Artículos
Volumetry of subdural hematomas in computed tomography images: ABC methods versus an intelligent computational technique
Volumetría de hematomas subdurales en imágenes de tomografía computarizada: métodos abc versus una técnica computacional inteligente
Volumetry of subdural hematomas in computed tomography images: ABC methods versus an intelligent computational technique
Archivos Venezolanos de Farmacología y Terapéutica, vol. 37, no. 4, pp. 326-330, 2018
Sociedad Venezolana de Farmacología Clínica y Terapéutica

This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International.
Abstract: This work evaluates the performance of some methods oriented towards the generation of the volume of four subdural hematomas (SDH), present in multi-layer computed tomography images. To do this, firstly, a reference volume is considered to be that obtained by a neurosurgeon using the manual planimetric method (MPM), which allows the generation of manual segmentations of space-occupying lesions, which in this case are matched with the SDH. The MPM consists of: a) Manually drawing the outline that delimits the SDH, in each of the layers or sections in which the SDH is present. b) Calculate the partial area using the number of pixels contained in each contour. c) Obtain the total SDH area by adding the partial areas. d) Calculate the volume considering the total number of layers, the total area of the SDH and the thickness of each layer. Secondly, the volumetry of the 4 SDHs is obtained considering both the original version of the ABC/2 method and two of its variants, identified in this paper as ABC/3 method and 2ABC/3 method. The ABC methods allows for the calculation of the volume of the hematoma under the assumption that the SDH has an ellipsoidal shape. In these methods, A is the maximum diameter of the SDH, B is the length of the SDH measured, perpendicularly, with respect to the parameter A; while C represents the product of the thickness of the cut by the number of cuts in which the SDH is present. In third place, an intelligent automatic technique (SAT) is implemented that generates the three-dimensional segmentation of each SDH and from it the volume of the hematoma is calculated by multiplying the voxel dimensions by the number of voxels that make up the SDH. In the context of the present work, the expression SAT method will be used to refer to the new methodology that is proposed to calculate the volume of the SDH. The SAT consists of the pre-processing, segmentation and post-processing stages. During pre-processing, a thresholding algorithm and a bank of computational filters are used to address artifact and image noise problems. In segmentation, the growth of regions is applied to pre-processed images. Finally, a morphological dilation filter is used as a technique to perform the post-processing of the segmented images. In order to make judgments about the performance of the SAT, the Dice coefficient (Dc) is used to compare the dilated segmentations of the SDH with the SDH segmentations generated manually, by a neurosurgeon. The combination of parameters linked to the highest Dc, allows to establish the optimal parameters of each of the computational algorithms that make up the SAT. Finally, the percentage relative error is calculated as a metric to evaluate the methodologies considered. The results show that the SAT method exhibits the best performance generating an average percentage error of less than 5%.
Keywords: ABC Methods, Automatic Intelligent Technique, Segmentation, Volumetry of subdural hematomas.
Resumen: Mediante este trabajo se evalúa el desempeño de algunos métodos orientados hacia la generación del volumen de cuatro hematomas subdurales (SDH), presentes en imágenes de tomografía computarizada multicapa. Para ello, en primer lugar, se considera como volumen de referencia el obtenido por un neurocirujano usando el método manual planimétrico (MPM) el cual permite generar segmentaciones manuales de lesiones ocupantes de espacio, que en este caso se hacen coincidir con los SDH. El MPM consiste en: a) Trazar manualmente el contorno que delimita el SDH, en cada una de las capas o cortes en las que el SDH está presente. b) Calcular del área parcial usando el número de píxeles contenido en cada contorno. c) Obtener el área total del SDH mediante la suma de las áreas parciales. d) Calcular el volumen considerando el número total de capas, el área total del SDH y el espesor de cada capa. En segundo lugar, la volumetría de los 4 SDH es obtenida considerando tanto la versión original del método ABC/2 como dos de sus variantes, identificadas en este trabajo como método ABC/3 y método 2ABC/3. Los métodos ABC, permiten calcular el volumen del hematoma bajo la suposición de que el SDH tiene forma elipsoidal. En estos métodos, A es el diámetro máximo del SDH, B es la longitud del SDH medida, perpendicularmente, respecto al parámetro A; mientras que C representa el producto del grosor del corte por el número de cortes en los que está presente el SDH. En tercer lugar, se implementa una técnica automática inteligente (SAT) que genera la segmentación tridimensional de cada SDH y a partir de ella se calcula el volumen del hematoma multiplicando las dimensiones del vóxel por el número de vóxeles que conforman el SDH. En el contexto del presente trabajo, se utilizará la expresión método SAT para hacer referencia a la nueva metodología que se propone para calcular el volumen de los SDH. La SAT consta de las etapas de pre-procesamiento, segmentación y pos-procesamiento. Durante el pre-procesamiento, se emplea un algoritmo de umbralización y un banco de filtros computacionales para abordar los problemas de artefactos y ruido de las imágenes. En la segmentación, el crecimiento de regiones se aplica a las imágenes pre-procesadas. Finalmente, un filtro de dilatación morfológica se usa como técnica para realizar el pos-procesamiento de las imágenes segmentadas. Con el propósito de emitir juicios de valor acerca del desempeño de la SAT, se utiliza el coeficiente de Dice (Dc) para comparar las segmentaciones dilatadas del SDH con las segmentaciones del SDH generadas, manualmente, por un neurocirujano. La combinación de parámetros vinculada con el Dc más elevado, permite establecer los parámetros óptimos de cada una de los algoritmos computacionales que conforman la SAT. Finalmente, el error relativo porcentual es calculado como métrica para evaluar las metodologías consideradas. Los resultados muestran que el método SAT exhibe el mejor desempeño generando un error porcentual promedio inferior al 5%.
Palabras clave: Métodos ABC, Técnica automática inteligente, Segmentación, Volumetría de hematomas subdurales.
INTRODUCTION
Among the different types of hematomas or intracranial and extracerebral hemorrhages, one type are subdural hematomas (SDH). Normally, SDH are pathologies caused by traumatic brain injuries or craneoencephalic traumas (CET) that cause the laceration of brain tissue or its vessels1 and are located below the dura mater membrane that surrounds the brain1. According to the time of evolution, from the moment of the CET, they are classified as: acute (up to 3 days), subacute (up to 2 weeks) and chronic (more than 2 weeks)2.
Multilayered computed tomography (MSCT)3 is the most used diagnostic test to identify chronic SDH which are common in digital brain neuroimaging (DCNI), especially in patients with a high rate of postoperative recurrence4. In addition, the sizes of chronic pre- and post-operative subdural hematomas have been used in clinical trials to predict the risk of postoperative recurrence.
Additionally, the increasing incidence of this type of pathology has also increased the use of automatic computational techniques aimed at the accurate and efficient definition of the volume of these hematomas, since that volume is the main parameter considered by medical specialists, when addressing and monitoring SDH6.
Also, it is important to point out that the DCNI are accompanied by various imperfections such as noise3,7 and artifacts8. These imperfections become real challenges, when computational segmentation strategies are implemented oriented towards the generation of the morphology (normal or abnormal) of both the cerebral anatomical structures and space-occupying lesions, such as, for example, subdural hematomas.
Figure 1, generated based on multilayered computed tomography (MSCT) images, presents axial views of the 4 SDH that were considered in this work. Also in it, the presence of the main problems typical of this type of image linked to noise (Poisson) and the stair artifact are observed.
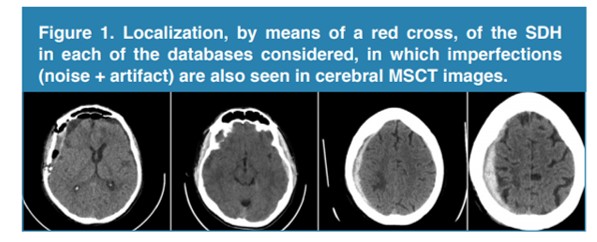
Figure 1.
Localization, by means of a red cross, of the SDH in each of the databases considered, in which imperfections (noise + artifact) are also seen in cerebral MSCT images
On the other hand, the most relevant attribute or predictor of an SDH is its volume. The reason why this attribute is so important is that its numerical value defines, in a high percentage, both the prognosis of the patient and the behavior to follow to address this disease7. Due to this, some methodologies oriented towards the estimation of said predictor have been reported in literature. Some of those methodologies are described below.
Stanišić et al.4,5, perform a comparative study between techniques that use linear measurements, to estimate the volume of the SDH, and a computational method that calculates the volume directly analyzing the 3D morphology of 107 SDH, present in corresponding MSCT images to 107 patients. They establish the limitations that linear methods have when estimating the volumes of SDH in patients evaluated after the surgical intervention.
Additionally, Wang et al.6, evaluate classic ABC methods to estimate the volume of SDH and validate them against a variant of these methods, proposed by them, in said publication. As a primary result they obtain that their variant exhibits a performance that surpasses the classic ABC methods.
Sucu et al.9, evaluated 28 computerized tomographies in which they determine the volume of SDH using the ABC/2 method. They emphasize the importance of determining if this method yields comparable results when estimating the volume of both acute and chronic SDH. They state that the mentioned method generates valid results for both types of bruises. In the ABC methods, the axial view of that layer or cut is used where the SDH exhibits its largest diameter which represents the parameter A, on the other hand, B is made to coincide with the diameter of the SDH perpendicular to the diameter; while C is the product of the thickness of the image by the number of cuts in which the SDH is present
On the other hand, this article constitutes an extension of the work presented in the reference11. The main contributions of the present work are:
a) Use an intelligent automatic technique (SAT) to calculate the volume of the ICH, present in 4 databases formed by three-dimensional brain images of MSCT. The aforementioned technique considers the stages of pre-processing, segmentation and post-processing. These stages are subjected to a validation process that uses the Dice coefficient to compare SDH segmentations obtained automatically and manually11.
b) Consider the percentage relative error (PrE) to perform a comparative study between the ABC methods and the SAT method, in such a way that their performance can be established when they obtain the volume of the SDH (Av). During the comparison, the one obtained by the manual planimetric method (MPM), applied by a neurosurgeon, is taken as the reference volume (Rv). The percentage relative error is calculated using the mathematical model given by equation 1.
Equation 1
MATERIALS AND METHODS
Description of the Data Bases used
The databases (DB) used were supplied by the Central Hospital of San Cristóbal-Táchira-Venezuela. They were acquired through the MSCT modality and consist of three-dimensional images (3D), corresponding to the anatomical structures present in the head of 4 male patients. Their numerical characteristics are presented in table 1.
Table 1. General characteristics of the databases considered in the present work.
| DB Label | Voxels Number | Voxel Dimensions (mm3) | Scanner Type | Age (years) |
| DB1 | 512x512x60 | 0.4551 x 0.4551 x 2.8096 | Siemens Spirit CT84299 | 37 |
| DB2 | 512x512x27 | 0.4882 x 0.4882 x 5.0521 | *GE Hi Speed DUAL CT | 21 |
| DB3 | 512x512x40 | 0.4023 x 0.4023 x 3.2780 | *GE Light Speed VCT IRIS | 81 |
| DB4 | 512x512x20 | 0.4589 x 0.4589 x 6.2784 | *GE Light Speed VCT IRIS | 38 |
As table 1 reveals, high variability in the size of the voxel is observed and we are in the presence of a group of 4 patients whose age ranges between 21 and 81 years. In addition, the identification of the tomographs allows the inference about the robustness of the proposed technique in the face of inter-tomograph variability.
In order to compliment and validate the study, manual segmentations are available, generated by a neurosurgeon, corresponding to the hematomas present in the four DBs. These segmentations represent the ground truth that will serve as a reference to validate the results linked to the segmentation.
Smart Automatic Technique (SAT) for the segmentation of SDHs.
By means of figure 2, a schematic diagram is presented that synthesizes the computational algorithms that make up the SAT. For a detailed description of the SAT, reference11 should be reviewed, since, as indicated above, this article is an extension of that work.
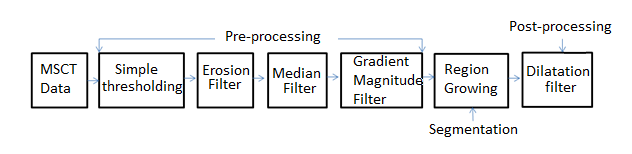
Figure 2.
Block diagram of the intelligent automatic technique proposed in6.
On the other hand, it is necessary to point out that the Dice coefficient (Dc)3 is a metric used to compare segmentations of the same 2D or 3D image, obtained by different methodologies. In the medical context, usually, the Dc is considered to establish how similar, spatially, manual segmentation (RD) and automatic segmentation (RP) usually are, and that generates the morphology of any anatomical structure. Additionally, the Dc is maximum when a perfect overlap between RD and RP is reached but it is minimal when RD and RP do not overlap at all. In addition, the values expected for the Dc are real numbers between 0 (minimum) and 1 (maximum). The mathematical model that defines the Dc, is given by Equation 2.

Equation 2
Clinical utility of the volumes occupied by the hematomas
1- Lesion located in the anterior or middle cranial fossa with volume greater than 30 cm..
The main clinical utility of the characterization of hematomas by obtaining the volume lies in the decision making that is made to establish the behavior to be followed to address the presence of bruising in a patient. In this sense, patients whose lesions meet any of the following criteria must be taken to surgical10.
1- Lesion located in the anterior or middle cranial fossa with volume greater than 30 cm3.
2- Displacement of the midline (imaginary line between occipital eminence and crista gally) greater than one cm, from its original position.
3- Compression, displacement or occupation of specific areas of the brain (mass effect).
4- Location of the hematoma in the cortical zone.
5- Lesion located in the posterior fossa (cerebellum, stem) with a volume between 10 cm3 and 15 cm3 depending on the clinical presentation of the patient.
Quantification of the hematomas considering the determination of the respective volume
Measuring the volume of bruises is important to define the final behavior before the process by which the patient passes. The volume and behavior of the lesion define parameters called surgical criteria which are fundamental at the time of treatment.
Obtaining the volumes related to the automatic segmentations
The proposed technique generates the automatic segmentation of the SDH present in each of the 4 databases described. From such segmentations, the volume of the hematoma, candidate to be characterized, is calculated by multiplying the voxel dimensions by the number of voxels that make up the automatically segmented SDH.
RESULTS
Quantitative results
During the segmentation process, it was applied as a criterion that the optimal parameters of the algorithms that make up the SAT are those that produce the highest Dc. At the end of the tuning process, a maximum Dc of 0.8876 was obtained, which indicates a good correlation between the manual segmentations and those obtained by the SAT. Additionally, table 2 shows that the average value of the Dc obtained for SDH segmentation, using the SAT method, is comparable to that reported in references12,13.
| Authors | Technique | Modality | Average Dc |
| Kamnitsas et al(2017)12 | Neural network Convolutions | MSCT | 0.9032 |
| Prakash et al(2012)13 | Regularized level sets | MSCT | 0.8971 |
| Vera et al. (Technique proposed in the current work) | SAT | MSCT | 0.8765 |
Qualitative results
Figure 3, shows a 2-D view of both the original SDH and the processed versions after applying the SAT technique to one of the DB considered.
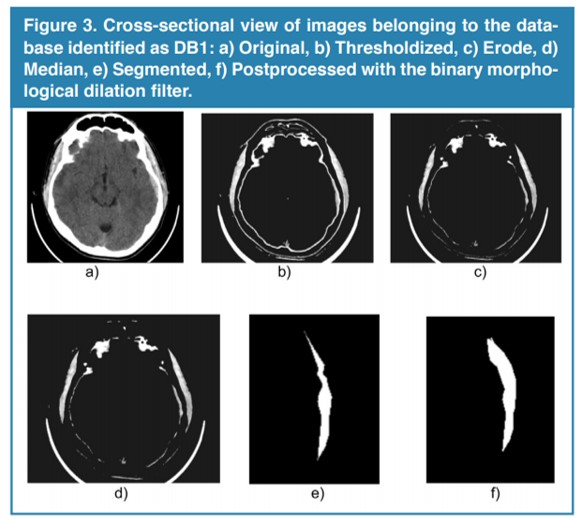
Figure 3.
Cross-sectional view of images belonging to the database identified as DB1: a) Original, b) Thresholdized, c) Erode, d) Median, e) Segmented, f) Postprocessed with the binary morphological dilation filter.
On the other hand, figure 4 shows an excellent three-dimensional representation of the 4 segmented subdural hematomas.
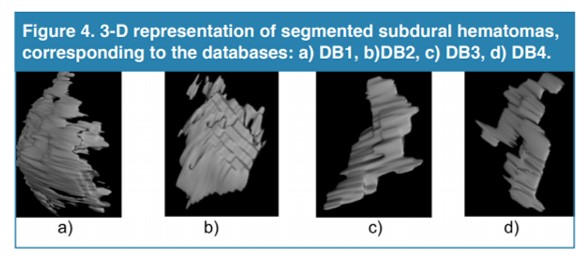
Figure 4.
3-D representation of segmented subdural hematomas, corresponding to the databases: a) DB1, b)DB2, c) DB3, d) DB4.
In figure 4, it can be seen that this type of hematoma does not have a defined shape and therefore, in general, it can be said that the geometric hypothesis considered by the ABC methods to estimate the volumes of the SDH is not always valid. On the other hand, table 3 shows the values for the volumes calculated for the SDHs that is, using both the SAT method and the ABC methods considered.
| Volume (cm3) | |||||
| Database | MPM | SAT | ABC/2 | ABC/3 | 2ABC/3 |
| DB1 | 15.17 | 15.69 | 15.81 | 10.54 | 21.08 |
| DB2 | 8.95 | 9.32 | 11.07 | 7.38 | 14.76 |
| DB3 | 3.51 | 3.63 | 4.49 | 2.99 | 5.98 |
| DB4 | 2.09 | 2.26 | 2.46 | 1.64 | 3.30 |
It can be inferred from the information presented in table 3 that SAT, ABC/2 and 2ABC/3 methods estimate the value of the volume; while the ABC/3 method underestimates it. According to Huttner et al.14, the ABC/3 method has not been validated clinically and, indeed, can exhibit excellent behavior in cases in which the patient consumes anticoagulants or has undergone radio and/or chemotherapy.
On the other hand, table 4 presents the values corresponding to the relative percentage errors related to each of the methods considered.
| Percentage relative error (%) | ||||
| SAT | ABC/2 | ABC/3 | 2ABC/3 | |
| DB1 | 3.43 | 4.22 | 30.52 | 38.96 |
| DB2 | 4.13 | 23.69 | 17.54 | 64.92 |
| DB3 | 3.42 | 27.92 | 14.81 | 70.37 |
| DB4 | 8.13 | 17.70 | 21.53 | 57.89 |
| Average PercentageRelative error (%) | 4.78 | 13.38 | 21.1 | 58.03 |
According to table 4, it can be affirmed that the SAT method generates the best average percentage relative error (Erp). In addition, the ABC methods exhibit the best performance in ABC/2, although in small volume hematomas tend to produce higher errors. This may be due to the fact that this method is based on the hypothesis that the SDH has an ellipsoidal shape and according to14, this is not always fulfilled (see, additionally, figure 4).
In this section it is important to remember that the main surgical utility of the determination of SDH volumes is that they define, in a high percentage, the behavior to be followed regarding the patient. In this sense, if only volume is considered, hematomas that exceed the threshold of 30 cm3 are susceptible to surgery. Following this criterion, and considering the results of the volume obtained by the MPM and those derived from the SAT method, which yielded the lowest PrE, no patient is a candidate for surgery.
CONCLUSIONS
In general, it can be said that the main characteristic of ABC methods is their simplicity and efficiency, although their performance, in many concrete situations, is not always the best option. In this sense, the fulfillment of the geometric hypothesis that an SDH has an ellipsoidal shape represents the main limitation of these methods, especially when it comes to patients who have SDH with no definite shape, relatively small and/or large volume. However, when the SDH complies with the aforementioned hypothesis, these methods have an acceptable performance and, in particular, the ABC/2 method has a good prestige since it has been clinically validated, while its variants do not yet have that condition. Additionally, in several investigations it has been verified that these methods have as an additional disadvantage the property of being operator-dependent.
In the context of the present work, we have used an intelligent automatic technique (SAT) whose tuning allows the precise segmentation of the SDH, present in computed tomography images. This statement is based on the fact that the Dc obtained is comparable with that reported in the literature. The segmentations generated, automatically, by the SAT allows for the calculation of the volume of each SDH in a precise and efficient manner. This volume is vital to address the hematoma that affects the health status of a patient and decide whether or not it is surgically treated.
Because the SAT method generated the lowest average percentage error, which did not exceed 5%, it can be said that the performance of the SAT method exceeded the ABC methods considered. In part, this is due to the fact that the SAT does not assume any geometric consideration when it generates the volume of an intracerebral hematoma.
Regardless of the type of scanner with which the images of cerebral tomography were acquired, in the present work, the technique developed allowed the successful segmentation of all the hematomas present in the 4 databases considered. This is an indication that the aforementioned computational technique, based on intelligent operators, is robust to inter-subject and inter-tomographic variability.
REFERENCES
[1] Stippler M. Craniocerebral trauma. In: Daroff RB, Jankovic J, Mazziotta JC, Pomeroy SL, eds. Bradley's Neurology in Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2016:chap 62.
[2] Mezzadri J., Goland J., y Sokolvsky M. Introducción a la Neurocirugía. Capítulo: Patología vascular II. Ediciones Journal. Segunda edición. 2011.
[3] Vera M. Segmentación de estructuras cardiacas en imágenes de tomografía computarizada multi-corte. Ph.D. dissertation, Universidad de los Andes, Mérida-Venezuela, 2014.
[4] Stanišić M., Hald J., Groote I., Pripp A., Ivanović J., Kolstad F., Sundseth J., Züchner M., Lindegaard K. (2013). Volume and densities of chronic subdural haematoma obtained from CT imaging as predictors of postoperative recurrence: a prospective study of 107 operated patients. Acta Neurochir (Wien) 2013 Feb; 155(2): 323–333.
[5] Stanišić M., Groote I., Hald J., Pripp A. (2014). Estimation of Chronic Subdural Hematoma Size Using CT Imaging: A Comparison of In-Plane Thickness to 3D Volumetry. Open Journal of Modern Neurosurgery, 2014, 4, 1-6.
[6] Wang Y., Li Y., Zhu Y., Lin T., Zhang Y., Huaizhang Shi Y. (2017). A novel and precise method for evaluation of chronic subdural hematoma volume. Int J Clin Exp Med 2017;10(4):6198-6203.
[7] Maiera A, Wigstrm L, Hofmann H, Hornegger J, Zhu L, Strobel N, Fahrig R. Three-dimensional anisotropic adaptive filtering of projection data for noise reduction in cone beam CT. Medical Physics. 2011;38(11):5896–909.
[8] Kroft L, De Roos A, Geleijns J. Artifacts in ECG–synchronized MDCT coronary angiography. American Journal of Roentgenology.2007;189(3):581–91.
[9] Sucu H., Gokmen M., Gelal F. The value of XYZ/2 technique compared with computer-assisted volumetric analysis to estimate the volume of chronic subdural hematoma. Stroke 2005; 36: 998-1000.
[10] Freeman, W., Barrett, K., Bestic, J.,Meschia, J., Broderick, D., Brott, T. Computer-assisted volumetric analysis compared with ABC/2 method for assessing warfarinrelated intracranial hemorrhage volumes. 2008, Neurocritical Care, 9, 307–312.
[11] Vera M., Huérfano Y., Contreras J., Vera M. I., Salazar W., Vargas S., Chacón J. y Rodríguez J. (2017). Desarrollo de una Técnica Computacional No Lineal para la Segmentación de Hematomas Subdurales, presentes en Imágenes de Tomografía Computarizada Cerebral. AVFT Archivos Venezolanos de Farmacología y Terapéutica. 36(6), 168-173
[12] Kamnitsas K., Lediga C., Newcombeb V., Simpsonb J., Kaneb A., Menonb D., Rueckerta D., Glockera B. Efficient Multi-Scale 3D CNN with fully connected CRF for Accurate Brain Lesion Segmentation. Medical Image Analysis, Vol 23, pp.1603-1659, 2017.
[13] Prakash K., Zhou S., Morgan T., Hanley D., Nowinski W. Segmentation and quantification of intra-ventricular/cerebral hemorrhage in CT scans by modified distance regularized level set evolution technique. Int J Comput Assist Radiol Surg. 2012; 7(5): 785-798.
[14] Huttner H., Steiner T., Hartmann M., Köhrmann M., Juettler E., Mueller S, Wikner J., Meyding U., Schramm P., Schwab S. y Schellinger P. (2006). Comparison of ABC/2 Estimation Technique to Computer-Assisted Planimetric Analysis in Warfarin-Related Intracerebral Parenchymal Hemorrhage. Stroke. 2006;37:404-408.
Author notes
m.avera@unisimonbolivar.edu.co