Artículos
Placental location in the uterus and its roles in fetal, maternal outcome and mode of delivery
Ubicación de la placenta en el útero y su función en el resultado fetal, materno y en el modo de parto

Placental location in the uterus and its roles in fetal, maternal outcome and mode of delivery
Archivos Venezolanos de Farmacología y Terapéutica, vol. 40, núm. 5, pp. 487-491, 2021
Sociedad Venezolana de Farmacología Clínica y Terapéutica

Esta obra está bajo una Licencia Creative Commons Atribución-SinDerivar 4.0 Internacional.
Recepción: Febrero , 28, 2021
Aprobación: Marzo , 15, 2021
Publicación: Agosto , 10, 2021
Abstract: Background: The placental location had a substantial correlation with pregnancy outcome and mode of delivery. The study aims to detect the location of the placenta in pregnant term woman and its relation to fetal and maternal health and then its affection on the mode of delivery in each type. Method: Cross-sectional study for 100 patients admitted to delivery (vaginal or C/S) in a public and private hospital in Babylon city in Iraq from January 2018 to December 2019. We check fetal wellbeing, GA (Gestational age), amount of amniotic fluid, and finally, we detect placental location. Take history about age, parity, any medical diseases for her examination such as BP, BMI, Abdominal examination, and PV. Examination. Then send for U/S to detect placental location, then detect the mode of delivery according to a pregnancy complication, fetal wellbeing, and obstetric indications after delivery check fetal weight. Results: 100 cases females evaluated for the location of placental, feto-maternal consequence, and style of delivery. Anterior placenta associate with a severe danger of diabetes mellitus that occurs during pregnancy and abruption placental. Concerning fetal consequence, an anterior placenta was significantly associated with intrauterine growth delay, while intrauterine fetal demise had no significant correlation. There is a positive correlation between fetal weight and placental location with the mode of delivery. Conclusion: Implantation of anterior placental related with a severe danger of pregnancy-induced hypertension, DM, abruption placental; intrauterine growth delay and intrauterine fetal demise also rise c/s delivery. The posterior placenta is associated significantly with preterm labor. Placental location is an essential determinant of pregnancy outcome.
Keywords: Anterior, posterior, fundal, placenta, c/s, vaginal delivery, pregnancy outcome, fetal and maternal outcome.
Resumen: Antecedentes: la ubicación de la placenta tuvo una correlación sustancial con el resultado del embarazo y el modo de parto. El estudio tiene como objetivo detectar la ubicación de la placenta en gestantes a término y su relación con la salud materna y fetal y luego su afectación sobre el modo de parto en cada tipo. Método: Estudio transversal de 100 pacientes ingresadas por parto (vaginal o C / S) en un hospital público y privado de la ciudad de Babylon en Irak desde enero de 2018 a diciembre de 2019. Verificamos el bienestar fetal, EG (edad gestacional), cantidad de líquido amniótico y, finalmente, detectamos la ubicación placentaria. Tome el historial de edad, paridad, cualquier enfermedad médica para su examen, como presión arterial, índice de masa corporal, examen abdominal y PV. Examen. Luego, envíe a U / S para detectar la ubicación de la placenta, luego detecte el modo de parto de acuerdo con una complicación del embarazo, el bienestar fetal y las indicaciones obstétricas después del parto, verifique el peso fetal. Resultados: 100 casos de mujeres evaluados para la ubicación de la placenta, consecuencia feto-materna y estilo de parto. La placenta anterior se asocia con un grave peligro de diabetes mellitus que se produce durante el embarazo y el desprendimiento de placenta. Con respecto a las consecuencias fetales, una placenta anterior se asoció significativamente con el retraso del crecimiento intrauterino, mientras que la muerte fetal intrauterina no tuvo una correlación significativa. Existe una correlación positiva entre el peso fetal y la ubicación de la placenta con el modo de parto. Conclusión: Implantación de placenta anterior relacionada con un grave peligro de hipertensión inducida por el embarazo, DM, desprendimiento de placenta; El retraso del crecimiento intrauterino y la muerte fetal intrauterina también aumentan c / s del parto. La placenta posterior se asocia significativamente con el trabajo de parto prematuro. La ubicación de la placenta es un determinante esencial del resultado del embarazo.
Palabras clave: Anterior, posterior, fondo uterino, placenta, c / s, parto vaginal, resultado del embarazo, resultado fetal y materno.
Introduction
The placenta is an organ that attaches the developing fetus by the umbilical cord to the uterine layers to permit nutrient uptake, thermo-regulation, waste removal, and gas exchange by the mother's blood supply; to fight against internal infection, and to produce hormones that preserve the pregnancy. So that the determination of the location of the placenta inside the uterus is useful to discover any complications earlier and manage them accordingly. The blood supply of the uterus comes from the uterine and ovarian arteries. Each uterine artery supplies its corresponding side of the uterus, it has a substantial number of branches, and has anastomoses with the contralateral uterine artery1, the blood supply of the uterus is not constantly spread. The location of placental implantation and then placenta location inside the uterus are significant elements of placental blood source and therefore the fetal and maternal outcomes2. Several studies described that placental location has special effects on pregnant females like preterm birth3, intrauterine growth retardation (IUGR)2, fetal malposition, malpresentation, and the development of hypertension4,5. The anterior placental location was demonstrated to be associated with increased risks of fetal intrauterine growth retardation and when the placenta is situated in the fundus zone transport the risk of early separation of the membrane is higher. Studies on the idea that connections between IUGR and the placental location are conflicting4,6. The placenta attaches to the uterus wall, and the fetal umbilical cord arises from it. The organ is commonly attached to the top, front, or back of the uterus. In rare cases, the placenta might attach to the lower part of the uterus. When this occurs, it has called a low-lying placenta (placenta Previa)7. This study aimed to detect the location of the placenta in pregnant term woman and its relation to fetal and maternal health and its influence on the mode of delivery in each type.
Methods
In this study, 100 pregnant women were enrolled randomly with their previous consent. Their histories concerning any medical diseases like hypertension, diabetes, vaginal bleeding, decrease size of the abdomen, decrease fetal movement were evaluated4,8,9. All eligible patients underwent routine CTG (Cardiotocography), abdominal examination and measure neonatal birth weight after delivery whether vaginally or cesarean section (C/S) (mode of delivery). Patients were enrolled with singleton pregnancies who checked in U/S (37 - 41 weeks' gestation) from January 2018 to the end of December 2019 and who delivered at Babylon hospitals. The exclusion criteria were any patients who were contraindicated for vaginal delivery, multiple pregnancies, cases of persistent placenta Previa, persistent low‐lying placentas, preterm baby and fetal anomalies, and previously scarred uterus. We depend on the last U/S that determined placental location. General history was obtained to achieve baseline data on all participants, such as age, gravidity, parity, body mass index, medical and obstetric histories. The delivery information was collected, including gestational age (GA) at delivery, birth weight, and diagnosis of any diseases that present or exacerbate in pregnancy.
All data were analyzed using SPSS 22 (SPSS, Chicago, IL, USA). Data were expressed as mean ± standard deviation and the frequencies as percentages. Differences between the two groups were assessed using the Chi-square test. P-value considered significant at ≤ 0.05.
Results
Data from this study showed that the percentage of each type of placental location whether anterior, posterior, and fundal, and its relationship with fetal and maternal wellbeing and mode of delivery. The low-lying placenta was excluded from this study because too many studies were done for this subject and need much data to find its relationship with the fetal and maternal outcome because it is dangerous and needs close follow-up.
In the present study, we found a relationship between placental location and other factors in pregnancy. These a cross-sectional study of 100 women with age of 31.6±6 years old, from which 90% of them were 25 years and more, a BMI of 30±5, with a gestational age of 37±2 weeks and fetal weight of 3132±682. 77% were multiparty, 33% had a previous miscarriage and 13% had previous preterm. 26%, 14%, 7%, 25%, 17%, and 13% presented pregnancy-induced hypertension (PIH), pregnancy-induced diabetes mellitus (P.DM), AP (Amniotic Pressure), PROM (prelabor rupture of membranes), IUD (intrauterine device), and IUGR (intrauterine growth retardation), respectively. 66% delivered normally while 34% delivered by C/S, 45% were obese and 81% had a baby with 2500 g weight and more (Table 1).
| Variables | Frequency | Percentage | ||
| parity | multipara | 77 | 77.0% | |
| Nullipara | 23 | 23.0% | ||
| Previous miscarriage | No | 67 | 67.0% | |
| Yes | 33 | 33.0% | ||
| Previous Preterm | No | 87 | 87.0% | |
| Yes | 13 | 13.0% | ||
| Hypertension | No | 74 | 74.0% | |
| Yes | 26 | 26.0% | ||
| DM (diabetes mellitus) | No | 86 | 86.0% | |
| Yes | 14 | 14.0% | ||
| Abruption’s placenta | No | 93 | 93.0% | |
| Yes | 7 | 7.0% | ||
| Premature rupture membrane | No | 75 | 75.0% | |
| Yes | 25 | 25.0% | ||
| Intrauterine death | No | 83 | 83.0% | |
| Yes | 17 | 17.0% | ||
| Intrauterine growth retardation | No | 87 | 87.0% | |
| Yes | 13 | 13.0% | ||
| Mode of delivery | C/S | 34 | 34.0% | |
| NVD | 66 | 66.0% | ||
| Maternal Age | less than 25 years | 10 | 10.0% | |
| 25 and above | 90 | 90.0% | ||
| BMI (body mass index) | normal | 12 | 12.0% | |
| overweight | 43 | 43.0% | ||
| obese | 45 | 45.0% | ||
| Baby Weight | less than 2500 g | 19 | 19.0% | |
| 2500 g and more | 81 | 81.0% |
In figure 1 is shown that 41% of females presented fundal placental location, while 37% of them with anterior location and 22% of females with a posterior placental location.
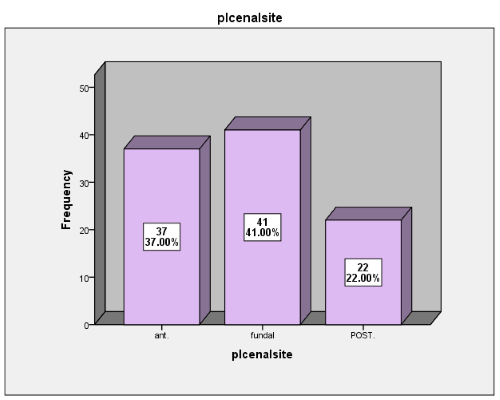
Figure 1.
Distribution of placental location.
According to Table 2, there is a significant association between placental location and previous miscarriage; 54% of anterior placenta have a previous miscarriage and 24% of fundal placenta have previous miscarriage while 13% of posterior placenta have a previous miscarriage. In addition, there is a significant association between placental location and previous preterm; 27% of anterior placenta have the previous preterm and 7% of fundal placenta have the previous preterm while 0% of posterior placenta have the previous preterm. There is a significant association between placental location and P.DM; 30% of anterior placenta have DM and 0% of fundal placenta have DM while 14% of posterior placenta have DM. Also, a significant association between the placental location and AP; 0% of anterior placenta have AP and 0% of fundal placenta have AP while 14% of posterior placenta have AP. There is a significant association between placental location and PROM; 8% of anterior placenta have PROM and 34% of fundal placenta have PROM while 36% of posterior placenta have PROM. There is a significant association between placental location and IUGR; 27% of anterior placenta have IUGR and 0% of fundal placenta have IUGR while 14% of posterior placenta have IUGR. There is a significant association between placental location and age of females; 100% of anterior placenta at age ≥25 years old and 85% of fundal placenta at age ≥25 years old while 82% of posterior placenta at age ≥25 years old. There is no significant association between placental location and parity, PIH, and IUD (Table 2).
| variables | placental location | P-value | |||
| Anterior | fundal | posterior | |||
| parity | multipara | 30 | 32 | 15 | 0.51 |
| 81.1% | 78.0% | 68.2% | |||
| primi | 7 | 9 | 7 | ||
| 18.9% | 22.0% | 31.8% | |||
| Previous miscarriage | no | 17 | 31 | 19 | 0.002 |
| 45.9% | 75.6% | 86.4% | |||
| yes | 20 | 10 | 3 | ||
| 54.1% | 24.4% | 13.6% | |||
| previous preterm | No | 27 | 38 | 22 | 0.004 |
| 73.0% | 92.7% | 100.0% | |||
| Yes | 10 | 3 | 0 | ||
| 27.0% | 7.3% | 0.0% | |||
| DM (diabetes mellitus) | no | 26 | 41 | 19 | 0.001 |
| 70.3% | 100.0% | 86.4% | |||
| yes | 11 | 0 | 3 | ||
| 29.7% | 0.0% | 13.6% | |||
| hypertension | No | 23 | 33 | 18 | 0.12 |
| 62.2% | 80.5% | 81.8% | |||
| Yes | 14 | 8 | 4 | ||
| 37.8% | 19.5% | 18.2% | |||
| AP (Amniotic Pressure) | No | 37 | 41 | 15 | 0.0001 |
| 100.0% | 100.0% | 68.2% | |||
| Yes | 0 | 0 | 7 | ||
| 0.0% | 0.0% | 31.8% | |||
| PROM (prelabor rupture of membranes ) | No | 34 | 27 | 14 | 0.011 |
| 91.9% | 65.9% | 63.6% | |||
| Yes | 3 | 14 | 8 | ||
| 8.1% | 34.1% | 36.4% | |||
| IUD (intrauterine device) | No | 29 | 32 | 22 | 0.06 |
| 78.4% | 78.0% | 100.0% | |||
| Yes | 8 | 9 | 0 | ||
| 21.6% | 22.0% | 0.0% | |||
| IUGR (intrauterine growth retardation) | No | 27 | 41 | 19 | 0.002 |
| 73.0% | 100.0% | 86.4% | |||
| Yes | 10 | 0 | 3 | ||
| 27.0% | 0.0% | 13.6% | |||
| Maternal age | <25 years | 0 | 6 | 4 | 0.035 |
| 0.0% | 14.6% | 18.2% | |||
| 25 and above | 37 | 35 | 18 | ||
| 100.0% | 85.4% | 81.8% |
P-value less than 0.05 (significant).
Figure 2 shows the distribution of placental location and mode of delivery. 10% of anterior placenta normally delivered, 41% of fundal placenta delivered normally, while 15% of posterior placenta normally delivered, 27% of anterior placenta delivered by C/S.
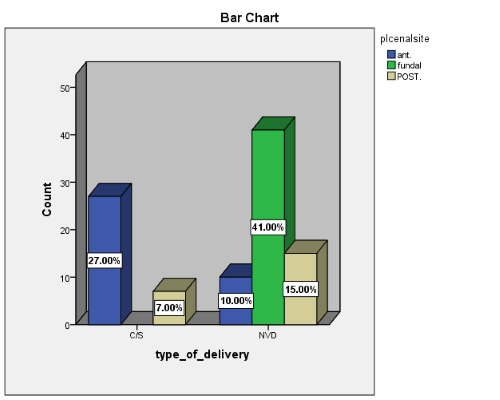
Figure 2.
Distribution of placental location and mode of delivery. P-value 0.0001 (significant).
Figure 3 demonstrates the distribution of placental location and BMI of females. 60% of the anterior placenta are obese, and 46% of the fundal placenta are obese, while 18% of the posterior placenta are obese.
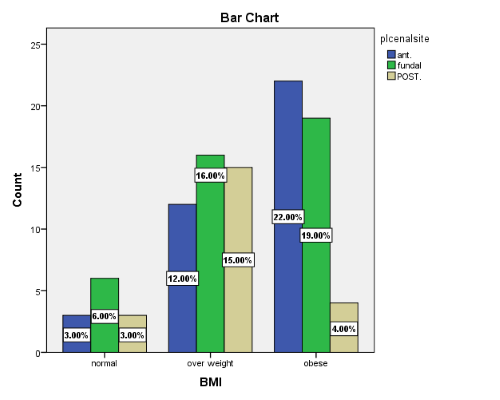
Figure 3.
Distribution of placental location and BMI of females. P-value 0.035 (significant)
Figure 4 reveals the distribution of placental location and baby weight. 28% of anterior placenta delivered the baby with weight ≥2500gm, 38% of fundal placenta delivered baby with weight ≥2500gm, while 15% of posterior placenta delivered the baby with weight ≥2500gm.
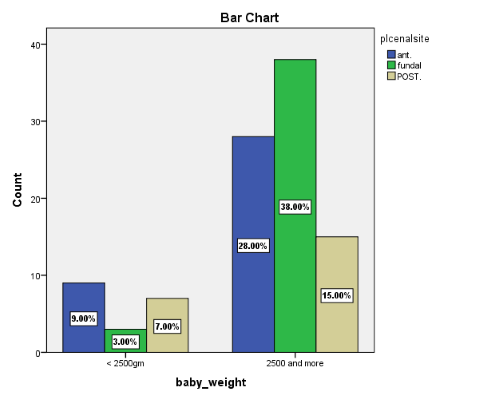
Figure 4.
Distribution of placental location and baby weight. P-value =0.035 (significant).
Discussion
In this study, we establish the location of the placenta by U/S in term pregnant woman; we found that many complications may occur with anterior type than posterior and fundal types due to less blood supply for this area, such as Diabetes mellitus, placental abruption, intrauterine growth retardation while we found premature rupture membrane more with fundal placenta because fetal membrane which is fragile point present low down and preterm delivery more with the posterior placenta. C/S rate increase with anterior one; the acceptable explanations are many complications occur during pregnancy. In addition, it increases malposition and malpresentation. Kalafat et al.10 stated a significant association between fundal placenta and hypertension and the study of 2. Kalanithi et al.,2 there is a substantial correlation between placental location and pre-eclampsia, Granfors et al.6 stated that anterior and posterior placentas are more common in pregnancies with IUGR while no case of IUGR in our pregnant sample and that corresponding to our result, while no correlation between placental location and hypertension in our study. This study showed a significant association of hypertension and IUGR with placental location, either fundal or anterior.
On the contrary, a current study of >3000 pregnancies11 defines the danger of consuming IUGR fetus not increased by placental implantation location. Roberts et al.3 identified that the fundal placenta takes a significantly advanced danger of early separation of the membrane. The hypothetical that placental fundal location seats the frailest point of the membrane above the cervical os and therefore disposes the females to an early disagreement of the membrane with entirely of the considerable opposing concerns, and that not consistent to our consequences. Since of the rough uterine blood source2, there is elongation in the posterior wall of the gravid uterus12 and slightly thicker13]. These issues may distress the uterine blood source, particularly as the uterus enlarges to put up the pregnancy. Warland et al.14, described that placental location either posteriorly and anteriorly is more likely to consequence in stillbirth. Its exact reason is unknown. Many studies have shown a significant association of anterior placenta with high occurrence of hypertension, DM, abruption placenta, IUD, and IUGR, and no significant association between placental location with hypertension and intrauterine demise. Karthika et al.15, not detect a significant difference in BMI mean in placental location groups. In contrast, the current study detects a substantial association between the IUGR significant association with the anterior location of the placenta. Lucy et al.2 designated a meaningful positive relationship between IUGR and lateral location of the placenta, relatively than anterior plus posterior. Granfors et al.. stated that the fundal location of the placentas is further public than the anterior and posterior location in pregnant females with pre-eclampsia and/or IUGR. Kalafat et al.10show a significant connotation between the fundal location of the placenta and hypertension; in some revisions, the fundal location of the placenta associated with a lesser danger of problems than other placental locations, and so, the posterior placental location was selected1,6,11,13,16. SGA, besides preterm birth, was additional communal in females with a lateral or fundal location of the placenta, matched with the posterior location of the placenta16. Other studies show no association between the fundal location of the placenta and the SGA fetus11,16,17. A current study found that fundal and lateral location of the placenta associated with a breach appearance in full-term deliveries, approving consequences from previous studies16,18. A fundal or anterior location of the placenta prevents activities of the fetus essential for an impulsive version to a cephalic appearance. Preceding studies show that the anterior location of the placenta is associated with unsuccessful experimental of outside version19. There is a high risk of cesarean delivery in our study than vaginal delivery, which could be explained by many accompanying medical diseases and the important cause of malpresentation or malposition that delayed or obstructed labor; there is a significant correlation between the location of the placenta and mode of delivery.
CONCLUSION
Our data shows that the posterior placental location is the least related to a number of adverse pregnancies, delivery, and infant outcomes. In addition, anterior placental location seems to be associated with a slightly increased risk of harmful complications in pregnancy and delivery outcomes. All these complications lead to increase C/S more than vaginal delivery there are few studies about placental location and the adverse outcome, so we need a large number of reports on that subject to support or discard our finding.
References
1. Sieunarine K, Boyle DC, Corless DJ, Noakes DE, Ungar L, Marr CE, Lindsay I, Del Priore G, Smith JR. Pelvic vascular prospects for uterine transplantation. Int Surg. 2006 Jul-Aug;91(4):217-22.
2. Kalanithi, L.E.G., Illuzzi, J.L., Nossov, V.B., Frisbæk, Y., Abdel-Razeq, S., Copel, J.A. and Norwitz, E.R. (2007), Intrauterine Growth Restriction and Placental Location. Journal of Ultrasound in Medicine, 26: 1481-1489.
3. Roberts CL, Wagland P, Torvaldsen S, Bowen JR, Bentley JP, Morris JM. Childhood outcomes following preterm prelabor rupture of the membranes (PPROM): a population-based record-linkage cohort study. J Perinatol. 2017 Nov;37(11):1230-1235.
4. Magann EF, Doherty DA, Turner K, Lanneau GS, Jr, Morrison JC, Newnham JP. Second trimester placental location as a predictor of an adverse pregnancy outcome. J Perinatol. 2007; 27:9–14.
5. Zia S. Placental location and pregnancy outcome. J Turk Ger Gynecol Assoc. 2013;14(4):190-193.
6. Granfors M, Stephansson O, Endler M, Jonsson M, Sandström A, Wikström AK. Placental location and pregnancy outcomes in nulliparous women: A population-based cohort study. Acta Obstet Gynecol Scand. 2019 Aug;98(8):988-996.
7. Weiner Z, Younis JS, Blumenfeld Z, Shalev E. Assessment of uterine placental circulation in thrombophilic women. Semin Thromb Hemost. 2003 Apr;29(2):213-8.
8. Adam I, Haggaz AD, Mirghani OA, Elhassan EM. Placenta previa and pre-eclampsia: analyses of 1645 cases at Medani Maternity Hospital, Sudan. Front Physiol. 2013; 4:32. Published 2013 Feb 28.
9. Newton ER, Barass V, Cetrulo CL. The epidemiology and clinical history of asymptomatic previa. ObsteGynecol. 1984; 148:7438.
10. Kalafat, E., Thilaganathan, B., Papageorghiou, A., Bhide, A. & Khalil, A. Significance of placental cord insertion site in twin pregnancy. Ultrasound in Obstetrics and Gynecology, 2018,52, 378–384.
11. Abramowicz, J. S. & Sheiner, E. Ultrasound of the Placenta: A Systematic Approach. Part II: Functional Assessment (Doppler). Placenta, 2008, 29, 921–929.
12. Ishibashi, H, Miyamoto, M, Shinmoto, H, et al. The use of magnetic resonance imaging to predict placenta previa with placenta accreta spectrum. Acta Obstet Gynecol Scand. 2020; 00: 1– 9.
13. Ptacek I, Sebire NJ, Man JA, Brownbill P, Heazell AE. Systematic review of placental pathology reported in association with stillbirth. Placenta. 2014 Aug;35(8):552-62
14. Warland J, McCutcheon H, Baghurst P. Placental position and stillbirth: a case-control study. Journal of Clinical Nursing. 2009; 18:1602–6.
15. Karthika , Devarajan K, Kives S, Ray JG. Placental location and newborn weight. J Obstet Gynaecol Can. 2012; 34:325–9.
16. Fung TY, Sahota DS, Lau TK, Leung TY, Chan LW, Chung TK. Placental site in the second trimester of pregnancy and its association with subsequent obstetric outcome. Prenat Diagn. 2011; 31: 548‐ 554.
17. Magann EF, Doherty DA, Turner K, Lanneau GS Jr, Morrison JC, Newnham JP. Second trimester placental location as a predictor of an adverse pregnancy outcome. J Perinatol. 2007; 27: 9‐ 14.
18. Witkop CT, Zhang J, Sun W, Troendle J. Natural history of fetal position during pregnancy and risk of nonvertex delivery. ObstetGynecol. 2008; 111: 875‐ 880.
19. Kok M, van der Steeg JW, van der Post JA, Mol BW. Prediction of success of external cephalic version after 36 weeks. Am J Perinatol. 2011; 28: 103‐ 110.
Notas de autor
ban200372@gmail.com