Artículos
Relation between difficulty level of laparoscopic procedures and the incidence of complications during urologic laparoscopic surgery in Dr. Sardjito Hospital
Relación entre el nivel de dificultad de los procedimientos laparoscópicos y la incidencia de complicaciones durante la cirugía laparoscópica urológica en el Hospital Dr. Sardjito
Relation between difficulty level of laparoscopic procedures and the incidence of complications during urologic laparoscopic surgery in Dr. Sardjito Hospital
Archivos Venezolanos de Farmacología y Terapéutica, vol. 40, núm. 5, pp. 474-478, 2021
Sociedad Venezolana de Farmacología Clínica y Terapéutica

Esta obra está bajo una Licencia Creative Commons Atribución-SinDerivar 4.0 Internacional.
Recepción: Febrero , 28, 2021
Aprobación: Marzo , 15, 2021
Publicación: Agosto , 10, 2021
Abstract: Background: Laparoscopy is a minimally invasive procedure in which a camera and a light source are inserted into the abdomen, whereas the postoperative incision appears to be smaller than the conventional surgery incisions. In the field of urologic surgery, this method of surgical approach causes a few complications. Method: This research is a retrospective design using secondary data from medical records in Dr. Sardjito Hospital through a timeframe of January 2017 to January 2020. Included in this study were 82 cases of laparoscopic surgery patients. Study results were presented descriptively and analytically. Results: The incidence significantly increased with the increased difficulty level (p< 0.05). Statistically were the highest morbidities found in radical cystectomies, around 55%, if compared to other procedures (p<0.05). Types of complications found were vascular injuries (4 cases) and organ injuries (5 cases). Five laparoscopic procedures (6.1%) had to be converted to open procedures. There were no significant differences between the three groups according to conversion to open procedures (p > 0.05). Conclusion: The difficulty level of the procedures was correlated to the intraoperative complications. The higher the difficulty level of the urology laparoscopic procedures, the higher the incidence of complications. To decrease the incidence of complications, there have to be regularly scheduled standardized courses, to increase the knowledge in laparoscopic procedures, anatomical knowledge, and exposure to the different procedures.
Keywords: Laparoscopic urology, difficulty level, intraoperative complication.
Resumen: Antecedentes: La laparoscopia es un procedimiento mínimamente invasivo en el que se inserta una cámara y una fuente de luz en el abdomen, mientras que la incisión postoperatoria parece ser más pequeña que las incisiones de la cirugía convencional. En el campo de la cirugía urológica, este método de abordaje quirúrgico también causa algunas complicaciones. Método: Esta investigación es un diseño retrospectivo utilizando datos secundarios de registros médicos en el Hospital Dr. Sardjito durante el período de enero de 2017 a enero de 2020. Se incluyeron en este estudio 82 casos de pacientes de cirugía laparoscópica. Los resultados del estudio se presentaron de manera descriptiva y analítica. Resultados: La incidencia aumentó significativamente con el aumento del nivel de dificultad (p<0,05). Estadísticamente las mayores morbilidades encontradas fueron en las cistectomías radicales, alrededor del 55%, si se comparan con otros procedimientos (p <0,05). Los tipos de complicaciones encontradas fueron lesiones vasculares (4 casos) y lesiones de órganos (5 casos). Cinco procedimientos laparoscópicos (6,1%) tuvieron que convertirse en procedimientos abiertos. No hubo diferencias significativas entre los tres grupos según la conversión a procedimientos abiertos (p> 0,05). Conclusión: El nivel de dificultad de los procedimientos se correlacionó con las complicaciones intraoperatorias. Cuanto mayor sea el nivel de dificultad de los procedimientos laparoscópicos urológicos, mayor será la incidencia de complicaciones. Para disminuir la incidencia de complicaciones, se deben programar cursos estandarizados regularmente, para aumentar el conocimiento en procedimientos laparoscópicos, el conocimiento anatómico y la exposición a los diferentes procedimientos.
Palabras clave: Urología laparoscópica, nivel de dificultad, complicación intraoperatoria.
Introduction
Along with the ever-changing times, experts have developed various modern technologies, especially in the health sector. With the slogan "Dangerous Disease Requires Treatment That Is Not Too Harmful" surgeons have been using minimally invasive technology in their daily practice, one of which is the use of laparoscopy1-3.
Laparoscopy is a diagnostic and therapeutic surgical tool used to view intra-abdominal organs. Various studies have begun to assess the effectiveness and efficiency of laparoscopy when compared with conventional surgery. The results suggest that laparoscopy has the same effectiveness with an acceptable efficiency value when compared to conventional surgery. Laparoscopy shows clear advantages, namely reduced postoperative pain, better cosmetic aspects, faster recovery, shorter length of stay, and lower costs. Based on these various studies, laparoscopy is used throughout various surgeries, especially in various urological cases4-6.
Laparoscopic surgery does have many advantages, but that just like any other surgical intervention, laparoscopy also comes with a few complications. Significant complications of laparoscopy include vascular, visceral, intestinal, and urological injuries. Operational complications are classified into 2 groups based on the Satava hierarchy system, namely error 1. where there are no harmful consequences or errors that can be ignored, and error 2. where the error must be immediately identified and corrected (serious complications). Based on the European Scoring System (ESS) laparoscopic urological surgery is divided into 3 groups based on the complexity of the operation, namely: easy, difficult, and very difficult7-10.
Patients and Methods
Research Methods
The research design used in this study is a retrospective study of patient medical record data starting from surgery until patients were allowed to be treated as outpatients. The sampling technique used was Non-Probability Sampling using convenience sampling (accidental sampling). The reason for using this method is due to the unknown population of patients undergoing urologic laparoscopy at Dr. Sardjito Hospital.
Patient Study
The operating protocol at Dr. Sardjito Hospital was that all patients had been described and had signed informed consent beforehand. Samples taken in this study were urology patients who were performed laparoscopic measures at Dr. Sardjito Hospital from January 2017 to January 2020. The inclusion criteria of the sample in this study were urology patients who have performed a laparoscopy with pre-operative albumin, hemoglobin, and electrolyte values within normal limits. Meanwhile, exclusion criteria were patients who have had previous operations and patients with other comorbid diseases.
Statistics
In this study, the analysis was performed using SPSS statistical software ver. 22. The p-value was calculated using Chi-Square, and a value of p<0.05 was considered statistically significant.
Results
In this study, it was found that the characteristics of respondents were divided into gender, age, postoperative hospital stay, intraoperative bleeding, and duration of surgery. Based on the gender of the respondent, consisting of men and women. As for the characteristics of other respondents, it was averaged based on available data.
The general characteristics of patients from a total of 82 cases and 9 cases with complications are shown in Table 1. Various actions were taken to deal with the complications that arise so that no further morbidity and mortality occur. The incidence of complications in this study was around 11%. Gender in total cases was known to be higher in males than females, whereas in cases with complications the incidence of females was higher than males. On the other hand, the results of this study indicate that complications clearly occur in older patients. For the length of stay, it is known that in cases with complications it took 2 times longer than the time needed in total cases. In addition, as is well known, that the bleeding volume of surgery and the duration of surgery clearly increase in patients who have complications.
Complications Occurring in Laparoscopic Urology
Laparoscopic urology is divided into 3 groups, namely easy, difficult, and very difficult. The incidence of complications in all three groups is shown in figure 1. It is known that the more difficult the surgery performed, the incidence of complications will also increase significantly (p < 0.05).
The types of complications that occur are shown in figure 2, which consists of venous injuries, arterial injuries, and organ injuries. The incidence of vascular injury and organ injury is almost the same, namely, in this study, there were found 4 vascular injuries including inferior vena cava injury (2 cases), iliac artery injury (1 case), abdominal aortic injury (1 case), and organ injury (5 cases) including 1 case of pleural injury, 1 case of ileal injury, and 3 cases of rectal injury.
Convert Durante Operations to Open Operations
As shown in Table 2, cases of conversion to open surgery were 5 cases including 0 cases in the easy group, 1 case of the difficult group, and 4 cases in the very difficult group. Of the various cases, it is known that conversion to open surgery is carried out due to complications. It can be seen in Table 2 that the percentage of conversion to open operations is 6.1% of the total cases. With statistical analysis, there was no significant difference in the incidence rate of conversion from surgery to open surgery between easy, difficult, and very difficult groups (p > 0.05).
| Total cases(n = 82) | Cases with complications(n = 9) | |
| Male | 46 (56.1 %) | 3 (33.33 %) |
| Female | 36 (43.9 %) | 6 (66.67 %) |
| Average age (years) | 43 | 50 |
| Average length of stay (days) | 7 | 16 |
| Intraoperative bleeding (ml) | 586 | 2167 |
| Average surgery duration (hours) | 4 | 6 |
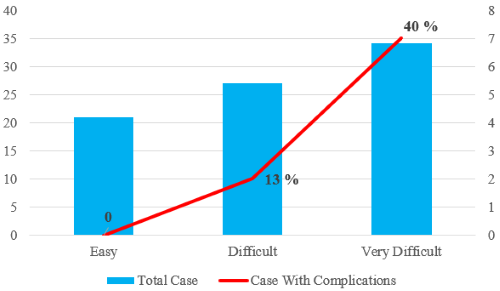
Figure 1.
Graph of the types of complications in urologic laparoscopy (p < 0.05)
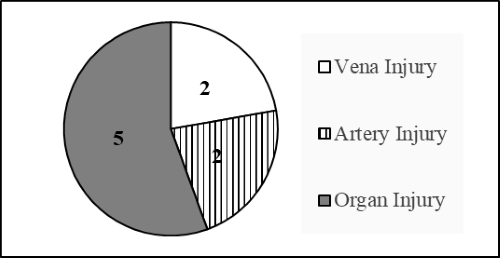
Figure 2.
Complications in the action group
| Urologic laparoscopic actions Total Case Convert to Open Operations | Complications | |||
| Easy 21 (25,6 %) | Resection of renal cyst | 4 | 0 | 0 |
| Cryptorchidism (diagnostic) | 9 | 0 | 0 | |
| Insertion tenckhoff catheter | 8 | 0 | 0 | |
| Difficult 27 (32,9 %) | Adrenalectomy | 4 | 0 | 0 |
| Ureterolithotomy | 3 | 0 | 0 | |
| Nephroureterectomy | 3 | 0 | 1 | |
| Pyeloplasty | 2 | 0 | 0 | |
| Nephrectomy | 11 | 1 | 1 | |
| Ureteral neoimplantation | 3 | 0 | 0 | |
| Tumor retroperitoneal | 1 | 0 | 0 | |
| Very Difficult 34 (41,5 %) | Partial nephrectomy | 3 | 0 | 0 |
| Nephrectomy (living donor) | 14 | 0 | 1 | |
| Partial cystectomy | 2 | 0 | 0 | |
| Radical cystectomy | 10 | 3 | 5 | |
| Radical nephrectomy | 4 | 1 | 1 | |
| Radical prostatectomy | 1 | 0 | 0 | |
| Total | 82 | 5 (6.1%) | 9 (11%) | |
Discussions
Complication incidence increases with an increase in the difficulty of urologic laparoscopy surgery. Based on ESS, laparoscopy surgery is divided into 3 difficulty groups, easy, difficult, and very difficult. This research found that very difficult surgeries showed complications with the highest incidence, followed by the other groups. This occurs because of complex anatomy and higher difficulty level. It is known that patients with complications must immediately receive treatment to correct the condition for a preferable prognosis and may undergo outpatient care11,12.
This research found the main complication was vascular injury. In the beginning, the nescience of anatomy and surgery technique caused bleeding, requiring immediate treatment or conversion of a method to open surgery. However, after laparoscopy was popularized, complications originating from adhesion, majorly being vascularization at tumor surfaces, and difficult surgery positions. During kidney and adrenal laparoscopy in difficult groups, is known in two vena cava inferior injuries13,14.
Vascular vena cava inferior wall avulsion mainly happens from surgery errors. Furthermore, there are two arterial injury cases (1 case Aorta abdominalis injury and 1 case of Iliaca artery injury) in this research. Injury in the big artery might be an iatrogenic vascular injury, the worst vascular injury. The aorta is very susceptible to retroperitoneal dissection, like in nephrectomy or retroperitoneal lymph gland dissection. In many cases, injuries happen because of organs reached close to the adventitia aorta, making imaging pre-surgery mandatory to guide intra-operative management13.
The data show that open surgery conversions in complication cases were done. There are many reasons for injuries in big blood vessels during laparoscopy, such as the lack of understanding of laparoscopic anatomy, an overwhelming amount of force, or surgery errors that can cause unpredicted situations, anatomical variations, or local dysplasia, and adhesions leading to increasing surgery difficulty. Laparoscopic treatment recommendations for major blood vessel injuries are as following; hemostasis by clamping or pressing, exact dissociation of perivascular tissue to clog blood vessel, sewing with 4-0 atraumatic stitches, and clamping blood vessel with a vascular clamp. However, if bleeding occurs and it is impossible to create a clear surgical environment, the operation method has to be conversed to open surgery. Furthermore, if bleeding cannot be stopped effectively in a short time, the patient also has to undergo open surgery13,14.
This study found that pleural injury is a secondary condition from diaphragmatic injury. This usually happens in upper surgical areas like kidney and adrenal surgeries. This research had 1 hemothorax case that happened during nephrectomy kidney donor surgery. Hemothorax is a complication seldomly reported. A previous study reported one case (0.08%) from 1129 patients that underwent urological laparoscopy surgeries. It is known that the intercostal artery ruptured, causing blood accumulation in the pleura after urological surgery. Conditions like this need thoracotomy treatment to correct patients' condition. Other reports have shown the existence of hemothorax after pyeloplasty laparoscopy, kidney mass cryoablation, and percutaneous nephrolithotomy15.
Every procedure inside or near the stomach have the risk of accidental intestine injury for example cystectomy, laparoscopy, percutaneous nephrolithotomy, cystostomy, depending on size and location of the injury and whether injury involves electrocautery16.
If the injury is caused by electrocautery, segmental resection must be done. The small intestine can usually be reconnected safely. The big intestine is normally also reconnected if the fecal spillage is minimal. Delayed identification of intestine injury is usually accompanied by prolonged ileus, abscess, and intraperitoneal sepsis. Early symptoms after laparoscopy do not imply intestinal injury. The patient may only show pain in one trocar wound, bloated stomach, diarrhea, and leucopenia. Surgical exploration and washing are indicated in patients with uncontrollable leakage to obtain or identify a leak source. Controlled leakage (abscess) or retroperitoneal intestine injury in patients is declared stable if percutaneous drainage management has succeeded17,18.
Rectal injury is an interesting intestinal injury case in urology. Not more than 1% of cases of complications in prostatectomy nor cystectomy have been reported. Computed tomography (CT) images of a previous study showed air in the urinary bladder and rectum in patients with rectum injuries that were not identified in surgical treatment that needed proximal intestine diversion. Cystogram examination showed fistula between the urethra and rectum19.
Developments in surgical technique have decreased surgery duration and complication incidences, being that various unpredictable complications are still present in urological laparoscopy. Indication in urological laparoscopy must closely be controlled and must be accompanied by a thorough understanding of micrological structure during surgery to prevent accidental injuries. Complications can be minimalized by improving surgical technique, substantiate anatomy knowledge, and increased experience. This through this surgeon can benefit from minimally invasive surgeries, without causing complications20.
Conclusion
In this research, a relation between difficulty level of surgery and intraoperative complication incidences in urological laparoscopy has been established in RSUP Dr. Sardjito (a public hospital). The more difficult the urological laparoscopy the higher the level of incidences of complications occurred. Complications that were discovered in the study included vascular and organ injuries, which needed corrections with laparoscopy or open surgeries, depending on objective condition. This is related to the anatomy understanding and difficulty of surgery.
References
1. Wein AJ. et al. Campbell-Wals Urology, Elsevier. 2016.
2. Taneja SS. dan Shah O. Complications of Urologic Surgery Diagnosis, Prevention, and Management Fifth Edition. Elsevier. 2018. doi: 10.1017/CBO9781107415324.004.
3. Zollinger R, dan Ellison E. () Zollinger’s Atlas of Surgical Operations, Mc Graw Hill Medical. 2011. doi: 10.1007/s13398-014-0173-7.2.
4. Jiang X, Danerson C, Schnatz PF. The safety of direct trocar versus veress needle for laparoscopic entry: A meta-analysis of randomized clinical trials. Journal of Laparoendoscopic dan Advanced Surgical Techniques. 2012;22(4):362–370. doi: 10.1089/lap.2011.0432.
5. Kaistha S. et al. Laparoscopic Access: Direct Trocar Insertion Versus Open Technique. Journal of Laparoendoscopic dan Advanced Surgical Techniques. 2019;29(4):489–494. doi: 10.1089/lap.2018.0408.
6. Guo J. et al. Intraoperative serious complications of laparoscopic urological surgeries: A single institute experience of 4,380 procedures. International Braz J Urol. 2019;45(4):739–746. doi: 10.1590/S1677-5538.IBJU.2018.0601.
7. Montes SFP. Intraoperative laparoscopic complications for urological cancer procedures’, World Journal of Clinical Cases. 2015;3(5): p. 450. doi: 10.12998/wjcc.v3.i5.450.
8. Patel PG. et al. Direct Trocar Entry in Laparoscopic Surgeries: A Retrospective Study Body Mass Index Emergency or Planned Surgery. Research Article Gastroenterology & Hepatology Journal (GHJ) Gastroenterol Hepatol J. 2017;1(1):29–33.
9. Sanli O. et al. Prospective evaluation of complications in laparoscopic urology at a mid-volume institution using standardized criteria: Experience of 1023 cases including learning curve in 9 years. Journal of Minimal Access Surgery. 2016;12(1):33–40. doi: 10.4103/0972-9941.158154.
10. Taye MK. et al. Open versus closed laparoscopy: Yet an unresolved controversy’, Journal of Clinical and Diagnostic Research.2016;10(2): QC04–QC07. doi: 10.7860/JCDR/2016/18049.7252.
11. Petrut B. et al. V1 - Accidents and complications of the laparoscopic approach. European Urology Supplements.2019;18(2):e2425. https://doi.org/10.1016/S1569-9056(19)32116-5
12. Sabharwal A, Kumar A. Laparoscopic Surgery in Urology. Apollo Medicine.2006;3(4): 371-375. https://doi.org/10.1016/S0976-0016(11)60225-1
13. Cheng S. et al. Management of major vascular injury in laparoscopic urology. Laparoscopic, Endoscopic and Robotic Surgery.2020;3(4):107–110. https://doi.org/10.1016/j.lers.2020.08.002
14. Liu Z. et al. Completely laparoscopic versus open radical nephrectomy and infrahepatic tumor thrombectomy: Comparison of surgical complexity and prognosis. Asian Journal of Surgery. 2021;44(4):641–648. https://doi.org/10.1016/j.asjsur.2020.12.003
15. Ngo TK. et al. Symptomatic pneumopericardium – A rare complication following retroperitoneal laparoscopic nephrectomy: A case report. International Journal of Surgery Case Reports. 2021;79:299–301. https://doi.org/10.1016/j.ijscr.2021.01.059
16. Cathelineau GVX. et al. Complications of Transperitoneal Laparoscopic Surgery in Urology: Review of 1,311 Procedures at a Single Center. The Journal of Urology.2002;168(1):23–26. https://doi.org/10.1016/S0022-5347(05)64823-9
17. Rios DS. et al. Post-surgical complications in patients with bladder cancer treated with cystectomy: Differences between open and laparoscopic approach. Actas Urológicas Españolas (English Edition). 2019;43(6):305–313. https://doi.org/10.1016/j.acuroe.2019.05.001
18. Hindi SA. Khalaf Z. The outcome of laparoscopic-assisted orchidopexy in very young children: A single hospital experience. Journal of Pediatric Urology. 2021. https://doi.org/10.1016/j.jpurol.2021.03.004
19. Kim TN. et al. Three different laparoscopic techniques for the management of iatrogenic ureteral injury: A multi-institutional study with medium-term outcomes. Asian Journal of Surgery. 2021. https://doi.org/10.1016/j.asjsur.2021.01.027
20. Manfredi M. et al. 586 - Perioperative complication predictors in laparoscopic adrenalectomy a single-center multivariate analysis. European Urology Open Science. 2020;19(2):e911. https://doi.org/10.1016/S2666-1683(20)33189-X