Articles
Hospital rough cut capacity planning in a General Surgery service
Planeación agregada de la capacidad hospitalaria en un servicio de Cirugía General
 Yasniel Sánchez-Suárez yasnielsanchez9707@gmail.com
Maylín Marqués-León maylin.marques@umcc.cu
Arialys Hernández-Nariño arialishn.mtz@infomed.sld.cu
Orlando Santos-Pérez orlando-santos@empai.cu
Yasniel Sánchez-Suárez yasnielsanchez9707@gmail.com
Maylín Marqués-León maylin.marques@umcc.cu
Arialys Hernández-Nariño arialishn.mtz@infomed.sld.cu
Orlando Santos-Pérez orlando-santos@empai.cu
Hospital rough cut capacity planning in a General Surgery service
DYNA, vol. 90, no. 225, pp. 45-54, 2023
Universidad Nacional de Colombia
Received: 12 June 2022
Revised document received: 29 November 2022
Accepted: 14 December 2022
Abstract: Hospital services constitute a fundamental pillar in the development of society. The objective of this article is to provide medium-term capacity planning improvements in a General Surgery service. A procedure was designed for capacity planning based on process analysis and design as well as the patients’ clinical characteristics. Some of the main results were: the demand of the Major Diagnostic Categories was predicted, the rooms were identified as the limiting resource in this kind of service, where an 82.82 % of them were used, the necessary wards reservations were calculated for the year 2021, with a rate of 163, 96 and 59 times for incisional, inguinal and umbilical hernia surgeries respectively, and a system of capacity improvement actions which were projected. The analysis of capacity using the proposed heuristic method makes possible to identify limiting resources, enhance performance and devise strategies to meet the demand.
Keywords: Capacity planning, hospital management, patients flow, General Surgery service.
Resumen: Los servicios hospitalarios constituyen un pilar fundamental en el desarrollo de la sociedad. El objetivo del artículo es proyectar mejoras en la planeación de la capacidad a mediano plazo en un servicio de Cirugía General. Se diseñó un procedimiento para la planeación de la capacidad en función de las características clínicas de los pacientes y basado en el análisis y diseño de procesos. Entre los principales resultados: se pronosticó la demanda de las Categorías Diagnósticas Mayores, se identificó que los salones son el recurso limitante en este servicio, los cuales se aprovecharon un 82.82 %, se calcularon las reservas necesarias de salones para el año 2021, las cuales fueron: 163, 96 y 59 veces en cirugías de hernia incisional, inguinal y umbilical respectivamente y se proyectó un sistema de acciones de mejora de la capacidad. El análisis de la capacidad mediante el método heurístico propuesto permite identificar recursos limitantes, potenciar el desempeño y trazar estrategias en función del cumplimiento de la demanda.
Palabras clave: Planeación de la capacidad, gestión hospitalaria, flujo de pacientes, servicio de Cirugía General.
1. Introduction
Currently, health-related services are regarded as a very important and attractive sector for the application of tools from different managerial areas, with the aim of seeking better results both economically and in terms of patient satisfaction. Among these services, hospital services stand up with a great diversity and presence; in charge of providing specialized care and health restoration, through advanced technology.
For a consistent and clarifying approach to hospital management it is important to understand that a hospital has very complex, diverse and dynamic characteristics [1]. Thus, hospital management should be implemented through policies, systems, components, processes and instruments which, when integrated in a coherent, holistic and cohesive manner, maximize the quality of care and patient satisfaction [2].
The dynamics of those processes require that the professionals in charge of management have updated and proven effective tools that allow them to analyze, program, plan, prioritize and decide on the best way to manage the available resources in order to provide a good service and guarantee an excellent quality assistance to their patients and stakeholders [3].
Process management and improvement is one of the best practices currently recognized in the field of business management [4]. There are many experiences in the improvement of hospital processes. The process approach to hospital management is increasingly applied, a philosophy that shows a holistic approach and pursues hospital excellence with a strategic vision [5], the process representation as a synthesized way to see relationship between activities [6], analysis of patient waiting times [7], level of service provided [8], the planning process [9], such as the uses of case mix measurement systems [10,11] and, within them, the Major Diagnostic Categories (MDC) as a more universal, mutually exclusive patient grouping system, according to affected organs or systems, based on the main diagnosis of the episode [12], the MDC can be disaggregated in more specific ways into the Diagnosis Related Groups (DRGs) as a system for grouping patients into clinically coherent classes with equal resource consumption [13-15], are of vital importance for increasing hospital efficiency [16].
Healthcare also represents a highly relevant field of business, ideal for the application of operations management concepts and tools [17], which seeks to ensure a fast, agile and simple way to address health problems from a vision focused on the process, the capacity, inventory, workforce and quality [15].
Hospital institutions, like any other healthcare organization, need to optimize their results, as any other healthcare organization, to optimize their performance and meet patients' needs [18], thus, managing health-related services involves planning and coordinating various scarce resources (many of which are expensive and highly specialized), as well as taking into consideration multiple and often conflicting stakeholders.
The management of service constraints such as operating wards, healthcare personnel and hospital furnishing such as beds, is emerging as a challenge for healthcare managers [19], on the other hand, achieving high levels of capacity utilization, studying the variability in demand and uncertainty in service times can cause these resources to be unavailable when required or underutilized, are some of the privileges of managing capacity [20].
Hospital capacity services can be measured under different criteria: quality, safety, efficiency or effectiveness [21], from the perspective of operations management is one of the tools that allow determining the quality of resources per unit of time available to meet the demand; which favors:
- 1. The control of limited resources,
- 2. Work organization, and
- 3. Avoiding possible complications generated by inadequate capacity planning.
Duarte Forero and Camacho Oliveros [20] in accordance with Green [22], stated that the analysis of capacity management in hospitals requires approaches that integrate the intrinsic characteristics of their operation (performance as a service, patient flow, resource management), their impact on the output variables and the parameters of improvement policies.
The analysis carried out by the authors of this research, on 17 methodologies aimed at identifying techniques or approaches for calculating capacity revealed that 82.35 % are applied in general and high complexity hospitals, while 17.65 % are applied at the primary level of care.
Among the most commonly applied techniques or approaches for capacity analysis are process simulation applied in 64.7 % of the methodologies from different angles and perspectives, capacity estimation from the point of view of resource allocation [23], focus on the percent of service usage [24,25], in the quality of service, through the use of value maps [26] and distribution of service times [27], based on estimated lengths of stay [28], the material flow [20] and yields [29].
On the other hand, linear programming models have been applied, in a 17.65 % of the procedures consulted, based on the calculation of human resources as a determining factor of capacity [30], or average length of stay.
The following techniques are also used for capacity analysis although to a lesser extent: Management indicators (11.76 %), Demand forecasts (11.76 %), Hypothesis tests based on future capacity analysis (5.88 %), Analysis and information gathering techniques (5.88 %).
Models, methodologies and procedures are designed to answer three questions for capacity decisions: how much capacity is needed, when capacity is needed, and where it should be located. These decisions are fundamentally influenced by the existence of a good balance in the process that takes into account the actual level of the organization in terms of customer demand, the availability of resources and that complies with the existing work standards [8].
The literature recognizes the need for capacity planning in hospital institutions as a tool for improving the quality of services. Most of the research focuses its studies on service simulation in order to predict the behavior of capacity and to foresee an uninterrupted flow during the process through the different stages of treatment: formation of homogeneous groups of patients (case-mix), demand forecasting and simple tabular methods to be used by the medical staff, which among their output information contain decisive capacity indicators.
It is necessary to take into consideration the limiting resources, the characteristics of the system (treatment stage), as well as the planning horizon. The procedure presented here is for medium-term capacity planning, which can be disaggregated for more specific planning by integrating other methods such as simulation and linear programming.
Faustino Pérez Hospital, located in the province of Matanzas, Cuba, presented as the object of study of this research, integrates the secondary level of care and constitutes for some specialties the hospital to which all the municipalities of the province attend. In the fulfillment of its mission and objectives, the specialized personnel carry out various tasks, among which is teaching and research.
For 20 years researchers from the University of Matanzas (including the authors of this research) have reported several studies on hospital organizations, which have been aligned to the hospital improvement program being developed in Cuba and, nowadays, to government management agenda based on science and innovation. The institution's management proposes the need to start with the accreditation reports and find possible actions for improvement in the hospital's processes.
The possibility of improving capacity planning strategies is identified in order to raise patient satisfaction levels and reduce their average length of stay through the management of patient flows focused on their trajectory. For a more detailed analysis, the quality management team suggests consulting other documents that provide information of interest for the effective deployment of the research.
Consequently, the review of documents such as the General Hospital Regulations, Board of Directors, audits´ reports, interviews with managers, specialists and nurses, on-call deliveries, and direct observation, the following were identified as the main shortcomings affecting capacity in the service: inefficient scientific methods for capacity analysis, increase in emergency operations and cancellation of elective ones, high hospital stay, and deficient organization of activities in key processes.
The objective of the article is to project improvements in medium-term capacity planning in a General Surgery service.
2. Methodology
2.1. Procedure for hospital capacity planning
Operations planning has been studied from various perspectives, in this sense Hulshof et al. [11] summarize 5 general methods for decision making in health systems: computational simulation, Markov processes, mathematical programming, queuing theory and heuristic methods. Although heuristic methods do not guarantee an optimal solution, since they require too much time for an exact approach, they allow iterative improvement of problems based on the optimization of a candidate solution.
Methodologies for the development of heuristic methods for capacity planning are shown in the literature, among which the following are quoted:
-
Arnaout [31]: proposes a procedure based on heuristic methods for the optimization of operating rooms through the use of simulation, the iterations performed are based on solving operational problems for the scheduling of the operating room translated into the identification of limiting resources: machines (surgical equipment), time, human resources (surgeon and surgical team) and medical resources. Although it is a procedure that allows the optimization of operating rooms, it does not allow the integration of other limiting resources present in the patient's treatment stages.
-
Orejuela Cabrera et al [32]: proposes a procedure for production scheduling in a workshop environment, where he proposes a procedure for the calculation of capacity in a service company in Colombia; he makes a grouping of product families according to the number of orders, an element that allows him to determine representative products for the calculation of capacity and from this, to determine the limiting capacity or bottleneck, to then schedule operations. It is considered the main theoretical reference for contextualization in hospital services, since it has the following limitations: it restricts the analysis of capacity only to the time limiting resource which, although determinant, in health services there are other resources that limit capacity, such as beds, medical personnel or diagnostic means.
-
Bretthauer and Heese [33] propose a model based on queuing theory for hospital capacity planning based on iteration and creation of probable scenarios that can limit patient flow.
Although the methodologies listed above show a solution to capacity problems from the perspective of recognizing a limiting resource, they do not allow a medium-term capacity programming, nor do they consider the behavior of demand. Based on the analysis of previous methodologies and on the gaps found, the authors of this research propose a procedure for aggregated capacity planning in hospital centers (Fig. 1), consisting of four (4) logically articulated stages.
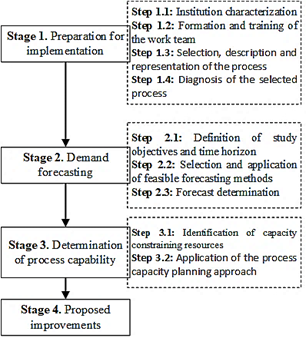
Figure 1
Procedure for hospital capacity planning
Source: Own design.
Stage 1. Preparation for implementation
The stage is structured in four (4) steps related to the conformation and training of the work team for the subsequent selection and representation of the process that serves as support for the diagnosis of the same.
Step 1.1: Institution characterization
As a premise, it is necessary to analyze the characteristics that distinguish the activity of the hospital organization in order to become familiar with it, as well as to identify the main problems that affect the capacity of the process prior to the formation of the work team.
Step 1.2: Formation and training of the work team
A team of seven to nine people, usually members of the Board of Directors and from the different key result areas, should be formed. One of the members should be appointed as project coordinator and a plan of the activities to be carried out should be established. The implementation of a training strategy in key thematic nuclei, such as: operations management, operations planning, hospital capacity planning and hospital casuistry.
Step 1.3: Selection, description and representation of the process
For the selection of the process to be studied, several criteria can be considered: interest of the organization, key process, levels of impact of the process, complaints or dissatisfaction with the process or its final product (patient satisfaction). A support tool for the selection of processes is the General Process Map. Once it has been drawn up, experts’ consultation, interviews, surveys or brainstorming rounds can be carried out to allow an accurate and objective selection.
Another important tool in the description of the process is the flow diagram, among which the As-Is stand out, an useful instrument to represent activities and their sequences as they happen [12].
Step 1.4: Diagnosis of the selected process
The objective of this step is to define the fundamental problems affecting the process and their root causes. For the selection of these problems, tools such as Brainstorming will be used. This group technique allows to generate original ideas in a relaxed atmosphere, to free the creativity of the teams, to generate an extensive number of ideas, to involve everyone in the process, to identify opportunities for improvement, etc. These ideas are then transferred to a cause-effect diagram (fish diagram, Ishikawa diagram).
Stage 2. Demand forecasting
Knowing the demand in health processes is a key element to determine the capacity of a process in this type of facility. Its determination (annual, monthly, daily) according to the needs or characteristics of the process. The purpose of this stage is to determine the demand of the selected process. It is necessary to previously take MDC into count, which define the behavior of the demand of the service according to homogeneous groups of patients.
The proposed procedure for this end takes as a reference the procedures used by [8,34,35] for time series-based demand forecasting service processes. There are MDC whose behavior and frequency can be related to time series, respiratory diseases are an example of this when analyzing how in winter the emergencies and admissions for this cause increase [36], on the other hand some obstetrics behaviors; for example, births seem to increase nine months after carnival and vacation periods [12], in emergency departments using historical data [37], in the case of surgical department MDCs, it is presented as a variable spaced in time that has a trend, seasonality and cycles characterized by the quality of life and comorbidities associated with the main reason for surgery.
Step 2.1: Definition of study objectives and time horizon
When defining the objectives of the study, the following aspects, among others, should be considered: What is the purpose of the study? Here the time horizon of the study is defined, whether the forecast is long, medium or short term, as well as the duration of the components of the historical series, elements that influence the selection of methods and the cost-benefit assessment.
Step 2.2: Selection and application of feasible forecasting methods
Nowadays, making decisions about feasible forecasting methods is becoming easier due to the variety of software designed for service demand planning, among them: WINQSB, ForePlanner, Statgraphics Centurion XV and IBM SPSS Statistics. IBM SPSS Statistics 22 will be used in the research because it is a professional software and has the advantage of an expert modeler, used to solve a wide variety of business and research problems.
Step 2.3: Forecast determination
Once a determined forecast is obtained, it is necessary to incorporate the subjective criteria of the specialists conducting the study and those experts on whom they rely, which allow rounding off the given forecast according to their experiences. In support of the activity, the forecast questionnaire is designed, as shown in Table 1.
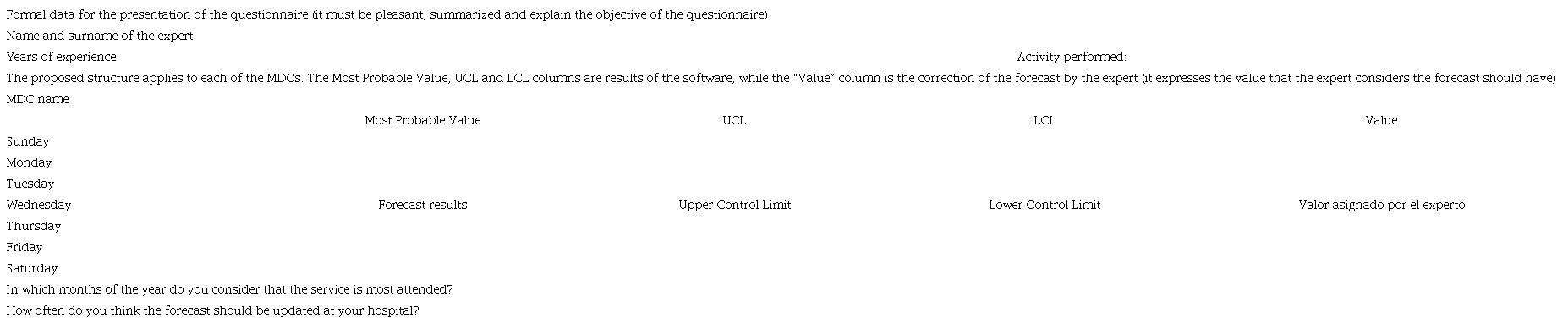
Source: Own design.
Stage 3. Determination of process capacity
The purpose of this stage is to determine the capacity available in the care processes in order to determine whether they can assimilate the expected demand and to propose measures that contribute to the improvement of their capacity planning.
Step 3.1: Identification of capacity constraining resources
The literature review, direct observation and interviews with service workers allow the identification of a set of capacity limiting resources in hospital institutions. The most common in hospitalization processes are usually: Beds, Human resources, Operating rooms and Diagnostic means. Diagnosing each of these resources in the institution under study allows a better analysis of the capacity of its processes and provides more detailed information when calculating it.
Step 3.2: Application of the method for process capacity planning approach
Based on an analysis of the most relevant methodologies for process capacity calculation and the characteristics of hospital processes, it is decided to use the heuristic methods for capacity calculation.
The heuristic methods are an algorithm for capacity calculation proposed by [38], in a second version of the one published by the same author in 1986, which was adapted to the characteristics of hospital processes. In the proposed method, the items resulting from the reduction of programs used in production are replaced by the defined MDCs, the demand values come from the demand forecast for each of the MDCs. The time costs are homologated to the resource costs that define the limitation or not in the process capacity according to the trajectories of the different MDC of the process. The variables: Available Time Pool (Fj), Load (Qj), Capacity (Cap), Proportionality Index (bj), Statutory Interruptions (Ps) and % Utilization (Util) are necessary for the application of the method, the relation of equations appears in the application of this method are shown in Table 2.

Source: Own design.
Then, the lowest capacity of the process is sought in terms of the MDC, which is compared with the number of patients predicted to enter the system; if this is higher, the process can assume the demand without any problem, otherwise, it constitutes a limiting point or bottleneck. The criteria for selecting the fundamental point are as follows:
-
Economic criterion: it is the treatment staging that creates the highest profits or generates highest costs (equipment, materials, etc.).
-
It is the operation or treatment staging that all patients go through, regardless of their trajectory after case composition.
-
The most time-consuming treatment staging
-
Investment criteria
Stage 4. Proposed improvements opportunities
The application of the methodology proposed in any hospital institution allows proposing a set of measures to contribute to the improvement of the planning of its services.
3. Discussion of results
The following results are obtained from the application of the proposed procedure for the analysis of capacity in hospital processes.
Stage 1. Preparation for implementation
Step 1.1: Institution characterization
The procedure is applied at the "Faustino Pérez Hernández" Clinical and Surgical Teaching Hospital, located in Matanzas, Cuba. It is located on the central highway 101 km northwest of Matanzas city, belongs to the teaching and research area of Matanzas Provincial Health Directorate. It is classified according to the complexity of its second level services and is in charge of providing health services to Cuban and foreign citizens in the specialties and modalities defined by the center.
Step 1.2: Formation and training of the work team
The work team is structured with seven members who hold positions in the entity: (1) Head of the Quality Organizational Unit, (2) Medical Auditor, (3) Head of the Nursing Department, (4) Deputy Director of Medical Assurance, (5) Deputy Medical Director, (6) Head of the Urgent, Emergency and Transport Center and (7) Residents. They are trained in 3 workshops where the main thematic nuclei addressed in the study are discussed.
Step 1.3: Selection, description and representation of the process
The definition of the process to be studied was based on the graphic representation of these processes by means of the hospital's General Process Map. It was verified with the group of experts through interviews and meetings. It shows the flow of services rendered and the interaction between them. Among the key processes of the institution, Hospitalization is considered as one of the most relevant, defined by most of the experts (95 %) as the central axis of the hospital. Its importance lies in the large number of sub-processes that make it up, given that 19 of the 30 medical services provided by the institution are grouped in the aforementioned process.
The present research will be carried out in the General Surgery service, as requested by the institution's management due to the importance given to it and the lack of previous studies in this service. The representation of the process is shown in Fig. 2.
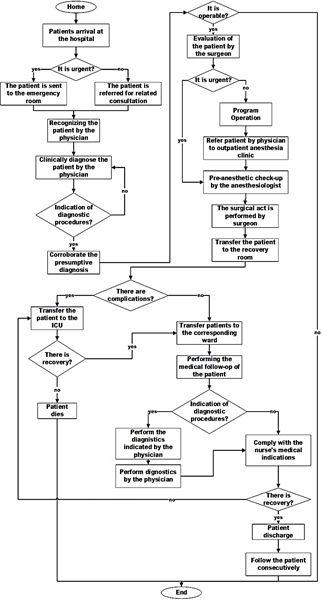
Figure 2
AS-IS diagram of the General Surgery service.
Source: Own design.
Step 1.4: Diagnosis of the selected process
Currently the highest number of interventions in the surgical activity lie in this area with a total, according to the Revitalization of 2019 (internal document), of 6152 operations out of 25614 performed in the period, which represents 24 % of the total number of surgeries performed.
In order to find out the main problems affecting capacity in the General Surgery service, an unstructured brainstorming was carried out together with the selected group of experts. This discussion led to the formation of an Ishikawa diagram (Fig. 3), whose fundamental problem is deficiencies in the capacity of the General Surgery service. The fundamental causes of these deficiencies are shortage of medical supplies, underutilization of operating rooms, deficiencies in process activities, and insufficient room capacity.
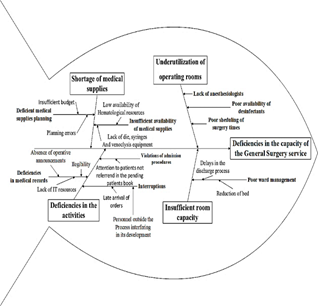
Figure 3
Ishikawa diagram.
Source: Own design.
Stage 2. Demand forecasting
As a premise of the stage, it is necessary to have the main MDCs of the entity, in order to work with a smaller group of patients according to homogeneous surgical categories. In the event of not having the MDCs, it is necessary to have sufficient information for their preparation. The fundamental MDCs of surgical type conformed in the general surgery service of the Hospital "Faustino Pérez Hernández" are: Inguinal Hernia, Umbilical Hernia and Incisional Hernia as they are among the 35 first causes of death in both sexes according to the Health Statistical Yearbook in 2018.
Step 2.1: Definition of study objectives and time horizon
A three-year database was collected, broken down into 12 months for each of the MDCs under study, thus consisting of 36 values for each MDC. The data pertain to the period from 2018 to 2020. The historical records were determined by reviewing advertisements and operative reports.
Step 2.2: Selection and application of feasible forecasting methods
For the selection and application of the most probable forecast method, the SPSS 22 software for Windows was used in its Expert Modeler variant, which allowed the forecast of the number of surgeries per MDC to be attended by months for the year 2021 in the General Surgery service of the "Faustino Pérez Hernández" Hospital.
Step 2.3: Forecast determination
The results of the forecast for each of the MDC are shown in Table 3.
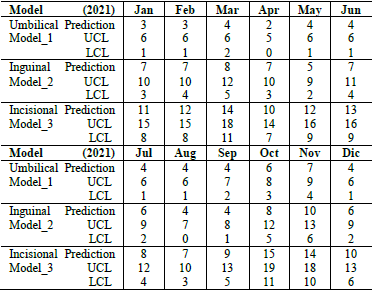
Source: Research data from SPSS 22 software.
In the result of the application of the prognostic method for the time series corresponding to the number of surgeries to be performed, the Simple Seasonal Method was used for the groups related by diagnosis: umbilical and inguinal hernia, and the Winters Additive Method for incisional hernia.
The prognostic results were presented to the working group (Prognostic Questionnaire) and they agreed to maintain the values obtained in the software because their results are in accordance with the behavior of these surgeries in previous years. They also stated that, although the hospital does not have an updated waiting list, from experience the demand could tend to increase, however, under the current conditions of the process it would not be possible to assume such an increase. The above corroborates to some extent the problem of this research and highlights the need to investigate further the capacity of the system.
Stage 3. Determination of process capacity
Step 3.1: Identification of capacity constraining resources
The main resources that limit the capacity of the General Surgery service are identified according to the defined MDC and a method for calculating the capacity of the service is applied. Through direct observation of the service's activities, it was possible to determine the main capacity-limiting resources that may affect the MDCs analyzed.
-
Number of beds in the recovery room. Patients undergoing hernia surgery remain in the recovery room until the anesthesia wears off, since this type of surgery is ambulatory. After that, they leave the institution.
-
The number of operating rooms is a key limiting resource also present in the service analyzed. An operating room can only attend one patient at a time and must be sterilized at the end of one surgery in order to be able to start another. These must have optimal hygienic-sanitary conditions and an adequate climate to avoid subsequent infections or re-interventions.
-
The human resources present in the process and that determine the capacity are the surgeons, anesthesiologists and nurses. The surgeon is the physician in charge of the patient's surgery, while the anesthesiologist sedates the patient and monitors his vital signs until the process is completed and the anesthesia wears off. The nurses are in charge of the ward and take care of the patients until they leave the center.
Step 3.2: Application of the method for process capacity planning approach
The heuristic methods explained in the proposed methodology to determine if the facility can assimilate the expected demand and a linear programming model is applied to determine the optimal combination of performing operations in the facility. Data were collected for the MCCs defined in the second stage, by reviewing documents, experience of PhDs and experts.
-
The surgery process has 2 operating rooms for open surgery during three days of the week. Within these, hernias are operated on one day per week in both rooms.
-
The number of beds installed in the recovery room are 10.
-
The duration times of the surgeries were determined from the review of operative reports that have the start and end time of the operation. The times of those surgeries that for eventual reasons altered the investigation were eliminated and an average value was calculated, and the mode was also considered. In addition, for the time in the operating room, the time of application and fixation of the anesthesia (Spinal-Epidural for the three types of hernia), which ranges from 15 to 20 minutes, and the time of preparation of the operating room to enter the next case, which takes 30 minutes, were analyzed.
-
For the time spent in the recovery room, the nurses were asked to record the times of entry and exit of the room by the patients under study for one month. The results were averaged to obtain an average length of stay per MDC.
-
The time taken by the anesthesiologists to provide the service is composed of the time it takes to apply and fix the anesthesia, the time it takes to perform the surgery and the time it takes for the patient to react after the surgery (moving the feet in the case of Spinal-Epidural anesthesia). The latter ranges from 30 to 60 minutes according to experts, regardless of the type of surgery.
-
For the calculation of the time fund it is assumed that one works 8 hours/day, 1 day/week, 4 weeks/month, and 12 months/year. This time is the same for doctors and rooms. The loss factor for regulatory interruptions is 0.10.
Table 4 shows the length of stay by MDC in the General Surgery service according to the above data.
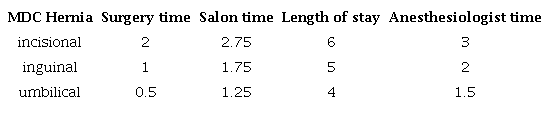
Source: Research data.
The heuristic methods are applied to determine the service capacity limitations (Table 5). The results of the demand forecast and the times shown in Table 4 are used.
The available capacity is 163, 96 and 59 for incisional, inguinal and umbilical hernias, respectively. The resource of the operating room was determined as the fundamental point under the criterion that this is where the greatest use of expendable resources is to be found, being the costliest and the scarcest at present due to the difficult situation in which the country finds itself.
The application of this method showed that the rooms are the resource that most limits the capacity of this service; however, they have the capacity to cover the expected demand for hernias in 2021. It is necessary to make decisions related to their scheduling in order to be more efficient and effective in capacity planning.
On the other hand, the number of patients that an anesthesiologist can attend is determined. These specialists are the ones who spend the most time attending patients, as they are present during the entire surgery and part of the recovery period. Of the two anesthesiologists belonging to the General Surgery service, only one attends open surgery cases.
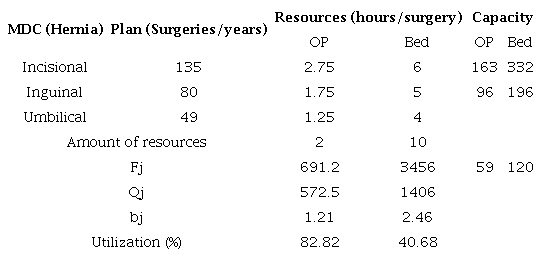
Where: OP (Operating room) Source: Research data.
According to the established protocols, an anesthesiologist must perform 3 to 7 surgeries in a day, depending on the complexity and duration of the surgeries.
Five surgeries were taken as a reference to rule out extreme situations and it was determined that an anesthesiologist can perform 240 surgeries per year, lower than the expected demand of 264 hernia surgeries per year.
The method presents a medium level of precision as it is a medium-term capacity planning method and provides a heuristic solution (Feasible but not optimal). It is effective to clarify that as planning descends from a strategic level to an operational one, the degree of precision is higher as more information needs to be handled. In this sense, expert criteria play a fundamental role, analyzing possible fluctuations or foreseeing changes.
Stage 4. Proposed improvements opportunities
In this stage, a set of measures for the improvement of the capacity of the General Surgery Service of the "Faustino Pérez Hernández" Hospital was elaborated (Table 6).

Source: Own design.
4. Conclusions
The results obtained allowed fulfilling the objective. Based on the main deficiencies found in the research, a set of measures aimed at improving, in the first instance, the planning capacity in the General Surgery process of the "Faustino Pérez Hernández" Clinical Surgical Hospital were proposed.
In the practical development, several tools from the business and hospital management fields with methodological value were applied and adapted, such as systems diagnostics through flow diagrams, Ishikawa diagram, case-mix analysis and demand forecasting, thus serving as a case study in the subjects of management operations for undergraduate and graduate students. It allows the service to take proactive actions and create capabilities based on future demand, an element that improves the performance of the service.
The analysis of capacity by means of the proposed heuristic method revealed that the limiting resource in the process is the anesthesiologists, and in order to meet the predicted demand it is necessary to increase their number, the capacity of the rooms and beds, as well as the percentage of usage, obtaining an 82.82 % in the rooms and a 40.68 % of the beds.
There are three acknowledged limitations of the proposed method, those are the medium level of precision since it does not offer an optimal solution; analysis of external factors that influence the designed plan, which is not included; a high flexibility in decision making is denoted, as it is influenced by expert criteria, which makes it difficult to outline concrete strategies from the strategic-tactical level.
Among the positive implications of the proposed procedure for health managers is the possibility of projecting actions to improve the capacity of services in a medium term, outlining strategies based on demand fulfillment, and analyzing the degree of resource utilization. It contributes to clinical management by making it possible to know the types of patients according to their clinical characteristics.
4.1. Future research
This research remains in the capacity planning in a medium-term (1 year) of a General Surgery service where the limiting resources are beds and wards. The heuristic method is proposed then to achieve planning, due to its easy application. Analyzing the different limiting resources that may affect medium-term capacity planning and the time horizon to determine the demand are proposed for further research. Besides to include the use of some other feasible methods, such as simulation, which would provide more detailed capacity planning in shorter terms (daily, weekly and monthly).
References
Halter, M., Joly, L., de Lusignan, S., Grant, R.L., Gage, H. and Drennan, V.M., Capturing complexity in clinician case-mix: classification system development using GP and physician associate data, BJGP Open, 9(1), pp. 1-10, 2018. DOI: https://doi.org/10.3399/bjgpopen18X101277
Ferreira Jr., R.R. y Adelino Paulo, P., La calidad de vida en el trabajo y el ausentismo como indicadores de resultado de gestión hospitalaria, Ciencias Administrativas, 6(11), pp. 2314-3738, 2018. https://doi.org/10.24215/23143738e015
Hurtado-Camacho, L.F., Diseño de una metodología de mejoramiento del flujo de pacientes para un servicio de hospitalización adultos de tercer nivel de la ciudad de Cali, Tesis de grado, Departamento de Industrial, Universidad Autónoma de Occidente, Santiago de Cali, Colombia, 2015.
Medina-León, A., Nogueira-Rivera, D., Hernández-Nariño, A. y Viteri, J., Relavancia de la gestión por procesos en la planificación estratégica y la mejora continua. Revista Eídos, (2), pp. 65-72, 2010. https://doi.org/10.29019/eidos.v0i2.62
Jabalera, M., Pons, M., Gómez, E., del Castillo, M. y Grupo de Trabajo EMC2., Hacia la excelencia en gestión hospitalaria. Un modelo de gestión estratégica, Journal of Healthcare Quality Research, 34(3), pp. 148-153, 2019. DOI: https://doi.org/10.1016/j.jhqr.2019.02.005.
Davari, F., Nasr-Isfahani, M., Rezvani, M., Omidallah, M. and Pakravan, F., Process management model in the emergency department of a University Hospital: reduction of patient waiting times by changes in human resources, Journal of Research in Medical and Dental Science, 6(2), pp. 578-585, 2018. DOI: https://doi.org/10.5455/jrmds.20186289
Boulain, T., Malet, A. and Maitre, O., Association between long boarding time in the emergency department and hospital mortality: a single‑center propensity score‑based analysis, Internal and Emergency Medicine, 15(3), pp. 479-489, 2020. DOI: https://doi.org/10.1007/s11739-019-02231-z
Rodríguez-Sánchez, Y., Contribución a la planificación de la capacidad en los procesos asistenciales en la atención primaria de salud, Tesis PhD, Departamento Industrial, Universidad de Matanzas, Matanzas, Cuba, 2017.
Bottani, E., Bigliardi, B. and Franchi, B., Process optimization in the hospital environment: a systematic review of the literature and results’ analysis, Procedia Computer Science, 200, pp. 1674-1684, 2022. DOI: https://doi.org/10.1016/j.procs.2022.01.368
Sharoda, A.P., Madhu, C.R. and DeFlitch, J.C., A Systematic review of simulation studies investigating emergency department overcrowding, Simulation, 86(8-9), pp. 559-571, 2010. DOI: https://doi.org/10.1177/0037549709360912
Peter-Hulshof, J.H., Kortbeek, N., Boucherie, R.J., Hans, E.W. and Bakker, P.J.M., Taxonomic classification of planning decisions in health care: a structured review of the state of the art in OR/MS. Health Systems, 1, pp. 129-175, 2012. DOI: https://doi.org/10.1057/hs.2012.18
Hernández-Nariño, A., Contribución a la gestión y mejora de procesos en instalaciones hospitalarias del territorio matancero, Tesis PhD, Departamento Industrial, Universidad Matanzas, Matanzas, Cuba, 2010.
Águila, A. y Sepúlveda, V., Experiencia en el desarrollo e implementación de la metodología de grupos relacionados por diagnóstico en un hospital universitario chileno. Evaluación a diez años de funcionamiento, Revista Médica de Chile, 147(12), pp. 1518-1526, 2019. DOI: https://doi.org/10.4067/S0034-98872019001201518
Borjas-Félix, A.K., Cachay-Ramírez, M.E., Díaz-Ramos, F.Y. Gonzales-Tasayco, C.J.D., Grupos Relacionados por el Diagnóstico (GRD) como herramienta de gestión clínica para medir el producto sanitario en la unidad de cuidados intensivos del Hospital Regional Docente de Cajamarca, MSc. Thesis in Health Services Management, Esan Graduate School of Business, Lima, 2020.
Marqués-León, M., Negrin-Sosa, E., Hernández-Nariño, A., Nogueira-Rivera, D. y Medina-León, A., Modelo para la planificación de medicamentos y materiales de uso médico en instituciones hospitalarias, Gestión y Política Pública, 26, pp. 79-124, 2017. DOI:
Zapata, M., Importancia del sistema GRD para alcanzar la eficiencia hospitalaria, Revista Médica Clínica Las Condes, 29(3), pp. 347-352, 2018. DOI: http://doi.org/10.1016/j.rmclc.2018.04.010.
Chase, R. y Jacob, R., Administración de operaciones. Producción y cadena de suministros. McgGraw-Hill / Interamericana Editores, S.A., México, 2011.
Hernández-Rodríguez, A.R., Bases metodológicas para la gestión por procesos en los servicios hospitalarios. INFODIR [Online]. 35, pp. 1-23, 2021. [date of reference July 25th of 2022]. Available at: Available at: https://revinfodir.sld.cu/index.php/infodir/article/view/785
Grida, M. and Zeid, M., A system dynamics-based model to implement the Theory of constraints in a healthcare system, Simulation , 95(7), pp. 1-13, 2019. DOI: https://doi.org/10.1177/00375497187889
Duarte-Forero, E.L. Y Camacho-Oliveros, M.Á., Planeación de la capacidad hospitalaria: un enfoque desde el flujo de pacientes con Dinámica de Sistemas, INGE CUC, 16(1), pp. 217-233, 2020. DOI: http://doi.org/10.17981/ingecuc.16.1.2020.16.
Jiménez-Paneque, R.E. Indicadores de calidad y eficiencia de los servicios hospitalarios: una mirada actual. Revista Cubana de Salud Pública, [Online]. 30(1), pp. 17-36, 2004. [date of reference September 22th of 2022]. Available at: Available at: https://www.redalyc.org/articulo.oa?id=21430104
Green, L., Capacity planning and management in hospitals, in operations research and health care. A handbook of methods and applications, Kluwer Academic Ed., Boston, USA, 2005, pp. 15-42.
Rojas-Ortega, A.E., Alvarez-Pomar, L. y Parra-Peña, J., Diseño metodológico para la ubicación de ambulancia del sector de atención prehospitalario en Bogotá D.C., Revista Ingeniería Industrial [Online]. 6(1), pp. 77-94, 2007. [date of reference September 22th of 2022]. Available at: Available at: https://revistas.ubiobio.cl/index.php/RI/article/view/121/3347
Delgado-Encinas, K. y Mejía-Puente, M., Aplicación de la simulación discreta para proponer mejoras en los procesos de atención en el área de emergencia de un hospital público, Revistas de Investigación UNMSM, 14(1), pp. 047-054, 2011. https://doi.org/10.15381/idata.v14i1.6209
Chapilliquén-Zapata, F., Diagnóstico del proceso de atención por consultorio externo de un establecimiento de salud utilizando simulación discreta, Tesis de grado, Universidad de Piura, Piura, Perú, 2013.
Swallmeh, E., Tobail, A., Abo Hamad, W., Gray, J. and Arisha, A., Integrating simulation modelling and value stream mapping for leaner capacity planning of an emergency department, in: 2014 The Sixth International Conference on Advances in System Simulation (SIMUL2014), 2014, pp. 256-262.
Ceballos, F., Betancourt-Villegas, J.P. y Betancourt-Villegas, J.D., Simulación discreta aplicada a los modelos de atención en salud, Investigación e Innovación en Ingenierías, 2(2), pp. 10-14, 2014. https://doi.org/10.17081/invinno.2.2.2045.
Báez-Ardila, J., Araujo-Cortés, C., Camacho, M., Duarte, E. y Naranjo, A., Metodología para el análisis de capacidades del servicio de hospitalización en un hospital de Bogotá. Revista Ingenio [Online]. 9(1), pp. 45-55, 2016. [date of reference September 22th of 2022]. Available at: Available at: https://www.researchgate.net/publication/317416342.
Shahverdi, B., Miller-Hooks, E., Tariverdi, M., Ghayoomi, H., Prentiss, D. and Kirsch, T.D., Models for assessing strategies for improving hospital capacity for handling patients during a pandemic, Disaster Medicine and Public Health Preparedness, 12(6), pp. 778-790, 2022. DOI: https://doi.org/10.1017/dmp.2022.12
Reveco, C. and Weber, R., Gestión de capacidad en el servicio de urgencia en un hospital público. Revista Ingeniería de Sistemas [Online]. 25, pp. 57-75, 2011. [date of reference July 25th of 2022]. Available at: Available at: http://www.dii.uchile.cl/~ris/RISXXV/hospital.pdf.
Arnaout, J.P., Heuristics for the maximization of operating rooms utilization using simulation. Simulation , 00(0), pp. 1-11, 2009. DOI: https://doi.org/10.1177/0037549709352497
Orejuela-Cabrera, J.P., Ocampo-Carrillo, J.J. and Micán-Rincón, C.A., Propuesta metodológico para la programación de la producción en las PYMES del sector artes gráficas, área publi-comercial, Estudios Gerenciales, 26(114), pp. 97-118, 2010. DOI: https://doi.org/10.1016/S0123-5923(10)70104-2
Bretthauer, K.M. and Heese, H.S., Blocking in healthcare operations: a new heuristic and an application. Production and Operations Management Society, 20(3), pp. 375-391, 2011. DOI: https://doi.org/10.1111/J.1937-5956.2011.01230.X
Diéguez-Matellán, E.L., Contribución a la planificación de servicios complementarios extrahoteleros en destinos turísticos, Tesis PhD, Departamento Industrial, Universidad de Matanzas, Matanzas, Cuba, 2008.
Marqués-León, M., Modelo y procedimientos para la planificación de medicamentos y materiales de uso médico en instituciones hospitalarias del territorio matancero, Tesis PhD, Departamento Industrial, Universidad de Matanzas, Matanzas, Cuba, 2013.
Becerra, M., Jerez, A., Aballay, B., Garcés, H.O. and Fuentes, A., Forecasting emergency admissions due to respiratory diseases in high variability scenarios using time series: a case study in Chile, Science of the Total Environment, 706, art. 134978, 2019. https://doi.org/10.1016/j.scitotenv.2019.134978
Zhang, Y., Zhang, J., Tao, M., Shu, J. and Zhu, D., Forecasting patient arrivals at emergency department using calendar and meteorological information, Applied Intelligence, 52, pp. 11232-11243, 2022. DOI: https://doi.org/10.1007/s10489-021-03085-9
Acevedo-Suárez, J.A., Modelos y estrategias de desarrollo de la logística y las redes de valor en el entorno de Cuba y Latinoamérica, PhD, Departamento de Ingeniería Industrial, Instituto Superior Politécnico José Antonio Echeverría, La Habana, Cuba, 2008.
Notes