Artículos
Liver abscess mimicking tumor: A pediatric case report
Absceso hepático que simula un tumor: reporte de un caso pediátrico
 María Vera
Miguel Vera
Antonio Bravo
María Vera
Miguel Vera
Antonio Bravo
Liver abscess mimicking tumor: A pediatric case report
Archivos Venezolanos de Farmacología y Terapéutica, vol. 39, núm. 4, pp. 516-520, 2020
Sociedad Venezolana de Farmacología Clínica y Terapéutica

Esta obra está bajo una Licencia Creative Commons Atribución-SinDerivar 4.0 Internacional.
Recepción: 28 Mayo 2020
Aprobación: 15 Junio 2020
Publicación: 07 Julio 2020
Resumen: Se presenta un case clínico de un niño de 3 años con antecedentes médicos de amebiasis intestinal parcialmente tratada. El paciente ingresó en la Unidad de Pediatría del Hospital Central San Cristóbal, Táchira, Venezuela, con dolor abdominal y fiebre. Se evaluó un abdomen plano y una hepatomegalia palpable de 3 cm por debajo del reborde costal derecho. La ecografía abdominal reveló un hígado agrandado en el área anterosuperior derecha. Se evaluó una lesión ocupante de espacio redondeado, predominantemente sólida, con patrones de eco mixto, mediante ultrasonido. El diagnóstico preliminar emitido fue de abdomen médico agudo con lesión hepática ocupante de espacio considerada absceso hepático amebiano o tumor hepático, anemia microcítica hipocrómica moderada y desnutrición con talla baja. Durante la evolución del caso, fue necesaria una primera exploración de tomografía computarizada para explotar la capacidad de esta técnica de imagen para escanear un absceso como una pseudocápsula periférica que muestra el borde realzado. Sin embargo, esta forma teórica asociada con abscesos en tomografía computarizada no se pudo verificar en este estudio. En este punto, los patrones de eco mixto del ultrasonido preliminar y la imprecisión de la tomografía computarizada para clasificar la lesión como un absceso o un tumor, no permiten establecer un diagnóstico definitivo. Se propone terapia con antibióticos. La progresión de la lesión ocupante de espacio se realizó mediante ecografía y tomografía computarizada durante la evolución clínica. Los controles de imágenes reflejan una ligera disminución de la lesión hepática, que se diagnostica como un absceso hepático. Se realizó drenaje transhepático percutáneo. Finalmente se diagnosticó un absceso hepático amebiano en resolución.
Palabras clave: Absceso hepático, tumor de hígado, amebiasis, terapia antibiótica, ultrasonido, tomografía computarizada.
Abstract: A case report of a 3-year-old boy with past medical history of intestinal partially treated amebiasis, is presented. The patient was admitted to Pediatric Unit, San Cristóbal Central Hospital, Táchira, Venezuela, with abdominal pain and fever. An abdominal bloating and a 3 cm palpable hepatomegaly below the right costal margin were assessed. Abdominal ultrasound revealed a liver enlarged in the right antero-superior area. A rounded space-occupying lesion, predominantly solid, with mixed‐echo patterns, was assessed using ultrasound. The preliminary diagnosis issued was of acute medical abdomen with hepatic space-occupying lesion considered amebic liver abscess or liver tumor, moderate hypochromic microcytic anemia, and malnutrition with short stature. During the case evolution, a first computerized tomography exploration was necessary in order to exploit the capacity of this imaging technique to scan an abscess as a peripheral pseudo-capsule showing rim enhancement. Nevertheless, this theoretical shape associated with abscesses on computerized tomography scans was unable to verify in this study. At this point, the mixed-echo patterns of the preliminary ultrasound study and the imprecision of the computerized tomography scan to categorize the lesion as an abscess or a tumor, do not allow establishing a definitive diagnosis. A management based on antibiotic therapy is then proposed. The progression of the space-occupying lesion was performed using ultrasound and computerized tomography scans during the clinical evolution. The imaging controls probe a slight decrease of the liver lesion, which is diagnosed as a liver abscess. Percutaneous transhepatic drainage was performed. An amoebic liver abscess in resolution was finally diagnosed.
Keywords: Liver abscess, liver tumor, amebiasis, antibiotic therapy, ultrasound, computerized tomography.
Introduction
The accumulation of purulent secretion in a newly formed cavity is defined as an abscess, which can cause a mass effect and behave like a space-occupying lesion, in some organ of the human body1. In the liver, this inflammatory space-occupying lesion is called a hepatic abscess. These abscesses, according to its etiology, are categorized into pyogenic, amoebic, fungal and mycobacterial2. In general, the most common hepatic abscesses are the pyogenic and amebic liver abscesses3. Amebic abscess is caused when the Entamoeba histolytica trophozoite migrates to the liver through the portal circulation; while the pyogenic liver abscess is almost always due to a bacterial infection4.
The amebic abscess represents less than 1% of the extraintestinal infections associated with the amebic infection in humans. This disease occurs unusually in the left lobe of the liver, it is common at the right lobe mainly located at the posterior, external and superior portion however, it is often seen below the diaphragm, that is, located as ‘antero superior’. It is also unusually present as multiple abscesses, yet 70% of cases it shows as a single lesion5. Regarding the differential considerations, it has been reported in the literature that at the time of diagnosis, according to symptomatology, an amoebic liver abscess can be mistaken with pyogenic abscess, biliary tract disease, hepatitis, pneumonia, appendicitis, or pancreatitis6.
Due to its nature as a space-occupying lesion, the amebic liver abscess must be distinguished from the pyogenic liver abscess, echinococcal cyst, and hepatic tumors5. The diagnosis of pyogenic liver abscess should be associated with the age of the patient, the significant comorbidities, and the surgery and/or biliary disease history7. Echinococcal cysts are asymptomatic in nature; nevertheless, they may be accompanied by a secondary infection and then present as an abscess8. In patients with a clinical history of infection, and with risk factors or evidenced malignancy, a liver mass can lead to a differential diagnosis, a hepatic tumor may be indistinguishable from an abscess9.
The limited literature on the incidence of amoebic liver abscesses in children converges in order to conclude that it is a childhood rare disease10, and that represents between 21 and 30% of cases of liver abscess11. The appearance of amoebic liver abscesses in children is mainly influenced by endemic factors12. In childhood, an acute clinical presentation is verified with symptoms such as fever, chills, abdominal pain, nausea, diarrhea and vomiting. In a very small number of cases, children develop a cough, which can easily divert attention away from the liver13. Even though, the amoebic liver abscess is life-threatening, imaging techniques and the amebicide pharmaceutical effectiveness lead to a very favorable prognosis.
The technique commonly regarded as an imaging front line tool for amebic liver abscesses assessment, is the ultrasound. The ultrasonographic studies reveal the amebic liver abscess as a round or oval homogeneous mass, with abscess wall, peripheral halo, and low level internal echoes14. The low cost, non-invasively treating and availability are determining features in the preference of ultrasound as a medical imaging technique for detecting the amebic liver abscesses. However, when the patient presents a clinical condition less likely of amebic liver abscesses, it is suggested to rely on computed tomography in order to differentiate the inflammatory lesion from other liver lesions15.
In front of the CT scanner, the amebic liver abscess consists of a single chamber with smooth or nodular border, for the latter, one or more septum appears. A common imaging feature is the enhancing wall; nevertheless, it is not a generalization16. Since the amoebic liver abscess corresponds to encapsulated lesion, the shape of its peripheral wall is associated, in CT, with a target or double-rim appearance. CT is the imaging modality used as the main alternative for scanning amebic liver abscess if ultrasound is inconclusive for its diagnosis; however, the amebic liver abscess aspect is variable and nonspecified even for CT17.
Case presentation
A 3-year-old boy presented to the children's emergency room of the San Cristóbal Central Hospital in Táchira, Venezuela with 3 days of fevers and abdominal pain. The preschool patient with a height of 108 cm and weight of 14 kg was referred from an ambulatory center because a history of intestinal partially treated amebiasis and recurrent fever episodes. The ambulatory referral is accompanied by an abdominal ultrasonographic study.
At the children's emergency room, an abdominal bloating was assessed by means the abdominal examination with a 3 cm palpable hepatomegaly below the right costal margin. The assessment of the ultrasound study of the abdomen, referred from the ambulatory and shown in Figure 1, revealed a liver enlarged in the right anterosuperior area of the right lobe at hepatic segment VIII.

Figure 1
Abdominal ultrasound A mixedecho rounded spaceoccupying lesion is observed in the anterosuperior portion of the liver with a tendency to homogeneity
From the ultrasound study analysis, a rounded space-occupying lesion, predominantly solid, with mixed-echo patterns, a volume of 65.5 cc and it not vascularized on Doppler, was also assessed. As a conclusion of the ultrasound study, the following is presented: findings in probable relation with liver abscess, without intrahepatic dilatation of bile ducts. However, the quality of the ultrasound images is very poor.
On physical examination, the patient was in clinical conditions, as pertinent positive findings, he was the globose abdomen, soft, depressible, with bowel sounds, pain upon deep palpation in the epigastrium, hypochondrium and right flank. Tachycardia and the generalized cutaneous-mucous pallor, are also assessed, the rest of the physical examination without alterations. Table 1 shows the collection of physical examination finding.
The admission paraclinical tests were conducted, the laboratory investigations showed hemoglobin 10.3 g/dL, total leukocyte count 17000 cells/mm3 (neutrophils 70%, lymphocytes 28%), platelet count 461000 cells/mm3, with 33.9% haematocrit. The coprology and uroanalysis are non-pathological; the latter showed leukocytes of 1–2/hpf. Nevertheless, the routine coprology lacks sensitivity and agar plate culture is time-consuming.
A preliminary diagnosis of acute medical abdomen was assumed, it is due to hepatic space-occupying lesion, which must be differentiated between amoebic abscess and tumor. The diagnosis at that point was a hepatic abscess of amoebic etiology associated with a history of treated intestinal amebiasis; however, imaging does not reveal conclusive features and even associating the space-occupying lesion with a tumor. Moderate hypochromic microcytic anemia and malnutrition with short stature are also diagnosed.
| Measure | Value |
| Heart rate | 129 bpm |
| Respiratory rate | 24 rpm |
| Body temperature | 39°c |
| Oxygen saturation | 98% |
| Blood pressure | 95/60 mmHg |
| Weight | 14 KG |
| Height | 1.08 m |
| Head circumference | 51 cm |
| Chest circumference | 56 cm |
| Abdominal circumference | 48 cm |
| Weight/Height | Percentile 3 |
| Height/Age | Percentile 3 |
| Weight/Age | Percentile 50 |
Accordingly, the patient was admitted for hospitalization and the antibiotic therapy was started. An abdominal CT and additional paraclinical of the laboratory were ordered. CT scan was planned in order to differentiate the hepatic space-occupying lesion, of the preliminary diagnosis, between an amebic liver abscess and a liver tumor. Additionally, the pediatric interconsultations linked to gastroenterology, infectology, and surgery services were requested.
The fundamental idea with the unenhanced CT scan was to check whether the space-occupying lesion correlated with a liver abscess; for this, the lesion was to submit with the shape of a peripheral pseudo-capsule showing rim enhancement. As can be seen in Figure 2, the theoretical shape associated with abscesses on computerized tomography scans was unable to verify in this first non-contrast imaging study.
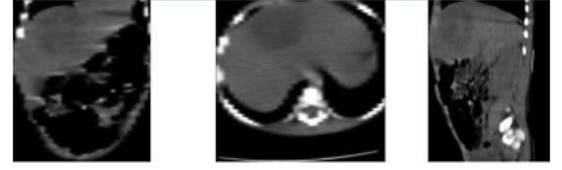
Figure 2.
Abdominal CT. The liver lesion on CT does not have the appearance of a peripheral pseudo-capsule showing rim enhancement, rather it is in the form of a solid liver mass.
Further, in Figure 2, the appearance of the hepatic space-occupying lesion was of a heterogeneous solid lesion, which implies that CT scan without contrast, in this case, it does not allow to differentiate a complex necrotic and cystic cancer from a liver abscess. So far, no other explanation for the symptoms in the current case was discovered despite thorough gastroenterologic, infectology, surgery, and paraclinical examinations. Table 2 shows paraclinical of the laboratory.
| Measure | Value |
| Glycemia | 60mg/dL |
| PT | 13.8 s |
| PTT | 14 s |
| GOT | 31U/L |
| GPT | 39.4 U/L |
| ALP | 60.2 U/L |
| GGT | 26.9 U/L |
| LDH | 141.4 U/L |
| TB | 1 mg/dL |
| DB | 0.3 mg/dL |
| IB | 0.70 mg/dL |
| CPR | 12 (6) mg/L |
The management based on antibiotic therapy continued on intravenous metronidazole at 1.5 g per day for 10 days. During the evolution of the case the patient underwent a pre contrast CT in order to qualify whether the space-occupying lesion varied from iso to hyperdense, but with the peripheral contrast enhancement because this is a contrast CT feature when the lesion corresponds with a liver abscess. For such imaging examination, a normal protocol of creatinine and urea is verified. In addition, the status of the alpha-fetoprotein tumor marker is evaluated, resulting negative. Figure 3 shows the contrast CT of the space-occupying lesion.

Figure 3.
Contrast-enhanced CT of abdomen. The pathological features of an amebic liver abscess that include an outstanding chronic inflammatory response circumscribed around a stringy rim with a very small center necrotic and suppurative, were not verified in the contrast-enhanced CT.
The double-target distinctive feature of the amebic liver abscess on contrast-enhanced CT consisted of three segments, 1) a hypodense cavity, 2) an inner hyperdense ring that surrounds the central hypodense cavity, and 3) an external hypodense zone. This distinctive feature cannot be verified on CT scan as it is shown in Figure 3; therefore the lesion cannot be differentiated from the benign solid and malignant masses.
Nevertheless, this follow-up contrast-enhanced CT scan three weeks after starting antibiotic therapy shows an apparent reduction in the size of the hepatic space-occupying lesion. In this sense, the use of digital image processing techniques is considered as a computer-aided tool to support the diagnosis18. Thus, the space-occupying lesion was segmented from the two three-dimensional CT images without and with contrast, which are shown in Figure 2 and Figure 3, respectively. The volume of the two the three-dimensional pathological structures is quantified, and then their values were compared in order to determine if the size of the liver lesion varied.
The results of the liver lesion segmentation from the CT scan before and after antibiotic therapy shown that the size of this lesion decreased between two explorations; the volumes quantified were of 63.2 cm3 and of 58.9 cm3, respectively. Further, the result associated with contrast-enhanced CT segmentation documented slight decrease in size of the lesion 21 days after first volume assessment from an ultrasonography examination of 65.5 cm3.
The progression of the space-occupying lesion shape was then performed by means of un-contrast and contrast computerized tomography scans during the clinical evolution, with an analysis supported by a computer-aided image processing. The analysis verifies the slight decrease in the space-occupying lesion in the liver, which is associated with therapy with antibiotics. Accordingly, as diagnosis, the lesion is mapped with a liver abscess of amoebic etiology.
Percutaneous transhepatic drainage was performed. As a clinical protocol, abscess drainage should be considered in patients with a high risk of rupturing the abscess, the risk factor is a diameter of the cavity greater than 5 cm19. The volume approximate removed through therapeutic aspiration was of 30.00 cc3. An amoebic liver abscess in resolution was finally diagnosed.
After drainage, the patient remains hospitalized under antibiotic treatment and evaluation by gastroenterology, infectology, pediatric surgery, and medical pediatrics. Finally, the patient is discharged, in good clinical condition. Satisfactory resolution of his pathology was verified and controls were established by gastropediatrics.
Discussion
Amebiasis is an infection that affects 10% of the world population; this infection is considered as endemic parasitic in tropical and subtropical regions20. Because overcrowding and sanitation are commonly deficient in tropical and subtropical countries, the prevalence may be more than 50% in such regions. In Venezuela, a South America country a large population of children, the amebiasis is registered as the main parasitic disease, reporting 100,000 cases a year with 80 deaths, and with a higher frequency in children between 1-4 years of age21.
The amebic hepatic abscess is secondary to colonization and invasion of the wall of the large bowel by E. histolytica, even in cases where it is not possible to demonstrate a clinical history of dysentery, or the presence of the parasite in coprology studies4. This kind of liver abscess is more common in men as in women and it is less common in children, and at childhood amebic liver abscesses are more common in those under 3 years of age22. The normal criteria used to diagnosis require of positive imaging findings.
Usually, the boundaries of the liver abscesses are ill distinguished in ultrasound, their appearance is variable; the lesion is predominantly hypoechoic (with some internal echoes) but can become hyperechoic. The color Doppler support allows demonstrating the central perfusion absence23. The amebic hepatic abscess wall enhancement is possible using contrast-enhanced ultrasound only during the arterial phase. The technique allows characterizing the abscesses by depicting the internal septations, which is important because drainage is not recommended in very septate abscesses. However, the hepatic abscess may appear solid and mimic a hepatic tumor24.
Although the contrast-enhanced CT scan can define exactly the imaging typical feature of double target, associated with amebic liver abscess, differential diagnoses such as necrotic hepatic tumor, complicated biliary cysts, bruises, hydatid cyst, and liver metastases, may occur due to liver abscess appearance at imaging17,25. Differentiation between a single abscess without rim enhancement and tumor mass without necrotic metastases is normally difficult. The segmental improvement surrounding the hepatic lesion would be a clue to the differentiation of the abscess of other hepatic lesion26. In follow-up by computerized tomography, a distinctive feature corresponds with a decrease in size of the lesion, which is performed including medical image processing techniques.
In conclusion, the diagnosis of the amebic hepatic abscess in children may be suggested by specific CT findings obtained by means of computer-aided image analysis in the appropriate clinical setting.
Referencias
1. Kelley, W. Medicina interna. Médica Panamericana, 1993.
2. Branum, G.D., Tyson, G.S., Branum, M.A., Meyers, W.C. Hepatic abscess. Changes in etiology, diagnosis, and management. Annals of surgery. 1990; 212(6):655-662. https://doi.org/10.1097/00000658-199012000-00002.
3. Kurland, J.E., Brann, O.S. Pyogenic and amebic liver abscesses. Current Gastroenterology Reports. 2004; 6(4):273-279. https://doi.org/10.1007/s11894-004-0078-2
4. Sayek, I., Onat, D. Pyogenic and amebic liver abscess. In: Holzheimer, R.G, Mannick, J.A, editors. Surgical Treatment: Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt; 2001. https://www.ncbi.nlm.nih.gov/books/NBK6955
5. Choudhuri, G., Rangan, M. Amebic infection in humans. Indian Journal of Gastroenterology. 2012; 31(4):153-162. https://doi.org/10.1007/s12664-012-0192-2
6. Marx, J.A., Rosen, P. Rosen's emergency medicine: concepts and clinical practice. Elsevier, 2017.
7. Castillo, S. Manterola, C. Morphological characteristics of liver abscesses according its etiology. International Journal of Morphology. 2020; 38(2),406-414. https://dx.doi.org/10.4067/S0717-95022020000200406
8. Pandiaraja J. Diagnostic difficulty of liver lesion. Journal of family medicine and primary care, 2016; 5(3), 722-724. https://doi.org/10.4103/2249-4863.197290
9. Kim, J.W., Shin, S.S., Heo, S.H., Lim, H.S., Hur, Y.H., Kim, J.H. Hepatic abscess mimicking hepatocellular carcinoma in a patient with alcoholic liver disease. Clinical and molecular hepatology. 2013; 19(4): 431-434. https://doi.org/10.3350/cmh.2013.19.4.431
10. Mishra, K., Basu, S., Roychoudhury, S., Kumar, P. Liver abscess in children: an overview. World Journal of Pediatrics. 2010; 6(3):210-216. https://doi.org/10.1007/s12519-010-0220-1
11. Roy Choudhury, S., Khan, N.A., Saxena, R., Singh Yadav, P., Patel, J.N, Chadha. R. Protocol-based management of 154 cases of pediatric liver abscess. Pediatric Surgery International. 2017; 33: 165-172. https://doi.org/10.1007/s00383-016-4009-8
12. Pai-Jui, Y., Chien-Chang, C., Ming-Wei, L., Hung-Yu, Y., Hsun-Chin, C. Pediatric liver abscess: trends in the incidence, etiology, and outcomes based on 20-years of experience at a tertiary center. Frontiers in Pediatrics. 2020; 8:1-8. https://doi.org/10.3389/fped.2020.00111
13. Mortelé, K.J., Segatto, E., Ros, P.R. The infected liver: radiologic-pathologic correlation.. RadioGraphics. 2004; 24:937-955. https://doi.org/10.1148/rg.244035719
14. Ralls, P.W., Quinn, M.F., Boswell, W.D., Colletti, P.M., Radin, D.R., Halls, J. Patterns of resolution in successfully treated hepatic amebic abscess: sonographic evaluation. Radiology. 1983; 149(2):541-543.
15. Chuang, C., Wu, S., Chen, A., Tsai, M., Lin, C., Chen, W. Pitfalls in a sonographic diagnosis of liver abscess in children. Pediatrics and Neonatology. 2012; 53(2):98-104. https://doi.org/10.1016/j.pedneo.2012.01.006
16. Radin, D.R., Ralls, P.W., Colletti, P.M., Halls, J.M. CT of amebic liver abscess. American Journal of Roentgenology. 1988; 150(6):1297-1301.
17. Bächler, P., Baladron, M.J., Menias, C., Beddings, I., Loch, R., Zalaquett, E., Vargas, M., Connolly, S., Bhalla, S., Huete, A. Multimodality imaging of liver infections: differential diagnosis and potential pitfalls. RadioGraphics. 2016; 36(4):1001-1023. https://doi.org/10.1148/rg.2016150196
18. Vera, M., Medina, R., Del Mar, A., Arellano, J, Huérfano, Y., Bravo, A. An automatic technique for left ventricle segmentation from MSCT cardiac volumes. Journal of Physics: Conference Series. 2019; 1160(012001):1-7.
19. VanSonnenberg, E., Mueller, P.R., Schiffman, H.R., Casola, G., Simeone, J.F., Cabrera, O.A., Gosink, B.B. Intrahepatic amebic abscesses: indications for and results of percutaneous catheter drainage. Radiology. 1985; 156(3): 631-635.
20. Haque, R., Huston, C.D., Hughes, M., Houpt, E., Petri, W.A. Jr. Amebiasis. The New England Journal of Medicine. 2003; 348(16):1565-1573.
21. Araujo, J., García, M.E., Díaz-Suárez, O., Urdaneta, H. Amebiasis: importance of the diagnosis and treatment. Minireview. Investigación Clínica. 2008; 49(2):265-271. Available from: http://ve.scielo.org/scielo.php?script=sci_arttext&pid=S0535-51332008000200013&lng =es&tlng=es.
22. Harrison, H.R., Crowe, C.P., Fulginiti, V.A. Amebic liver abscess in children: clinical and epidemiologic features. Pediatrics. 1979; 64(6):923-928.
23. Gebel, M. Ultrasound in gastroenterology and hepatology. Wiley-Blackwell, 2000.
24. Hui, J.Y., Yang, M.K., Cho, D.H., Li, A., Loke, T.K.L., Chan, J.C.S., Woo, P.C.Y. Pyogenic liver abscesses caused by Klebsiella pneumoniae: US appearance and aspiration findings. Radiology. 2007; 242(3):769-776. https://doi.org/10.1148/radiol.2423051344
25. Mathieu, D., Vasile, N., Fagniez, P.L., Segui, S., Grably, D., Lardé D. Dynamic CT features of hepatic abscesses. Radiology. 1985; 154(3):749-752. https://doi.org/10.1148/radiology.154.3.3969480
26. Gabata, T., Kadoya, M., Matsui, O., Kobayashi, T., Kawamori, Y., Sanada, J., Terayama, N., Kobayashi, S. Dynamic CT of hepatic abscesses: significance of transient segmental enhancement. American Journal of Roentgenology. 2001; 176(3):675-679. https://doi.org/10.2214/ajr.176.3.1760675