot be widely recommended.
Two multicenter studies demonstrated that the daily use of emollients, with application on all the skin, significantly reduced the cumulative incidence of AD in children at 12 and 36 months, which corresponded to a relative risk reduction, between 30% and 50%.32,33 It is necessary to evaluate the cost-effectiveness of this intervention.34
Secondary prevention. The daily use of emollients in patients with mild-moderate disease prevents and delays exacerbations, as well as decreases the use of topical steroids and prolongs eczema-free time.35,36,37 Although there is controversial evidence,38 it seems that vitamin D supplementation during the winter season improves AD related to winter.39,40
3. Can we predict the duration of atopic dermatitis?
Recommendation. Maternal eczema, onset after two years old, severe onset, are associated with long duration of dermatitis periods (over 14 years old) (moderate 2a). Nevertheless, no single factor is enough to predict the duration of the disease (strong 2b). The creation of a prognostic model evaluating the magnitude of each individual factor could be useful.41
Explanation. Most childhood dermatitis remitted before puberty, nevertheless, from 1% to 25% of patients persist with symptoms even in adulthood.20,41 Findings from 14 systematic reviews published before 2016 observed that persistent atopic dermatitis is associated with more severe disease at the time of diagnosis, onset after the age of two years and being a female.42 A systematic review including 45 studies was considered and found that a later onset increased persistence.43 Some genetic factors have been associated with persistent dermatitis, but these factors are not easy to use in clinical practice.44
Some studies suggest that children with atopy from house dust mites or foods before their first year should be considered at risk of AD persistence;45,46 although it is not clear if atopy is a consequence of greater severity, it could be used as a duration predictor.
4. Does the cutaneous microbiota influence the control of atopic dermatitis?
Recommendation. The cutaneous microbiota influences the control of AD (strong 1b), however, heterogeneity in intervention strategies on bacterial overgrowth (topic or systemic antibiotics), makes comparative evaluations and the power of evidence difficult to extend and evaluate (moderate 2a).
Explanation. Microbial colonization of skin begins, more effectively, after birth and depends, in part, on the type of delivery; cesarean delivery children have a cutaneous microbiota profile that resembles maternal skin, while cutaneous microbiota of vaginal delivery children has a more diversified profile, similar to the maternal vaginal scenario.47 During puberty, new changes occur in skin microbiota.48 There are several mechanisms by which changes in microbial skin diversity (dysbiosis) affect the development of atopic dermatitis; the production, by these dysbiosis bacteria, of several enzymes, such as: proteases (which induce corneocyte desquamation); lipases (which break down lipids of skin barrier); ceramidases (which break down the ceramides present in the barrier structure).49,50 This bacterial overgrowth, with subsequent biofilm formation and mainly related to the pathogenic strains of Staphylococcus aureus (methicillin-resistant Staphylococcus aureus), would be directly related to changes in the cutaneous barrier.51,52,53
Cutaneous microbiota is associated with dermatitis severity, but it is less clear its effect in the pathogenesis; antibiotic interventions are also expected to be able to improve the dermatitis symptom scores. However, a systematic review,54 in 21 studies with different interventions (oral antibiotics, antibacterial soaps, topical steroids/antibiotics/antifungal, baths with antibacterial solutions) did not show differences statistically significant.
5. Is the use of probiotics in atopic dermatitis useful?
Recommendation. There is a potential effect of the use of probiotics in the prevention of atopic dermatitis (moderate 3a); however, methodological limitations, a wide variety of strains and the dosage schemes, lead to discordant and contradictory results and their routine use is not recommended.
Explanation. Probiotics could help dermatitis through restoration in the function of the intestinal barrier, degrading food antigens, regulating the Th1 and Th2 response, regulating the composition and activity of the intestinal microbiota and stimulating the production of IgA.55 The WAO in a systematic review indicates that is likely net benefit from using probiotics the primary prevention of eczema.56 The use of Lactobacillus rhamnosus, Lactobacillus salivarius, Bifidobacterium lactis and others, in several small studies has shown relief of symptoms, which results in an improvement of SCORAD,57,58 being more effective during the first two years of life.
Although probiotics are safe and are used as a reasonable option of dermatitis preventive treatment in under-6-month children or high-risk pregnant women, their impact on active treatment appears to be reduced.59,60
However, in order to apply this recommendation, solving several practical questions that currently do not have an answer is necessary, for instance: Does the type of microbiota affect the impact of probiotics? What dosage? For how long? What strains should be used?.61 The lack of control of these variables in the different clinical trials limits the ability to implement this intervention.
6. Can restriction diet help as a treatment of atopic dermatitis?
Recommendation. In patients with an objective demonstration of exacerbation of dermatitis by a food, dietary restriction is indicated (moderate 3a). Atopy to food allergens is not enough to initiate a dietary restriction (strong 1a).
Explanation. Frequently, patients associate food consumption with the onset or worsening of their disease.62,63,64 The sensitization to foods in children with AD is very prevalent, being the majority of cases asymptomatic (without clinical relevance).65,66 The subgroup of moderate to severe AD have a higher risk of sensitization to food allergens and this is translated into a high risk of true food allergy.65,67,68 The clinical history, along with an allergology evaluation, can help to identify suspect foods, but it is necessary to verify with restriction diets for 3 to 4 weeks or controlled oral challenges.
The avoidance of foods previously tolerated or never ingested due to a positive skin test without clinical confirmation of hypersensitivity reactions, is associated with an increased risk of severe reactions, after their reintroduction into the regular diet.69,70,71,72 Therefore, the avoidance of food should only occur in cases of AD with clinical impact confirmation.73 In cases in which negative results in oral challenges or food restrictions did not improve AD, foods must be reintroduced.74
7. Are non-pharmacological interventions useful in the treatment of dermatitis?
Recommendation. The hydration of the skin is a non-pharmacological intervention with adequate evidence for the treatment and prevention of eczema exacerbation in dermatitis (moderate 2a). Although the evidence is weak and the magnitude of this measure is not known, we recommend the use of hypochlorite, loose and preferably cotton-made clothing in patients with AD (low 3a-4). We discourage the use of products with perfume or clothing that may increase sweating (low 3b).
Explanation. The treatment of AD is a challenge because it is a chronic disease, which occurs with periods of outbreak and remission. The therapeutic approach of dermatitis includes two aspects: the management of active eczema and the prevention of new exacerbations.
The emollient preparation should be chosen according to the skin dryness degree, the areas of application, and the patient’s acceptance.75,76 Using tight or rough clothes, personal care products with alcohol or perfume, exposing oneself to heat or carrying out activities inducing heavy sweating, among others, should be avoided as far as possible.77,78 Some recommendations with low evidence but cost-effective are usually done: baths should be tempered and brief, no more than five minutes. Skin hygiene and cleaning should be smooth, scabs should be removed; avoid perfumes. Using hypochlorite during bath could reduce colonization of some bacteria.79,80,81 Using comfortable, loose and preferably cotton-made clothing seems to prevent skin exacerbation.
8. Do antihistamines help in the treatment of atopic dermatitis?
Recommendation. Some studies support the use of second-generation antihistamines to decrease pruritus in dermatitis (low 4). However, due to the lack of high-level evidence, we cannot make a recommendation in favor of or against the use of H1-antihistamines in the treatment of dermatitis-associated pruritus.
Explanation. Pruritus is usually the most distressing feature of AD.82 Histamine is one of the multiple mediators of itching in dermatitis. However, it is not clear if it has a key role.83 There are no large, randomized, double-blind, and placebo-controlled studies with precise endpoints on the efficacy of antihistamines in AD. Antihistamines (especially first generation) have been used in dermatitis to reduce scratching, however, these drugs, in most of the studies, are not more effective than placebo.84,85,86,87 Nevertheless, some studies, especially those with second-generation antihistamines, suggest a possible positive effect in pruritus and repair of the cutaneous tissue;88,89,90,91 these effects increased with a topical steroid.92
First generation sedating antihistamines have been used in dermatitis to promote sleep84,85 but sedating antihistamines reduce the rapid-eye-movement (REM)-sleep, affecting the quality of sleep and directly interfering with work efficiency in adults and learning skills in children.93
9. When and what immunomodulator should be used in atopic dermatitis?
Recommendation. The decision to start systemic therapy should be based on the severity of the symptoms, but also on the impact on the patient’s quality of life, as well as on the consideration of the risks and benefits of systemic therapies for each individual patient (strong 1b). Many randomized controlled trials (RCTs) with immunomodulator interventions for dermatitis have not used standardized efficacy outcome measures, which makes interpretation of results difficult. In addition, comparative studies between the existent systemic treatments in dermatitis are rare.
Explanation. Most patients with AD respond satisfactorily to conventional topical management. However, 10% to 50% of patients may not achieve adequate disease control with these regimens and require systemic immunomodulatory/immunosuppressive therapies. Before considering a systemic therapy, it should be determined whether the failure of conventional therapies is due to the severity of the disease, comorbidities, or lack of adherence to the treatment. The action mechanism of each one of these interventions is explained in detail in the previous dermatitis-SLAAI guideline.20 In table 1, we present some details of each one of some of these therapies. It is important to note that most of these therapies are not approved by the FDA or EMA for dermatitis.

The selection of the systemic drug for dermatitis, more than a selection step by step, should be based in individual safety profile, availability and access. The use of immunosuppressants can facilitate the onset of respiratory or skin infections. *These medications may have other contraindications, the most frequently described are presented in the table. **Different scales have been used to evaluated efficacy-effectivity, we present the effect size in percent as standard unit. The safety and efficacy of dupilumab in children have not been established.
-
Dupilumab. It was approved in early 2017 for moderate-to-severe adult dermatitis.94,95 Dupilumab is a fully human monoclonal antibody that blocks the alpha subunit of the receptor interleukin (IL) 4 and IL-13. The blockade by dupilumab of these key drivers of type 2 helper T-cell (Th2)-mediated inflammation help in the treatment of AD. Patients treated with dupilumab had marked and rapid improvement in all the evaluated measures of AD disease activity; Dupilumab also reduces the need for systemic steroids (NCT01259323, NCT01385657, NCT01639040, and NCT01548404.).95,96,97,98
-
Phototherapy or photochemotherapy. It is one of the alternatives with the highest number of articles and some RCT supporting its effectiveness. However, the need of attendance to the center of execution between 2 to 4 times per week limits its access and use.99,100,101,102 Different forms of light therapy are available, and have proved efficacy: narrowband (NB)-UVB, broadband (BB)-UVB, UVA, UVA1, cold-light UVA1, UVA and UVB (UVAB), full-spectrum light (including UVA, infrared and visible light), psoralen plus UVA, and other forms of phototherapy. One of the principal limitations for phototherapy is the requirement to attend several times per week for its application. However, some new home-applied modalities are being developed.103
-
Systemic corticosteroids (SCSs). They are not recommended as a control intervention for the treatment of dermatitis. Their use should be limited to very short terms (up to 1 week) during acute flares in need of immediate relief and as a transition to steroid-sparing therapies because of their adverse-effect potential.104,105,106
-
Cyclosporine A (CSA). It is an approved drug for severe dermatitis in some countries and numerous studies showed improvement of the skin symptoms by at least 50% after six to eight weeks of therapy.107,108,109,110,111 Once the drug is stopped the symptoms reappear quickly, eventually reaching pretreatment values approximately after 8 weeks from the end of treatment.109,110,111 CSA has been shown to be effective and relatively safe in adults who received up to 1 year of continuous treatment,112,113,114,115,116 but some of these studies had high dropout rates.116 The staff recommended choosing the regimen on an individual basis; it could be reasonable to start with a dose of 2.5 mg/kg/day,114,117 unless a rapid improvement is considered necessary, when a dose of up to 5 mg/kg/day may be used.116,118,119
-
Methotrexate (MTX). Patients receiving MTX should be monitored for hepatic and pulmonary toxicity, and myelosuppression.120 Different studies have shown good efficacy for MTX.121,122 MTX has some advantages and disadvantages compared to CSA but it seems to have a similar effectivity;122,123,124 The onset of control seems to be faster with ciclosporin, but relapse after stopping the medication seems to be less frequent with MTX
-
Azathioprine (AZA). Efficacy of AZA (2.5 mg/kg/day) was tested in some RCT, especially in adults,107,125 with efficacy (30 to 70%) in the severity of eczema and skin pruritus. In an RCT comparing MTX (10-22.5 mg/week) with AZA (1.5-2.5 mg/kg/day), at week 12, no statistically significant differences were found in the clinical impact (MTX SCORAD of 42% (standard deviation [SD], 18%) vs AZA 39% [SD, 25%]),126 but abnormalities in blood count (mostly lymphocytopenia) were statistically and significantly more frequent in the AZA group (p = 0.002).
-
Mycophenolate (MMF). Some case reports or uncontrolled clinical trial data from adults indicate that MMF could be effective in dermatitis.127,128,129,130,131 In an observer-blinded randomized controlled trial in 55 patients, a lower dose CSA (3 mg/kg/d) was found to be equally effective to oral MMF (EC-MPS, 1440 mg/d) as a maintenance therapy for severe dermatitis during a maintenance phase of 30 weeks and a 12-week follow-up period.112 The MMF group had a slower onset of action with 29% of the MMF patients requiring short courses of systemic glucocorticoids compared to none in the CSA group.132
Therapies like omalizumab, interferon gamma, and others, have been used in atopic dermatitis and may be useful for some patients but there are only case reports and case series supporting this recommendation. Some clinical trials are being conducted with omalizumab, but no results have been reported (Clinicaltrials.gov NCT01678092, NCT01179529).
10. What new pharmacological treatments are available for dermatitis?
Recommendation. Dupilumab is recommended in severe AD (strong 1a). Crisaborole is recommended in mild and moderate AD, but a safety-efficacy comparison to other topical interventions is needed (strong 1a).
From the dermatitis-SLAAI guideline in 2015 to these days, two molecules were released to the market and approved by the Food and Drugs Administration (FDA): crisaborole, a topical phosphodiesterase 4 (PDE4) inhibitor, became available in late 2016 in the United States and Europe for mild-to-moderate dermatitis. It can be used topically. Clinical trials have demonstrated its efficacy in treating patients with mild to moderate atopic dermatitis (children > 2 years) (AD-301: NCT02118766; AD-302: NCT02118792).133,134 The potency of crisaborole seems to be equivalent to the one of a moderate-potency steroid , but the frequency of adverse effects seems to be lower; as of now, there is no evidence of atrophy, telangiectasia, or hypopigmentation, resulting from its use.135 However, there are few equivalence or superiority studies comparing this molecule to topical steroids, therefore, at the moment, crisaborole is recommended at the same level as the use of steroids or calcineurin inhibitors.
Dupilumab has been shown to be effective in adult patients refractory to topical steroids and also in patients who did not respond to CSA.136 Among the adverse effects that have been described are the increase of eosinophils in the blood (without apparent clinical impact, but it requires more studies) and a high frequency of conjunctivitis.137 The high cost of dupilumab and the lack of studies in children are the main limitations for its use.
Conclusions
For this update, we covered a small number of topics. However, these were systematically reviewed. Many interventions have been proven in patients with dermatitis, but due to the lack of studies with an adequate design, most of these interventions have a weak or moderate recommendation. Further studies are needed in order to predict the duration and severity of the disease, as well as which interventions are the most appropriate for each patient.
Funding
This article was supported by the Group of Clinical and Experimental Allergy, from the Clinic IPS Universitaria of the University of Antioquia (Medellín, Colombia).
Acknowledgment
Special thanks to the scientific societies that participated as external reviewers of the guide: Mauricio Sarrazola and Eizabeth García (Asociación Colombiana de Alergia Asma e Inmunología); Mirta Álvarez Castelló, and Olaine Gray (Sociedad Cubana de Alergia, Asma e Inmunología Clínica); Natalia Hernández (Asociación Colombiana de Dermatología); Dirceu Solé (Associação Brasileira de Alergia e Imunologia); and Diana Gavazza (Academia Colombiana de Pediatría y Puericultura).
References
Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI, ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124(6):1251-1258. DOI: 10.1016/j.jaci.2009.10.009
Grize L, Gassner M, Wüthrich B, Bringolf-Isler B, Takken-Sahli K, Sennhauser FH, et al. Trends in prevalence of asthma, allergic rhinitis and atopic dermatitis in 5-7-year old Swiss children from 1992 to 2001. Allergy. 2006;61(5):556-562. DOI: 10.1111/j.1398-9995.2006.01030.x
Weber AS, Haidinger G. The prevalence of atopic dermatitis in children is influenced by their parents’ education: results of two cross-sectional studies conducted in Upper Austria. Pediatr Allergy Immunol. 2010;21(7):1028-1035. DOI: 10.1111/j.1399-3038.2010.01030.x
Solé D, Mallol J, Wandalsen GF, Aguirre V, Latin American ISAAC Phase 3 Study Group. Prevalence of symptoms of eczema in Latin America: results of the International Study of Asthma and Allergies in Childhood (ISAAC) Phase 3. J Investig Allergol Clin Immunol. 2010;20(4):311-323. Available at: http://www.jiaci.org/issues/vol20issue4/6.pdf
Barnetson RS, Rogers M. Childhood atopic eczema. BMJ. 2002;324(7350):1376-1379. DOI: 10.1136/bmj.324.7350.1376
Gustafsson D, Sjöberg O, Foucard T. Development of allergies and asthma in infants and young children with atopic dermatitis: a prospective follow-up to 7 years of age. Allergy. 2000;55(3):240-245. DOI: 10.1034/j.1398-9995.2000.00391.x
Kemp AS. Cost of illness of atopic dermatitis in children: a societal perspective. Pharmacoeconomics. 2003;21(2):105-113. DOI: 10.2165/00019053-200321020-00003
Lapidus CS, Schwarz DF, Honig PJ. Atopic dermatitis in children: who cares? Who pays? J Am Acad Dermatol. 1993;28(5 Pt 1):699-703.
Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact Questionnaire. Br J Dermatol. 1998;138(1):107-113. DOI: 10.1046/j.1365-2133.1998.02034.x
Adamson AS. The economics burden of atopic dermatitis. Adv Exp Med Biol. 2017;1027:79-92. DOI: 10.1007/978-3-319-64804-0_8
Wollenberg A, Barbarot S, Bieber T, Christen-Zaech S, Deleuran M, Fink-Wagner A, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5):657-682. DOI: 10.1111/jdv.14891
Wollenberg A, Barbarot S, Bieber T, Christen-Zaech S, Deleuran M, Fink-Wagner A, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. J Eur Acad Dermatol Venereol. 2018;32(6):850-878. DOI: 10.1111/jdv.14888
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-926. DOI: 10.1136/bmj.39489.470347.AD
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383-394. DOI: 10.1016/j.jclinepi.2010.04.026
Davies E, Rogers NK, Lloyd-Lavery A, Grindlay DJC, Thomas KS. What’s new in atopic eczema? An analysis of systematic reviews published in 2015. Part 1: epidemiology and methodology. Clin Exp Dermatol. 2018;43(4):375-379. DOI: 10.1111/ced.13377
Johansson SG, Bieber T, Dahl R, Friedmann PS, Lanier BQ, Lockey RF, et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Allergy Clin Immunol. 2004;113(5):832-826. DOI: 10.1016/j.jaci.2003.12.591
Schäfer T, Krämer U, Vieluf D, Abeck D, Behrendt H, Ring J. The excess of atopic eczema in East Germany is related to the intrinsic type. Br J Dermatol. 2000;143(5):992-998. DOI: 10.1046/j.1365-2133.2000.03832.x
Böhme M, Wickman M, Lennart-Nordvall S, Svartengren M, Wahlgren CF. Family history and risk of atopic dermatitis in children up to 4 years. Clin Exp Allergy. 2003;33(9):1226-1231. DOI: 10.1046/j.1365-2222.2003.01749.x
Schmid-Grendelmeier P, Flückiger S, Disch R, Trautmann A, Wüthrich B, Blaser K, et al. IgE-mediated and T cell-mediated autoimmunity against manganese superoxide dismutase in atopic dermatitis. J Allergy Clin Immunol. 2005;115(5):1068-1075. DOI: 10.1016/j.jaci.2005.01.065
Sánchez J, Páez B, Macías A, Olmos C, de Falco A. Atopic dermatitis guideline. Position paper from the Latin American Society of Allergy, Asthma and Immunology. Rev Alerg Mex. 2014;61(3):178-211.
Mizrahi M. Arguments from expert opinion and persists bias. Argumentation. 2018;32(2):175-95. DOI: 10.1007/s10503-017-9434-x
Brożek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140(4):950-958. DOI: 10.1016/j.jaci.2017.03.050
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015; 350: g7647. DOI: 10.1136/bmj.g7647
Okoli C, Pawlowski SD. The Delphi method as a research tool: an example, design considerations and applications. 2004;42(1):15-29. DOI: 10.1016/j.im.2003.11.002
Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. DOI: 10.1016/j.jclinepi.2010.07.015
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: clinical practice guidelines. BMJ. 2016;353:i2089. DOI: 10.1136/bmj.i2089
Schünemann HJ, Mustafa R, Brozek J, Santesso N, Alonso-Coello P, Guyatt G, et al. GRADE Guidelines: 16. GRADE evidence to decision frameworks for tests in clinical practice and public health. J Clin Epidemiol. 2016;76:89-98. DOI: 10.1016/j.jclinepi.2016.01.032
Thijs JL, Strickland I, Bruijnzeel-Koomen CAFM, Nierkens S, Giovannone B, Csomor E, et al. Moving toward endotypes in atopic dermatitis: identification of patient clusters based on serum biomarker analysis. J Allergy Clin Immunol. 2017;140(3):730-737. DOI: 10.1016/j.jaci.2017.03.023
Muraro A, Lemanske RF, Hellings PW, Akdis CA, Bieber T, Casale TB, et al. Precision medicine in patients with allergic diseases: airway diseases and atopic dermatitis-PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2016;137(5):1347-1358. DOI: 10.1016/j.jaci.2016.03.010
Orivuori L, Mustonen K, Roduit C, Braun-Fahrländer C, Dalphin JC, Genuneit J, et al. Immunoglobulin A and immunoglobulin G antibodies against β-lactoglobulin and gliadin at age 1 associate with immunoglobulin E sensitization at age 6. Pediatr Allergy Immunol. 2014;25(4):329-337. DOI: 10.1111/pai.12246
von Berg A, Filipiak-Pittroff B, Schulz H, Hoffmann U, Link E, Sußmann M, et al. Allergic manifestation 15 years after early intervention with hydrolyzed formulas-the GINI Study. Allergy. 2016;71(2):210-219. DOI: 10.1111/all.12790
Simpson EL, Chalmers JR, Hanifin JM, Thomas KS, Cork MJ, McLean WH, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol. 2014;134(4):818-823. DOI: 10.1016/j.jaci.2014.08.005
Horimukai K, Morita K, Narita M, Kondo M, Kitazawa H, Nozaki M, et al. Application of moisturizer to neonates prevents development of atopic dermatitis. J Allergy Clin Immunol. 2014;134(4):824-830. DOI: 10.1016/j.jaci.2014.07.060
Chalmers JR, Haines RH, Mitchell EJ, Thomas KS, Brown SJ, Ridd M, et al. Effectiveness and cost-effectiveness of daily all-over-body application of emollient during the first year of life for preventing atopic eczema in high-risk children (The BEEP trial): protocol for a randomised controlled trial. Trials. 2017;18(1):343. DOI: 10.1186/s13063-017-2031-3
Tiplica GS, Kaszuba A, Malinauskienė L, Konno P, Boralevi F, Garrigue E, et al. Prevention of flares in children with atopic dermatitis with regular use of an emollient containing glycerol and paraffin: a randomized controlled study. Pediatr Dermatol. 2017;34(3):282-289. DOI: 10.1111/pde.13113
Åkerström U, Reitamo S, Langeland T, Berg M, Rustad L, Korhonen L, et al. Comparison of moisturizing creams for the prevention of atopic dermatitis relapse: a randomized double-blind controlled multicentre clinical trial. Acta Derm Venereol. 2015;95(5):587-592. DOI: 10.2340/00015555-2051
Fukuie T, Hirakawa S, Narita M, Nomura I, Matsumoto K, Tokura Y, et al. Potential preventive effects of proactive therapy on sensitization in moderate to severe childhood atopic dermatitis: a randomized, investigator-blinded, controlled study. J Dermatol. 2016;43(11):1283-1292. DOI: 10.1111/1346-8138.13408
Muehleisen B, Gallo RL. Vitamin D in allergic disease: shedding light on a complex problem. J Allergy Clin Immunol. 2013;131(2):324-329. DOI: 10.1016/j.jaci.2012.12.1562
Camargo CA, Ganmaa D, Sidbury R, Erdenedelger K, Radnaakhand N, Khandsuren B. Randomized trial of vitamin D supplementation for winter-related atopic dermatitis in children. J Allergy Clin Immunol. 2014;134(4):831-835. DOI: 10.1016/j.jaci.2014.08.002
Sidbury R, Sullivan AF, Thadhani RI, Camargo CA. Randomized controlled trial of vitamin D supplementation for winter-related atopic dermatitis in Boston: a pilot study. Br J Dermatol. 2008;159(1):245-247. DOI: 10.1111/j.1365-2133.2008.08601.x
Sánchez J, Sánchez A, Cardona R. Particular characteristics of atopic eczema in tropical environments. The Tropical Environment Control for Chronic Eczema and Molecular Assessment (TECCEMA) cohort study. An Bras Dermatol. 2017;92(2):177-183. DOI: 10.1590/abd1806-4841.20175140
Solman L, Lloyd-Lavery A, Grindlay DJC, Rogers NK, Thomas KS, Harman KE. What’s new in atopic eczema? An analysis of systematic reviews published in 2016. Part 1: treatment and prevention. Clin Exp Dermatol. 2019;44(4):363-369. DOI: 10.1111/ced.13885
Kim JP, Chao LX, Simpson EL, Silverberg JI. Persistence of atopic dermatitis (AD): a systematic review and meta-analysis. J Am Acad Dermatol. 2016;75(4):681-687. DOI: 10.1016/j.jaad.2016.05.028
Thorsteinsdottir S, Stokholm J, Thyssen JP, Nørgaard S, Thorsen J, Chawes BL, et al. Genetic, clinical, and environmental factors associated with persistent atopic dermatitis in childhood. JAMA Dermatol. 2018;155(1):50-57. DOI: 10.1001/jamadermatol.2018.4061
Pajno GB, Peroni DG, Barberio G, Pietrobelli A, Boner AL. Predictive features for persistence of atopic dermatitis in children. Pediatr Allergy Immunol. 2003;14(4):292-295. DOI: 10.1034/j.1399-3038.2003.00060.x
Guo MM, Tseng WN, Ou CY, Hsu TY, Kuo HC, Yang KD. Predictive factors of persistent infantile atopic dermatitis up to 6 years old in Taiwan: a prospective birth cohort study. Allergy. 2015;70(11):1477-1484. DOI: 10.1111/all.12706
Domínguez-Bello MG, Costello EK, Contreras M, Magris M, Hidalgo G, Fierer N, et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci U S A. 2010;107(26):11971-11975. DOI: 10.1073/pnas.1002601107
Park YJ, Lee HK. The role of skin and orogenital microbiota in protective immunity and chronic immune-mediated inflammatory disease. Front Immunol. 2017;8:1955. DOI: 10.3389/fimmu.2017.01955
Baldwin HE, Bhatia ND, Friedman A, Eng RM, Seite S. The Role of cutaneous microbiota harmony in maintaining a functional skin barrier. J Drugs Dermatol. 2017;16(1):12-18. DOI: 10.25251/skin.1.supp.138
Nakatsuji T, Chen TH, Narala S, Chun KA, Two AM, Yun T, et al. Antimicrobials from human skin commensal bacteria protect against. Sci Transl Med. 2017;9(378). DOI: 10.1126/scitranslmed.aah4680
Di Domenico EG, Cavallo I, Bordignon V, Prignano G, Sperduti I, Gurtner A, et al. Inflammatory cytokines and biofilm production sustain Staphylococcus aureus outgrowth and persistence: a pivotal interplay in the pathogenesis of atopic dermatitis. Sci Rep. 2018;8(1):9573. DOI: 10.1038/s41598-018-27421-1
Jinnestål CL, Belfrage E, Bäck O, Schmidtchen A, Sonesson A. Skin barrier impairment correlates with cutaneous Staphylococcus aureus colonization and sensitization to skin-associated microbial antigens in adult patients with atopic dermatitis. Int J Dermatol. 2014;53(1):27-33. DOI: 10.1111/ijd.12198
Cavalcante FS, Abad ED, Lyra YC, Saintive SB, Ribeiro M, Ferreira DC, et al. High prevalence of methicillin resistance and PVL genes among Staphylococcus aureus isolates from the nares and skin lesions of pediatric patients with atopic dermatitis. Braz J Med Biol Res. 2015;48(7):588-594. DOI: 10.1590/1414-431X20154221
Birnie AJ, Bath-Hextall FJ, Ravenscroft JC, Williams HC. Interventions to reduce Staphylococcus aureus in the management of atopic eczema. Cochrane Database Syst Rev. 2008(3):CD003871. DOI: 10.1002/14651858.CD003871.pub3
Yeşilova Y, Çalka Ö, Akdeniz N, Berktaş M. Effect of probiotics on the treatment of children with atopic dermatitis. Ann Dermatol. 2012;24(2):189-193. DOI: 10.5021/ad.2012.24.2.189
Fiocchi A, Pawankar R, Cuello-Garcia C, Ahn K, Al-Hammadi S, Agarwal A, et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics. World Allergy Organ J. 2015;8(1):4. DOI: 10.1186/s40413-015-0055-2
Niccoli AA, Artesi AL, Candio F, Ceccarelli S, Cozzali R, Ferraro L, et al. Preliminary results on clinical effects of probiotic Lactobacillus salivarius LS01 in children affected by atopic dermatitis. J Clin Gastroenterol. 2014;48(Suppl 1):S34-S36. DOI: 10.1097/MCG.0000000000000233
Huang R, Ning H, Shen M, Li J, Zhang J, Chen X. Probiotics for the treatment of atopic dermatitis in children: a systematic review and meta-analysis of randomized controlled trials. Front Cell Infect Microbiol. 2017;7:392. DOI: 10.3389/fcimb.2017.00392
Wickens K, Barthow C, Mitchell EA, Stanley TV, Purdie G, Rowden J, et al. Maternal supplementation alone with Lactobacillus rhamnosus HN001 during pregnancy and breastfeeding does not reduce infant eczema. Pediatr Allergy Immunol. 2018;29(3):296-302. DOI: 10.1111/pai.12874
Boyle RJ, Bath-Hextall FJ, Leonardi-Bee J, Murrell DF, Tang ML. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008(4):CD006135. DOI: 10.1002/14651858.CD006135.pub3
Yang HJ, Min TK, Lee HW, Pyun BY. Efficacy of probiotic therapy on atopic dermatitis in children: a randomized, double-blind, placebo-controlled trial. Allergy Asthma Immunol Res. 2014;6(3):208-215. DOI: 10.4168/aair.2014.6.3.208
Sánchez J, Sánchez A. Epidemiology of food allergy in Latin America. Allergol Immunopathol (Madr). 2015;43(2):185-195. DOI: 10.1016/j.aller.2013.07.001
Sánchez J, Sánchez A. Epidemiologic studies about food allergy and food sensitization in tropical countries. Results and limitations. Allergol Immunopathol (Madr). 2019;47(4):401-408. DOI: 10.1016/j.aller.2018.11.001
Estrada-Reyes E, Pardo-Castañeda MG, Toledo-Bahena ME, Lerma-Ortiz ML, Del Río-Navarro B, Nava-Ocampo AA. A case-control study of food hyper-sensitivity, timing of weaning and family history of allergies in young children with atopic dermatitis. Allergol Immunopathol (Madr). 2007;35(3):101-104. DOI: 10.1157/13106777
Jøhnke H, Norberg LA, Vach W, Høst A, Andersen KE. Patterns of sensitization in infants and its relation to atopic dermatitis. Pediatr Allergy Immunol. 2006;17(8):591-600. DOI: 10.1111/j.1399-3038.2006.00453.x
Roerdink EM, Flokstra-de Blok BM, Blok JL, Schuttelaar ML, Niggemann B, Werfel T, et al. Association of food allergy and atopic dermatitis exacerbations. Ann Allergy Asthma Immunol. 2016;116(4):334-338. DOI: 10.1016/j.anai.2016.01.022
Rennick GJ, Moore E, Orchard DC. Skin prick testing to food allergens in breast-fed young infants with moderate to severe atopic dermatitis. Australas J Dermatol. 2006;47(1):41-45. DOI: 10.1111/j.1440-0960.2006.00221.x
Levy SA, Dortas Junior SD, Pires AH, Abe AT, Valle SO, Coelho VP, et al. Atopy patch test (APT) in the diagnosis of food allergy in children with atopic dermatitis. An Bras Dermatol. 2012;87(5):724-728. DOI: 10.1590/s0365-05962012000500009
David TJ. Anaphylactic shock during elimination diets for severe atopic eczema. Arch Dis Child. 1984;59(10):983-986. DOI: 10.1136/adc.59.10.983
Barbi E, Gerarduzzi T, Longo G, Ventura A. Fatal allergy as a possible consequence of long-term elimination diet. Allergy. 2004;59(6):668-669. DOI: 10.1111/j.1398-9995.2004.00398.x
Flinterman AE, Knulst AC, Meijer Y, Bruijnzeel-Koomen CA, Pasmans SG. Acute allergic reactions in children with AEDS after prolonged cow’s milk elimination diets. Allergy. 2006;61(3):370-374. DOI: 10.1111/j.1398-9995.2006.01018.x
Chang A, Robison R, Cai M, Singh AM. Natural history of food-triggered atopic dermatitis and development of immediate reactions in children. J Allergy Clin Immunol Pract. 2016;4(2):229-236. DOI: 10.1016/j.jaip.2015.08.006
Fleischer DM, Bock SA, Spears GC, Wilson CG, Miyazawa NK, Gleason MC, et al. Oral food challenges in children with a diagnosis of food allergy. J Pediatr. 2011;158(4):578-583. DOI: 10.1016/j.jpeds.2010.09.027
Eapen AA, Kloepfer KM, Leickly FE, Slaven JE, Vitalpur G. Oral food challenge failures among foods restricted because of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;122(2):193-197. DOI: 10.1016/j.anai.2018.10.012
Santer M, Rumsby K, Ridd MJ, Francis NA, Stuart B, Chorozoglou M, et al. Adding emollient bath additives to standard eczema management for children with eczema: the BATHE RCT. Health Technol Assess. 2018;22(57):1-116.
Antonijević MD, Novac O, O’Hagan BM. Can emollients of similar composition be assumed to be therapeutically equivalent: a comparison of skin occlusivity and emulsion microstructure. Clin Cosmet Investig Dermatol. 2018;11:461-465. DOI: 10.2147/CCID.S176943
Jung HJ, Bae JY, Kim JE, Na CH, Park GH, Bae YI, et al. Survey of disease awareness, treatment behavior and treatment satisfaction in patients with atopic dermatitis in Korea: a multicenter study. J Dermatol. 2018;45(10):1172-1180. DOI: 10.1111/1346-8138.14540
Sala-Cunill A, Lazaro M, Herráez L, Quiñones MD, Moro-Moro M, Sánchez I, et al. Basic skin care and topical therapies for atopic dermatitis: essential approaches and beyond. J Investig Allergol Clin Immunol. 2018;28(6):379-391. DOI: 10.18176/jiaci.0293
Eriksson S, van der Plas MJA, Mörgelin M, Sonesson A. Antibacterial and antibiofilm effects of sodium hypochlorite against Staphylococcus aureus isolates derived from patients with atopic dermatitis. Br J Dermatol. 2017;177(2):513-521. DOI: 10.1111/bjd.15410
Harris V, Smith SD. Lifting the biofilm lid on the antibacterial and antibiofilm effects of sodium hypochlorite against Staphylococcus aureus in atopic dermatitis. Br J Dermatol. 2017;177(2):347-348. DOI: 10.1111/bjd.15692
Asch S, Vork DL, Joseph J, Major-Elechi B, Tollefson MM. Comparison of bleach, acetic acid, and other topical anti-infective treatments in pediatric atopic dermatitis: a retrospective cohort study on antibiotic exposure. Pediatr Dermatol. 2019;36(1):115-120. DOI: 10.1111/pde.13663
Church MK, Maurer M. H1-antihistamines and itch in atopic dermatitis. Exp Dermatol. 2015;24(5):332-333.
Ohsawa Y, Hirasawa N. The role of histamine H1 and H4 receptors in atopic dermatitis: from basic research to clinical study. Allergol Int. 2014;63(4):533-542. DOI: 10.2332/allergolint.13-RA-0675
Munday J, Bloomfield R, Goldman M, Robey H, Kitowska GJ, Gwiezdziski Z, et al. Chlorpheniramine is no more effective than placebo in relieving the symptoms of childhood atopic dermatitis with a nocturnal itching and scratching component. Dermatology. 2002;205(1):40-45. DOI: 10.1159/000063138
Wahlgren CF, Hägermark O, Bergström R. The antipruritic effect of a sedative and a non-sedative antihistamine in atopic dermatitis. Br J Dermatol . 1990;122(4):545-551. DOI: 10.1111/j.1365-2133.1990.tb14732.x
Frosch PJ, Schwanitz HJ, Macher E. A double blind trial of H1 and H2 receptor antagonists in the treatment of atopic dermatitis. Arch Dermatol Res. 1984;276(1):36-40. DOI: 10.1007/bf00412560
Savin JA, Dow R, Harlow BJ, Massey H, Yee KF. The effect of a new non-sedative H1-receptor antagonist (LN2974) on the itching and scratching of patients with atopic eczema. Clin Exp Dermatol . 1986;11(6):600-602. DOI: 10.1111/j.1365-2230.1986.tb00515.x
Hannuksela M, Kalimo K, Lammintausta K, Mattila T, Turjanmaa K, Varjonen E, et al. Dose ranging study: cetirizine in the treatment of atopic dermatitis in adults. Ann Allergy. 1993;70(2):127-133.
Langeland T, Fagertun HE, Larsen S. Therapeutic effect of loratadine on pruritus in patients with atopic dermatitis. A multi-crossover-designed study. Allergy. 1994;49(1):22-26. DOI: 10.1111/j.1398-9995.1994.tb00768.x
La Rosa M, Ranno C, Musarra I, Guglielmo F, Corrias A, Bellanti JA. Double-blind study of cetirizine in atopic eczema in children. Ann Allergy . 1994;73(2):117-122.
Yamanaka K, Motomura E, Noro Y, Umeda K, Morikawa T, Umeda-Togami K, et al. Olopatadine, a non-sedating H1 antihistamine, decreases the nocturnal scratching without affecting sleep quality in atopic dermatitis. Exp Dermatol . 2015;24(3):227-229. DOI: 10.1111/exd.12630
Kawashima M, Tango T, Noguchi T, Inagi M, Nakagawa H, Harada S. Addition of fexofenadine to a topical corticosteroid reduces the pruritus associated with atopic dermatitis in a 1-week randomized, multicentre, double-blind, placebo-controlled, parallel-group study. Br J Dermatol . 2003;148(6):1212-1221. DOI: 10.1046/j.1365-2133.2003.05293.x
Church MK, Maurer M, Simons FE, Bindslev-Jensen C, van Cauwenberge P, Bousquet J, et al. Risk of first-generation H(1)-antihistamines: a GA(2)LEN position paper. Allergy . 2010;65(4):459-466. DOI: 10.1111/j.1398-9995.2009.02325.x
Hamilton JD, Suárez-Fariñas M, Dhingra N, Cardinale I, Li X, Kostic A, et al. Dupilumab improves the molecular signature in skin of patients with moderate-to-severe atopic dermatitis. J Allergy Clin Immunol. 2014;134(6):1293-1300. DOI: 10.1016/j.jaci.2014.10.013
Beck LA, Thaçi D, Hamilton JD, Graham NM, Bieber T, Rocklin R, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Engl J Med. 2014;371(2):130-139. DOI: 10.1056/NEJMoa1314768
Silverberg JI, Simpson EL, Ardeleanu M, Thaçi D, Barbarot S, Bagel J, et al. Dupilumab provides important clinical benefits to patients with atopic dermatitis who do not achieve clear or almost clear skin according to the Investigator’s Global Assessment: a pooled analysis of data from 2 phase III trials. Br J Dermatol . 2019;181(1):80-87. DOI: 10.1111/bjd.17791
Storan ER, Woolf RT, Smith CH, Pink AE. Clearance of molluscum contagiosum virus infection in patients with atopic eczema treated with dupilumab. Br J Dermatol . 2019;181(2):385-386. DOI: 10.1111/bjd.17712
Blauvelt A, Rosmarin D, Bieber T, Simpson EL, Bagel J, Worm M, et al. Improvement of atopic dermatitis with dupilumab occurs equally well across different anatomic regions: data from phase 3 clinical trials. Br J Dermatol . 2019;181(1):196-197. DOI: 10.1111/bjd.17703
Tintle S, Shemer A, Suárez-Fariñas M, Fujita H, Gilleaudeau P, Sullivan-Whalen M, et al. Reversal of atopic dermatitis with narrow-band UVB phototherapy and biomarkers for therapeutic response. J Allergy Clin Immunol. 2011;128(3):583-593. DOI: 10.1016/j.jaci.2011.05.042
Clayton TH, Clark SM, Turner D, Goulden V. The treatment of severe atopic dermatitis in childhood with narrowband ultraviolet B phototherapy. ClinExp Dermatol . 2007;32(1):28-33. DOI: 10.1111/j.1365-2230.2006.02292.x
Meduri NB, Vandergriff T, Rasmussen H, Jacobe H. Phototherapy in the management of atopic dermatitis: a systematic review. Photodermatol Photoimmunol Photomed. 2007;23(4):106-112. DOI: 10.1111/j.1600-0781.2007.00291.x
Brownell J, Wang S, Tsoukas MM. Compliance and phototherapy. Clin Dermatol. 2016;34(5):582-586. DOI: 10.1016/j.clindermatol.2016.05.007
Cline A, Unrue EL, Collins A, Feldman SR. Adherence to a novel home phototherapy system with integrated features. Dermatol Online J. 2019;25(3). Available at: https://www.clarifymed.com/wp-content/uploads/DOJ-Adherence-Publication-March-2019.pdf
Drucker AM, Eyerich K, de Bruin-Weller MS, Thyssen JP, Spuls PI, Irvine AD, et al. Use of systemic corticosteroids for atopic dermatitis: International Eczema Council consensus statement. Br J Dermatol . 2018;178(3):768-775. DOI: 10.1111/bjd.15928
Roekevisch E, Spuls PI, Kuester D, Limpens J, Schmitt J. Efficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: a systematic review. J Allergy Clin Immunol. 2014;133(2):429-438. DOI: 10.1016/j.jaci.2013.07.049
Yu SH, Drucker AM, Lebwohl M, Silverberg JI. A systematic review of the safety and efficacy of systemic corticosteroids in atopic dermatitis. J Am Acad Dermatol. 2018;78(4):733-740. DOI: 10.1016/j.jaad.2017.09.074
Berth-Jones J, Takwale A, Tan E, Barclay G, Agarwal S, Ahmed I, et al. Azathioprine in severe adult atopic dermatitis: a double-blind, placebo-controlled, crossover trial. Br J Dermatol . 2002;147(2):324-330. DOI: 10.1046/j.1365-2133.2002.04989.x
Berth-Jones J, Graham-Brown RA, Marks R, Camp RD, English JS, Freeman K, et al. Long-term efficacy and safety of cyclosporin in severe adult atopic dermatitis. Br J Dermatol . 1997;136(1):76-81. DOI: 10.1046/j.1365-2133.1997.d01-1146.x
Salek MS, Finlay AY, Luscombe DK, Allen BR, Berth-Jones J, Camp RD, et al. Cyclosporin greatly improves the quality of life of adults with severe atopic dermatitis. A randomized, double-blind, placebo-controlled trial. Br J Dermatol . 1993;129(4):422-430. DOI: 10.1111/j.1365-2133.1993.tb03170.x
van Joost T, Heule F, Korstanje M, van den Broek MJ, Stenveld HJ, van Vloten WA. Cyclosporin in atopic dermatitis: a multicentre placebo-controlled study. Br J Dermatol . 1994;130(5):634-640. DOI: 10.1111/j.1365-2133.1994.tb13111.x
Sowden JM, Berth-Jones J, Ross JS, Motley RJ, Marks R, Finlay AY, et al. Double-blind, controlled, crossover study of cyclosporin in adults with severe refractory atopic dermatitis. Lancet. 1991;338(8760):137-140. DOI: 10.1016/0140-6736(91)90134-b
Haeck IM, Knol MJ, Ten Berge O, van Velsen SG, de Bruin-Weller MS, Bruijnzeel-Koomen CA. Enteric-coated mycophenolate sodium versus cyclosporin A as long-term treatment in adult patients with severe atopic dermatitis: a randomized controlled trial. J Am Acad Dermatol. 2011;64(6):1074-84. DOI: 10.1016/j.jaad.2010.04.027
Koppelhus U, Poulsen J, Grunnet N, Deleuran MS, Obitz E. Cyclosporine and extracorporeal photopheresis are equipotent in treating severe atopic dermatitis: a randomized cross-over study comparing two efficient treatment modalities. Front Med (Lausanne). 2014;1:33. DOI: 10.3389/fmed.2014.00033
Zonneveld IM, De Rie MA, Beljaards RC, Van Der Rhee HJ, Wuite J, Zeegelaar J, et al. The long-term safety and efficacy of cyclosporin in severe refractory atopic dermatitis: a comparison of two dosage regimens. Br J Dermatol . 1996;135(Suppl 48):15-20. DOI: 10.1111/j.1365-2133.1996.tb00704.x
Granlund H, Erkko P, Remitz A, Langeland T, Helsing P, Nuutinen M, et al. Comparison of cyclosporin and UVAB phototherapy for intermittent one-year treatment of atopic dermatitis. Acta Derm Venereol. 2001;81(1):22-27. DOI: 10.1080/00015550120235
Harper JI, Ahmed I, Barclay G, Lacour M, Hoeger P, Cork MJ, et al. Cyclosporin for severe childhood atopic dermatitis: short course versus continuous therapy. Br J Dermatol . 2000;142(1):52-58. DOI: 10.1046/j.1365-2133.2000.03241.x
Czech W, Bräutigam M, Weidinger G, Schöpf E. A body-weight-independent dosing regimen of cyclosporine microemulsion is effective in severe atopic dermatitis and improves the quality of life. J Am Acad Dermatol. 2000;42(4):653-659. DOI: 10.1067/mjd.2000.103815
Bunikowski R, Gerhold K, Bräutigam M, Hamelmann E, Renz H, Wahn U. Effect of low-dose cyclosporin a microemulsion on disease severity, IL-6, IL-8 and tumor necrosis factor alpha production in severe pediatric atopic dermatitis. Int Arch Allergy Immunol. 2001;125(4):344-348. DOI: 10.1159/000053836
Bunikowski R, Staab D, Kussebi F, Bräutigam M, Weidinger G, Renz H, et al. Low-dose cyclosporin A microemulsion in children with severe atopic dermatitis: clinical and immunological effects. Pediatr Allergy Immunol. 2001;12(4):216-223. DOI: 10.1034/j.1399-3038.2001.012004216.x
Totri CR, Eichenfield LF, Logan K, Proudfoot L, Schmitt J, Lara-Corrales I, et al. Prescribing practices for systemic agents in the treatment of severe pediatric atopic dermatitis in the US and Canada: the PeDRA TREAT survey. J Am Acad Dermatol. 2017;76(2):281-285. DOI: 10.1016/j.jaad.2016.09.021
Weatherhead SC, Wahie S, Reynolds NJ, Meggitt SJ. An open-label, dose-ranging study of methotrexate for moderate-to-severe adult atopic eczema. Br J Dermatol . 2007;156(2):346-351. DOI: 10.1111/j.1365-2133.2006.07686.x
Goujon C, Viguier M, Staumont-Sallé D, Bernier C, Guillet G, Lahfa M, et al. Methotrexate versus cyclosporine in adults with moderate-to-severe atopic dermatitis: a phase III randomized noninferiority trial. J Allergy Clin Immunol Pract. 2018;6(2):562-569. DOI: 10.1016/j.jaip.2017.07.007
Law Ping Man S, Bouzillé G, Beneton N, Safa G, Dupuy A, Droitcourt C. Drug survival and postdrug survival of first-line immunosuppressive treatments for atopic dermatitis: comparison between methotrexate and cyclosporine. J Eur Acad Dermatol Venereol. 2018;32(8):1327-1335. DOI: 10.1111/jdv.14880
El-Khalawany MA, Hassan H, Shaaban D, Ghonaim N, Eassa B. Methotrexate versus cyclosporine in the treatment of severe atopic dermatitis in children: a multicenter experience from Egypt. Eur J Pediatr. 2013;172(3):351-356. DOI: 10.1007/s00431-012-1893-3
Meggitt SJ, Gray JC, Reynolds NJ. Azathioprine dosed by thiopurine methyltransferase activity for moderate-to-severe atopic eczema: a double-blind, randomised controlled trial. Lancet. 2006;367(9513):839-846. DOI: 10.1016/S0140-6736(06)68340-2
Schram ME, Roekevisch E, Leeflang MM, Bos JD, Schmitt J, Spuls PI. A randomized trial of methotrexate versus azathioprine for severe atopic eczema. J Allergy Clin Immunol. 2011;128(2):353-359. DOI: 10.1016/j.jaci.2011.03.024
Ballester I, Silvestre JF, Pérez-Crespo M, Lucas A. Severe adult atopic dermatitis: treatment with mycophenolate mofetil in 8 patients. Actas Dermosifiliogr. 2009;100(10):883-887. DOI: 10.1016/S1578-2190(09)70559-1
Fallah Arani S, Waalboer-Spuij R, Nijsten T, Neumann HA, Thio B. Enteric-coated mycophenolate sodium in psoriasis vulgaris: an open pilot study. J Dermatolog Treat. 2014;25(1):46-49. DOI: 10.3109/09546634.2012.723124
Grundmann-Kollmann M, Podda M, Ochsendorf F, Boehncke WH, Kaufmann R, Zollner TM. Mycophenolate mofetil is effective in the treatment of atopic dermatitis. Arch Dermatol. 2001;137(7):870-873. DOI: 10-1001/pubs.Arch Dermatol.-ISSN-0003-987x-137-7-dst10044
Murray ML, Cohen JB. Mycophenolate mofetil therapy for moderate to severe atopic dermatitis. ClinExp Dermatol. 2007;32(1):23-27. DOI: 10.1111/j.1365-2230.2006.02290.x
Dias-Polak D, Bergman R, Avitan-Hersh E. Mycophenolate mofetil therapy in adult patients with recalcitrant atopic dermatitis. J Dermatolog Treat. 2019;30(1):49-51. DOI: 10.1080/09546634.2018.1468068
Heller M, Shin HT, Orlow SJ, Schaffer JV. Mycophenolate mofetil for severe childhood atopic dermatitis: experience in 14 patients. Br J Dermatol . 2007;157(1):127-132. DOI: 10.1111/j.1365-2133.2007.07947.x
Paller AS, Tom WL, Lebwohl MG, Blumenthal RL, Boguniewicz M, Call RS, et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adults. J Am Acad Dermatol. 2016;75(3):494-503. DOI: 10.1016/j.jaad.2016.05.046
Draelos ZD, Stein Gold LF, Murrell DF, Hughes MH, Zane LT. Post hoc analyses of the effect of crisaborole topical ointment, 2% on atopic dermatitis: associated pruritus from phase 1 and 2 clinical studies. J Drugs Dermatol. 2016;15(2):172-176.
Zane LT, Hughes MH, Shakib S. Tolerability of crisaborole ointment for application on sensitive skin areas: a randomized, double-blind, vehicle-controlled study in healthy volunteers. Am J Clin Dermatol. 2016;17(5):519-526. DOI: 10.1007/s40257-016-0204-6
de Bruin-Weller M, Thaçi D, Smith CH, Reich K, Cork MJ, Radin A, et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: a placebo-controlled, randomized phase III clinical trial (LIBERTY AD CAFÉ). Br J Dermatol . 2018;178(5):1083-1101. DOI: 10.1111/bjd.16156
Fukuda K, Ishida W, Kishimoto T, Fukushima A. Development of conjunctivitis with a conjunctival proliferative lesion in a patient treated with dupilumab for atopic dermatitis. Allergol Int . 2019;68(3):383-384. DOI: 10.1016/j.alit.2018.12.012
Glossary
AD: atopic dermatitis
AZA: azathioprine
CSA: cyclosporine A
FDA: Food and Drugs Administration
GRADE: Grading of Recommendations, Assessment, Development, and Evaluation
IL: interleukin
MTX: methotrexate
RCT: randomized controlled trial
SCORAD: Severity Scoring Atopic Dermatitis
SCSs: systemic corticosteroids
SLAAI: Sociedad Latinoamericana de Asma, Alergia e Inmunología
WAO: World Allergy Organization
Supplementary material 1.
Systematic review Check List from the PRISMA statement for the dermatitis-SLAAI guideline review of 10 interventions
Table present, is kindly offered freely for the PRISMA Group (2009) (for more information, visit http://www.prisma-statement.org). We highlight those recommendations that we did not make with red.
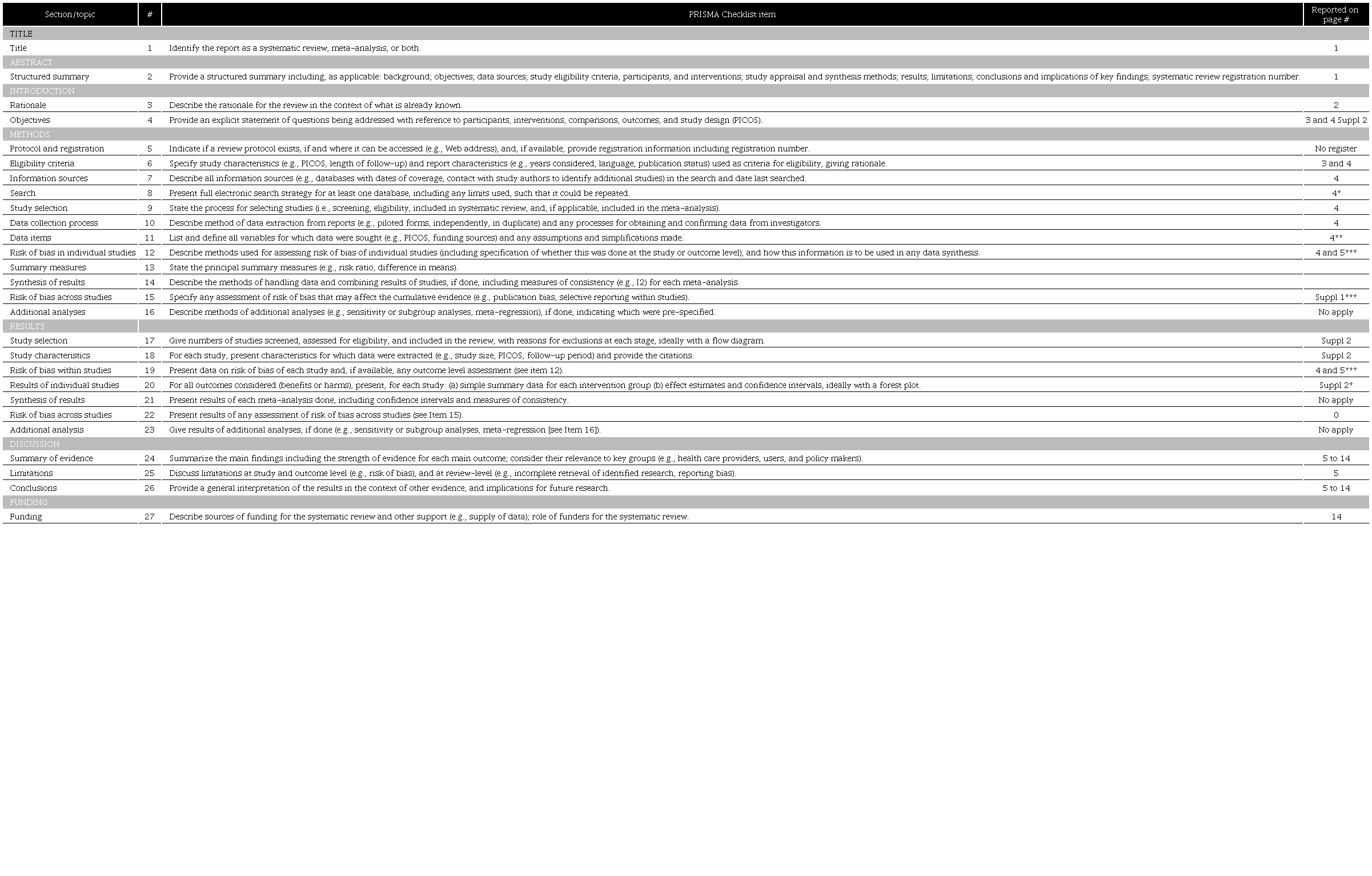
Topic 2 and 5: the protocol for this systematic review was no register in any database. Topic 12, 19, 22: see *** * We summarize the search strategy using the flowchart proposed by PRISMA (see supplemental material 2). Additional information could be asked to the staff by email to the corresponding author. ** In supplement material 2, PICO strategy for each question is presented. *** Lack of information to do the correct analysis of an article (e.g.: no clarity control group or measuring parameter), was identified by the reviewers (two for each question), and this was withdrawn if it did not allow to obtain a specific evaluation, however, a standardized evaluation to avoid risk of bias was not used. When a research group or center presented two or more results of an intervention in the same research, we only considered that which included more patients or had a better design.
Supplementary material 2
PRISMA flow diagram and PIC strategy
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and
Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097. For more information, visit http://www.prisma-statement.org
Notes
Author notes
*Correspondence: Jorge Sánchez. jorgem.sanchez@udea.edu.co