Artículos
Neurofeedback effects on cognitive performance in children with attention deficit
Efecto del Neurofeedback en el desempeño cognitivo de niños con déficit de atención
 Manuel E. Riaño-Garzón m.riano@unisimonbolivar.edu.co
Edgar Alexis Díaz-Camargo e.diaz@unisimonbolivar.edu.co
J. Isaac Uribe-Alvarado iuribe@ucol.mx
Julio C. Contreras-Velásquez j.contrerasvelasquez@hotmail.com
Juan Salazar juanjsv18@hotmail.com
Valmore Bermudez
Manuel E. Riaño-Garzón m.riano@unisimonbolivar.edu.co
Edgar Alexis Díaz-Camargo e.diaz@unisimonbolivar.edu.co
J. Isaac Uribe-Alvarado iuribe@ucol.mx
Julio C. Contreras-Velásquez j.contrerasvelasquez@hotmail.com
Juan Salazar juanjsv18@hotmail.com
Valmore Bermudez
Neurofeedback effects on cognitive performance in children with attention deficit
Archivos Venezolanos de Farmacología y Terapéutica, vol. 37, no. 3, pp. 205-211, 2018
Sociedad Venezolana de Farmacología Clínica y Terapéutica

This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International.
Abstract: The objective of this research was to analyze the effects of an intervention program through neurofeedback, on the cognitive performance in children with inattention indicators. A quasi-experimental pretest-posttest study was used under a positivist epistemology, with a comparative analysis for each evaluated cognitive process. A sample of 29 cases was intentionally selected from a group of children and young adolescents with low performance indicators from a Therapeutic Center from Cucuta-Colombia. The neurofeedback program was developed in 20 sessions with the purpose of increase low-beta waves (12-16 Hz) and inhibition theta waves (4-7 Hz). A comparative statistically analysis with five months of difference was carried out using Wilcoxon test, finding significant differences between the pretest and the posttest in neuropsychological tests of auditory-visual attention, encoding memory and planning. The results are discussed with empirical backgrounds that have shown positive effects in this type of interventions.
Keywords: Attention deficit, Neurofeedback, Neurotechnology intervention, Child Neuropsychology.
Resumen: El objetivo de esta investigación fue analizar los efectos de un programa de intervención a través de neurofeedback, sobre el desempeño cognitivos in niños con indicios de inatención. Un estudio cuasi-experimental pretest-postest fue realizado con un análisis comparativo para cada proceso cognitivo evaluado. Una muestra de 29 casos fueron intencionalmente seleccionados de un grupo de niños y adolescentes con indicadores de bajo desempeño de un centro terapéutico de Cúcuta-Colombia. El programa neurofeedback fue desarrollado en 20 sesiones con el propósito de incrementar la ondas beta-bajas (12-16 Hz) e inhibir las ondas theta (4-7 Hz). Un análisis estadístico comparativo de 5 meses de diferencia fue llevado a cabo mediante el test de Wilcoxon, encontrando diferencias significativas entre los test neuropsicológicos de atención auditiva y visual, codificación de memoria y planificación. Los resultados son discutidos con antecedentes empíricos que han mostrado efectos positivos en este tipo de intervenciones.
Palabras clave: Deficit de atención, Neurofeedback, Neurotecnología, Neuropsicología infantil.
INTRODUCTION
The Attention Deficit Hyperactivity Disorder (ADHD), is typical of the childhood on which different factors are involved, producing in the child alterations on the attention, impulsivity and motor hyperactivity (Curtis, Clemente, González and Hernández, 2016). Similarly, the American Psychiatric Association (APA, 2013) considers it as a disorder of the neurological development characterized by a persistent pattern of inattention, hyperactivity and impulsiveness that interfere in the normal functioning of the child.
In accordance with Fernandez et al. (2012) the main significant interventions have been stimulants, psycho-social therapy and combined treatments for these approaches; additionally, the author mentions the existence of alternative strategies such as nutritional supplements, relaxation and Neurofeedback (NFB). The drug treatment has been an option with significant results in children and teenagers with ADHD (Rose, Reeves, Gut, & Germak, 2015; Cavadas, Pereira, & Mattos, 2007; Fernández-Mayoralas, Fernández-Perrone, & Fernández-Jaén, 2012); however, NFB emerges as a new non-drug treatment, and preliminary findings indicate a similar improvement in comparison with the drug treatment (Meisel, Aggensteiner, García and Servera, 2012), likewise, Hodgson, Hutchinson & Denson (2014) reported a history of NFB as a therapeutic alternative to reduce the symptoms of ADHD.
NFB is a variant of the Biofeedback, which relies on the use of software and hardware that allows a person to voluntarily control the electrical activation of the body (Frank, Khorshid, Kiffer, Moravec & Mckee, 2010); in this case, it refers specifically to the modification of the electrical activity in the cerebral cortex.
Using the NFB technique a person can get information about any psychophysiological process aiming to learn how to modify this process on a voluntary basis (Riaño, 2012, Evans 2007). Gaviria, Calderón and Barrera (2014) note that NFB seeks through operant conditioning that the patient learns to control the electrical brain activity to increase the desired brainwaves frequency and remove the unwanted. Therefore, it is important to mention that changes of electroencephalographic patterns of attention deficit are modified through voluntary control of brain waves.
According to the characteristics of the attention disorder, Cueli, Rodríguez, García, Areces & González (2015) mention that the treatment should be directed to increase the cortical activity. In accordance with these authors, NFB has been considered like treatment that allows the increment of this activation, not only by the feedback that allows the patient to be aware, to recognize and increase his/her own level of activation, but also to establish new neural pathways. Rodriguez & Criado (2014) consider the NFB as training to patients with ADHD, developed by the individual control of brain waves oriented to increase the beta activity and decrease the theta activity to improve the care processes and the self-control behavioral measures.
Regarding the effectiveness, the results of the studies indicate that the NFB treatment produces improvements in the control of the behavior and in the attention symptoms (Moreno, Delgado, Aires & Meneres 2013; Bernal, 2014; Álvarez, González-Castro, Núñez, González-Pienda & Bernardo, 2007); Likewise, NFB effects have been reported through the increment of the sensorimotor rhythm (SMR) and beta wave (12Hz-16Hz) on the selective attention skills (Mohammadi, Malmir, & Khaleghi, 2015), as well as improvements in auditory attention, phonological awareness (Au, Ho, Choi, Leung, Waye, Kang, & Au, 2014), reaction times (Bakhshayesh, Hansch, Wyschkon, Rezai, & Esser, 2011), attention and memory (Riaño-Garzón & Diaz-Camargo, 2018) and IQ (Leins et al., 2007).
The study on NFB in children is important considering recent reports that indicate that children from Cúcuta-Colombia have inferior results in attention and planning tasks compared to previous studies from other cities in Colombia and Mexico (Riaño, Díaz, Torrado, Salomón, Salón & Raynaud, 2017).
Likewise, it is necessary to explore the non-invasive NFB effects as treatment with empirical support, devoid of training to parents or caregivers as principles of therapy (Loro-López y cols., 2009; Helwig 2011; Rangel 2014), lifestyle modification (Morales Aguilar, Lastre-Amell, & Pardo Vásquez, 2018), no side-effects (Lake, 2010; Valverde e Inchauspe, 2014), improving performance in attentional control tasks and other cognitive process, decreasing ADHD symptoms. Thus, the objective of this research was to analyze the effects of an intervention program through NFB, on the cognitive performance in children with inattention indicators.
METHOD
Design
A quasi-experimental pretest-posttest study was conducted for analyzing NFB training program effects on the tasks of auditory and visual attention performance. Additionally, memory processes and executive functioning were evaluated, considering theoretical relationship between these processes and the attentional skills (Etchepareborda & Diaz, 2009).
Participants
Minors from six to 14 years old (Boys, n=21 and Girls, n=8) with school reports of attention difficulties, poor academic performance and behavioral problems. By intentional sampling, 18 children from 6 to 9 years old, and 11 young adolescents from 10 to 14 years old (WHO, n.d.) were selected given less than 25 percentile results in attention tests according to Colombian standardization of Child Neuropsychological Evaluation - ENI (Matute, Rosselli, Ardila & Ostrosky, 2013). Participants were were referred by school during the period 2014-2016. Cases with clinical diagnosis other than ADHD and with pharmacological management were excluded. The study was approved by the Bioethics Committee of Simón Bolivar University (act number: C2021770117, January 10th, 2017).
Procedure
The intervention program was developed in three phases: a) Initial evaluation of attention processes, memory and executive functions. B) Implementation of NFB training protocol and c) Post-intervention assessment.
Instruments
Evaluación Neuropsicológica Infantil - ENI is a Mexican-Colombian standardized test with test-retest reliable in visual attention (r = 0.77-0.88) and reliability among qualifiers of 0.858-0.987 (Matute et al, 2013). The following ENI subtest were used: 1) Visual attention was assessed through “cancelación de letras y dibujos” test. 2) Auditory attention through the task of direct and inverse digit retention. 3) Encoding memory it was evaluated using the learning curve (4 trials / 12 words) and for long-term memory spontaneous word list recovery was used, 4) Cognitive flexibility it was evaluated by card classification subtest and 5) Planning assessment, “Pirámide de México” was used which consists of building designs with blocks counting the number of movements.
Neurofeedback training
The NFB training was done through the Brainmaster 2.5 software and 2EB Clinical system. The electrodes fixed to the scalp at Cz location according to the International 10/20 system with two mastoid electrodes like reference. The NFB protocol was performed under contingencies of auditory and visual reinforcement, aim to low-beta wave increase (12-16 Hz) and theta wave inhibition (4-7 Hz) in a monopolar montage. This training was developed in twenty sessions (two sessions per week, each session lasting 30 minutes). During the montage, participants performed five-minute attentional training activities with Mental Games-Mindplace. software.
Statistical analysis
Qualitative variables were expressed in absolute and relative frequencies. The normality distribution was determined through the Shapiro-Wilk test, concluded there was no normality in data distribution, thus quantitative variables were expressed in medians (Q1-Q3) and nonparametric statistics were used.
Comparison pretest-postest resulted from direct scores analysis in each sub-test of the ENI scale, in groups of children and young adolescents, differences analysis was performed using Wilcoxon test. All analyses were carried out using the SPSS v21.0, statistically significant results were considered when .<0.05.
RESULTS
A total of 29 minors were studied, (Boys, n=21 and Girls, n=8) with age between six to 14 years old. Table 1 shows differences in pretest-posttest cognitive performance, finding statistically significant differences in scores of auditory attention tasks, visual attention, encoding-long-term-memory and planning.
Table 1. Differences in pretest-posttest cognitive performance
| Neuropsychological test | Md | Q1 | Q3 | Z | P value | |
| Auditory attention Direct digits | Pretest | 4.0 | 4.0 | 4.0 | -3.900 | .000* |
| Postest | 5.0 | 4.0 | 5.0 | |||
| Auditory attention Inverse digits | Pretest | 3.0 | 2.0 | 3.0 | -4.134 | .001* |
| Postest | 4.0 | 3.0 | 4.0 | |||
| Visual attention drawing | Pretest | 14.0 | 5.5 | 19.0 | -3.595 | .000* |
| Postest | 20.0 | 15.0 | 23.5 | |||
| Visual attention letters | Pretest | 16.0 | 6.5 | 27.5 | -3.559 | .000* |
| Postest | 24.0 | 12.5 | 30.0 | |||
| Encoding memory | Pretest | 24.5 | 20.2 | 29.0 | -4.628 | .000* |
| Postest | 31.0 | 27.0 | 38.0 | |||
| Long-term memory | Pretest | 7.0 | 5.3 | 9.0 | -2.880 | .004* |
| Postest | 8.0 | 7.0 | 9.8 | |||
| Failure to maintain set | Pretest | 1.0 | 0.0 | 1.5 | -.182 | .856 |
| Postest | 1.0 | 0.0 | 2.0 | |||
| Category | Pretest | 1.0 | 1.0 | 2.0 | -2.660 | ,008* |
| Postest | 2.0 | 1.0 | 3.0 | |||
| Perseveration error | Pretest | 10.0 | 6.5 | 13.0 | -1.803 | ,071 |
| Postest | 7.0 | 4.0 | 11.0 | |||
| Planning | Pretest | 5.1 | 4.0 | 7.5 | -4.335 | ,000* |
| Postest | 8.0 | 7.3 | 9.0 | |||
| Md: Median, Q1: Percentile 25, Q3: Percentile 75.*Wilcoxon test. Significance=p<0.05 | ||||||
In attention process, increase in the volume of digits retention task were observed. Likewise, in the drawings and letters selection task, errors of omission and commission were decreased while execution speed in task was increased. In words memory tasks, major volume of words recall was observed, both short and long term. Finally, in the planning tasks through designs, to decrease in number of movements for the realization of each model was found (Figure 1).
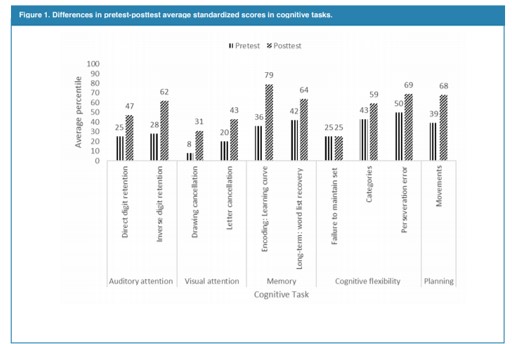
Figure 1
For the detailed analysis of the increments, direct scores of each subtest of the ENI scale were averaged grouped by age and percentile scores. Finally, the percentile scores were averaged between the groups of age and are presented for each evaluated process (Table 2).
Table 2. Differences in pretest-posttest cognitive performance according to age groups.
| Children | Young adolescents | |||||||||||
| Neuropsychological tests | Md | Q1 | Q3 | Z | P Value | Md | Q1 | Q3 | Z | P Value | ||
| Auditory attention Direct digits | Pretest | 4.0 | 3.0 | 4.0 | -3.162 | 0.002* | 4.0 | 4.0 | 5.0 | -2,333 | 0.020* | |
| Postest | 4.0 | 4.0 | 5.0 | 5.0 | 5.0 | 6.0 | ||||||
| Auditory attention Inverse digits | Pretest | 2.0 | 2.0 | 3.0 | -3.035 | 0.002* | 3.0 | 3.0 | 3.0 | -2,887 | 0.004* | |
| Postest | 3.0 | 2.8 | 4.0 | 4.0 | 4.0 | 4.0 | ||||||
| Visual attention drawing | Pretest | 11.5 | 3.0 | 15.5 | -2.987 | 0.003* | 19.0 | 14.0 | 23.0 | -1,956 | 0.050* | |
| Postest | 18.0 | 13.0 | 22.0 | 22.0 | 19.0 | 33.0 | ||||||
| Visual attention letters | Pretest | 11.5 | 0.0 | 18.5 | -2.182 | 0.02* | 27.0 | 17.0 | 34.0 | -2,805 | 0.005* | |
| Postest | 17.0 | 9.8 | 24.5 | 33.0 | 26.0 | 49.0 | ||||||
| Encoding memory | Pretest | 22.0 | 20.0 | 26.0 | -3.628 | 0.000* | 29.0 | 29.0 | 32.0 | -2,936 | 0.003* | |
| Postest | 29.0 | 26.0 | 31.5 | 36.0 | 31.0 | 40.0 | ||||||
| Long-term memory | Pretest | 6.0 | 5.0 | 7.5 | -2.708 | 0.007* | 9.0 | 9.0 | 10.0 | -1,275 | 0.202 | |
| Postest | 7.0 | 7.0 | 9.0 | 10.0 | 8.0 | 12.0 | ||||||
| Failure to maintain set | Pretest | 1.0 | 0.0 | 1.0 | -0.264 | 0.79 | 1.0 | 0.0 | 2.0 | ,000 | 1.00 | |
| Postest | 1.0 | 0.0 | 1.0 | 1.0 | 0.0 | 2.0 | ||||||
| Category | Pretest | 1.0 | 1.0 | 2.0 | -1.748 | 0.08 | 1.0 | 1.0 | 2.5 | -2,041 | 0.041* | |
| Postest | 2.0 | 1.0 | 2.0 | 3.0 | 1.5 | 3.0 | ||||||
| Perseveration error | Pretest | 10.0 | 7.0 | 12.8 | -1.360 | 0.17 | 11.0 | 2.5 | 15.0 | -1,365 | 0.172 | |
| Postest | 8.0 | 6.3 | 11.8 | 3.0 | 1.0 | 9.0 | ||||||
| Planning | Pretest | 5.1 | 3.0 | 8.3 | -3.313 | 0.001* | 5.1 | 5.0 | 7.0 | -2,807 | 0.005* | |
| Postest | 7.6 | 7.0 | 9.3 | 8.7 | 8.0 | 9.0 | ||||||
| Md: Median, Q1: Percentile 25, Q3: Percentile 75.*Wilcoxon test. Significance= p<0.05 | ||||||||||||
A correlational analysis between the auditory attention and memory processes was carried out, pre and posttest analysis, considering that attention is a basic function for the encoding memory and storing of information (Table 3).
| Cognitive Process | Enconding memory Pretest | Long-term memory Pretest | Enconding memory Postest | Long-term memory Postest |
| Auditory attention Pretest | .563 (.002)** | .450 (.016)* | .393 (.038)* | .521 (.004)** |
| Auditory attention Postest | .563 (.002)** | ,519 (.005)** | ,518 (.005)** | ,642 (.000)** |
| Spearman correlation coeficient (P value) *p<0.05 **p<0.01 | ||||
DISCUSSION
The significant improvements found in auditory and visual attention tasks are consistent with the information reported by Moreno et al. (2013), Bernal (2014), Mohammadi et al. (2015), Gadea, Aliño, Garijo, Espert, & Salvador (2016) and Álvarez et al. (2007), who noted significant statistically changes in attention variables thanks to the interventions with NFB, which in accordance with the approaches stated by Jiménez et al. (2012) allow suggesting an improvement in memory due to the strengthening of voluntary care processes.
The differences found in follow-up attention processes can be explained by changes in theta and beta electrical activity. In first, theta activity maybe consider as neurophysiological markers of the ADHD (Yordanova, Heinrich, Kolev, & Rothenberger, 2006), for example, increased theta showed association between diminished attention test performance (Bink et al., 2015). Also, in children with a diagnosis of ADHD, observing high rates of slow alpha and theta waves in frontal lobes (Meisel et al, 2012; Boutros Fraenkel & Feingold, 2005), while Meier, Perrig, & Koenig (2015), finding excessive beta power at frontal, central and parietal brain lobes in adults with ADHD symptoms.
In this sense, previous findings that have reported a relationship between the increase of 4-7 Hz slow activity (theta waves) with a low blood flow in frontal lobes in ADHD (Gunkleman & Johnston, 2005, Toomin 2002) and low metabolism of the glucose (Gonzalez-Castro, Álvarez, Gonzalez-Pienda, Álvarez, & Muñiz, 2010) which would explain inattention-impulsive component; likewise, the presence of low beta (12-16Hz) brain activity in the central region is called sensory motor rhythm which is related to high voluntary attention capacity and a greater cortical activation (Meisel, Servera, Garcia-Banda, Cardo & Moreno, 2013; Franco, 2006) Likewise, some reports indicate low levels of beta rhythms in cases of attention deficit (Butnik, 2005, Gonzalez-Castro et al., 2010; Bakshsayesh et al., 2011), and others add activation predominance of slow waves in prefrontal regions (Álvarez et al., 2007; Walker, 2010) which from a physiological look would explain the inattention in intervened children as well as those therapeutic effects of the NFB training.
Using the predictive model selected, it was found that the memory processes can be improved as a result of the increment in attention abilities, noting that the attention capacity allows the access to the memory as pointed by Jiménez et al. (2012). This can be explained warning that the memory processes will be favored by storing or encryption strategies, which depend on the maturity in executive functions (Ramírez, Arenas & Henao, 2005; Gomez-Perez, Ostrosky-Solis & Próspero-García, 2003). Additionally, previous studies have pointed out that attention disorders at an old age have shown memory capabilities and reduced impulse control (Valdizan & Izaguerri-García, 2009).
Differences were found in auditory attention specifically in inverse digits task, that is related with working memory, similar finding to Ghaemi & Toozandehjani (2016) report, who showed NFB effects on working memory in children evaluated through digit span task, with an intervention protocol of 20 sessions with synchronization of region Cz, with increase of SMR waves and inhibition of theta waves, as used in this study. Hosseini, Pritchard-Berman, Sosa, Ceja, & Kesler (2016), have also reported improvements in working memory, nevertheless, the authors intervened young adult population, also adding improvements in other functioning executive processes such as inhibitory control and alternating attention.
In relation to long-term memory, in the current research none statistically significant changes were observed, however studies carried out with adults showed NFB effects in this process even with patients with strokes (Kober, Schweiger, Witte, Reichert, Grieshofer, Neuper, & Wood, 2015), it should be noted that NFB training protocols based on Alpha waves protocols have been used to find this effect which is similar to the initial results of Hanslmayr, Sauseng, Doppelmayr, Schabus, & Klimesch (2005).
The cognitive flexibility processes evaluated using the card classification test did not show significant statistically changes, however, when analyzing by groups of age, a greater increase in the number of categories was observed as well as a decrease of repetitive response in the group of young adolescents, which is a consistent finding in relation to the reports of Kouijzer, van Schie, Gerrits, Buitelaar & de Moor (2013), who highlighted NFB effects in the improvement of the cognitive flexibility, the group of age was formed by school students who were from 12 to 18 years old. With the latter, it is possible to expect greater changes in the cognitive flexibility in ages of secondary school students, which is explained by their neurodevelopmental; insofar maturity in these processes has been reported in the age of 12 years old (Cinan, 2006), as well as greater cognitive flexibility between 12 and 16 years old in comparison with other groups of age that were even higher (Hauser, Iannaccone, Walitza, Brandeis, & Brem, 2015). The latter agrees to the findings of Hosseini et al. (2016) who reported improvements in development of flexibility cognitive through NFB training in a sample from 19 to 33 years old. In this sense, a higher impact of the intervention on cognitive flexibility is expected in young adult population.
It is worth mentioning that the changes reported in both the attention processes and the executive functioning allow inferring better self-regulation skills in intervened children.
CONCLUSIONS
We concluded that NFB training for therapeutic purposes is effective and efficient to increase indicators of attention, short-term memory, and planning, noting that changes were obtained with an intensity of 20 sessions, classifying it as an effective treatments in the cost-duration perspective. The impact of the increment in the capacities of attention processes should be mentioned from the indirect effects of the program, finding in the study that auditory attention variability predicts 40% of the memory performance. Additionally, it is also noted the relationship with attention, as a basic process that enables the development of the memory-knowledge, even the intelligence.
These results, besides validating the NFB effects in a Colombian border context, should be taken into account as a strategy that used along to other therapies, can enhance the effects getting effectiveness and efficiency to the management of the attention deficit that involves behavioral, contextual and physiological components. The extension of the study using representative samples is expected, including randomization, long term follow-up and comparisons with the control group that would allow classifying this intervention alternative as highly efficient.
Compliance with Ethical Standards and limitations
Conflict of Interest: Authors declare that it has no conflict of interest.
Limitations: We identified some methodological deficiencies, such as the absence of a control group and the sample size which was divided into comparison age group.
Ethical approval: The children and their parents voluntarily accepted the participation of the evaluation and intervention processes as well as the publication of the findings while preserving the confidentiality of their personal data. The well-being of the children was guaranteed, using other intervention procedures in which they are not shown increasing results above the two deviations in the standardized tests. The children were not exposed to risks of any kind. All procedures performed were in accordance with the ethical standards of the Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Bioethics Committee of Simón Bolivar University (act number: C2021770117, January 10th, 2017).
Informed consent: A written informed consent was obtained from children and their parents to participate in the study.
REFERENCES
Akhutina, T. y Pilayeva, N. (2004). Metodología para el desarrollo y la corrección de la atención en niños escolares. México: BUAP.
Alvarez, L., Gonzales-Castro, P., Nuñez, J., Gonzales-Pienda, J., Bernardo, A. (2008). Evaluación y control de la activación cortical en los déficit de atención sostenida. Clin Health Psychol, 8 (2). 509-524.
American Psychiatric Association (2013). Manual diagnóstico y estadístico de trastornos mentales (5°ed). Washington DC: American Psychiatric Publishing.
Ato, M; López, J J; & Benavente, A; (2013). Un sistema de clasificación de los diseños de investigación en psicología. Anales de Psicología, 29 (3), 1038-1059.
Au, A., Ho, G. S. M., Choi, E. W. M., Leung, P., Waye, M. M. Y., Kang, K., & Au, K. (2014). Does it help to train attention in dyslexic children: Pilot case studies with a ten-session neurofeedback program. International Journal on Disability and Human Development, 13(1), 45-54. doi:http://dx.doi.org/10.1515/ijdhd-2013-0005
Bakhshayesh, A., Hansch, S., Wyschkon, A., Rezai, M., & Esser, G. (2011). Neurofeedback in ADHD: a single-blind randomized controlled trial. Eur Child Adolescent Psychiatry, 20, 481–491, DOI 10.1007/s00787-011-0208
Bernal, C. (2014). Neurofeedback en niños con Trastorno por Déficit de Atención e Hiperactividad. [online] Repositorio Digital Institucional CES. Recuperado de http://bdigital.ces.edu.co:8080/repositorio/handle/10946/1614
Bink, M., van Boxtel, G. J., M., Popma, A., Bongers, I. L., Denissen, A. J., van Nieuwenhuizen, C. (2015). EEG theta and beta power spectra in adolescents with ADHD versus adolescents with ASD + ADHD. European Child & Adolescent Psychiatry, 24(8), 873-886. doi:http://dx.doi.org/10.1007/s00787-014-0632-x
Boutros N, Fraenkel L, Feingold A. (2005) A four-step approach for developing diagnostic tests in psychiatry: EEG in ADHD as a test case. Neuropsychiatry Clin Neurosci; 17, 455-64.
Butnik, S. (2005). Neurofeedback in Adolescents and Adults with Attention Deficit Hyperactivity Disorder. JCLP/In Session, 61(5), 621–625.
Cavadas, M., Pereira, L. D., & Mattos, P. (2007). Effects of methylphenidate in auditory processing evaluation of children and adolescents with attention deficit hyperactivity disorder]. Arquivos De Neuro-Psiquiatria, 65(1), 138-143.
Cinan, S. (2006). Age-Related Changes in Concept Formation, Rule Switching, and Perseverative Behaviors: A Study Using WCST with 12 Unidimensional Target Cards. Cognitive Development, 21(3), 377-382.
Corsi, E., Barrera, P., Flores, C., Perivancich, X., & Guerra, C. (2015). Efectos de un programa combinado de técnicas de modificación conductual para la disminución de la conducta disruptiva y el aumento de la conducta prosocial en escolares chilenos. Acta Colombiana De Psicología, 12(1), 67-76.
Cueli, M., Rodríguez, C., García, T., Areces, D., y González, P. (2015). Estudio experimental sobre el Neurobiofeedback: una mejora de la concentración en el ADHD a través del nirHEG y la fluidez sanguínea. Revista de Psicología Clínica con Niños y Adolescentes, 2(2), 135-141.
Curtis, D. L., Clemente, C. M., González, J. P. H., y Hernández, P. J. R. (2016). Evolución histórica del concepto del trastorno por déficit de atención e hiperactividad. Canarias Pediátrica, 40(1), 40-46.
Delgado-Mejia I., & Etchepareborda, M. (2013) Trastornos de las funciones ejecutivas. Diagnóstico y Tratamiento. Revista de Neurología; 57, 95-113.
Duarte, E. (2015) Neurofeedback como tratamiento para el trastorno por déficit de atención (TDA) (Tesis doctoral). Universidad Complutense de Madrid, España.
Echeburúa, E., & Corral, P. D. (2001). Eficacia de las terapias psicológicas: de la investigación a la práctica clínica. Revista Internacional de Psicología clínica y de la salud, 1(1), 181-204.
Etchepareborda, M; Diaz, A. (2009). Aspectos controvertidos en el trastorno de déficit de atención. Medicina; 69, 51-63.
Evans, J. R. (2007). Handbook of neurofeedback: dynamics and clinical applications. New York: Haworth Medical Press.
Fernández, S. (2012). Eficacia de las intervenciones con niños y adolescentes con Trastorno por Déficit de Atención con Hiperactividad (TDAH). Anuario de psicología/The UB Journal of psychology, 42(1), 19-33.
Fernández-Mayoralas, D. M., Fernández-Perrone, A.L., & Fernández-Jaén, A. (2012). Actualización en el tratamiento farmacológico del trastorno por déficit de atención e hiperactividad/Advances in the pharmacological treatment of attention-deficit/hyperactivity disorder. Acta Pediatrica Espanola, 70(6), 239-246.
Franco, A. (2006). Como vivir sin Ritalina. Medellín: Novedades S.A.
Frank, D., Khorshid, L., Kiffer, J., Moravec, C. & Mckee. M. (2010). Biofeedback in medicine: who, when, why and how? Mental Health in family Medicine, 7, 85-91.
Gadea, M., Aliño, M., Garijo, E., Espert, R., & Salvador, A. (2016). Testing the benefits of neurofeedback on selective attention measured through dichotic listening. Applied Psychophysiology and Biofeedback, 41(2), 157-164. doi: http://dx.doi.org/10.1007/s10484-015-9323-8
Gaviria, J., Calderón, L., y Barrera, M. (2014). ¿Es efectivo el entrenamiento en Neurofeedback para el tratamiento del TDAH? Resultados a partir de una revisión sistemática. CES Psicología, 7(1), 16-34.
Ghaemi, H., & Toozandehjani, H. (2016). The effectiveness of neurofeedback on working memory, visual memory and reading ability in children with dyslexia. Journal of Current Research in Science, (2), 870-875.
Gómez-Perez, E. Ostrosky-Solis, F. & Próspero-García, O. (2003) Desarrollo de la atención, la memoria y los procesos inhibitorios: relación temporal con la maduración de la estructura y función cerebral. Revista de Neurología, 37 (6), 561-567.
González-Castro, P., Alvarez, L., González-Pienda, J., Álvarez, D. y Muñiz, J. (2010). Cortical activation and attentional control in ADAH subtypes. International Journal of Clinical and Health Psychology. 10 (1), 23-39.
Gunkelman, J. & Johnstone, J. (2005). Neurofeedback and the Brain. Journal of Adult Development. 12 (2-3) 93-99.
Hauser, T. U., Iannaccone, R., Walitza, S., Brandeis, D., & Brem, S. (2015). Cognitive flexibility in adolescence: Neural and behavioral mechanisms of reward prediction error processing in adaptive decision making during development. NeuroImage, 104, 347-54. doi: http://dx.doi.org/10.1016/j.neuroimage.2014.09.018
Hanslmayr, S., Sauseng, P., Doppelmayr, M., Schabus, M., & Klimesch, W. (2005). Increasing individual upper alpha power by neurofeedback improves cognitive performance in human subjects. Applied Psychophysiology and Biofeedback, 30(1), 1-10. doi:http://dx.doi.org/10.1007/s10484-005-2169-8
Helwig, J. (2011). Sleep Disturbance in Children and Adolescents with ADHD: Unique Effects of Medication, ADHD Subtype, and Comorbid Status. Theses and Dissertations. 1321.
Hodgson, K., Hutchinson, A. D., & Denson, L. (2014). Nonpharmacological treatments for ADHD: A meta-analytic review. Journal of Attention Disorders, 18(4), 275-282. doi: http://dx.doi.org/10.1177/1087054712444732
Hosseini, S. H., Pritchard-Berman, M., Sosa, N., Ceja, A., & Kesler, S. R. (2016). Task-based neurofeedback training: A novel approach toward training executive functions. NeuroImage, 134, 153-159. doi: http://dx.doi.org/10.1016/j.neuroimage.2016.03.035
Jiménez, J., Hernández, S., García, E., Díaz, A., Rodríguez, C. & Martín, R. (2012). Test de atención D2: Datos normativos y desarrollo evolutivo de la atención en educación primaria. European Journal of Education and Psychology, 5(1),93-106. doi: 10.1989/ejep.v5i1.93
Kober, S. E., Schweiger, D., Witte, M., Reichert, J. L., Grieshofer, P., Neuper, C., & Wood, G. (2015). Specific effects of EEG based neurofeedback training on memory functions in post-stroke victims. Journal of Neuroengineering and Rehabilitation, 12: 107.
Kouijzer, M. E., J., van Schie, H., T., Gerrits, B. J., L., Buitelaar, J. K., & de Moor, J. (2013). Is EEG-biofeedback an effective treatment in autism spectrum disorders? A randomized controlled trial. Applied Psychophysiology and Biofeedback, 38(1), 17-28. doi:http://dx.doi.org/10.1007/s10484-012-9204-3
Lake J. (2010). Integrative Management of ADHD: what the evidence suggests. [Online]. Psychiatric times: 8-11, [Citado en Julio 2011] Obtenido en: http://www.individualandfamilychoices.com/Text/complementary%20therapies%20including%20neurofeedback%20for%20ADHD.pdf
Leins, U., Goth, G., Hinterberger, T., Klinger, C., Rumpf, N. & Strehl, U. (2007). Neurofeedback for Children with ADHD: A Comparison of SCP and Theta/Beta Protocols. Applied Psychophysiol Biofeedback, 32, 73–88, DOI 10.1007/s10484-007-9031-0.
Loro-López M, Quintero J, García-Campos N, Jiménez-Gómez B, Pando F, Varela-Casal P, Campos JA, Correas-Lauffer J. (2009). Actualización en el tratamiento del trastorno por déficit de atención/hiperactividad. Rev Neurol, 49 (05):257-264
Manga D, Ramos F. (2011) El legado de Luria y la neuropsicología escolar. Psychology, Society & Education 2011; 3: 1-13.
Matute, E., Rosselli, M., Ardila, A., y Ostrosky, F. (2013). Evaluación Neuropsicológica Infantil – ENI 2. México: Manual Moderno.
Mayer, K., Wyckoff, S. N., Fallgatter, A. J., Ehlis, A. C., & Strehl, U. (2015). Neurofeedback as a nonpharmacological treatment for adults with attention-deficit/hyperactivity disorder (ADHD): study protocol for a randomized controlled trial. Ensayos, 16(1), 1.
Meier, N. M., Perrig, W., & Koenig, T. (2015). Is excessive electroencephalography beta activity associated with delinquent behavior in men with attention-deficit hyperactivity disorder symptomatology? Neuropsychobiology, 70(4),210-219. doi:http://dx.doi.org/10.1159/000366487
Meisel V., Servera M., Garcia-Banda G., Cardo E., Moreno I. (2013). Neurofeedback and standard pharmacological intervention in ADHD: a randomized controlled trial with six-month follow-up. Biol Psychol, 94(1):12-21
Meisel, V., Aggensteiner, P. M., García, G., y Servera, M. (2012) El neurofeedback como procedimiento de intervención en caso de TDAH: fundamentos y posibilidades. En Asociación española de Psicología Conductual (2012), Avances en Psicología Clínica, 639-642. doi: 978-84-695-3599-8.
Morales Aguilar, R., Lastre-Amell, G., & Pardo Vásquez, A. (2018). Estilos de vida relacionados con factores de riesgo cardiovascular. Archivos Venezolanos de Farmacología y Terapéutica, 37(2), 54-62.
Moreno, I., Delgado, G., Aires, M., & Meneres, S. (2013). Administering the CPT/IVA to evaluate the effects of neurofeedback in ADHD. Anuario de Psicología Clínica y de la Salud, 9, 49-50.
Moreno, I. Delgado, G. Camacho, C. Meneres, S. y Servera, M. (2015). Neurofeedback, tratamiento farmacológico y terapia de conducta en hiperactividad: análisis multinivel de los efectos terapéuticos en electroencefalografía. International Journal of Clinical and Health Psychology, 15(3), 217-225.
Mohammadi, M. R., Malmir, N. & Khaleghi, A. (2015). Comparison of sensorimotor rhythm (SMR) and beta training on selective attention and symptoms in children with attention Deficit/Hyperactivity disorder (ADHD): A trend report. Iranian Journal of Psychiatry, 10(3), 165-174.
Ortega, A. Ariza, A. Delgado, D. y Riaño, M. (2015). Programa de estimulación sobre procesos atencionales en niños con TDAH. Fronteras Del Saber 6, 31-38.
Ortiz, A., & Moreno, I. (2015). Perfil electroencefalográfico de niños con TDAH. Revista de Psicología Clínica con Niños y Adolescentes, 2(2), 129-134.
Ramírez, L., Arenas, A. & Henao, G. (2005). Caracterización de la memoria visual, semántica y auditiva en niños y niñas con déficit de atención tipo combinado, predominantemente inatento y grupo control. Revista electrónica de investigación psicoeducativa, 7 (3), 89-108.
Rangel, J.F. (2014). El trastorno por déficit de atención con o sin hiperactividad (TDA/H) y la violencia: Revisión bibliográfica. Salud Mental, 37: 75-82.
Riaño-Garzón, M., & Diaz-Camargo, E.A. (2018). Neurofeedback Training to Increase of Cognitive Skills in Patient with Traumatic Brain Injury (TBI). Journal of Neurology & Stroke, 8(1), 00270. DOI: 10.15406/jnsk.2018.08.00270
Riaño, M., Diaz, E.A., Torrado, J., Salómón, J., Salón, Y. & Raynaud, N. (2017). Habilidades cognoscitivas en niños que inician edad escolar de la base de la pirámide: estudio comparativo. En: Graterol, M., Mendoza, M., Contreras, J., Graterol, R. & Espinoza, J. (2017). La base de la pirámide y la innovación frugal en América Latina. Maracaibo: Astro Data.
Riaño, M. (2012). Neurofeedback: Principios y Aplicaciones Clínicas Actuales. Signos Vitales, 4,19-22.
Riaño, M. y Quijano, M.C. (2015). La función reguladora del lenguaje, Intervención en un caso de atención deficitaria. Acta Neurológica Colombiana, 31(1),71-78.
Rodríguez, P., y Criado, I. (2014). Plan de tratamiento multimodal del TDAH. Tratamiento psicoeducativo. Pediatría Integral, 18(9),624-631.
Rose, S. R., Reeves, G., Gut, R., & Germak, J. (2015). Attention-Deficit/Hyperactivity disorder medication treatment impact on response to growth hormone therapy: Results from the ANSWER program, a non-interventional study. The Journal of Pediatrics, 167(6), 1389-1396. doi:http://dx.doi.org/10.1016/j.jpeds.2015.08.036
Solovieva Y., Quintanar L. y Lázaro E. (2008) Mecanismos de los lóbulos frontales en niños preescolares con déficit de atención y niños normales. Acta Neurológica Colombiana, 24, 2: 64-75.
Tirapu-Ustárroz J, Muñoz-Céspedes JM, Pelegrín-Valero C, Albéniz-Ferreras A (2006). Propuesta de un protocolo para la evaluación de las funciones ejecutivas. Revista de Neurología; 41, 177-86.
Valdizan, J.R. & Izaguerri-García, A.C. (2009). Trastorno por déficit de atención/hiperactividad en adultos. Revista de Neurología, 48 (Supl 2): S95-S99.
Valverde, M., & Inchauspe, J. (2014). Alcance y limitaciones del tratamiento farmacológico del trastorno por déficit de atención e hiperactividad en niños y adolescentes y guías de práctica clínica. Una revisión bibliográfica. Revista de la asociación española de neuropsiquiatría, 121 (34): 37-74.
Walker, J. (2010). Recent Advances in Quantitative EEG as an Aid to Diagnosis andas a Guide to Neurofeedback Training for Cortical Hypofunctions, Hyperfunctions, Disconnections, and Hyperconnections. Applied Psychophysiology Biofeedback 35, 25–27.
WHO (n.d). Very young adolescents [online February 2018]. Retrieved from http: http://www.who.int/reproductivehealth/topics/adolescence/very_young_ados/en/
Yordanova, J., Heinrich, H., Kolev, V., & Rothenberger, A. (2006). Increased event-related theta activity as a psychophysiological marker of comorbidity in children with tics and attention-deficit/hyperactivity disorders. NeuroImage, 32(2), 940-955. doi:http://dx.doi.org/10.1016/j.neuroimage.2006.03.056.